
Abstract
Objectives
Functional chronic venous disease is an underestimated syndrome quite present in the general population. It affects up to 20% of the general population and is based on the presence of venous symptoms without instrumental evidence of anatomic and morphologic damage. The aim of this review article is to provide the reader with the most updated information on this phenomenon.
Methods
Medline and Scopus databases were searched without time limit using the key-word: ‘Functional chronic venous disease of legs’, C0s patients. We decided to include all the studies conducted about functional chronic venous disease. Randomised trials, cohort studies and reviews were contemplated in order to give a breadth of clinical data. Only publications in English were considered. We excluded all the studies with insufficient statistical analysis, possible biases and contradictions, not clear end-points, inconsistent or arbitrary conclusions.
Results
Of the 326 records found, after removal of 68 duplicates, 143 matched our inclusion criteria. After reading the full-text articles, 133 manuscripts were excluded. Ten full text articles were assessed for eligibility and four studies were excluded because of the following reasons: (a) no specific or important content and (b) insufficient data; the final set included six articles.
Conclusions
Functional chronic venous disease is a complex syndrome and further evidences are needed in order to assess the pathophysiology, the morbidity and the correct treatment of this venous dysfunction.
Keywords
Introduction
Chronic venous disease (CVD) is a very common condition affecting western adult population with a prevalence of <10%, among individuals younger than 30 years for both sex, and with a prevalence up to 77%, in individuals aged ≥70 years.1,2
According to clinical classes (C) of the Clinical–Etiology–Anatomy–Pathophysiology (CEAP) classification, 3 patients belonging to the first C class (C0), with no visible or palpable signs of venous disease, may even experience subjective perception of CVD-related leg symptoms, which include aching, pain, tightness, skin irritation, heaviness, muscle cramps and other complaints attributable to venous dysfunction, and, in this case, patients are classified as C0s.
The presence of C0s can be defined as a status of Functional Chronic Venous Disease (FCVD) and, in the past two decades, different definitions have been used such as hypotonic phlebopathy (HP), phlebopathic diathesis, pre-varicose syndrome, functional phlebopathy, functional chronic venous insufficiency, functional venous disease.4–6 Andreozzi et al. found an important prevalence rate of hypotonic phlebopathy in more than 15% in an Italian epidemiologic study called the Acireale Project and conducted on the general population in a small town of 50,000 inhabitants. 4 A further Italian Study 7 which studied the correlation between visible signs, symptoms and presence of functional disease showed that 80% of C0 subjects complaining of subjective symptoms had legs without instrumental evidence of anatomic and morphologic damage.
Considering the relevance of the problem, and the lack of any reviews on this condition, the aim of this review article is to provide the reader with the most updated information on this phenomenon.
Methods
This systematic review was conducted and is reported in accordance with the PRISMA guidelines. 8
Inclusion and exclusion criteria
We decided to include all the studies conducted on FCVD. Randomised trials, cohort studies and reviews were contemplated in order to give a breadth of clinical data. Only publications in English were considered. We excluded all the studies with insufficient statistical analysis, possible biases and contradictions, not clear end-points, inconsistent or arbitrary conclusions.
Search strategy
Two members of the research team (RS, SdF) performed a comprehensive literature research using terms identified and agreed by the Authors. Medline and Scopus databases were searched without time limit using the keywords: ‘Functional chronic venous disease of legs’ and ‘C0 patients’.
Data extraction and risk of bias assessment
Two review authors (MA, PM) independently assessed both titles and abstracts searched through Medline and Scopus potentially eligible studies. In case of ambiguous or unclear result, the study was retrieved in full and assessed further by all authors independently and included if pertinent. All studies were assessed by using the Downs and Black quality checklist.9,10
Results
Study selection
Of the 326 records found, after removal of 68 duplicates, 143 matched our inclusion criteria (Figure 1).
PRISMA diagram.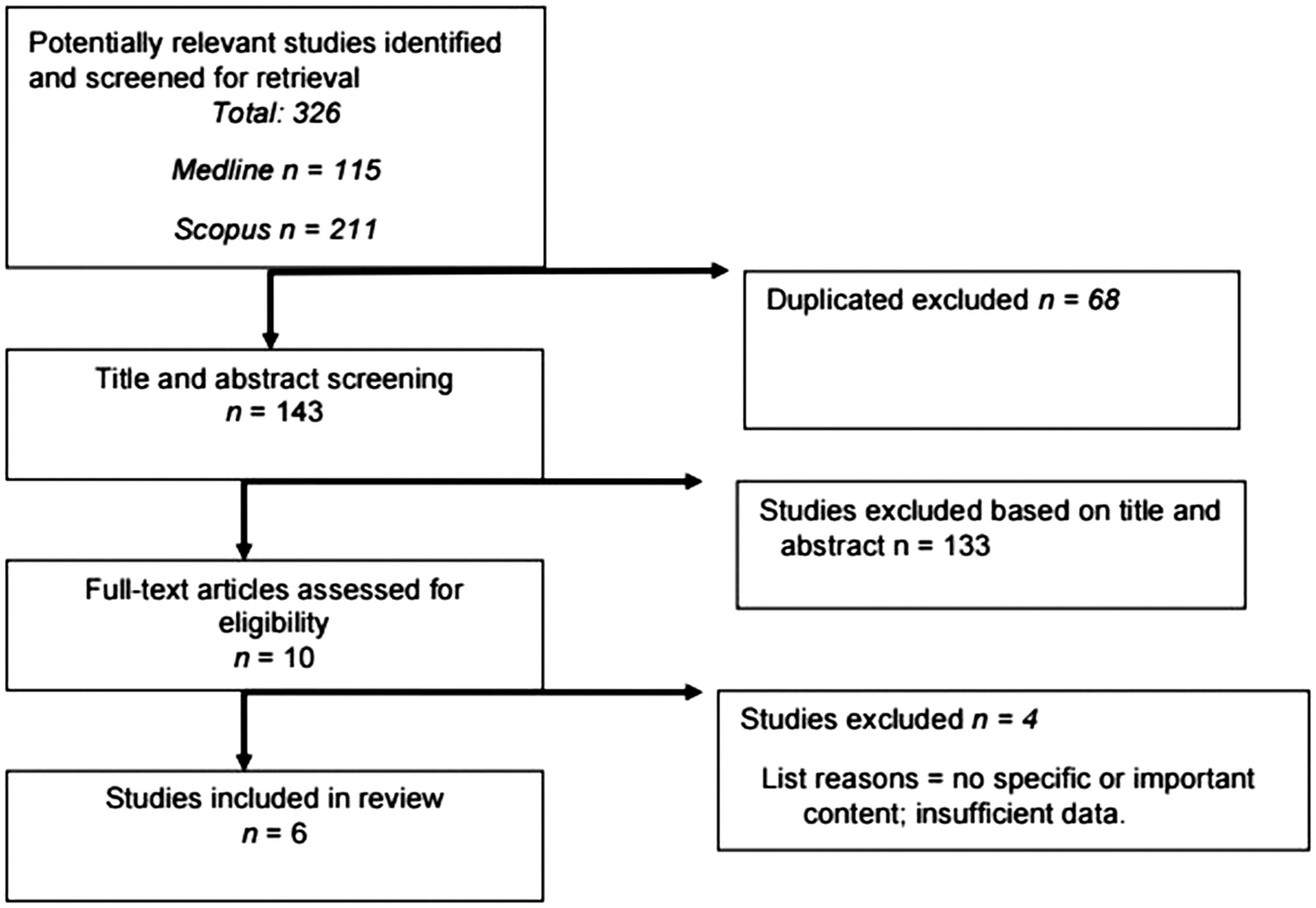
After reading the full-text articles, we decided to exclude 133 manuscripts based on title and abstract. Ten full text articles were assessed for eligibility and four studies were excluded because of the following reasons: (a) no specific or important content and (b) insufficient data; the final set included six articles.
Epidemiology of FCVD
Andreozzi et al.
4
during the 3-year trial, of the Acireale Project, which started in September 1989 and ended in July 1992, found an overall prevalence of hypotonic phlebopathy (HP) of 15.90%, and, among these patients, the authors identified four subgroups according to the typology and duration of symptoms and with duplex examination showing, always, venous patency and absence of valve dysfunction of reflux:
HP with subjective symptoms always present. This condition accounted for 26.83% cases of total HP. Latent HP with subjective symptom referred intermittently (spring, summer pregnancy, hard standing work, etc). This condition accounted for 27.43% cases of total HP. Enhanced HP with subjective symptoms continuously present during the examination period, but occasionally in the past, and related to an identifiable cause. This condition accounted for 29.89% cases of total HP. Senile HP with subjective symptoms continuously present since the sixth decade, and never or occasionally in the past. This condition accounted for 15.89% cases of total HP.
The prevalence of HP was twofold in females than in males, while Latent, Enhanced and Senile HP showed no difference according to sex.
The prevalence of phlebostatic symptoms in HD were mainly heavy legs (74.39%), followed by night resting cramps and restless leg syndrome (29.26%). The prevalence of the investigated risk factors in HD were family history (42.07%), obesity (37.19%) and constipation (29.26%). Among women with HD, pregnancy represented a significant risk factor (50.56%).
The study by Chiesa et al. 7 confirmed the role of Body Mass Index (BMI) and family history of CVD in FCVD.
In the San Diego Population Study which enrolled 2408 adults who were randomly selected from an ethnically diverse population, aching was the most commonly reported symptom (15%) related to CVD in participants C0s with normal legs (assessed by either functional or visible status). 11
The Vein Consult Program 12 was an international, observational, prospective survey that collected global epidemiological data on CVD-related symptoms, organized within the framework of routinary General Practitioner (GP) consultations of five geographical zones: Western Europe, Central and Eastern Europe, Latin America, the Middle East and the Far East totalling 20 countries and screened a population of 91,545 subjects. It was found that 19.7% of the study population could be included in C0s class. In this study of all screened women, 18.5% were at the C0s stage versus 22.4% of screened men. Whatever the age group, men were more likely to be assigned to the C0s class of the CEAP than women, except in the 18–34 age range. Screened subjects were younger in the C0s than the C1–C6 population: 48.3 ± 16.8 years versus 55.5 ± 15.3 years. No significant difference in the mean BMI was found between the C0s and the C1 to C6 sub-groups of screened participants. From a geographical point of view, this study found that C0s subjects were more prevalent, in Western Europe and the Far East. In the C0s population, the symptom distribution and ranking were similar to those of symptomatic subjects in the C1–C6 classes, except that night cramps ranked higher.
A recent epidemiological survey in Belgium and Luxembourg, 13 with a cohort of 6009 patients included in the study, reported that, on clinical examination by the GP, 61.3% of the patients had CVD or 75.2% if C0s patients were included.
Pathophysiology, molecular and instrumental features
Two major mechanisms are believed to be responsible for pain and heaviness in CVD: (a) venous wall tension caused from the dilatation of vein (prolonged standing position in a normal subject or venous incompetence in ill subjects) and (b) hypoxia of the tunica media of the venous wall due to the alteration of the vasa vasorum. 14 Restless leg syndrome and night muscle cramps seem to be related mainly to hypoxia of the tunica media and with haemorheologic disorders such as hyperviscosity and hyperaggregation, which are constant findings in CVD. 14 Leukocyte-endothelium interaction may account for an abnormal inflammatory response involved in venous symptoms. Furthermore, the extracellular matrix (ECM) is pivotal for the nutrition and the homeostasis of endothelial cells 14 and it has been showed previously that the alterations of ECM, mediated by metalloproteinases, are already present from the very early stages of CVD, 15 and this may have also a role in the onset of symptoms. 14
Moreover, nerve structures known as C-nociceptors, that can be activated by inflammatory mediators, have been found both in the media of varicose veins and in the perivenous connective tissue.12,16
Furthermore, Allegra et al. 5 postulated even a role of estrogens and endocrine changes in the pathogenesis of FCVD, and this aspect needs further investigation, especially, in the light of the latest findings about the function of these hormones on the veins. 17
Andreozzi 6 suggested that subjective symptoms in HP could also be caused by the reduction of the venous wall tone caused by the reduction of the muscle – venous calf pump and increase of the venous wall compliance, which can be easily detected with the strain-gauge plethysmography, reflection light photopletismography (PPG), Laser Doppler evaluation and Duplex Ultrasound measuring, in this latter case, the difference between the vein diameter in supine and upright position at the level of the popliteal vein, tibio-peroneal trunk and gastrocnemial veins.
Treatments
FCVD patients are poorly treated in general: in fact in the Vein Consult Program only 13% of C0s patients received lifestyle advice and 8% were prescribed a venoactive drug. 12
From a pharmacologic point of view, C0s patients are frequently encountered in primary care practice and potentially represent the largest target population for venoactive drugs (VADs) treatment. 18 Current VADs may exert positive effects on the main trigger points of symptoms onset restoring the homeostasis between endothelial cells and smooth muscle cells of the media, improving haemorrheological disorders, attenuating leukocyte-endothelium interactions 18 and counteracting ECM alterations. 19
Blazek et al. 20 conducted a study on a population of hairdressers who were randomized to wear medical compression stockings (MCS) (ankle pressure 15–20 mmHg). All patients, including the subgroup of C0s patients that in this study was 54%, experienced substantial leg symptoms relief after wearing MCS.
Discussion
FCVD or C0s patients are defined as those presenting with one or more CVD-related symptoms, but showing no clinical signs of the disease during a physical examination, and generally no abnormalities on a duplex scan. 12
The prevalence of FCVD, based on the few studies, present in the current literature ranges from 13.9 to 19.7% in the general population.4,6,11–13
From the Vein Consult Program, we learned that men seem more likely to be assigned to the C0s class compared with women and, in general, the mean age of onset is lower compared with the other C classes. 12
Symptoms associated with FCVD may include numbness, aching, sensation of burning, pain, night cramps, swelling, sensations of throbbing or heaviness, itching, restless legs. However, although not pathognomonic, these symptoms may be suggestive of FCVD, especially if they are exacerbated by heat or dependency in the day’s course, and relieved with leg rest and/or elevation. 12 Night cramps seem to be more specific for FCVD. 12
There is also great evidence that the symptoms of FCVD individuals are greatly improved with conservative treatments, both by VADs and compression therapy.12,18,20
An important limitation of the studies present in the current literature is that there is no longitudinal study evaluating FCVD subjects, thus, their CVD progression is not predictable at the moment. Considering also that spontaneous consultations for venous problems are less frequent among FCVD subjects compared with the C1–C6 patients, 12 probably such patients should deserve more investigation because of the possible progression of their clinical status towards more severe classes of CVD.
Furthermore, quite often in many studies, information regarding venous incompetence is certainly limited in accuracy, particularly for the presence or the absence of venous reflux in smaller tributaries, which can contribute to the presence of symptoms and this would overestimate the prevalence of FCVD.
Another important issue to be solved is to demonstrate a specific and significant association between symptoms and venous dysfunction in C0 patients, distinguishing them from other diseases of the legs, such as arthrosis, peripheral arterial disease, spinal disc herniation, etc. 21 Moreover, the results from the Bonn Vein Study 1 22 postulated also that common symptoms like feeling of heaviness and tightness of the legs are significantly associated only for C2–C6 patients, and that, generally, restless legs and muscle cramps seem to be even less specific.
Conclusion
Further studies based on molecular biology will help physicians to better understand the basis and the pathophysiology of FCVD and further clinical longitudinal studies are needed in the next future to clarify the behaviour of FCVD and the destiny of patients affected, in order to better diagnose and treat this widespread clinical condition.
Footnotes
Authors’ contributions
RS and SdF researched literature and conceived the study and provided critical revision of the article. MA and PM were involved in data collecting and data analysis. GDC and MM wrote the first draft of the manuscript and were also involved in data collecting. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.