
Abstract
Objectives
The aim of this study is to evaluate the association of venous thromboembolism with arterial stiffness by cardio-ankle vascular index method.
Method
We included 52 patients with a documented lower extremity venous thromboembolism within the last six months and 52 healthy subjects to this cross sectional observational study.
Results
Cardio-ankle vascular index (8.58 ± 1.60 versus 7.05 ± 1.44, p < 0.001, respectively) and systolic blood pressure (128.02 ± 7.13 mmHg versus 123.94 ± 8.12 mmHg, p = 0.008, respectively) were significantly higher among patients with venous thromboembolism than controls. Cardio-ankle vascular index was an independent predictor of venous thromboembolism in multivariate logistic regression analysis (p < 0.001, odds ratio = 1.864, 95% confidence interval = 1.370–2.536). Cardio-ankle vascular index value > 7.8 had a sensitivity of 82.7% and a specificity of 80.8% for predicting venous thromboembolism (area under curve = 0.789, 95% confidence interval = 0.698–0.863, p < 0.001) in receiver operating characteristic curve analysis.
Conclusion
We found that arterial stiffness was increased in patients with venous thromboembolism which highlights the fact that arterial and venous circulation is in continuum and an insult may affect both of these circuits.
Introduction
Vascular system is composed of arterial and venous circulation. Although both circuits are in continuum, the disorders involving these circuits are evaluated separately. Venous thromboembolism (VTE) is a multifactorial disease.1,2 For the formation of thrombosis, endothelial damage and/or thrombogenic tendency and/or stasis is required. Atherosclerosis, arteriolosclerosis, and venous thrombosis have common etiologies including inflammation and endothelial dysfunction. Arterial stiffness is an important marker of atherosclerosis and arteriolosclerosis. Arterial stiffness is associated with major adverse cardiovascular events. 3 As a result of increased arterial stiffness, systolic blood pressure increases and this leads to ventricular hypertrophy and increased myocardial oxygen demand. 4 Increased arterial stiffness is related to coronary atherosclerosis and recurrence of adverse cardiac events.5,6 Cardio-ankle vascular index (CAVI), which is weakly influenced by systolic blood pressure, is a sensitive marker for the atherosclerosis and arteriolosclerosis.6–8 However, the alteration in arterial system in patients with VTE is underevaluated. The aim of this study is to evaluate the association of VTE with arterial stiffness by CAVI method.
Methods
Study populations
We included 52 patients with a history of venous thrombosis within the last six months and 52 healthy subjects to this cross sectional observational study (Figure 1). All patients had documented lower extremity venous thrombosis. Patients with hypertension, diabetes, active infection, coronary artery disease, heart failure, pulmonary hypertension, peripheral arterial disease, secondary VTE (cancer, pregnancy, leg trauma, immobilization for more than one week or current users of oral estrogen with or without concomitant progestin use), atrial fibrillation, and moderate to severe valvular heart disease were excluded from the study. Informed consent was given by all participants and the local ethics committee approved the study protocol.
Flow diagram.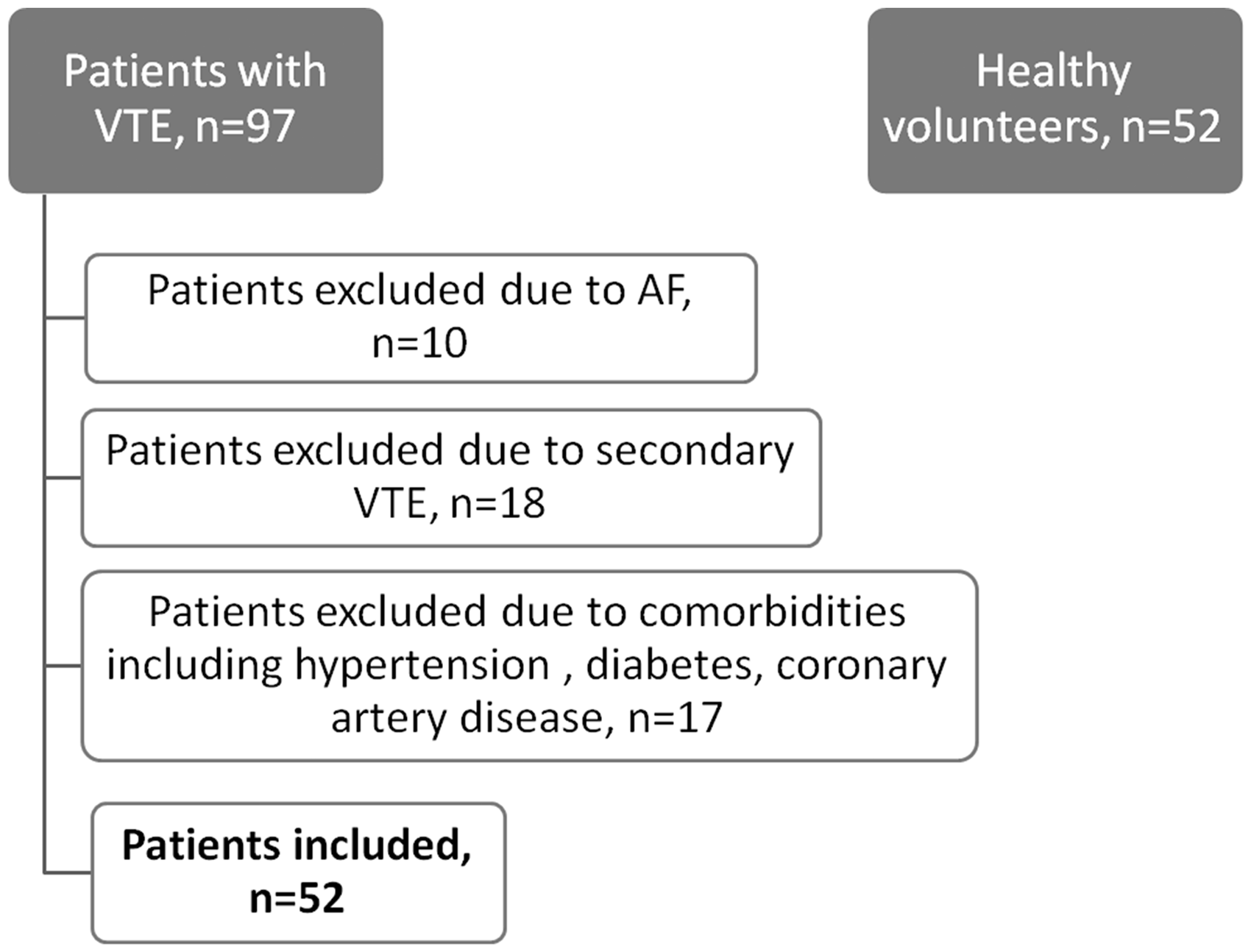
Basal demographic, clinical, and echocardiography evaluation
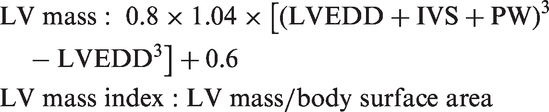
Weights of the patients, in light clothes and without shoes, were measured in kilograms, and their heights were also measured. Body mass index (kg/m2) was calculated by dividing body weight in kilograms by the square of body height in meters. Transthoracic echocardiography assessment (Vivid S5 General Electric, Norway) was performed in patients according to the standards of the American Society of Echocardiography. Left ventricular mass was calculated according to Devereux formula
Dyslipidemia was defined as total cholesterol >190 mg/dl or previous diagnosis of dyslipidemia. Patients who self-reported as having smoked during the previous six months were classified as smokers. Venous blood samples were drawn after a 12 h overnight fast. Serum glucose, total cholesterol, and triglycerides were determined using standard automatic enzymatic methods. High density lipoprotein (HDL) cholesterol was determined after specific precipitation and low density lipoprotein (LDL) cholesterol was determined by the Friedewald formula.
Blood pressure and CAVI measurements
Blood pressure was measured, in compliance with World Health Organization guidelines, by using a mercury sphygmomanometer (ERKA, Germany) with a cuff appropriate to the arm circumference, in patients at rest for 20 minutes (Korotkoff phase I for systolic blood pressure and V for diastolic blood pressure).

CAVI was measured using a VaSera VS-1000 CAVI instrument (Fukuda Denshi Co. Ltd., Tokyo, Japan). CAVI was measured in the morning after 15 minutes of rest. Briefly, cuff was applied to the bilateral upper arms and ankles, with the subject supine and the head held in the midline position. Electrocardiography, phonocardiography, and pressures and waveforms of brachial and ankle arteries were measured and pulse wave velocity and subsequently CAVI were calculated automatically. CAVI measurements were performed by experienced cardiologist who was blinded to ultrasonography.
CAVI is determined by the following equation

Statistical analysis
SPSS 17.0 for Windows was used for statistical analysis. An analysis of normality of the continuous variables was performed with the Kolmogorov–Smirnov test. Continuous variables are expressed as mean ± standard deviation and categorical variables are expressed as percentage. Comparisons of continuous variables were performed using the unpaired Student’s t-test or Mann–Whitney U test and categorical variables were compared with the chi-square test. Multivariate logistic regression analysis was performed in order to find independent associates of VTE. Variables including, CAVI, smoking, and systolic blood pressure were entered in the multivariate regression model. Receiver operating characteristic curve (ROC) analysis was carried out to find the cutoff value to predict VTE. A p value of ≤ 0.05 was considered statistically significant.
Results
The characteristics of patients.

LVEDV: left ventricle end diastolic volume; LVESD: left ventricle end systolic volume; VTE: venous thromboembolism.
The independent predictors of venous thromboembolism in multivariate logistic regression analysis.
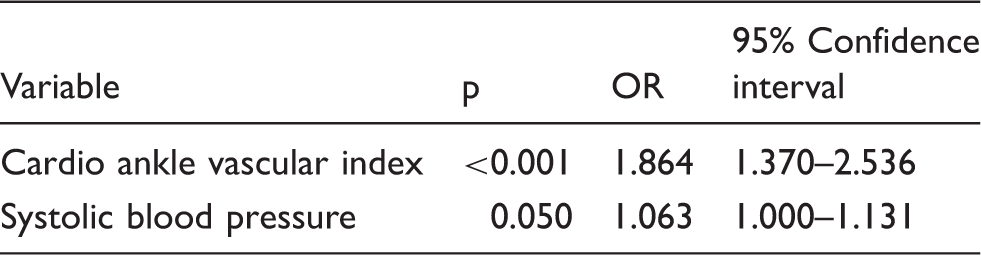
OR: odds ratio.
CAVI value > 7.8 had a sensitivity of 82.7% and a specificity of 80.8% for predicting VTE (area under curve = 0.789, 95%CI = 0.698–0.863, p < 0.001) in ROC analysis (Figure 2).
ROC curve demonstrating the sensitivity and specificity of CAVI for predicting venous thromboembolism. CAVI: cardio-ankle vascular index; ROC: receiver operating characteristic curve.
Discussion
We found that arterial stiffness was independently increased in patients with VTE.
The pathogenesis of VTE is multifactorial, including stasis, endothelial damage to the vessel wall, and thrombogenic tendency.1,2 However, in about one-third of the patients with VTE the cause is unexplained. The role of inflammation in the pathogenesis of VT is established in several studies.2,9 Neutrophilic infiltration of the vessel wall, cytokine, chemokine, and adhesion molecule overexpressions was demonstrated in patients with VTE. 2 Inflammation mediates a key role in the pathogenesis of atherosclerosis and causes an increase in arterial stiffness through deteriorating vascular functions. 10
Atherosclerosis and VTE are evaluated separately. However, cardiovascular events are increased in patients with VTE. Atherosclerosis may be a potential risk factor for VTE or these two distinct pathological conditions are simultaneously triggered by the same biological stimuli that are responsible for activating coagulation and inflammatory pathways in both arterial and venous system. Prevalence of carotid plaques was significantly higher in patients with spontaneous VTE. 11 Atherosclerosis and VTE share some common risk factors including hyperhomocysteinemia, smoking, and obesity. Additionally, Glynn et al. reported that VTE rosuvastatin treatment decreased the prevalence of VTE in the JUPITER trial. 12 This risk reduction appears to be an independent benefit of statin use, beyond the reduction in the risk of arterial thrombosis. We have shown that arterial stiffness is increased in patients with VTE and pleiotropic effects of statins may provide benefit for both recurrence of VTE and development of major adverse cardiovascular events in this patient subset. Additionally, aspirin usage may be considered due to the presence of subclinical organ dysfunction (arterial stiffness) in VTE patients.
Duran et al. studied the endothelial function in patients with VTE by aortic elastic properties and reported that aortic elastic properties were impaired and aortic stiffness was increased in patients with VTE. 13 Aortic distensibility and stiffness examines the proximal ascending aorta therefore reflects the elastic properties of ascending aorta. Aortic elastic properties significantly depend on blood pressure values. Additionally, aortic elastic properties deteriorate in patients with increased left ventricle mass index (LVMI). In their study, LVMI was significantly higher in patients with VTE which may have effected their findings but in our study the LVMI of the patients and controls was similar. We examined patients with CAVI. CAVI differs from other arterial stiffness measurement methods by independence of blood pressure. Furthermore, in contrary to other methods of arterial stiffness measurements including pulse wave velocity, augmentation index, and aortic elastic properties, CAVI is not a regional stiffness parameter instead it reflects the stiffness of whole arterial tree. CAVI is associated with epicardial fat thickness, atherosclerosis, chronic obstructive lung disease, coronary syndrome-x, dipping status, silent neuronal injury, diabetes, aging, chronic renal failure, dyslipidemia, smoking, hypertension, and obstructive sleep apnea.14–19 Additionally, vasoactive medications including alpha-blockers, beta-blockers, angiotensin-converting enzyme inhibitors also alter CAVI. 19 None of our patient used antihypertensive medications in this study. Vascular tree is in continuum. Coronary artery disease is prevalent in patients with peripheral artery disease.20,21 Additionally, arterial disease and coronary artery disease are common in patients with VTE. This may be related to common risk factors and vascular alterations. Furthermore, arterial stiffness is also increased in patients with chronic lower extremity venous disease. 22
Although we excluded patients with hypertension, systolic blood pressure was significantly higher in patients with VTE. This finding is associated with increased arterial stiffness in patients with VTE.
Limitations
This study has several limitations. First, the study scale is small.Biochemical markers associated with endothelial dysfunction and inflammation were not studied in this study. Furthermore, this study was performed in Turkey and may show regional variation.
Conclusion
In conclusion we found that arterial stiffness was increased in patients with VTE which highlights the fact that arterial and venous circulation is in continuum and an insult may affect both of these circuits.
Footnotes
Authors’ contribution
ACA, EH, TG, EK, and CYK researched literature and conceived the study. ACA, EH, TG, EK, and CYK were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. ACA wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical approval
This study was approved by Kartal Koş uyolu Heart Training and Research Hospital ethical committee (2013-012).
Guarantor
ACA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.