
Abstract
Background
High-quality non-invasive imaging of the deep venous system in the thorax is challenging, but nevertheless required for diagnosis of vascular pathology as well as for patient selection and preoperative planning for endovascular procedures.
Purpose
To compare the diagnostic quality of Gadofosveset-enhanced thoracic magnetic resonance venography, seven consecutive patients with suspected or known disease affecting the central thoracic veins were compared to seven consecutive magnetic resonance venography using conventional gadolinium-based contrast agents.
Materials and methods
Diagnostic capability, defined as the ability to assess vessel patency and pathologic conditions, for the major thoracic deep venous segments was assessed by two-independent readers. Both reviewers rated the overall subjective image quality on a four-graded scale, and inter-rater variability was analyzed using unweighted and weighted Cohen's kappa values.
Results
Diagnostic capability was generally considerably higher in the Gadofosveset group for all examined vessel segments. The overall images quality rating was significantly higher for the Gadofosveset group with a mean rating of 2.9 and 2.7 for the two-independent readers, compared to 1.2 and 1.0 for the control croup. Inter-rater variability showed less variability for the Gadofosveset group with a quadratic-weighted Cohen's Kappa value of 0.58 compared to 0.36 for the control group.
Conclusion
Our results show that Gadofosveset-enhanced magnetic resonance venography of the central thoracic veins is a reliable technique in clinical routine practice that results in diagnostic images, superior to conventional gadolinium-based contrast medium.
Keywords
Introduction
Non-invasive imaging of vascular pathology in central veins of the thorax can be performed using magnetic resonance venography (MRV), computed tomography venography (CTV), ultrasound (US) and digital subtraction angiography (DSA). Either US or DSA is the first choice in most centers for diagnosing deep vein thrombosis in the arm, but both techniques have very limited ability to visualize the central thoracic veins, and most centers therefore rely on MRV and CTV for this indication.1,2
MRV of the thorax is challenging because of the continuous movement of the heart and lungs. Sequences during breath-hold are limited to relatively short acquisition time. Sequences during tidal breathing produce artifacts, as does the movement of the heart. Some of these artifacts can be overcome by longer acquisition times using gated sampling. 3 However, the total acquisition time is limited when conventional contrast media are used since they are rapidly transferred from the blood into the extracellular space. Recent time-resolved technique circumvents some of these obstacles but does not generally produce images with sub-mm resolution. 4
With the introduction of endovascular interventions, there is a rising demand for high-quality high-resolution preoperative imaging, crucial for patient selection and preoperative planning for such procedures as catheter-based thrombolysis and recanalization of chronic venous occlusions.5,6
Gadofosveset (Vasovist®, formerly supplied by Bayer Schering Pharma AG, Berlin, Germany and Ablavar®, currently supplied by Lantheus Medical Imaging, North Billerica, ME, USA) is a gadolinium-based contrast agent that remains in the blood longer due to its high affinity to serum albumin. This feature allows longer acquisition time resulting in high-resolution images with fewer artifacts. The blood-pool effect also makes exact timing of the image acquisition less crucial, and the technical success-rate should therefore be high. The high affinity for albumin increases the T1-relaxivity 7 allowing high contrast-to-noise ratio using relatively low amount of gadolinium.
Gadofosveset was rapidly adopted as an angiographic contrast agent for arterial studies.8–14 Some studies have described the use of Gadofosveset for venous examinations of the lower extremities in patients without suspected venous pathology15,16 and in patients with deep vein thrombosis.17,18 Pfeil et al. 19 have showed excellent inter-rater reliability for MRV of the lower extremities on healthy subjects.
Several groups have described the use of Gadofosveset in the thorax20–23 as well as in the heart,24,25 generally with results comparable or superior to other contrast media or imaging modalities. However, these studies have not focused on the thoracic veins, and there are few studies on patients with pathology in the central thoracic veins.
In this report, we analyze our Gadofosveset-enhanced MRV of the thorax. We show that it is a reliable method that results in high-quality high-resolution images superior to those obtained using conventional gadolinium-based contrast media.
Materials and methods
Patients
Patient characteristics (gender, age, bodyweight and primary reason for referral) for the study group and the control group.
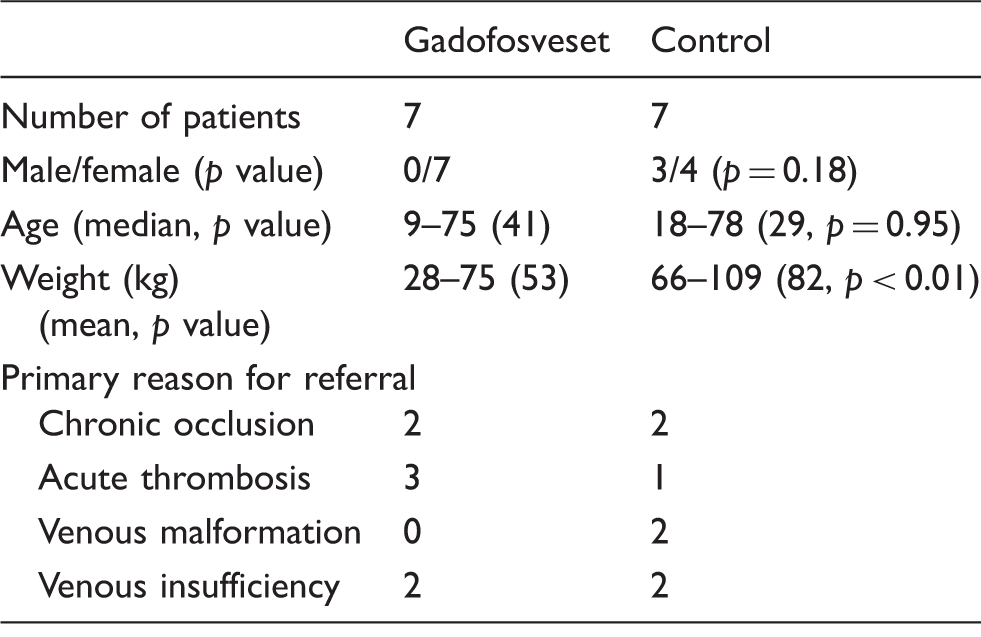
The differences in age and gender between the groups were not significant (two-tailed Mann–Whitney U-test), whereas the difference in bodyweight between the groups was significant.
Magnetic resonance imaging protocol
Because of the long inclusion time the magnetic resonance imaging (MRI) protocol varied slightly, due to upgrades of the different scanners. MRI was performed with different 1.5 T scanners (Symphony (six in the patient group/one control), Symphony Tim (0/5), Avanto (1/0), Sonata Vision (0/1), all from Siemens Healthcare/Medical Solutions, Erlangen, Germany). Matrix coils covering the thorax were used for all patients for signal reception. Angiographic sequences (Fl3D) were used for all examinations. The standard Fl3D sequences recommended by the vendor were used and modified according to the size of the subjects following the practice at the institution. The sequences were performed in coronary projection. In the Gadofosveset group, the slice thickness was 1.1–1.5 mm, TR/TE 2.76–3.63/1.02–1.44 ms, FA 25–26 ms, Number of average 1, Acquisition matrix 384 × 173–273, in one case 256 × 190, resulting in images with row 768 and columns 576–768, in one case 512 and 448, respectively. In the control group, the slice thickness was 1.0–1.4 mm, in one case 0.7 mm, TR/TE 2.9–4.58 ms, FA 25, Number of average 1, Acquisition matrix 256–512 × 77–358, in one case 832 × 682, resulting in images with rows 256–512, and columns 192–512, in one case 832 and 832, respectively.
Images were acquired during tidal breathing at first pass (arterial phase) and after 5 and 10 min (venous phases). Additional sequences such as T1-weighted Turbo Spin Echo (T1 TSE) and Turbo inversion recovery magnitude sequence (TIRM) were not evaluated in this study.
A single dose of 0.11 mL/kg bodyweight Gadofosveset trisodium (Vasovist® 0.25 mmol/mL, Bayer Schering Pharma AG, Berlin, Germany) was administered using a peripheral venous access and a power injector (Spectris Solaris, Medrad, Pittsburgh, USA). Gadofosveset doses ranged from 4.5 to 10.4 mL, with an average dose of 8.7 mL.
For the other contrast agents (Gadovist®, Dotarem® and Multihance®) used in the control population appropriate doses according to the manufacturer's suggestions were administered in a similar way.
Three patients in the control population were administered Gadoteric acid (Dotarem® 279.3 mg/mL; at doses 13, 20 and 20 mL). Three patients were administered Gadubutrol (Gadovist® 604.72 mg/mL; at doses 15, 17 and 17 mL). One patient was administered Gadobenate acid (Multihance® 334 mg/mL; at dose 17 mL).
Image analysis
Images were analyzed in Sectra IDS7 PACS (Sectra Medical Systems, Sweden) by two-independent radiologists (JW and LL). Image settings were adjusted to make identification and image data unavailable during the reading. Assessment was made of diagnostic ability of the images for the major central venous segments in the thorax. Examination was assessed as diagnostic if the segment could be clearly visualized and diagnosed. The diameter of the superior vena cava was measured, and the subjective overall image quality was rated on a four-graded scale ranging from 0 to 3 (0: non-diagnostic, 1: acceptable, 2: good, 3: excellent).
Statistical methods
Data were analyzed using standard statistical methods including Cohen's kappa coefficient (unweighted and quadratic weighting) for inter-reader variability assessment of the image quality index. Mann–Whitney U-test was used to detect significant differences between the study populations. For the weighted kappa analysis, quadratic weighting was used, and the relative distances between all steps were set to 1.
Results
The study population consists of all seven thoracic MRV performed at our hospital from 2006–2010. For comparison, seven consecutive thoracic MRV using other contrast media were used. The differences in age and gender between the groups were not significant (two-tailed Mann–Whitney U-test), but the difference in weight between the groups was significant.
There were no early reactions to the contrast medium or other adverse events related to the examinations according to the RIS-documentation. Serum creatinine was not measured after the examination for the majority of patients, thus making such an analysis impossible. No major technical problems were reported for any of the examinations. No long-term complications related to the contrast media, including nephrogenic systemic fibrosis was seen in any of the patient groups during follow-up. 26
Figure 1 shows examples of the images obtained by Gadofosveset-enhanced MRV.
The figure shows examples of Gadofosveset®-enhanced MRV. All images are taken at steady-state to get maximal enhancement of the veins. Panel A is a MIP-image showing the deep veins of the thorax and upper arms. Panel B is a patient with a thrombotic stenosis of the Superior Caval Vein (arrow). Panel C is showing a patient with extensive occlusive disease in the central thoracic veins, for example, the right Axilliary Vein (arrowheads), and multiple occluded segments including the Anonymous Vein, the left Axillary and Subclavian Veins (gray arrows) and parts of the Superior Caval Vein (arrow).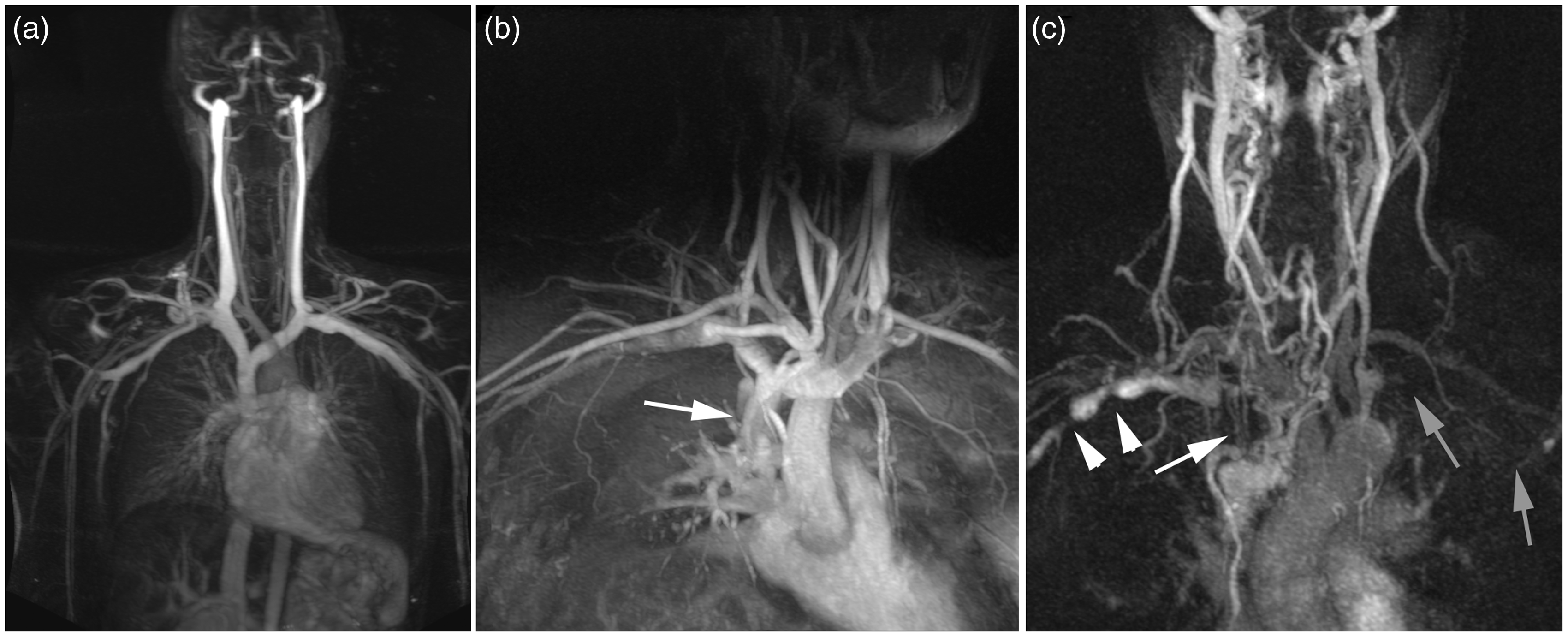
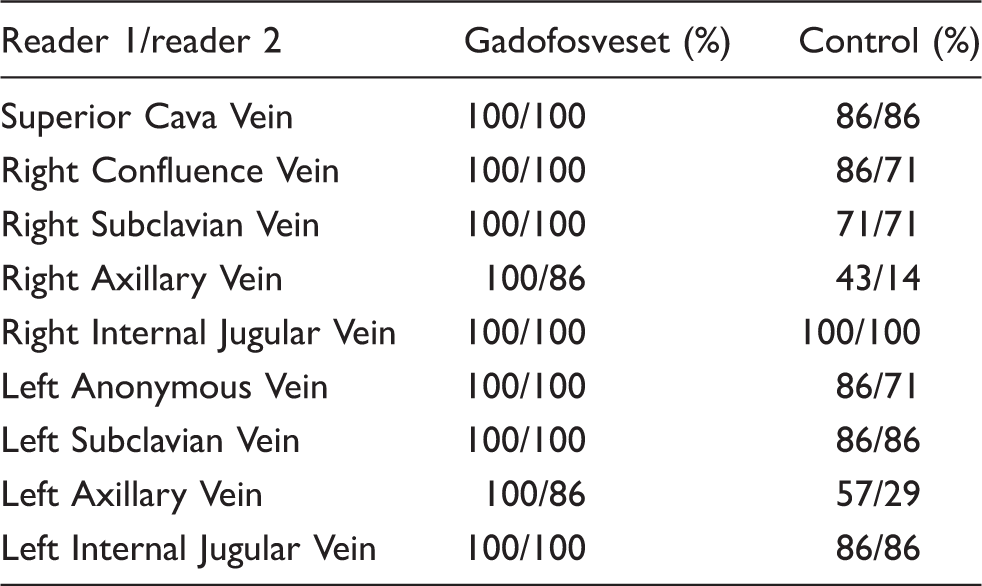
Assessment diagnostic ability, defined as whether or not the examination is diagnostic for the defined vessel segment, for the previously defined vessel segments made by the two-independent readers (reader 1/reader 2).
Subjective image quality score (range and mean) on a four-graded scale (0: non-diagnostic, 1: acceptable, 2: good, 3: excellent) by the two-independent readers (reader 1/reader 2) for the two groups, and inter-reader variability measured by the degree of agreement defined as the degree of identical scores from both readers, and by unweighted and quadratic-weighted Cohen's kappa value.
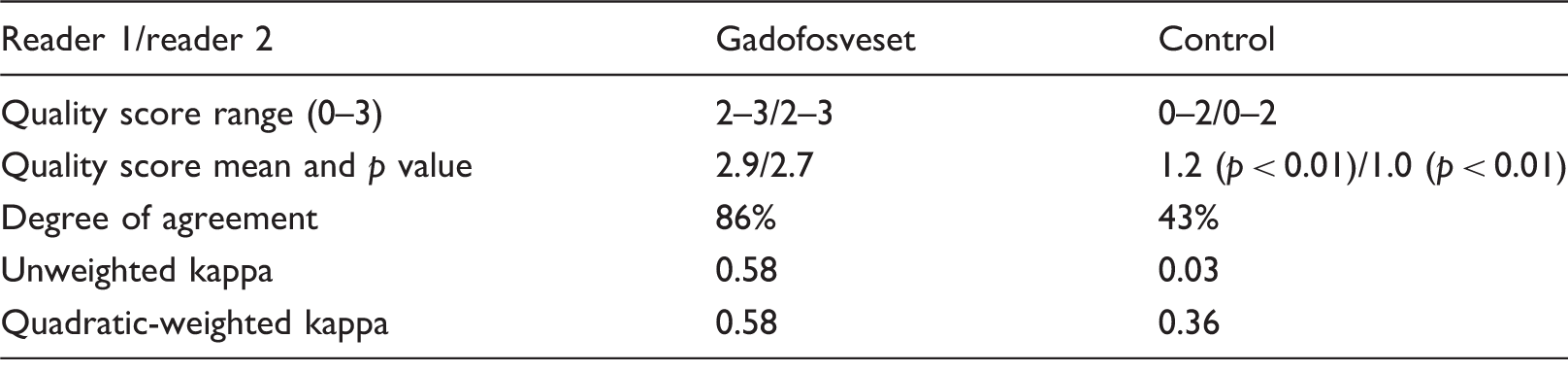
The unweighted and weighted kappa values are identical for the Gadofosveset group since both readers rated all examinations either 2 or 3. The differences in Quality score between the groups were significant for both readers according to two-tailed Mann–Whitney U-test.
The degree of agreement between the readers was higher for the Gadofosveset group (86% identical ratings), compared to the control group (43% identical ratings). Inter-rater reliability as described by Cohen's kappa (unweighted and quadratic-weighted kappa) was 0.58 for the Gadofosveset group. Unweighted kappa for the control group was 0.03 and quadratic-weighted kappa 0.32 suggesting a lower variability for the Gadofosveset group.
Discussion
The study population consists of all Gadofosveset-enhanced MRV of the thorax performed at our hospital, a tertiary university hospital providing care for a population of 1.5 million people, from 2006 to 2010. Consecutive MRV of the thorax using other contrast media was used for comparison. No technical problems or adverse events were noted in any of the study groups.
The small number of patients examined during this period probably in part reflects the difficulties in clinical evaluation, non-invasive imaging, as well as treatment, of the central veins in the thorax. The significant difference in weight between the study group and the control group may influence the outcome, but our impression is that weight is not as important for magnetic resonance (MR) of thorax as for the abdomen. The difference contrast media used in the control group is another possible source of error; however, the pharmacokinetic properties of them are relatively similar. and they all differ from Gadofosveset in a similar way.
The MR-parameters varied due to upgrades of scanners and clinical practice, which is to be expected in a retrospective study. However, the same type of sequence and scanners from the same vendor were used which made the images very similar. Even if it cannot be completely ruled out that differences in spatial resolution might have some impact on the results, the fact that the Gadofosveset group showed a higher robustness with more evaluable segments still stands and shows what would be expected in a varying clinical setting.
The high affinity for albumin makes blood-pool contrast agent suitable angiographic contrast agent, especially for venous examinations, because of the high signal to background ratio and the long-time frame making it possible to obtain high-resolution images. 7 These characteristics also makes the contrast agent relatively easy to use and very forgiving for less experienced MRI operators since the timing between contrast administration and image acquisition is of less importance compared to other gadolinium-based contrast agents. In our data, this is reflected in high overall quality and absence of failed examinations.
Almost all venous segments in the Gadofosveset group were well enhanced and assessed as diagnosable by both reviewers. This differs from the control population where a substantial part of the segments was assessed non-diagnosable. The difference was most pronounced for the axillary veins that are relatively small and located in the thoracic aperture where pulsatile artifacts and breathing artifacts are most pronounced, thereby making these vessels very challenging for imaging. This is probably due to the relatively high T1-signal of Gadofosveset, and to the blood-pool effect that allow longer acquisition time and thus high spatial resolution images as well as less uptake by surrounding tissues.
The difference in image quality score between the groups is considerable and highly significant even though it is based on a relatively small number of examinations. The Gadofosveset MRV was all rated good or excellent by both reviewers (2 or 3) with a mean score of 2.9 and 2.7 by the reviewers, respectively. The rating for the control population ranged between 0 and 2 by both reviewers with a mean score of 1.2 and 1.0 by the two reviewers, respectively.
The reliably high image quality of the Gadofosveset MRV is further supported by the result of the inter-reader variability analysis. Cohen's weighted kappa was 0.58 for the Gadofosveset group compared to 0.32 for the control group and degree of agreement of 86% for the Gadofosveset group compared to 46% for the control population. Although these results are based on a small patient material, it suggests that Gadofosveset is more reliable and produce diagnostic images of significantly higher quality than conventional gadolinium-based contrast agents.
It is possible for all MRV to obtain a first-pass (arterial) dataset that can be subtracted from the late (venous, or steady-state) dataset to produce images where the contrast in the arteries is subtracted; however, such subtraction may also induce artifacts and in our experience it is more advantageous to assess the venous pathology on unsubtracted images.
The majority of reports on Gadofosveset are describing arterial angiographies,8–14 also for the studies of the thorax20–23 and the heart.24,25 In all these reports, Gadofosveset has proven comparable or superior to other contrast media, due to the blood-pool effect. The blood-pool effect is probably even more useful for venography and especially so in the thorax where the continuous movement of the heart as well as respiratory artifacts makes MRV very challenging. This is therefore, in our mind, a good application for blood-pool agents.
In this report, we show that Gadofosveset provides high-resolution MRV in clinical routine practice with a good success-rate and good quality.
Footnotes
Authors' contributions
MÅ, PÅ and JW designed the study. MÅ, LL and JW performed data acquisition. MÅ, JW, PH and PÅ performed data analysis including statistical analysis. All authors read and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.