
Abstract

Station A: Superficial Venous Ablation
PAPER A1
A novel surgical technique for deep venous reflux suppression in femoral vein duplication
Vascular Diseases Center and Unit of Translational Surgery, University of Ferrara, Ferrara, Italy
Background
Femoral Vein (FV) duplication is a higher prevalent anatomical variant than what generally thought, being present in up to 55% of cases.
In primary and post-thrombotic reflux patterns the duplication feeds a closed circuit where an incompetent vessel constitutes the leaking point, while the other conduit represents the anterograde draining route.
Objective
To evaluate feasibility and effectiveness of a simple technique for managing deep venous reflux in case of FV duplication, consisting in the surgical closure of the leaking point.
Methods
The technique was initially tested on five patients, aged 59 ± 4, 3 males and 2 females. They all signed an informed consent form. An indication for surgery was given in presence of a venous leg ulcer older than 6 months, not healing, in stall (mean ulcer onset: 9 ± 2 months). Three patients were C6EsAdPr, and two C6EpAs-dPr. They underwent to echo-color-Doppler (ECD) assessment of deep venous reflux along the accessory femoral vein (AFV), with the leaking point at the vessel bifurcation with the FV. Better anatomical detail was preoperatively obtained by the means of MRV.
The technique consists in closing the refluxing femoral branch by a titanium clip. All the procedures were performed in Day Surgery.
Results
The technique is feasible and associated with improvement of limb haemodynamics. At 1 year follow up, clinical evaluation demonstrated a significant improvement of the venous clinical severity score from 20.4 ± 1.3 to 10.2 ± 2.6 (p < 0.0004). Three cases had complete ulcer healing, while the other 2 reduced their size by more than 50%. The ECD scan revealed in the iliac-femoral segment the resolution of the previous reflux, as a consequence of the interruption of the insufficient hydrostatic column. Moreover, the ECD investigation of the AFV below the interruption demonstrated the typical retrograde but not refluxing drainage toward the competent FV.
Air-plethysmography was performed in 3 of the 5 cases operated on. The treatment proposed herein led to a significant improvement in venous refilling time, venous volume and residual volume fraction. The ejection fraction remained unchanged.
Neither major nor minor complications were reported in any of the 5 cases.
Conclusions
The lower limb deep venous system constitutes one of the most fascinating but challenging topics in vascular surgery. Nowadays, therapeutic options such as valvuloplasty, transpositions and translocations are used in a limited number of cases and just in highly specialized Centres. The technique herein proposed, thanks to the high prevalence of FV duplication, gives the chance to treat a wider number of cases affected by primary or post-thrombotic deep venous reflux.
PAPER A2
How do we prevent tributary vein recurrence near the sapheno-femoral junction after endovenous ablation of the great saphenous vein
Matsusaka Ohta Clinic, Matsusaka, Japan
Background
Since being approved for health insurance coverage in Japan, endovascular ablation (EA) has become widely used for the treatment of primary leg varicose veins, an area in which it has made a major contribution. A few in-depth studies have examined long-term postoperative follow-up, but a higher incidence of tributary vein recurrence (TVR) after EA of the great saphenous vein (GSV) without high ligation (HL) was noted in some papers. From my experience with the surgical treatment of recurrent varices after surgery (REVAS), to prevent TVR, I considered that the view around the sapheno-femoral junction (SFJ) may not be suited to EA without HL, and HL + EA or stripping (S) may be better.
Patients and Methods
REVAS (after HL + S) that originated near the SFJ was surgically treated in 16 limbs (1.0% of all varicose vein surgeries) between January 2008 and June 2015, and the cases were divided into 12 TVRs and 4 neovascularizations (NVs). In 9 TVRs (75%) and 4 NVs (100%), tributary varicose veins in the thigh were found before the first surgery. In 10 TVRs (83%), the tributary veins connected within 1.5 cm from the SFJ, which could be a cause of REVAS if EA without HL were conducted. Based on these results, the treatment strategy for GSV reflux was decided based on the appearance of the SFJ (aneurysmal change, severe destruction of the terminal valve) and tributary veins (aneurysmal change, dilatation, and reflux which connect within 1.5 cm from SFJ) and on the patient’s general condition (obesity, anticoagulants, anti-platelet agents), and 318 GSV- radiofrequency ablation (RFA) candidates were divided into 275 EA without HL, 11 HL + retrograde EA, and 32 HL + S between September 2014 and December 2015. Tributary varicose veins and tributary veins with reflux in the thighs were resected in all limbs in which HL was performed.
Results
TVR and NV have not been observed in these 3 groups so far, though this is only the early result. In 275 limbs in the RFA without HL group, 251 (91%) limbs had tributary veins without reflux, whereas reflux of tributary veins was found in only one limb of this group.
Conclusion
Although this was a preliminary trial, this approach to preoperative classification would be effective for preventing tributary vein recurrence from the SFJ. Further discussion of the type of patients for whom HL + EA or S rather than EA without HL should be chosen is needed, and further long-term follow-up regarding recurrence is also required.
PAPER A3
Risk factors of endo-venous heat induced thrombosis after endo-venous laser ablation
Chiba Clinic for Varicose Veins, Chiba, Japan
Objective
Since endo-venous heat-induced thrombosis (EHIT) is decreasing and seldom inducing severe outcomes, the necessity of post-operative ultrasound evaluations is somewhat questioned. But, it may still cause venous thromboembolism. This study is to evaluate the incidence of heat-induced thrombosis and risk factors that may contribute to its formation after endo-venous laser ablation.
Methods
From September 2015 through January 2016, 281 endo-venous laser ablations were performed by single surgeon. 240 cases were done by 1470 nm laser with two-ring radial fibers, and 41 cases were done by 980 nm laser with bear-tip fibers. Ablation starting points were same for all cases. Type of laser, age, gender, operation time, linear endo-venous energy density, conditions about phlebectomy, and diameter of saphenous veins were analyzed. Duplex ultrasound was done for all patients preoperatively, and 1-3 days, 2-3 weeks, and 2-3 months after operations.
Results
No operative mortality was recorded. No class 3 or 4 EHIT, deep vein thrombosis, or pulmonary emboli occurred. The incidence of EHIT class 2 was 2.8 % (8 cases) and class 1 was 3.6 % (10 cases). By comparing groups with class 1 or 2 EHIT and without EHIT using student t-test, mean age was 74.0 ± 7.5 years old and 65.6 ± 12.3 (p = 0.0002), mean operation time was 47.1 ± 18.7 minutes and 36.0 ± 16.5 (p = 0.024). By comparing groups with class 2 EHIT and without class 2 EHIT (no EHIT or class 1 EHIT), mean age was 77.4 ± 7.5 years old and 65.8 ± 12.2 (p = 0.0029), mean operation time was 48.9 ± 22.0 minutes and 36.3 ± 16.6 (p = 0.152). Using Fisher’s exact test, class 2 EHIT was found with 5 patients (2.1%) in 1470 nm laser group and with 3 patients (7.3%) in 980 nm laser group (p = 0.096). Age and operation time were significant risk factors for EHIT. Using 980 nm laser showed a tendency to make more severe EHIT compared by using 1470 nm laser. In this study, other factors did not show any significant differences between the groups with EHIT and without EHIT, or between the groups with class 2 EHIT and with no or class 1 EHIT.
Conclusions
The older age and longer operation time could be the associated risk factors for EHIT. The usage of 980 nm laser showed a possibility to produce more severe EHIT than 1470 nm laser. Additional studies are required to analyze these and other factors that may predict EHIT.
PAPER A4
Edoxaban in the prevention of endovenous heat-induced thrombosis after endovenous laser ablation for varicose veins
1Department of Cardiovascular Surgery, Nagano Matsushiro General Hospital, Nagano, Japan
2Department of Clinical Laboratory and Pathology, Nagano Matsushiro General Hospital, Nagano, Japan
Objectives
Endovenous heat-induced thrombosis (EHIT) or deep vein thrombosis (DVT) is well recognized as a complication of endovenous laser ablation (EVLA) for varicose veins. The aim of this study was to evaluate the efficacy of edoxaban, an oral factor Xa inhibitor, for the prevention of EHIT or DVT after EVLA.
Methods
We reviewed 326 limbs in 304 patients undergoing EVLA (980-nm diode laser) between April 2013 and December 2015. Duplex ultrasound scanning was performed one day after EVLA. EHIT was classified into 5 classes; class 0: thrombus below junction, class 1: thrombus extending flush with junction, class 2: thrombus extending beyond junction with cross-sectional diameter of < 50%, class 3: thrombus extending beyond junction with cross-sectional diameter of > 50%, class 4: totally occlusive DVT. EHIT class 0 was followed up without anticoagulation (group A). EHIT class 1 was divided into two subgroups (group B); the EHIT was treated with edoxaban (edoxaban group), the EHIT was followed up without anticoagulation (control group). EHIT class 2 or 3 was treated with anticoagulation (group C). Patients were evaluated clinically and by ultrasound at 1 week, 1, 3, 6, and 12 months after EVLA.
Results
In the group A (259 limbs), the EHIT class significantly (p < 0.001) increased at one week (class 0 in 250, class 1 in 26 , class 2 in 12 and 3 class in 1 limb) after EVLA. In the group B (29 limbs), the median EHIT class at one week was significantly (p = 0.003) lower in the edoxaban group (11 limbs, class 1.5) than in the control subgroup (18 limbs, class 0). The incidence of EHIT class 2 or greater was lower in the edoxaban group than in the control group (0.9% vs 50%, p = 0.0426). The pain level and the bruising level at one week after EVLA did not differ between the groups. In group C (8 limbs), EHIT was treated with edoxaban in 4, warfarin in 2, others in 2 limbs. EHIT class 2 or 3 after one week was also treated with edoxaban or other oral anticoagulants. The EHIT class 2 or 3 resolved by 1 month in all limbs. No EHIT class 4 or DVT was detected after EVLA. No recanalization was observed in the limbs treated with edoxaban.
Conclusions
These data suggest that EHIT progression in one week is common after EVLA and edoxaban can control the progression of EHIT early postoperatively. Edoxaban may be beneficial in the prevention of EHIT or DVT after EVLA.
PAPER A5
Evaluation for occlusion rate of a great saphenous vein and its tributaries by ultrasound scan after varicose veins treatment with radiofrequency ablation
Department of Vascular Surgery, Nishinokyo Hospital, Nara, Japan
Introduction
We evaluated for occlusion rate of a great saphenous vein (GSV) and its tributaries by ultrasound scan after varicose veins treatment with Radiofrequency Ablation (RFA).
Subject and Methods
The subject of this study is 300 treated cases (average age 65.5 ± 11.6 years / 90 males and 210 females) using Endovenous Closure™ from May to November 2015. In all cases, the catheter tip was positioned 15 mm from the SFJ. On the next day of surgery ultrasound scan was performed for evaluation.
Results
After RFA, the distance from SFJ to the occlusion was 13.8 ± 6.8 mm on the average. The occlusion rate of main trunk of GSV was 100%. As for tributaries, the cases which the blood flow was found were regarded as positive. The cases which became occluded and which was not able to identify itself were regarded as negative. The average number of tributaries was 0.62 ± 0.63 which the blood flow was found. The breakdown is as follows: 0:139cases/1:137cases /2:24cases /3:0cases /4:0cases.
Discussion
It is considered that occlusion rate of tributaries is affected by the catheter tip position, shape of GSV around starting point for ablation and the positional relationships among tributaries. Therefore, the preoperative confirmation (evaluation) by ultrasound scan for SFJ is considered very important.
PAPER A6
Pilot study of the use of cyanoacrylate in the treatment of varicose veins
Section of Vascular Surgery, Imperial College London, Charing Cross Hospital, London, UK
Background
The treatment of varicose vein disease has changed significantly over the past decade. Endovenous ablation, especially using thermal methods, has become the new norm. However, it is often associated with patient discomfort during tumescent infiltration and the ablative procedure. The non-thermal, non-tumescent (NTNT) techniques are believed to be more advantageous as they eliminate these potential adverse events. In this study, the use of a new cyanoacrylate compound (Variclose vein sealing system, Biolas®, Ankara, Turkey) for the treatment of varicose vein disease is assessed.
Method
Patients with symptomatic varicose veins were invited to have their truncal saphenous incompetence treated using the new cyanoacrylate glue. Intraoperatively, their level of discomfort was assessed using a visual analogue scale (VAS) and categorical scale. Patients also had their clinical status (using VCSS) and quality of life (EQ-VAS, EQ-5D, AVVQ and CIVIQ-14) assessed at baseline and post-operative at 1 month as well as duplex scan at one month.
Results
Eighteen patients were recruited, eleven (61%) were females and the mean age was 52 years (range: 28 to 91 years). The mean maximum pain score using the VAS was 36.8 mm (standard deviation: ± 8 mm) and 4.2 ( ± 0.8) on the categorical number scale. The mean average discomfort was 26.8 ± 6 mm (VAS) and 3.2 ± 0.6 (categorical number scale). There was a marginal improvement in the clinical scores (VCSS improving from 3.5 to 3.4). Improvements were also noted in the generic quality of life scores (+3.9 in the EQ-VAS and + 0.012 in the EQ-3D). The AVVQ improved from 16.6 to 10.3 (-6.3) and CIVIQ-14 (from 31.4 to 20.0; -11.4). All veins were occluded at the end of the procedure, but to date at the one month follow-up, one of the veins had opened up (this patient was on long-term anti-coagulation which was not stopped peri-operatively). There were no serious adverse effects.
Conclusions
These preliminary results suggest that endovenous ablation using cyanoacrylate was safe and results in what appears promising improvement in quality of life similar to that seen in studies evaluating thermal techniques along with a low degree of intra-operative pain. Larger comparative studies are, however, required to confirm its effectiveness.
PAPER A7
A more comfortable method for tumescent anesthesia
Vein Therapies of Chattanooga, Chattanooga, Tennessee, USA
Some papers have described significant patient discomfort with current methods of tumescent anesthesia. We describe our method which usually only requires three 27 gauge skin wheals through which the rest of the anesthesia is delivered.
The initial injection site is at the proposed catheter introducer site, which is normally near the proximal calf (C). After the guide wire is introduced, another skin wheal is made at the distal thigh (DT) and at the proximal thigh (PT). After the catheter is introduced and positioned, chilled tumescent anesthesia is placed around the catheter in both a proximal and distal direction from the previously placed skin wheals in the thigh (DT and PT) and proximally from the calf skin wheal (C) using either a 5 inch spinal needle or a special blunt tipped trocar with side discharge openings. This normally requires 5 or 10 minutes. Proximal temperature at the saphenofemoral junction is usually recorded at 20°C (using the radiofrequency catheter).
This method significantly reduces patient discomfort and requires no additional time than the standard method of tumescent anesthesia delivery, which uses multiple needle sticks with the spinal needle and only in the proximal direction.
We have had excellent patient satisfaction in over 2000 cases.
PAPER A8
Clinical trial comparing endovenous radiofrequency thermal ablation and crossectomy with stripping for great saphenous varicose veins
Scientific Centre of Surgery named after M.A. Topchubashov, Azerbaijan Medical University, Baku, Azerbaijan
Purpose
Endovenous radiofrequency thermal ablation (ERFA) have comparable efficacy to surgery, but was associated with an earlier return to normal activity and improved quality of life. The aim: analysis of treatment results in patients with lower limb varicose disease (LLVD) according to a comparative study of short-term (<1 year) outcomes of VNUS Closure FAST™ ERFA and crossectomy with stripping of great saphenous vein (GSV).
Methods
157 patients with LLVD (C2-C6) were under observation. Basic group was introduced by ERFA in 82 patients (139 limbs), 19(23.2%) males, 63(76.8%) females (aged 20-75 years). Diameter of GSV-7.9 ± 1.7 mm. C2-9(6.5%), C3-41(29.5%), C4-58(41.7%), C5-14(10.1%), C6-17(12.2%). Coronary heart disease (CHD) was noted in 4(4.9%), arterial hypertension (AH)-22(26.8%), diabetes mellitus (DM)-6(9.8%), obesity-10(12.2%), peripheral arterial disease (PAD)-4(4.9%) patients. Tumescent anesthesia was used in 100%. Control group (75 patients-94 limbs) was performed by crossectomy, stripping of GSV, ligation of incompetent perforating veins (ICPVs) by spinal anesthesia. 23(30.7%) males and 52(69.3%) females (aged 18-69 years). C2-8(8.5%), C3-30(31.9%), C4-46(48.9%), C5-6(6.4%), C6-4(4.3%). CHD-4(5.3%), AH-10(13.3%), DM-7(9.3%), obesity-3(4%) PAD-2(2.8%) cases. Quality of life determined by the Aberdeen Varicose Vein Severity Score (AVVSS), clinical improvement - by Venous Clinical Severity Score (VCSS).
Results
Comparison of results show more regression of chronic venous disease attributes (edema, skin changes, ulcers) in ERFA group: 94% vers. 62% (p < 0.05). Return to habitual activity: ERFA-1.0 ± 1.6, crossectomy with stripping-7.4 ± 1.8 days. In basic group the average pre-procedure VVCS was 7.8 ± 2.6 (range 2-18), AVVSS-23.1 ± 6.2 (range 10-48), in control-7.2 ± 2.5 (range 2-16) and 22.7 ± 6.4 (range 11-44) resp., post-procedure decrease (during 1 year) was 0.28 ± 0.64 vers. 1.1 ± 0.44 and 3.1 ± 2.2 vers. 5.7 ± 1.8 resp. (p < 0.05). Pain scores on visual analogue scale (on 0 to 100 mm) for first 14 days after treatment show the best dynamics of pain decrease in ERFA group: 100% vers. 62% (p < 0.01). Complications in basic and control group: neuritis-0% vers. 4.4%, infection-0% vers. 7.1%, inguinal neovascularization-0% vers. 5.6%, deep vein thrombosis-0% vers. 2.4%, skin burn-1.4% vers. 0%, paresthesia-4.9% vers. 13.2%, skin pigmentation-5,4% vers. 14.2%, hematoma-0% vers. 11.1%. GSV ablation with reduction of ICPVs in basic and control group: 96% vers. 78% resp. (p < 0.05).
Conclusion
ERFA in comparision crossectomy with stripping of GSV demonstrated early return to habitual activity on 1-2 day, painless post-procedure period, regression of CVI symptoms, improvement of life quality and better cosmetic effect.
Station A: Winner of best ePresentation
PAPER A9
Sclerotherapy and vein gluing combined as a single procedure for saphenous veins
Aangioclinic® vein centers - Interventional Phlebology, Berlin - Munich, Germany – Zurich, Switzerland
Background
Gluing of veins is discussed as being superior to thermo-occlusive methods or sclerotherapy. However, approved gluing methods use continuous placement of larger amounts of aggressive and hardly resorbable cyanoacrylate (VenaSeal, VariClose). The effect depends on external manual compression. These drawbacks could be overcome by a new modality which combines pointwise gluing and catheter sclerotherapy (ScleroGlue® project).
Materials and Methods
18 patients (11f, 7 m, 42 – 69 y) with GSV insufficiency and diameters of 8 - 24 mm Ø (mean: 9.4 mm) underwent combined sclerotherapy (Aethoxysklerol 1%, 1 + 4 with air) and gluing, using a double catheter access including the VariClose gluing system (Biolas Inc.). Besides the GSV, auxiliary associated targets (refluxive side branches > 6 mm Ø, n = 22, and perforator veins < 6 mm Ø, n = 12) were included in the treatment plan. First sclerofoam was applied with a PTFE catheter (PhleboCath, 1.9/2.3 mm Ø) during withdrawal and then cyanoacrylate glue was injected during the spasm phase of the target vein while continuously withdrawing the gluing catheter (1.2/1.6 mm Ø). No manual compression was applied. There were no external compression media (stockings, bandages) used after the treatment.
Results
All cases (18/18) showed immediate saphenous occlusion and elimination of reflux. All auxiliary targets (34/34) were successfully reached by microfoam and occluded. The amount of glue used for saphenous veins was 10 - 33 mg (mean: 19.7 mg) per cm vein. Procedural time from first puncture to patient mobilization was 12 – 23 min. (mean: 16.5).
Conclusions
The ScleroGlue® method seems to provide reliable denaturation and effective GSV gluing, achieved without any external compression and using low quantities of glue. The procedure is very fast and requires no anesthesia except for the puncture site. Further studies will be performed 2016 with non-acrylate glues.
PAPER A10
Endovenous laser treatment with 940 nm: estimation of efficiency for ablation of saphenous veins
Azerbaijan Medical University, Scientific Centre of Surgery named after M.A. Topchubashov, Baku, Azerbaijan
Purpose
In the last decade, minimally invasive techniques, such as endovenous laser ablation (EVLA), radiofrequency ablation, and ultrasound guided foam sclerotherapy displayed noteworthy features including shortening hospitalization, early ambulant activity, and excellent cosmetic results. EVLA is an improved method to treat varicose great (GSV) and small saphenous veins (SSV) with a high satisfactory rate. The aim: to examine the effectiveness and feasibility of EVLA in patients with lower limb varicose disease.
Methods
461 patients (543 limbs) with lower limb varicose disease (LLVD), including primary and secondary (after deep vein thrombosis-DVT) varices, treated with EVLA (940 nm) were retrospectively studied. There were 376(81.6%) females and 85(18.4%) males (aged from 21 to 83, median-43.6 ± 15.5 years). C2-C3 was noted in 367(79.6%), C4-C6 was observed in 94(20.4%) cases. EVLA of GSV was used in all patients (100%), SSV- in 72(15.6%) persons. EVLA of incompetent perforating veins (ICPVs) was used in 76 cases (above knee-4, below knee-72) at 53(11.5%) patients. EVLA with foam sclerotherapy of incompetent varicose inflows by ultrasound controlled was used in 96 cases. Clinical improvement was determined by Venous Clinical Severity Score (VCSS).
Results
GSV and SSV ablation with reduction of ICPVs up to 3 years period were observed in 532(98.0%) limbs. There were 11(2.0%) cases of proximal GSV recanalization, including partial recanalization in 8(1.5%) and full recanalization in 3(0,5%) legs, which were successfully treated by re-EVLA and sclerotherapy. The cause of GSV recanalization was the development of obesity and incorrect use of compression bandaging. Complications: paresthesia-4.9%, skin pigmentation-5.6%, paravasal hematoma-4,5%, skin burn-0.6%. There were no cases of DVT and pulmonary embolism. The average VCSS score was 3.6 ± 1.2 at 3 days, 2.1 ± 1.6 at 3 months, 1.2 ± 1.8 at 6 months, 0.9 ± 1.2 at 12 months compared with 5.2 ± 2.0 preoperatively.
Conclusion
EVLA (940 nm) procedure has high immediate technical success, a short recovery time, and good cosmetic results. EVLA is an efficient treatment method for the treatment of the varicose GSV and SSV, achieving good short-term and long-term results, improves quality of life in patients with lower limb varicose disease.
PAPER A11
The new steam ablation of saphenous vein
Department of Peripheral Vascular Surgery, Ankara University, Ankara, Turkey
Background
Cosmetically better, less invasive and more successful minimal invasive treatment are essential in the treatment of varicose veins. Nowadays, endovenous Laser and RF are most commonly preferred thermal ablation treatment for incompetent saphenous veins. The steam ablation is a new thermal ablation method and it works by heating the vein wall with steam of 120 celcius.
Objective
The aim of this study was to analyse the clinical results of the steam ablation in patients with saphenous vein insufficiency.
Patients and methods
Since February 2013 to January 2016, forty-eight endovenous steam ablation procedures were performed in patients with incompetent saphenous vein (23-80 years old, 21female and 9 male, C2-4EpAsPr, 43VSM, 4VSP, 1Accessory S). The technique of steam ablation(CERMAVEIN, France) is the same as Laser and RF ablation. After cannulation of the GSV, the steam ablation catheter is positioned 2-3 cm distally from the SFJ. Ultrasound-guided tumescent anesthesia was applied along the length of GSV to reduce the pain, to cool the peri-venous tissues and to decrease the vein diameter. The steam dose delivered to the vein is 3-5/pulses per centimeter as the catheter is withdrawn in 1 centimeter increments. Before and after steam ablation, venous clinical severity score (VCSS) and Quality of life (QoL) assessment were recorded. All data of patients has been collected prospectively. Outcomes were studied retrospectively.
Results
Fortynine steam ablation procedures were successfully completed in thirty patient. All veins were obliterated with steam at the postoperative first day and one month follow-up. VCSS and QoL assessment improved from 3.81 to 0.27 and from 42 to 22, respectively, at the one month follow-up. No relevant complication except minimal brusing and one entry point burn were reported.
Conclusion
The new endovenous steam ablation is an effective and safe thermal ablation technique in the treatment of saphenous vein.
Station B: Superficial Venous Ablation, Lymphoedema, Perforators, Deep Venous, Other
PAPER B1
Prediction of radiofrequency ablation treatment outcome using plethysmography in great saphenous vein insufficiency
1Department of Thoracic and Vascular Surgery and Department of Medical and Health Sciences, Linköping University, Linköping, Sweden
2Department of Medical and Health Sciences, Linköping University, Linköping, Sweden
3Department of Clinical Physiology and Department of Medical and Health Sciences, Linköping University, Linköping, Sweden
Objectives
To evaluate whether the outcome of radiofrequency ablation treatment of great saphenous vein insufficiency may be predicted using strain-gauge plethysmography with selective occlusion of the superficial venous system.
Design
Experimental study
Materials and methods
17 patients (20 limbs) underwent endovenous radiofrequency ablation treatment for great saphenous vein insufficiency (C in CEAP, C2 - C5). Colour duplex (CDU) and strain-gauge plethysmography were performed with selective occlusion of superficial veins below the knee before and after radiofrequency ablation. Selective occlusion was validated in a control group (C-group) of 12 patients (14 legs) with ascending phlebography. In the radiofrequency ablation group time to reach 50% and 90% (T50, T90) of complete venous restitution was measured as well as relative maximal reflux rates (%EV/min). The methodological error and coefficient of variation (CV) were assessed.
Results
19 of 20 legs had complete postoperative obliteration using CDU and refilling times were improved after RFA (T50 11 ± 3 vs. 19 ± 3 sec, P < 0.0001; T90 27 ± 5 vs. 47 ± 6 sec, P < 0.001). The methodological error as well as CV for T50 was 4 sec and 16 % respectively.
With SGP, equivalence between preoperative superficial occlusion and postoperative baseline measurements was achieved in 15 of 17 legs for T50 and 12 of 17 for T90 (one leg excluded due to treatment failure and two due to remaining perforating veins). Mean differences (95% CI) were within the equivalence ranges (T50 1 (-1 to3) sec; T90 -3 (-11 to 4 sec)). In the C-group superficial vein occlusion was possible in 12 of 14 legs. The remaining patient (2 legs) had incomplete occlusion at the ankle level (lipodermatosclerosis) and complete occlusion at calf level.
Conclusions
Strain-gauge plethysmography with standardized superficial venous occlusion seems to be a reliable method for identifying venous reflux. It may be useful to predict results of successful radiofrequency ablation treatment.
PAPER B2
Isolated EVLA as a first stage treatment of varicose veins
Dr. Maurins Vein Clinic, Riga, Latvia
Aim
To demonstrate the outcome and side effects after isolated endovenous laser ablation (EVLA) of refluxing great saphenous vein (GSV) with a 1470 nm diode laser (Ceralas E 1470 nm, biolitec) and the 2ring radial fiber (ELVeS Radial 2ring™, biolitec).
Methods
Between November 2011 and March 2013, 150 legs in 150 consecutive patients where treated by EVLA for GSV incompetence using a 2ring radial fiber. All patients were randomized into 3 groups. Group A had no postoperative compression. Group B used postoperative compression with a thigh-length graduated compression stocking (23 - 32 mmHg) for 7 days and Group C used the same kind of stocking for 28 days postoperatively. Investigations where performed clinically and by duplex ultrasound by an experienced phlebologist prior to intervention (Screening visit), day of intervention (D0) and at follow-up visits at day 7 (D7) and 28 (D28) after the procedure for side effects, complications and occlusion.
Results
At day 28 4 patients were lost to follow-up, 2 in group A and 2 in group B. All GSVs showed complete occlusion without early recurrence of reflux within 28 days. The pain score in group A reduced from 1.4 on the day of the intervention to a mean of 0.9 at days 1-7 and to 0.5 at days 8-28. In group B and C the corresponding values were 1.0, 0.4, 0.4 and 1.5, 0.6, 0.4. The difference between groups A and B for D1-7 was significant (p = 0.009). The resolution of varicose vein tributaries without additional treatment was observed 76%, 69% and 88% in groups A to C. No significant differences between the groups appeared for return to normal activity, return to work, satisfaction with the treatment, leg circumference and for the improvement in VCSS and Villalta scales.
Conclusions
EVLA of GSV with a radially emitting 2ring laser fiber using a 1470 nm diode laser is a safe and efficient treatment option. In comparison with other studies using a bare fiber and lower wavelengths postoperative pain and ecchymoses are reduced. Wearing a compression stocking after the procedure only slightly reduces pain within the first week and couldn’t be obligatory. Isolated EVLA as the first stage of treatment lowers operation trauma, possible postoperative complications and restrictions. Two staged strategy for varicose vein treatment can be recommended.
PAPER B3
Early outcomes after radiofrequency ablation and mechanochemical ablation in the treatment of great saphenous vein incompetence
Hull York Medical School, Hull Royal Infirmary, Hull, UK
Objective
Thermal ablation treatment of varicose veins has become the first line treatment for superficial venous insufficiency. Newer, non-thermal ablation treatments have potential benefits for patient acceptability and decreased risk of heat-related complications, including peri-procedural pain and nerve injury. This study evaluated intra-procedural and post-procedural pain and quality of life after radiofrequency ablation (RFA) and mechanochemical ablation (MOCA) for great saphenous vein (GSV) incompetence.
Methods
Fifty-two patients with unilateral GSV incompetence were treated with either RFA or MOCA in this prospective observational study. Pain experienced during the procedure and for the first 7 post-procedural days was recorded on a 100 mm validated visual analogue scale (VAS). Clinical assessment was measured by clinical-etiology-anatomy-pathophysiology (CEAP) class and venous clinical severity score (VCSS). Patients had duplex ultrasound assessment of the leg and also completed general (Short Form 36, EuroQol) and disease-specific (Aberdeen Varicose Vein Questionnaire) quality of life questionnaires before and at 1, 6 weeks after treatment.
Results
52 patients were treated, 26 in each group, and all completed their 6-week follow-up. There were no significant differences between the groups regarding demographic data, CEAP classification, preoperative VCSS, and initial AVVQ. Patients treated with MOCA reported significantly less intra-procedural pain than patients treated with RFA (25.3 ± 18.6 mm vs 38.3 ± 25.8 mm; p = 0.04). At each of the first 3 post-procedural days, the difference between the groups was statistically significant. There was no significant difference between groups for return to normal activities (RFA median 2, IQR 1-7 vs MOCA median 3, IQR 1-7, p = 0.8). At 6 weeks, patients in both groups perceived an improved change in health status and disease-specific quality of life, and technically showed similar occlusion rates.
Conclusions
MOCA is associated with significantly less intra-procedural and post-procedural pain compared with RFA in the treatment of GSV incompetence. Both MOCA and RFA are related to improvement in clinical severity and general and disease-specific quality of life
PAPER B4
Surgical procedure for incompetent perforators – VANST technique
FLEBESTET Medical Clinic, Bucharest, Romania
Background
There are different options for the approach of the reflux at the insufficient perforating veins level: endovenous treatment, SEPS, the CHIVA approach, surgery.
In our opinion the treatment of the insufficient perforators must interrupt the venous reflux (by closing up the perforating veins).
The purpose of this paper is to present VANST technique for the treatment of the insufficient perforators. There are a few complex morphologic aspects of the perforating veins that can generate difficulties in applying the treatment and avoid recurrency:
– underfascial multiple branches + single trunk above the fascia – subfascial single trunk + multiple branches above the fascia – inter-perforators anastomosis
The topography of the non-saphenous perforating veins may also lead to difficulties in the therapeutic approach.
The Method
VANST (Varices’ Ambulatory Non-stripping Surgical Therapy) is a minimally invasive ambulatory surgical method of taking the varicose veins out of the circuit by disconnecting the ways of their filling-up (venous flux and reflux).
Through this procedure the varicose veins are left in place but they become just empty collapsed non-functional tubes.
The steps of the procedure are:
A.The marking on the skin of the places of the future incisions B.The surgical intervention:
–local anesthesia with 1% lidocaine –incisions of 1-3 mm. –the varicose veins (including saphenous trunks) are intercepted, sectioned and –ligated; the same procedure is applied for insufficient perforating veins (including their branches and anastomosis) –a non-compressive bandage is applied. C.The patient is immediately mobilized after the operation and leaves the clinic after 30 minutes. D.Post-operative check-ups (24 hours, 7 days, 2 months and every 6 months).
Results
The total number of cases operated on using the VANST technique : 2008 (in private practice-office based).
The closing-up and disappearance of the varicose veins occurs immediately in 100% of the cases. The insufficient perforating veins are also closed up and the reflux at their level is eliminated.
A 5-year follow-up of 1279 cases (63,7%) showed that the recurrence of the varicose veins after VANST occurred in 89 cases (6,95%).
Conclusions
A.- VANST is both a radical and a conservative method: the varicose veins are permanently taken out of the circuit but VANST preserves the patients’ normal venous capital. B.- VANST can be used for closing up the insufficient perforating veins (including their underfascial branches, non-saphenous perforators and inter-perforating anastomosis) in order to avoid the recurrency of the varicose disease.
Station B: Winner of the best ePresentation
PAPER B5
A specifically designed acquatic exercise protocol to reduce chronic lower limb oedema
1Vascular Diseases Center - Unit of Translational Surgery, University of Ferrara, Italy
2Idrokinetik Clinic, Ferrara, Italy
3Department of Neuroscience and Rehabilitation, S. Giorgio Hospital, University of Ferrara, Italy
Aims
Despite the fact that muscle pump activation is known to positively impact chronic lower limb edema, objective measurements of standardized exercises for venous-lymphatic rehab are lacking.
Moreover, water protocols are becoming extremely popular, claiming to promote also venous drainage, even if not enriched by evidence based-data.
The aim of this investigation is to determine the objective effectiveness of an addressed physical activity exploiting the advantages of an aquatic environment.
Methods
Thirty-two lower limbs of 16 patients affected by bilateral chronic leg swelling were included (12 females, 4 males).
All the patients underwent a protocol of 5 sessions of physical exercises specifically conceived inside a pool.
Volumetry, subcutaneous thickness, ankle range of motion and symptomatology were assessed as outcome measures.
Results
One week after the end of the protocol water plethysmography reported a significant reduction in all lower limbs volume, with an average reduction of 303.13 ± 69.72 ml (p = 0.00002) and of 334.38 ± 62.50 ml (p = 0.000003) in the right and left leg respectively.
At the end of every single session, in comparison with the previous session, a volume reduction was reported, with the exception of the volume variation among the fourth and fifth session. A significant volume decrease was reported among the baseline and the final assessment.
One week after the end of the protocol, the subcutaneous skin thickness and the circumferences significantly decreased in the assessment points (p < 0.0001).
No significant differences were reported regarding the venous hemodynamics.
At the same observation time, the ankle range of motion measurement reported a significant increase both in the dorsal and plantar flexion of the ankle, both on the right (dorsal 2.5o, p = 0.003; plantar 2.8o, p = 0.001) and left side (dorsal 4.1o, p = 0.0001; plantar 2.2o, p = 0.001).
A direct correlation was found among the assessed volume and the circumference value at the middle third of the leg (right leg: r2 = 0.88, p < 0.0001; left leg: r2 = 0.90, p < 0.0001), the subcutaneous thickness (right leg: r2 = 0.85, p < 0.0001; left leg: r2 = 0.71, p < 0.0001) and the ankle range of motion (right leg: r2 = 0.81, p < 0.002; left leg: r2 = 0.71, p < 0.0001).
VAS evaluation reported a significant change in the lower limb heaviness feeling of the patient, decreasing from 7.3 ± 2.1 to 5.5 ± 1.6 (p = 0.001).
Discussion
A specifically designed aquatic protocol is able to positively and objectively impact chronic leg swelling, offering a first line rehab for this medical condition.
PAPER B6
How to prevent lymphatic injuries in venous surgery
Department of Surgery, Unit of Lymphatic Surgery IRCCS S.Martino– IST Institute for Cancer Research University of Genoa, Genoa, Italy
Introduction
Lymphatic complications after great and small saphenous vein surgery have a variable but not ignorable incidence in literature. They often last long time, causing bothering and expensive problems for patients and surgeons. Authors developed a protocol to be applied to all patients undergoing venous surgery in order to avoid lymphatic injuries.
Materials and methods
Between January 2010 and December 2015, 95 patients with lower limb venous insufficiency and varices were studied and treated by the Unit of Lymphatic Surgery, at San Martino-IST IRCCS Hospital in Genoa. Blue Dye was used in all patients and injected into the thigh and below the internal malleolus 10 minutes prior to surgery. Blue lymph nodes and lymphatics were identified intra-operatively and preserved or used to perform multiple lymphatic-venous anastomoses (MLVA) with a competent collateral branch of the great or small saphenous vein. Exclusion criteria were post-thrombotic syndrome and oedema caused by systemic etiology.
Patients were followed up clinically and instrumentally (color Doppler duplex ultrasound and lymphoscintigraphy) for a period variable from 3 months to 6 years.
Results
The mean age of patients was 55,6 years (range 21 to 90 years). The clinical experience included 28 men and 67 women. Color Doppler duplex ultrasound was done in all patients. Lymphoscintigraphy was performed in 35 patients, who presented clinical signs of lymphatic impairment or were at risk for lymphatic complications. Fifty-eight patients were treated by greater saphenectomy and varicectomy; 21 patients underwent varicectomy; 10 patients crossectomy and varicectomy; 5 patients MLVA, greater saphenectomy and varicectomy; and 3 patients were treated by stripping of the small saphenous vein and varicectomy.
No lymphatic complications occurred. An improvement in volume between pre- and post-op measurements was observed in 5 patients with lower limb phlebo-lymphedema treated by MLVA. Lymphoscintigraphy demonstrated no post-operative lymphatic impairment and in 5 patients it showed an improvement of the Transport Index.
Conclusions
The anatomical relationship between lymphatic collectors and veins plays an important role for preventing lymphatic complications during venous surgical procedures. An accurate diagnostic investigation and proper surgical technique associated, when necessary, with microsurgical procedures demonstrated to be of paramount importance in avoiding lymphatic complications during venous surgery and in treating combined lymphatic and venous insufficiency.
PAPER B7
Lympha technique to prevent extremity lymphedema following cancer treatment
1Department of Surgery, Unit of Lymphatic Surgery, S. Martino Hospital, National Cancer Institute, University of Genoa, Italy
2Department of Surgery, Unit of Nuclear Medicine, S. Martino Hospital, National Cancer Institute, University of Genoa, Italy
3Department of Obstetrics and Gynecology, S. Martino Hospital, National Cancer Institute, University of Genoa, Italy
4Department of Surgery, Unit of Oncologic Surgery, S. Martino Hospital, National Cancer Institute, University of Genoa, Italy
Purpose
Inguinofemoral lymphadenectomy carries a high risk of lower limb lymphedema. Following our experience in preventing arm lymphedema after breast cancer treatment, we assessed the feasibility of performing multiple lymphatic-venous anastomoses after inguinofemoral lymph node completion (LYMPHA technique) and the possible benefit of LYMPHA for preventing lymphedema.
Methods
Between February, 2011 and October, 2014, 11 patients with vulvar cancer and 16 patients with melanoma of the trunk requiring inguinofemoral lymphadenectomy underwent lymph node dissection and LYMPHA technique. Blue dye was injected into the thigh 10 minutes prior to surgery. Lymphatics afferent to the blue nodes were used to perform multiple lymphatic-venous anastomoses (MLVA) using a collateral branch of the great saphenous vein.
Results
The mean age of patients in the vulvar cancer group was 52 years (range 48 to 75 years). In the melanoma group, there were 7 men and 9 women with a mean age of 41 years (range 37 to 56 years). Five patients with vulvar cancer underwent bilateral inguinofemoral lymphadenectomy, while the other 6 patients with vulvar cancer and all 16 patients with melanoma of the trunk had unilateral node dissection. All patients were treated by the LYMPHA technique. No lymphocele or infectious complications occurred. Transient lower extremity edema occurred in 1 melanoma patient (6.25 %) which resolved after 2 months, and permanent lower extremity edema occurred in 1 patient (9 %) with vulvar cancer.
Conclusions
Besides having previously showed positive results in avoiding arm lymphedema following breast cancer treatment, the LYMPHA technique appears feasible, safe and effective also for the prevention of lower limb lymphedema, thereby improving the patient's quality of life and decreasing healthcare costs.
PAPER B8
Our simplified SEPS (Subfascial Endoscopic Perforator Surgery) have considerable advantage in treatment of severe refractory stasis ulcers
1Departments of Vascular Surgery & Endoscopic Surgery, Takanobashi Central Hospital, Jinyoukai Medical Corporation, Hiroshima, Japan
2Department of Surgery, Mitsubishi Mihara Hospital, Mihara, Japan
As a new method for treating refractory leg ulcer cases with chronic venous insufficiency due to IPVs (insufficient perforating veins), SEPS (Subfascial Endoscopic Perforating Vein Surgery) was proposed in the 1990s in Europa and America. But now PAPs (percutaneous ablation of perforators) and sclerotherapy are provided instead.
The major reasons of a decline of SEPS are as follows; the first reason is technical difficulties of SEPS itself, and the second reason is that SEPS cannot be done as a day surgery. However, it is well known that SEPS can handle IPVs surely, and long-term results are superior and less complications of maneuver than the other methods.
Our SEPS procedures have been so simplified over the last 12 years by Japanese society for endoscopic therapy of venous disease (JSEPS), and the most important key point was to change the access port. The name of this port is Endo TIP® cannula, which was developed by the Karl Stortz Company in Germany. All of the installments, which we use for our Two Port System SEPS, were originally designed for laparoscopic cholecystectomy operation. Another point was the increase of choice for energy devices such as ultrasonic coagulation and cutting devices or vessel sealing system to sever IPVs.
Consequently, SEPS was authorized as the national advanced medical treatment by the Japanese Ministry of Health, Labor and Welfare in May, 2009 for the chronic venous insufficiency of C4b-C6 patients, according to the CEAP classification. From April 2014, SEPS has been fully covered by the national insurance system in Japan.
The aim of this study is to show our “simplified SEPS” operation procedures, which point out the differences from the original method by Peter Gloviczki and to report about the present condition of IPV (Insufficient Perforating Vein) treatments in Japan.
PAPER B9
Measurement of blood flow in the deep veins of the lower limb using the geko™ neuromuscular electrostimulation device
1The Vascular Noninvasive Diagnostic Centre, London, UK
2Department of Vascular Surgery, Imperial College, London, UK
3Department of Surgery, University of Nicosia Medical School, Nicosia, Cyprus
Objectives
A previous study using electrical stimulation of the common peroneal nerve (geko™) to activate the venous muscle pump measured blood flow in both the femoral and popliteal veins. Increased blood flow by as much as 70% was demonstrated in the femoral vein. Such an increase is assumed to be as a result of an increase in venous flow from the deep calf veins; however this has yet to be confirmed. The aim of this study was to conduct direct measurements to determine velocity and flow increase in individual calf veins in healthy individuals.
Methods
This was a single centre open-label intra-subject healthy volunteer comparison of blood flow in the peroneal, posterior tibial and gastrocnemial veins with and without the geko™ disposable device. The device was applied on the skin over the peroneal nerve in 18 volunteers. Peak venous velocity (PV) and ejected volume per individual stimulus (VS) and volume flow (VF) was determined using ultrasound.
Results
Peak velocity (PV) increased by 216% in the peroneal vein, 112% in the posterior tibial vein and 137% in the gastrocnemial vein (P < 0.001). Ejected volume per stimulus increased by 113% in the peroneal vein, 38% in the posterior tibial vein and 50% in the gastrocnemial vein (P < 0.003). Associated volume flows during the muscle contraction were increased by 36%, 25% and 17% respectively (P = 0.05)
Conclusion
This is the first time that neuromuscular electrostimulation (NMES) has been shown to be an effective method of increasing flow in the axial deep veins of the calf. Although stimulation was via the peroneal nerve, significant increases in velocity and volume flow occurred in all three axial calf veins. Enhancements of both blood velocity and volume flow are key factors in the prevention of venous stasis and ultimately deep vein thrombosis (DVT). Further studies are justified to determine the efficacy of the device in the prevention of DVT.
PAPER B10
Recurrent pulmonary emboli from popliteal vein aneurysm
Basildon Hospital, Basildon, Essex, UK
Introduction
We report a rare case of recurrent massive pulmonary emboli arising from a popliteal vein aneurysm, which was subsequently surgically repaired with good results to 2 years.
Case
A 23 year old female was referred to the vascular service with recurrent bilateral pulmonary emboli. Four years earlier she had suffered a cardiac arrest from a pulmonary saddle embolus and had received thrombolysis. Prior to this she had become non-compliant with warfarin. Thrombophilia screen was normal. Lower limb imaging was performed revealing a 45 × 27 mm saccular left popliteal aneurysm with no thrombus in the sac. The patient was offered repair of the aneurysm or lifelong anticoagulation. She underwent surgical repair via a medial popliteal approach 3 months after her second pulmonary embolism. The aneurysm was tangentially resected and a lateral venorrhaphy performed. She was anticoagulated with rivaroxaban indefinitely and a class II compression stocking applied for 3 months. She remains symptom free at 2 years follow up and has recently run the London marathon.
Literature review
More than 100 cases of popliteal vein aneurysms have been reported since 1976(Bergqvist et al., 2006), with presentation ranging from incidental to limb swelling(Spanos and Giannoukas, 2015), deep venous thrombosis(Gillman et al., 2008), pulmonary embolism or paradoxical embolic stroke(Manthey et al., 1994). The incidence is approximately 0.2% of those undergoing venous duplex imaging(Labropoulos et al., 1996). The largest aneurysm reported measured 9 cm in diameter (van der Voort and De Maeseneer, 2012)and morphology can be either saccular or fusiform. Conventional indications for repair are thromboembolism, thrombus in the sac, or limb swelling. Open surgical repair for saccular aneurysms involves clamping across the neck of the aneurysm, resecting the sac and a lateral suture repair. Fusiform aneurysms are treated with either resection and end to end anastomosis or ligation and vein bypass. There are no reports of endovascular repair. There is one report of recurrence (Gasparis et al., 2010)and one report of recurrent pulmonary embolism after repair(Donald and Edwards, 1982).
Learning Points
Patients with unexplained pulmonary emboli commonly receive imaging of their chest, abdomen and pelvis. We highlight the need to perform a venous duplex of both lower limbs if the embolic source remains cryptogenic. Popliteal vein aneurysm can also mimic a Baker’s cyst, requiring Doppler for differentiation. Surgical repair has a good short term safety profile. The long-term results of surgery and the optimum duration of post-operative anticoagulation are unknown.

Station C: Thrombosis, Basic Science
PAPER C1
The results of treatment of patients with inferior vena cava thrombosis
Belarusian State Medical University, Minsk, Republic of Belarus
Objectives
To determine the main causes, frequency of thromboembolic events (PE), results of diagnostic and treatment of thrombosis of the inferior vena cava (IVC).
Methods
A retrospective study in 22 inpatient patients with thrombosis of the IVC was carried out. The average age of twenty two patients who took part in the study was 53 ± 2 years. In cases of suspicion for a deep vein thrombosis (DVT) in the IVC system its causes, character, localization, prevalence and complications were determined by ultrasonography and phlebocavagraphy. IVC thrombosis management included anticoagulants, elastic compression, phlebotonics in all cases. Four (18.2%) patients with embologeneic thrombosis had undergone surgical procedures – thrombectomy from the IVC with its plication (2 cases), isolated IVC plication, cava-filter implantation.
Results
In twenty one of 22 patients the IVC thrombosis was associated with iliofemoral DVT due to malignancy (35%), inflammatory diseases (10%), surgery and parturition (10%). In two (10%) cases, there was a DVT of the lower extremities in history. In six (30%) cases causes of IVC thrombosis has not been established. Infrarenal, renal and suprarenal IVC thrombosis was diagnosed in 19 (86%), 2 (9%) and 1 (5%) patients respectively. Thrombus flotation in IVC with 2-8 cm head length was identified in 4 cases. PE occurred in three (13.6%) patients. Such complication as cava-filter thrombosis occurred in one case.
Conclusions
In all patients with proximal DVT of the lower extremities IVC involvement in the thrombotic process should be suspected. Early diagnosis and proper treatment IVC thrombosis can guarantee a favorable outcome of the disease and prevent complications. It’s necessary to continue an evaluating of elastic compression and phlebotonics in rehabilitation of patients after IVC thrombosis.
PAPER C2
Retrospective analysis of deep vein thrombosis incidence in patients with superficial vein thrombosis of the lower extremities
Belarusian State Medical University, Minsk, Republic of Belarus
Objectives
To evaluate the occurrence of deep vein thrombosis (DVT) in patients with superficial vein thrombosis (SVT).
Methods
A retrospective study in patients with sonographically proven SVT was carried out in Minsk center of vascular surgery. 93 patients with superficial vein thrombosis were enrolled. Every patient underwent color-coded duplex sonography of both lower extremities at the beginning of the study. Important risk factors (e.g., history of thromboembolic events, recent immobilization, active malignant disease, and the use of hormonal drugs) were investigated.
Results
In 18% of our patients, a concomitant, mostly asymptomatic DVT was found. In all of these patients, the DVT occurred in the affected leg. DVT of contralateral leg was not observed. The common femoral vein was most commonly involved (58.8%). In all patients with DVT, the SVT was located on the lower leg.
Conclusions
Superficial vein thrombosis is not a lifethreatening disease, but the risk of concomitant DVT cannot be ignored. Color-coded duplex sonography should be performed in patients with SVT to rule out DVT. Patient’s age and body mass index are not statistically proven risk factors.
PAPER C3
Long-term results of standard treatment of deep vein thrombosis
Belarusian State Medical University, Minsk, Republic of Belarus
Objectives
To investigate the apparent risk factors for post-thrombotic disease (PTD) and long-term outcomes of standard non surgical treatment of patients with lower extremity deep vein thrombosis (DVT).
Methods
From 137 patients who had DVT, 48 patients participated in the study. The median age was 59.1 (34-76) years. DVT of proximal localization was detected in 18 (37.5%) of respondents, distal – in 30 (62.5%). To identify PTD Villalta scale was used. Depending on the patients compliance to recommendations they were distributed as follows: eight (16.7%) patients followed full outpatient recommendations, partially – 27 (56.3%), did not follow the recommendations – 13 (27%).
Results
PTD has developed in 30 (62.5%) of 48 patients with DVT. In 7 (23%) patients PTD characterized by severe gravity, in 3 (10%) cases with the formation of trophic ulcers. At the age of 60 years and older PTD occurred in 17 (70.8%) cases. In the group of patients with DVT of proximal localization rate of PTD was 72.2%, with distal – 56.7%. From 30 patients with PTD overweight or obesity were found in 24 (80%) patients. In the group of patients with a history of DVT suffering < 3 years PTD has been noted in 47%, from 3 to 6 years – 64%, >6 years – 89%. With regular use of elastic compression PTD was observed in 60% patients, without use of – 33%.
Conclusions
The incidence of PTD among patients with DVT history has no tendency to decrease. Patients with DVT of proximal localization is in greater risk of PTD. Elimination of risk factors (overweight, varicose veins), prevention of DVT and its recurrence – the most appropriate PTD preventive strategy.
PAPER C4
Inferior vena cava (IVC) filters: current district general hospital practice
The Countess of Chester Vascular unit and VTE exemplar center, Chester, The UK
Background and objectives
Insertion of inferior vena cava (IVC) filter is a well-known procedure to safeguard lethal pulmonary embolism (PE). The most common indication for its usage is in patients with proximal deep venous thrombosis (DVT) and contra-indication for anti-coagulation.
There are other indications used in our local trust but no clear-cut guidelines on who should be the decision makers and its application for other indications. Recommendations in the literature guide the clinicians on how and when to use it. This study reviewed the practice in our hospital to assess if we follow these guidelines.
Methods
This retrospective study reviewed all the patients who had IVC filter insertion over a two-year period between January 2014 and January 2016. Patients’ demographics and comorbidities were collected. The indications for insertion, type of filter, retrieval data, complications and the grade and clinical specialty of the team who requested the procedure were all reviewed. The British committee for standards hematology’s guidelines was used as a reference for usage of IVC filter.
Results
50 patients (1:1 male to female, with average age of 64 years) were referred to have IVC filter insertion. One patient failed the procedure due to the load of thrombus in the IVC. Various medical and surgical (1:1) specialties had referred patients to interventional radiologists (IR). 34(69%) of the inserted filters were temporary and only less than half 16(47%) were retrieved. 3(9%) of these filters had a failed retrieval. 22% of these filters were inserted for prophylaxis against PE in patients without acute DVT. 25% of patients had their IVC filter inserted against current BHS guidance. One (2%) patient had acute desaturation and bradycardia during the insertion of the filter but settled after the procedure.
Conclusion
IVC filters are relatively simple and safe device for protection against PE. A significant number of patients had their filters inserted outside current guidance. Literatures recommend removal of IVC filter as soon as there are no more contraindications for anti-coagulation. Our Hospital lacked clear guidelines for IVC filter usage and retrieval, which led to a number of patients requiring unnecessary long-term anticoagulation. We are in the process of developing guidelines and will be followed by prospective monitoring.
PAPER C5
Catheter directed thrombolysis for acute ilio-femoral deep vein thrombosis: a retrospective single center observational study
1Liverpool Vascular and Endovascular Service (LiVES), Royal Liverpool University Hospital, Liverpool, UK
2Interventional Radiology, Royal Liverpool University Hospital, Liverpool, UK
Introduction
The National Institute for Health and Care Excellence (NICE) recommends that catheter directed thrombolysis (CDT) should be considered in selected patients with extensive acute ilio
Methods
This was a retrospective, single center, cohort observational study on patients treated with CDT between September 2012 and December 2015. The main outcome measures were treatment success defined as a patent ilio-femoral segment on imaging.
Results
30 patients were referred for consideration of CDT following a diagnosis of unilateral acute ilio-femoral DVT. Ten patients did not receive CDT. Four were treated conservatively (1 declined CDT, 3 were deemed unsuitable: one with congenital inferior vena cava (IVC) occlusion, one with resistance to warfarin and low molecular weight heparin and one with an iatrogenic injury to the left common iliac vein after rectopexy) and six underwent open surgical thrombectomy (five because thrombolysis was contraindicated and one with thrombus extending into the IVC). 20 patients (10 women and 10 men) were treated with CDT, ten had thrombolysis alone and ten had CDT with stenting. The median age was 50 (range 16 to 68) years. Initial diagnosis was by ultrasound, which was followed by CT venography and pulmonary angiography for procedural planning. All patients underwent unilateral intervention and the left lower limb was involved in fourteen (70%). An inferior vena cava filter was used in all patients. No major bleeding or symptomatic pulmonary emboli occurred. CDT failed to recanalise the ilio-femoral segment in two patients. All successfully treated patients reported symptomatic relief. The median inpatient stay was 11 (range 1 - 44) days. At a median follow up of 6 (1-12) months 12 (66%) patients had patent ilio-femoral segments confirmed on ultrasound. Three patients suffered re-occlusion of the iliac venous system and three others were lost to follow up.
Conclusion
CDT with selective adjunctive stenting is an effective method of treating acute ilio-femoral DVT.
PAPER C6
Recurrent thrombosis secondary to heparin-induced thrombocytopenia following venous recanalisation and stenting
Oxford University Hospitals NHS Foundation Trust, Oxford, UK
Case
A 37 year-old male presented with exertional left swelling and pain. He had been treated with Rivaroxaban for an acute left leg DVT and PE 6 months previously. Magnetic resonance venography demonstrated occlusion of the left common iliac vein and external iliac vein. Venous recanalisation and stenting was performed with placement of two Veniti Vici stents (14 × 120 mm and 14 x 90 mm). Post procedure he was anticoagulated with treatment dose Dalteparin. At day 2, US Doppler demonstrated complete thrombosis of the stented segment with extension into the common femoral vein and superficial femoral vein. He underwent thromboaspiration followed by catheter-directed lysis (Alteplase 1 mg/ml). After 8 hours of thrombolysis check venography demonstrated good thrombus clearance but a residual common femoral vein stenosis, therefore the stent was extended to the profunda origin with a 14 x 90 mm Veniti Vici stent. Completion venography demonstrated excellent flow. Post procedure the patient was placed on a heparin infusion aiming for an APTT of 90–120, given the early extensive thrombosis. It was noted that obtaining an adequately therapeutic APTT was difficult. After two days the patient reported leg swelling and US again demonstrated stent thrombosis. CT confirmed no evidence of stent collapse or constraint. Mechanical thrombectomy was performed using the Aspirex device and catheter-directed lysis (Alteplase 1 mg/hr) was recommenced. At this stage it was noted that the patient’s platelet count was dropping; following consultation with hematology and further investigations, type 2 heparin-induced thrombocytopenia (HIT) was diagnosed. All heparin was discontinued. Check venography demonstrated widely patent stents with excellent flow. Following discontinuation of thrombolysis, anticoagulation was changed to Fondaparinux for 14 days and the patient was then converted to Warfarin. No further episodes of thrombosis occurred. A 6-week US demonstrated widely patent stents with no evidence of thrombosis. At last review (5 months post procedure), the patient was completely asymptomatic and is currently in training for an iron-man event.
Conclusion
Heparin-induced thrombocytopenia is rare, <1%. This case highlights the need to consider the diagnosis in patients with recurrent stent thrombosis. In retrospect, the difficulty obtaining an adequately therapeutic APTT allied with the recurrent thrombosis suggested a hematological cause. The case underlines the importance of a multi-disciplinary team when performing endovascular venous intervention.
PAPER C7
Venous thromboembolism risk assessment model proposal for surgical patients
1Department of Surgery, University Putra Malaysia, Serdang, Malaysia
2Vascular Diagnostic and Screening Center, Nicosia, Cyprus and Imperial College, London, UK
Background and aim
Incidence of postoperative venous thromboembolism (VTE) in Asia is slightly lower than in European countries but its incidence is increasing in the recent literature. It is approaching the level reported in European patients not receiving prophylaxis in the early 1970s. Common risk factors reported to be associated with postoperative VTE in Europe have been compiled and analysed with the aim of producing a preoperative VTE risk scoring system for Asians.
Methods
Using a database of 676 surgical patients screened with I-125 Fibrinogen and confirmed with venography in the absence of VTE prophylaxis in St Mary’s Hospital, London from 1971 to 1972, the predictive power of these common risk factors was tested. Logistic regression analysis was used to calculate odds ratios (OR) to determine VTE independent predictors and their individual power.
Results
The incidences of deep venous thrombosis (DVT) and pulmonary embolism (PE) were 26.7% and 2.1% respectively. The significant independent predictors for DVT were age more than 60 years (OR = 8.91; 2.08 – 38.06, p < 0.01), previous history of DVT (OR = 5.53; 2.36 – 12.97, p < 0.01), varicose veins (OR = 2.79; 1.42 – 5.47, p < 0.01), major operation (OR = 2.37; 1.15 – 4.89, p < 0.05), postoperative infection (OR = 1.66; 1.01 – 2.73, p < 0.05), premedication with opiates (OR = 1.80; 1.11 – 2.93, p < 0.05), hip replacement (OR = 3.03; 1.18 – 7.82, p < 0.05), malignancy (OR = 1.64; 1.04 – 2.58, p < 0.05) and obesity (OR = 1.60; 1.01 – 2.55, p < 0.05). DVT was the most significant predictor for PE (OR = 32.52; 4.12 – 256.86, p < 0.01).
Conclusion
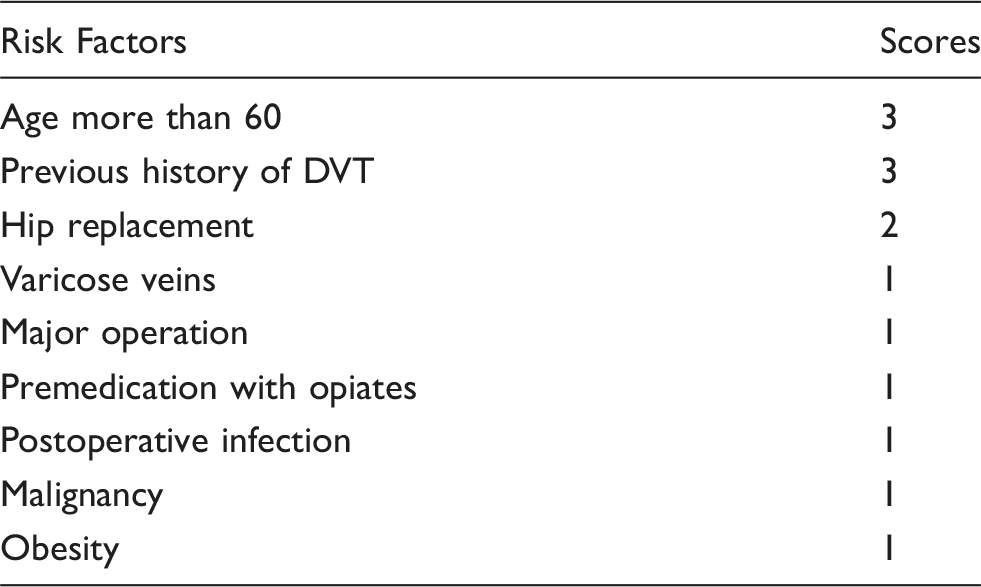
This proposed VTE risk scoring system needs to be validated in a prospective study in Asian patients.
Station C: Winner of the best ePresentation
PAPER C8
A tri-block polymer vepoloxamer-188 potentiates action of heparin and tissue plasminogen activator in animal models
1Josef Pflug Vascular Laboratory, Imperial College and Ealing Hospital and West London Vascular and Interventional Centre, London, UK
2Thrombosis and Hemostasis Research Laboratories, Loyola University Centre, Maywood, IL, USA
3Mast Therapeutics, San Diego, USA
4Department of Surgery, Loyola University Centre, Maywood, IL, USA
Aim
Vepoloxamer 188 (P-188) is a synthetic, organic compound that acts as a surfactant by binding hydrophobic pockets in the circulation. The P-188 has been shown to have anti-adhesive properties within the circulation and is currently being tested in patients with microcirculatory insufficiency such as in sickle cell disease. The aim of this study was to investigate drug interactions between P-188 and heparin and tissue plasminogen activator (tPA).
Materials & methods
The following tests were performed:
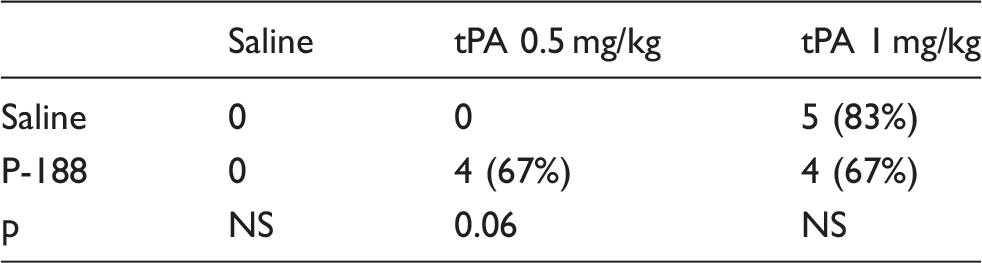
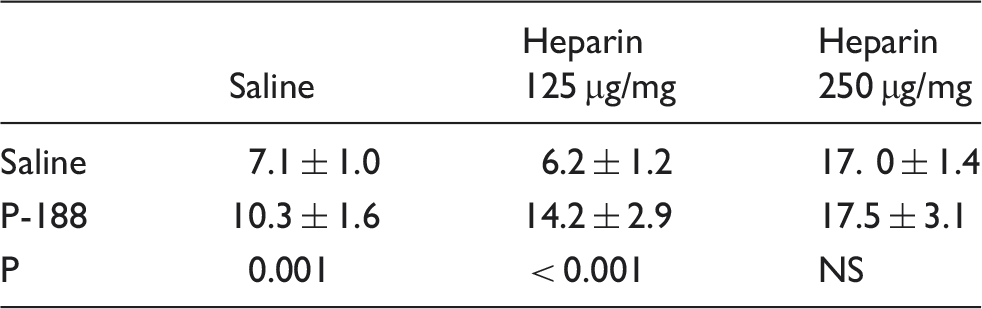
Bleeding Time (BT): Under general anesthesia, saline or P-188 (25 mg/kg) was administered to Sprague Dawley Rats via a tail vein. After 5 minutes, the rats were treated with either saline, low dose heparin (LDH) 125 µg/mg, or high dose heparin (HDH) 250 µg/kg (n = 6 each group). After 5 minutes, the distal 2 mm of the tail was cut and the bleeding time (BT) was measured. Statistical analysis was performed using the t-test. Clot Lysis (CL): Mosquito forceps were used to induce thrombosis in the internal jugular vein via intermittent jugular clamping. Once thrombosis was confirmed by continuous wave Doppler, either saline or P-188 (25 mg/kg) was administered via the tail vein. After 5 minutes, the rats were treated with saline, low dose tPA (LD tPA) 500 µg/mg or high dose tPA (HD tPA) 1 mg/kg (n = 6 each group). The time to clot lysis (detection of flow with Doppler) was recorded. No flow up to 15 minutes was recorded as no lysis. Statistical analysis was performed using the Fisher’s exact test.
Results
The P-188 increased the tail BT by itself and with LDH (Table 1). With HDH, P-188 had no additive effects. The P-188 alone did not influence the CL (Table 2). However, with LD tPA, it tended to facilitate CL (p = 0.06). With HD tPA, P-188 did no have an effect on CL.
Conclusion
Percent thrombolysis.
PAPER C9
Inflammatory and metabolic syndrome biomarker analysis of vascular outcomes in end-stage renal disease
1Josef Pflug Vascular Laboratory, Imperial College and Ealing Hospital and West London Vascular and Interventional Centre, London, UK
2Department of Nephrology, Loyola University Medical Center, Maywood, IL, USA
3Thrombosis and Hemostasis Research Laboratories, Loyola University Medical Center, Maywood, IL, USA
Aims
Bleeding times (min).
Materials and methods
Plasma samples were collected from 83 ESRD patients (mean age 65) prior to hemodialysis and were profiled using biochips for inflammatory and metabolic biomarker levels. Inflammatory cytokine arrays were used to profile the following: Interleukins; IL1a, IL1b, IL2, IL4, IL6, IL8, IL10, vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), interferon gamma (IFNγ), tumor necrosis factor alpha (TNFa) and monocyte chemo-attractant protein-1 (MCP1). Metabolic syndrome arrays were used to profile C peptide, ferritin, insulin, leptin, resistin, plasminogen activator inhibitor-1 (PAI-1). A retrospective review was performed in order to group patients based on history of stroke or TIA, ACS, CHF, and CAD.
Results
Of the 83 ESRD patients, 25 (30.1%) were found to have history of stroke/TIA, 14 (16.9%) were found to have history of ACS, 30 (36.1%) were found to have history of CHF and 39 (47.0%) were found to have history of CAD. Stroke/TIA patients were found to have decreased plasma IFNG levels (p = 0.042) and elevated plasma resistin, IL1a, and leptin levels (p = 0.008, 0.021, 0.026; respectively) when compared to patients without stroke/TIA. The ACS patients were found to have elevated plasma IL6 levels (p = 0.040) when compared to those without ACS. The CHF patients were found to have decreased plasma leptin levels (p = 0.031) and elevated plasma IL1b levels (p = 0.042) when compared to patients without CHF. The CAD patients were found to have elevated plasma IL1a levels (p = 0.049) when compared to ESRD patients without CAD.
Conclusion
Profiling of multiple inflammatory and metabolic syndrome biomarkers may aid in the risk stratification of ESRD patients for cerebrovascular and cardiovascular disorders. These studies demonstrate that biomarker profiling of vascular co-morbidities in ESRD may provide useful diagnostic and prognostic information in the management of ESRD patients.
PAPER C10
New insights into structure and pathogenetic reactivity of the human saphenous vein wall: focus on pericytes and influence of venotropic flavonoids
1Department of Physiology, University of Munich, Munich, Germany
2Department of Cardiac Surgery, Paracelsus University Nuremberg, Nuremberg, Germany
3Department of Anatomy, University of Munich, Munich, Germany
4Department of Cardiac Surgery, University of Munich, Munich, Germany
Background
Extreme perfusion conditions in human leg veins [occasional high hydrostatic pressures; drainage of the intramural vasa venarum (VV) into the parent vein; venous reflux into VV, particularly during valve incompetence], endanger these vessels by inflammation, thrombosis and varicosis/sclerosis. Accumulating evidence implies that these illnesses are inititated and fostered by pathogenetic reactivity in especially the venous intima and the abundant VV. Although incompletely understood, this behaviour—together with platelet and PMN-activities—plays a key role in the progression of unfavourable hydrodynamic conditions to inflammatory and thrombotic processes. We conducted detailed cell-biological investigations of human saphenous vein bypass remnants (HSV) with the aim of a) elucidating this phenomenon further at the cell-biological level and b) collecting more evidence for the specific venotropic action of quercetin- and kaempherol-glucuronide (QG, KG; main flavonols in a red vine leaf extract (Antistax®)).
Methods
Serial sectioning of HSV; selective histological staining methods and techniques (bright field-, fluorescence-, scanning- and transmission electron microscopy); identification, isolation and culture of endothelial cells and pericytes; determination of tissue factor (TF) concentration (activation of factor X) or prothrombinase assembly (PA, formation of thrombin) in the presence and absence of 10-100 µM QG or KG; histological examination of microvessel tightness via leakage of fluorescent plasma proteins; histological demonstration of accumulated flavonoids through their autofluorescence in confocal fluorescent light.
Results
Common to healthy venous intima and the walls of all VV segments (pre-capillary arterioles, capillaries, post-capillary venules) are a tight endothelial sheet (luminal surface) and a loose pericyte network (abluminal surface). The unique endothelium of the venules within the VV-system is contractile and rapidly becomes leaky in presence of inflammatory mediators. Whilst the antithrombotic endothelia of the intima and VV are characterized by the permanent absence of TF and PA, intimal and microvascular pericytes, in contrast, express enormous concentrations of TF and recruit additional amounts (up to the 25-fold concentration within 10 h) during preincubation with serum (29 ± 6 pmol coagulation factor Xa·min−1·10−6 cells; n = 32). Moreover, they readily assemble the prothrombinase complex (9 ± 2 nmol thrombin · min−1·10−6 cells; n = 28). This strongly proinflammatory and prothrombotic behaviour is almost abolished in presence of 100 µM QG and KG, which accumulate specifically in the intima and the VV walls during incubation (1 h). Additionally, these flavonoids prevent excessive leakage of plasma proteins from inflamed VV-venules in presence of simultaneously activated platelets and PMN.
Conclusions
The endothelial cells and pericytes of the intima and VV-system play a central role in the recruitment to and activation of zymogens of the hemostasis systems in the vein wall. Accumulated QG and KG intervene specifically and efficiently.
PAPER C11
Venous intima reconstructed in vitro: influence of simultaneously activated platelets and pmn in absence and presence of polyphenols from red wine leaves
1University of Munich (LMU), departments of cardiac surgery, anatomy and physiology, respectively
2Paracelsus university Nuremberg, department of cardiac surgery
Background
Most venous disorders originate from pathogenetic processes within the thin intimal wall layer of the veins. This intima consists of a luminal sheet of tightly coupled endothelial cells (EC) with well-organized junctional complexes and a subendothelial pericyte network embedded in dense extracellular matrix. In case of a tight endothelial layer (healthy vein), its anti-aggregatory, anti-coagulatory, anti-inflammatory and pro-fibrinolytic activities keep the blood fluid and free of inflammatory mediators. Any event that induces breakdown of this endothelial barrier (e.g. pathophysiological contraction of EC or mechanical lesions), however, results in direct contact between the blood and the pericytes. The latter then act as virtual antagonists of the EC and become the hotspots of inflammatory, pro-thrombotic and sclerotic reactions, especially in cooperation with platelets and PMN. To elucidate such intimal barrier function in more detail and to test the efficacy of venotropic polyphenols, we developed a new in-vitro intima model by cultivating intimal EC and pericytes in “sandwich style”.
Methods
Establishment of pure EC and pericyte cell fractions from proteolytically isolated venous intima preparations, co-culture of both in Transwell cultures. Measurement of hydraulic conductivity (Lp) and the selectivity index for albumin permeability (SIAlb) using a specially developed filtration system. Specific histological staining methods and sensitive microscopic techniques. Microcinematographic demonstration of endothelial contraction in the presence of standardized supernatants of simultaneously activated platelets and PMN (SP + PMN).
Results
The customized intima exhibited typical histological and functional features in vitro. During incubation in plasma-like solution, Lp and SIAlb were 2.6 ± 0.3·10−7 cm·s−1·cmH2O−1 and 0.9 ± 0.03, respectively. In contrast, incubation in Dulbecco culture medium supplemented by fetal calf serum (20 vol%, includes inflammatory mediators!) changed these values to 1.4 ± 0.1·10−6 cm·s−1·cmH2O−1 and 0.5 ± 0.04. SP+PMN induced rapid and maximal opening of EC-clefts and a maximal Lp within 30 min (Lp ≈2 ± 0.8·10−5 cm·s−1). This breakdown of the barrier function was preventable and/or reversible in the presence of 1–100·10−6 , M quercetin- or kaempherol-glucuronide (QG, KG; EC50: 30 or 20 µM, respectively), that are present in red vine leaf extract (Antistax®). The latter also contains an additional, very potent, intima-protective (EC50 ∼6 µM) polyphenol fraction of poorly defined composition, which could be isolated using Sephadex LH20 chromatography and methanol as eluent.
Conclusions
With the use of this new in-vitro model of the venous intima, systematic, detailed studies on the regulation of its barrier properties now appear feasible. Naturally occurring polyphenols, like the flavonols QG and KG in red wine leaf extracts, appear as potent anti-inflammatory drugs, which protect the intima and maintain their barrier function, thus obviating thrombotic and sclerotic processes.
PAPER C12
Transdermal application of therapeutic compounds targeting venous endothelial and smooth cells attenuates varicose and spider vein development
1Institute of Physiology and Pathophysiology, University of Heidelberg, Germany
2Division of Cardiovascular Physiology, University of Heidelberg, Germany
Varicose veins are commonly associated with swollen and painful legs which may potentially develop complications including skin ulcers, superficial thrombophlebitis, bleeding and inability to stand or to walk. Although not comparable in the extent of their severity, spider veins are defined as dilated, intradermal venules less than 1 mm in diameter which resemble varicose veins on a much smaller scale. Consequently, there is a need for a strategy to therapeutically interfere with the initiation and progression of varicosis and spider veins and the identification and manipulation of mechanisms controlling venous remodelling at the molecular level. To investigate whether spider veins are directly connected to the deeper vein plexus, blood perfusion of a spider vein (left leg, knee level) was measured from a healthy female volunteer using the PeriCam PSI blood perfusion imager. An increase in blood perfusion of a spider vein was observed when the volunteer was asked to actively contract the muscles of the leg as opposed to the low perfusion levels after prolonged standing without any muscle contraction. We therefore assume that superficial veins may also be affected by chronic venous hypertension and may thus be affected by an increased filling pressure in the underlying venous network. Correspondingly, chronic experimental increase of the filling pressure in saphenous veins of mice led to the development of dilated and bulged superficial veins. Based on these findings, we have utilized in vitro and in vivo models to better understand the underlying mechanisms of stretch-induced venous remodelling. Human umbilical vein smooth muscle (HUVSMCs) and endothelial cells (HUVECs) were exposed to biomechanical stretch for up to 24 hours which increased their MMP9 expression (HUVSMCs) and gelatinase activity (HUVSMCs, HUVECs). In order to identify novel molecular targets activated upon biomechanical stretch, a Phosho-Kinase Array (HUVSMCs/HUVECs) as well as genome-wide microarray procedure (HUVECs) have been utilized. Further, we have reproducibly evoked venous hypertension in vivo by ligating one large vein in the mouse auricle, resulting in the growth and enhanced tortuosity of the collateral veins. Based on that model, we have previously revealed that transdermal therapeutic blockade of the transcriptional activity of activator protein 1 (AP-1) or the proteasome inhibits venous remodeling. Aside from identification of novel stretch-induced signaling pathways, the use of in vivo and in vitro models opened further avenues into additional translational research approaches, where naturally-derived cream based formulations and naturally based plant extracts were tested in order to i) attenuate biomechanically evoked spider vein remodelling ii) gain further mechanistic insight into varicose and spider vein development and progression.
PAPER C13
Wound circulation speeds up immediately after a hyperbaric oxygen treatment
1Chalmers University of Technology, Gothenburg, Sweden
2Stanford University School of Medicine, Stanford, USA
Objectives
It has been established that hyperbaric oxygen therapy (HBOT) can facilitate wound healing in diabetic lower extremity ulcers. However, it is still an open question what the underlying physiological mechanisms are. We will here focus on the possible impact HBOT has on the tissue perfusion and vascular flow rates.
Methods
The above question was addressed by analysing the immediate effects of HBOT on the microvasculature of chronic wounds as assessed by fluorescent angiography. Patients underwent fluorescent angiography at four different time points: immediately prior and immediately after the first and second HBOT treatments. Photo imaging with infrared camera began concurrently with the initiation of the IC-Green™ injection and lasted for 150 seconds. The output data consisted of videos that were studied using image analysis tools. The wound edge was outlined manually by hand to create a mask for the wound bed, our main region of interest (ROI). The second ROI we analysed was the peri-wound defined algorithmically from the wound edge. We generated a time dependent intensity function by capturing the mean pixel intensities. Once we obtained this function we defined a number of features from it: the maximum intensity, the maximum inflow and outflow rates as well as four characteristic times measured from the injection time of the fluorescent. These times are: the first detection of a signal, when the intensity increased the fastest, when the max intensity occurred, the times when the intensity decreased the fastest.
Results
In this pilot study, we demonstrated that HBOT results in an immediate increased vascular flow both in the wound and in the peri-wound.
Conclusions
It was shown in this pilot study that HBOT has an immediate impact on the flow rates in the vascular system in and in the vicinity of a wound. This finding in itself raises new questions on the underlying physiological reasons for this process, that could in turn generate new studies, in vivo and in vitro, to give a better understanding how and why the HBOT treatment affects the wound healing process from a fluid dynamic view point. Eventually, insights in these processes might better explain the benefit of HBOT and may expand the repertoire of diseases that may serve to benefit from this modality.
PAPER C14
In vivo and in vitro effects of ruscus extract are mediated by muscarinic receptors
1Centre de Recherches Pierre Fabre, 17 Av. Jean Moulin, 81100 Castres, France
2Laboratory for Clinical and Experimental Research on Vascular Biology (BioVasc), Biomedical Center, State University of Rio de Janeiro, Rio de Janeiro – RJ - Brazil
Objective
The venotonic properties of Ruscus aculeatus (butcher’s broom) are well established, but its mechanism of action is not completely understood. The goal of the present study was to evaluate a possible contribution of muscarinic receptors and therefore we have tested Ruscus extract in vitro for its binding and functional properties at recombinant muscarinic receptor subtypes and in vivo for its impact on the microvasculature in the hamster cheek pouch preparation.
Material and Methods
Ruscus extract was tested in competition binding experiments at recombinant human muscarinic receptors, heterologously expressed in CHO cells. Its activity was further evaluated in cellular assays measuring Ca2+ liberation and AP-1 reporter gene activation. The impact of muscarinic blockade on prolonged Ruscus treatment outcome was evaluated in the hamster cheek pouch microcirculation examining several parameters, namely macromolecular permeability increase induced by either histamine or ischemia/reperfusion (I/R), mean arteriolar and venular diameters, functional capillary density and leukocyte rolling and sticking induced by I/R.
Results
Ruscus extract exhibited affinities to muscarinic receptor subtypes in a range of 50-100 µg/ml. It further behaved as an efficacious partial agonist at human recombinant M1 and M3 receptors for Ca2+ liberation, confirmed in an AP-1 reporter gene assay. In the hamster cheek pouch model, topical application of the muscarinic antagonist atropine completely or partially blocked Ruscus extract-induced reductions of (1) histamine and ischemia/reperfusion increases of macromolecular permeability, (2) venular diameter and (3) leukocyte rolling and sticking.
Conclusion
Our results show that Ruscus extract binds to different subtypes of muscarinic receptors and behaves as an efficacious partial agonist particularly of M1 and M3 receptor subtypes. In vivo, we have confirmed its anti-inflammatory and venotonic effects which were at least partially mediated via muscarinic receptors. Our findings constitute a new mechanism of action for this product, previously demonstrated to have adrenergic properties.