
Abstract
Objectives
To evaluate health-related quality of life after venous thromboembolism.
Methods
We conducted a cohort study, TEHS follow-up, including 1040 women with a first episode of venous thromboembolism and 994 women unexposed to venous thromboembolism. Patients were recruited from the “Thrombo Embolism Hormonal Study” (TEHS), a Swedish nation-wide case–control study on risk factors for venous thromboembolism in women 18–64 years of age. Quality of life was measured using SF-36 and VEINES-QoL/VEINES-Sym.
Results
On average there were no difference in mean SF-36 summary scales scores between exposed and unexposed women. Twenty percent of exposed women developed postthrombotic syndrome during follow-up. Women with postthrombotic syndrome had severely impaired quality of life with lower scores on all scales. Other predictors of low quality of life after venous thromboembolism were age, obesity, physical inactivity, and recurrent venous thromboembolism.
Conclusion
Long-term quality of life after venous thromboembolism in women was severely impaired among those developing postthrombotic syndrome, while quality of life in women not developing postthrombotic syndrome was similar to a control population.
Introduction
While etiology, diagnosis, and treatment of venous thromboembolism (VTE) have been extensively studied, only a few studies evaluated how VTE affects health-related quality of life (QoL).1–5 QoL can be analyzed using both disease-specific instruments to assess disease specific impact on QoL as well as generic instruments to be able to compare QoL with the general population and also with other patient groups. Previous studies reported that QoL is reduced in patients with VTE compared to population norms, and the predominant predictor of QoL after an episode of deep vein thrombosis (DVT) appears to be presence of postthrombotic syndrome (PTS).1,6–8 PTS is one of the most common long-term complications of DVT. PTS is a chronic condition characterized by pain, swelling, heaviness, cramping, and objective signs such as edema, hyperpigmentation, and varicose veins. PTS affects 20–50% of patients, after a symptomatic DVT in the lower extremity.9–13 Some studies have also described PTS after an asymptomatic DVT.14,15
The aim of this study was to evaluate the long-term effect on QoL after a first episode of VTE in young and middle-aged women compared to a control population. We also intended to assess how PTS and other patient characteristics affect QoL and to study the incidence of PTS and risk factors therefore.
Materials and methods
This is a follow-up study of the “Thrombo Embolism Hormone Study” (TEHS), a case–control study on risk factors on VTE in women. 16 Women with a first episode of DVT in the lower extremity or pulmonary embolism (PE) (exposed) were followed for a median of six years (range 2–9 years) with respect to PTS and QoL. Women with no previous VTE (unexposed) were followed for median of five years (range 2–8 years) with respect to QoL.
Study population
The methodology of TEHS has been described previously. 16 Briefly, 1433 women with a first episode of DVT in the lower limb or a PE were included as cases from 2002 to 2009 from 43 hospitals spread geographically in Sweden. The 1402 controls, matched to the cases by age, were randomly selected from the Swedish Population Register. Women who had been pregnant during the past three months, had a current malignancy, or a history of malignancy within the past five years were not eligible for inclusion in TEHS. The diagnosis of VTE was objectively verified by venography or Doppler ultrasound for DVT patients and by CT scan or ventilation–perfusion scintigraphy for PE patients.
Baseline information was collected through a telephone interview within three months of the diagnosis of VTE for exposed and at time of inclusion in the study for unexposed. The interview included questions on risk factors for VTE, weight, height, smoking, physical activity, and questions on leg symptoms (pain, heaviness, and swollen legs) and varicose veins prior to the symptoms of VTE in exposed and prior to the interview in unexposed.
Study procedures
In 2011, all women still living in Sweden were asked to participate in the follow-up study by a mailed questionnaire. After one month a reminder was sent to women not answering the questionnaire. Of the 2835 (1433 exposed, 1402 unexposed) women included in TEHS, 49 (37 exposed, 12 unexposed) were deceased at the time of follow-up. Three women had emigrated from Sweden and 715 (345 exposed, 370 unexposed) women rejected participation in the follow-up study. In total 34 (10 exposed, 24 unexposed) women had incomplete questionnaires regarding 36-Item Short-Form Health Survey (SF-36) and/or VEINES-QoL/VEINES-Sym and were therefore excluded. The final study population comprised 1040 women with previous VTE (exposed) and 994 women without previous VTE (unexposed).
Assessment of QoL
The comprehensive questionnaire included questions on lifestyle factors such as weight, height, smoking, and physical activity as well as questions on medication and use of compression stockings. To assess generic QoL, the questionnaire included questions according to SF-36.17,18 The SF-36 consists of 36 items and assesses general well-being during the previous 30 days. It contains eight subscales: physical functioning, social functioning, physical role functioning, emotional role functioning, mental health, vitality, bodily pain, and general health. Standard algorithms were used to calculate scores for the mental component scale (mcs), a summary score that reflects scores on the vitality, social functioning, mental health, and emotional role scales, and the physical component scale (pcs), a summary score that reflects scores on the physical functioning, physical role, bodily pain, and general health perceptions scales. Scores are expressed on a 0–100 scale, with higher values indicating better general well-being. 19
To analyze disease-specific QoL for women with a previous VTE, there were questions according to VEINES-QoL/VEINES-Sym. 20 The VEINES-QoL consists of 26 questions that assess venous symptoms (heavy legs, aching legs, swelling, night cramps, heat or burning sensation, restless legs, throbbing, itching, tingling, intensity of leg pain), limitations in daily activities due to chronic venous disease, psychological impact of chronic venous disease, change over the past year, and time of day when the leg problem is most intense. The VEINES-Sym is a subscale of the VEINES-QoL that measures venous symptoms. 20
Assessment of PTS
Self-reported Villalta scale.
All symptoms and signs score 0 if absent and 1 if present. Postthrombotic syndrome was considered present if score ≥ 4.
Statistical analysis
Standard algorithms were used to calculate scores for SF-36 mcs, SF-36 pcs, VEINES-QoL, and VEINES-Sym.17,21 Categorical data were compared using χ2 test. Continuous variables were presented as mean and standard deviation for normally distributed data and as median and interquartile range (IQR) for nonnormally distributed data. When comparing continuous data, we used t-test for normally distributed data and Mann–Whitney U for nonnormal data.
The difference between exposed and unexposed regarding QoL was analyzed using analysis of variance (ANOVA). The mean score of mcs and pcs, respectively, was used as the dependent variable and being exposed or unexposed to VTE was the main independent variable. Covariates being associated with the dependent variable in univariate analyses were included in the model as potential covariates. A backward selection procedure (p < 0.05) was used to select the variables for the final model. As covariates we included age (≥50 years/<50 years), physical activity (regular activity/inactive), BMI (<25/25–30/≥30 kg/m2), education (<10/≥10 years), and civil status (married or concomitant/single).
ANOVA was also used to assess possible predictors of QoL among women with a previous episode of VTE. Separate analyses were made for SF-36 pcs, SF-36 mcs, VEINES-QoL, and VEINES-Sym. The score of the QoL instrument was used as dependent variable and PTS was the main independent variable. Covariates being associated with the dependent variable in univariate analyses were included in the model as potential covariates. A backward selection procedure (p < 0.05) was used to select the variables for the final model.
For all QoL scales, a difference in three points was considered clinically relevant. For all analyses, p-values < 0.05 was considered significant.
To assess predictors of PTS, we used logistic regression comparing women with PTS to women without PTS. Risks were calculated and reported as both crude and adjusted odds ratios (ORs) and their corresponding 95% CIs. All variables significant in the univariate model were included in the multivariate model. P-values < 0.05 were considered significant. All statistical analyses were performed using SPSS, version 23 (IBM SPSS Inc., Chicago, Illinois, USA)
Results
Study participants
Baseline characteristics of patients at the time of inclusion in TEHS.
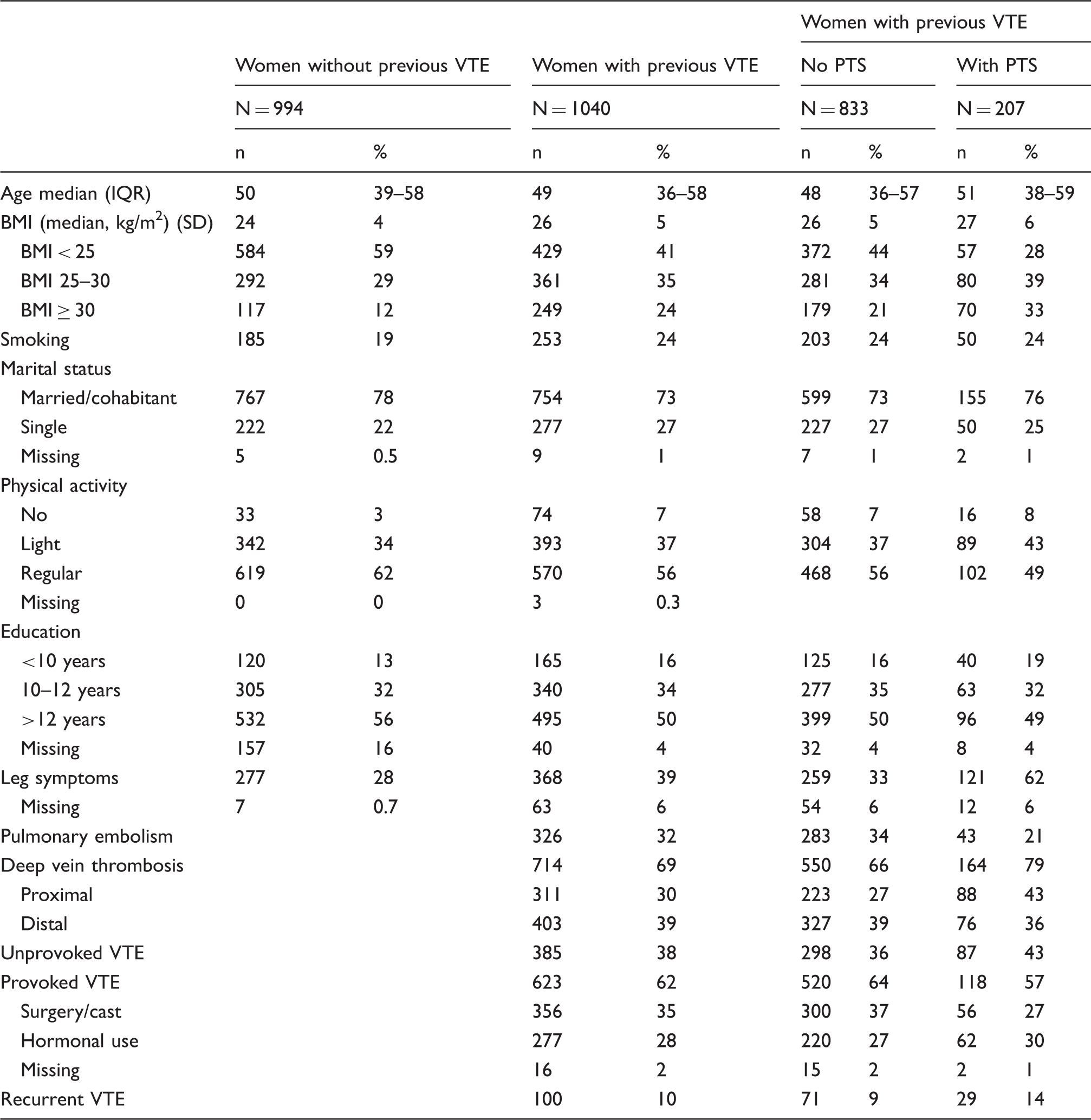
BMI: body mass index; IQR: interquartile range; PTS: postthrombotic syndrome; SD: standard deviation; VTE: venous thromboembolism.
Among women with VTE, 714 (69%) were diagnosed with DVT only, 297 (28%) with only PE, and 29 (3%) with DVT and concomitant PE. In women diagnosed with DVT, 44% had a proximal DVT, of which 174 (56%) were on the left side. Of the 403 women with distal DVT, 219 (54%) were in the left leg. Median time between VTE event and follow-up was six years (IQR 4.8–6.9). A total number of 100 women had a recurrent VTE event during follow-up, 30 as a distal DVT, 26 as proximal DVT, 43 as PE, and one had a sinus thrombosis. Thirty-two patients suffered from an ipsilateral recurrent DVT.
QoL in exposed women compared to unexposed
Among exposed women, 1017 completed all subscales of SF-36 and among the unexposed women, 994 completed all subscales. Women with previous VTE had significantly lower scores on the subscales of physical functioning (80.2 versus 87.2), physical role functioning (77.5 versus 82.8), mental health (75.9 versus 79.3), vitality (59.1 versus 64.3), and general health (66.6 versus 73.7). For the subscales of social functioning (84.2 versus 86.6), emotional role functioning (80.8 versus 84.7), and bodily pain (74.2 versus 73.7), there were only minor or no difference. For the SF-36 produced summary scales, pcs and mcs, there were only small, nonclinical significant differences (47.0 versus 49.2 and 47.5 versus 48.7).
Predictors of QoL in exposed and unexposed women, multivariate.
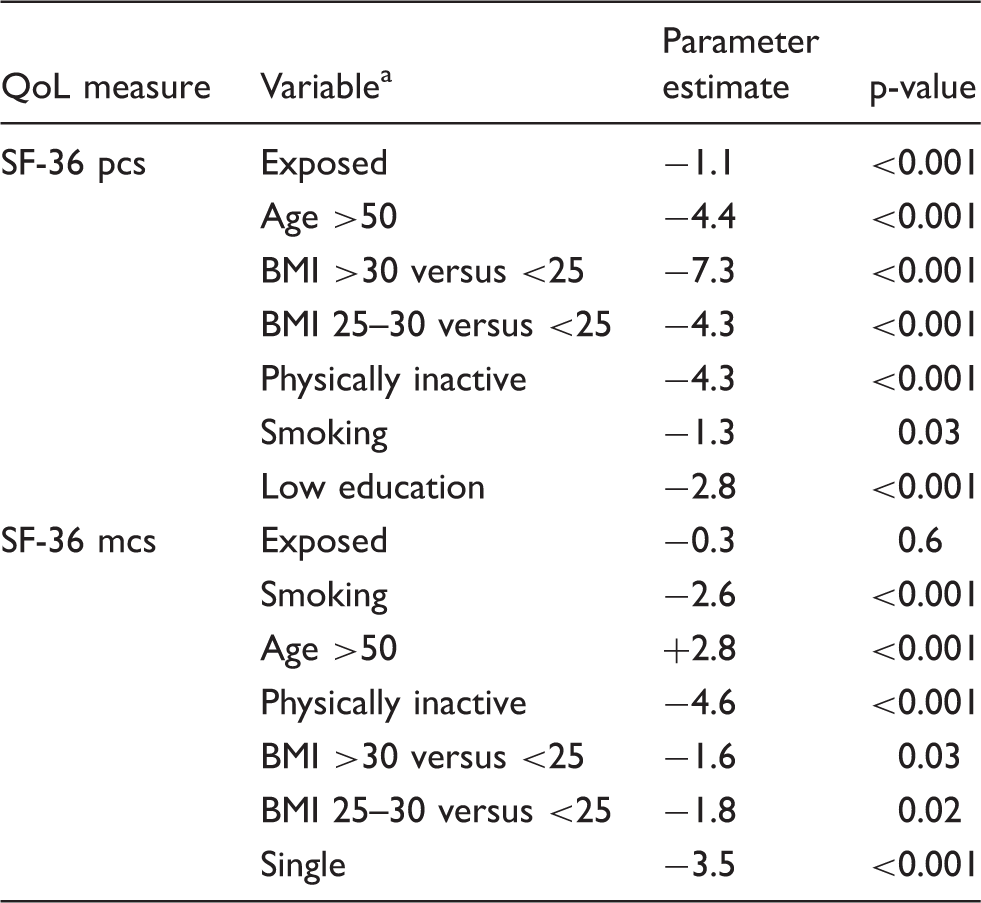
BMI: body mass index; mcs: mental component scale; pcs: physical component scale; QoL: quality of life; SF-36: 36-Item Short-Form Health Survey.
Variables included in the model: exposed/unexposed, age, BMI, physical activity, education, civil status, smoking.
Predictors of QoL in patients with VTE
Predictors of QoL in exposed women, multivariate.
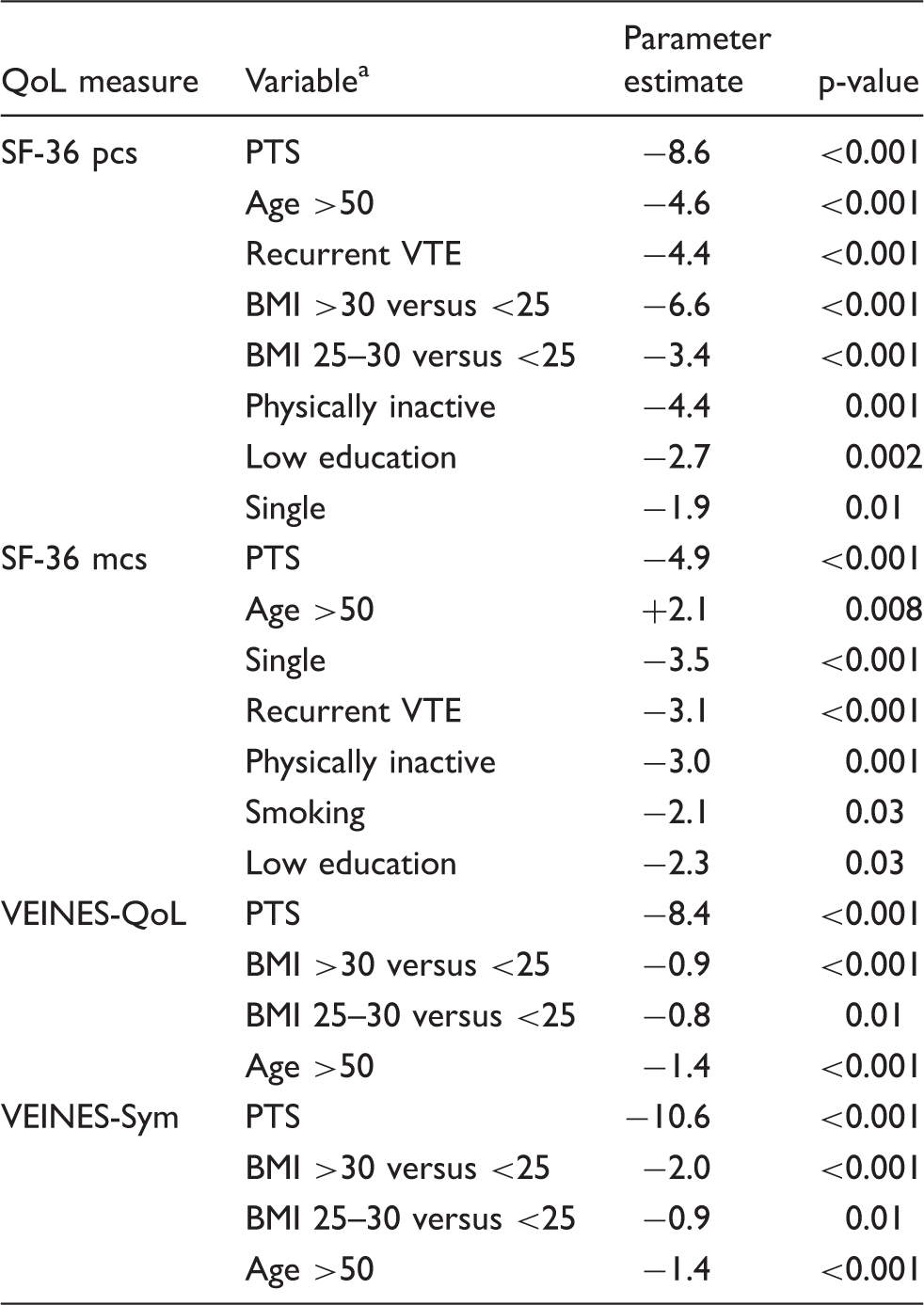
BMI: body mass index; mcs: mental component scale; pcs: physical component scale; PTS: postthrombotic syndrome; QoL: quality of life; SF-36: 36-Item Short-Form Health Survey; VTE: venous thromboembolism.
Variables included in the model: PTS, age, recurrent VTE, BMI, physical activity, education, civil status, smoking, provoked versus unprovoked VTE, and location of VTE (PE, proximal DVT, distal DVT).
PTS
Risk factors associated with postthrombotic syndrome in 1040 women after a first episode of VTE, presented as odds ratio (OR) and 95% confidence intervals (95% CI).

BMI: body mass index; DVT: deep vein thrombosis; VTE: venous thromboembolism.
Treatment with either combined hormonal contraceptives or menopausal hormone treatment.
Discussion
In this long-term follow-up study of Swedish women 18–64 years of age with a first episode of VTE and age-matched women without VTE, we found that on average there were no differences in QoL between the two groups. However, women developing self-reported PTS had markedly lower QoL compared to both unexposed women and exposed women without PTS, despite the location of the thrombosis. Our findings are consistent with previous studies reporting that occurrence of PTS is the predominant predictor of low QoL after DVT.1,3,6,22 Other factors affecting general physical health in our study were age, obesity, inactivity, and recurrent VTE. Women with recurrent VTE events had lower QoL even after adjusting for PTS.
In our study, QoL was not affected by having a proximal DVT, as opposed to a study by Kahn et al. 1 Even though our study had a larger number of study participant compared to the study by Kahn, the proportion of patients with proximal DVT was much lower. Despite a 90% power to detect a difference of 3 points in our study population, it might be that we missed significant associations of smaller magnitude.
To our knowledge there are few studies examining how QoL after VTE is affected by socioeconomic factors and physical activity. In one study from Norway 7 evaluating QoL after pregnancy-related DVT, low education was associated with having a higher risk of being among those with VEINES-QoL scores <25th percentile as compared with the ≥50th percentile. In TEHS follow-up, short education was associated with a small, but not clinically significant difference in mean SF-36 pcs and mcs, while VEINES-QoL was only affected by education in the univariate model.
Women reporting leg symptoms like pain, heaviness, and swollen legs prior to onset of VTE have in our study a threefold increased risk of PTS. Since there is no single gold standard objective test to diagnose PTS, the diagnosis is clinical. 23 The “International Society of Thrombosis and Haemostasis” recommends the Villalta scale to diagnose PTS. The Villalta scale comprises of five subjective symptoms and six objective signs. The symptoms and signs are not specific to PTS and could be due to primary venous insufficiency (PVI) rather than PTS. 24 Women in TEHS reporting leg symptoms prior to VTE might therefore be misdiagnosed with PTS at the time of follow-up rather than PVI. It might also be that these women have PVI prior to VTE and that venous insufficiency plays a role in the occurrence of PTS. A previous study comparing the Villalta score in the VTE leg and the contralateral leg has shown a strong correlation, suggesting it might be of clinical importance to evaluate the Villalta score in both legs to evaluate preexisting PVI. 25
The prevalence of PTS is low compared to other studies.10,13,24,26 The study included a large proportion of women with a distal DVT but analyzing only proximal DVT separately our result still shows a low prevalence of PTS. One explanation might be that the study population is young, since age has been found to be a risk factor for PTS in previous studies.13,26,27 Another risk factor that has been associated with PTS in one study is low quality of anticoagulant treatment. 22 The time in therapeutic range for patients treated with warfarin in Sweden is high compared to many other countries. 28
The strength of this study includes the large number of study participants, the long-term follow-up period, and the detailed information of lifestyle and socioeconomic factors. The cohort of TEHS follow-up is well defined and homogeneous with controls selected from the total population. We used both generic and disease-specific QoL instruments in exposed women being able to evaluate QoL comprehensively.
A few limitations have to be addressed. First, we used a modified Villalta scale to assess PTS. The scale has not been validated in our setting, but in the MEGA study the same modified scale was used and there was good correlation with the Villalta scale (kappa 0.88, 95% CI 0.79–0.96). 13 Studies from Norway validating modified Villalta scale found that patients usually overestimated their signs compared to professional health caregivers. 29 In our study, we used the Villalta scale only to assess whether women were developing PTS or not. We did not use it to grade severity of PTS. The prevalence of PTS is low compared to other studies and the reported Villalta points show good correlation with VEINES-QoL and VEINES-Sym points (Pearson correlation, r = 0.75). Another limitation is loss to follow-up. Women not accepting participation in the follow-up study are younger (mean age 44 versus 47 years for exposed and 44 versus 48 years for unexposed) and more often smokers (31% versus 25% for exposed and 28% versus 19% for unexposed) than participants. It should be noted though that the loss to follow-up was similar among exposed and unexposed women except slightly more married women among the exposed participated in the follow-up (73% versus 68% for exposed and 78% versus 77% for unexposed). More patient not accepting participation in TEHS follow-up were having a PE as primary VTE suggesting that the prevalence of PTS in the whole cohort might be overestimated. However, a sensitivity analysis stratified by location of thrombosis found no major difference in the risk estimates for the predictors of PTS.
The results may not be generalized to the whole population since the cohort only consists of young and middle-aged women.
In conclusion, we found that women who develop PTS after a first episode of VTE have severely impaired both generic and disease-specific QoL. On the other hand, women not developing PTS have similar QoL assessed with SF-36 compared to controls without VTE. Other predictors of low QoL were high BMI and lack of physical activity. To be able to improve QoL after an episode of VTE, it is important to find ways to prevent and treat PTS.
Footnotes
Acknowledgement
Thanks to Hans Järnbert Pettersson for support during statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TEHS was supported by unrestricted grants from Janssen-Cilag, Novartis, Organon, Schering, Wyeth, AFA Insurance, Center for Gender Medicine Karolinska Institutet and the Medical Products Agency. TEHS follow-up was supported by unrestricted grants from SSTH/Pfizer, SSTH/Leo Pharma, Stockholm County Council, Skandinaviska Forskningsstiftelsen för Åderbråck och andra Vensjukdomar and Insamlingsstiftelsen Kvinnor och Hälsa.
Ethical approval
Both at time of inclusion in TEHS as well as in TEHS follow-up the study participants gave their written informed consent according to the Helsinki Declaration. All women were informed that they at any time could leave the study and have their data destroyed. Both TEHS and TEHS follow-up were approved by the regional research ethics committees in Stockholm (KI 01-255, 04-469), Uppsala (Ups 01-277), Linköping (01-453), Göteborg (M088-01), Umeå (01-198), and for TEHS follow-up (EPN 2010/1200-31/1).
Contributorship
ML designed the follow-up study, collected the data, performed the statistical analyses, interpreted the data, and wrote the first draft of the manuscript. MH contributed to the design of the follow-up study and critically reviewed the manuscript. HK designed the original TEHS study and critically reviewed the manuscript. GL designed the follow-up study and critically reviewed the manuscript.
Guarantor
ML