
Abstract
Background
Portal vein aneurysms are rare dilations in the portal venous system, for which the etiology and pathophysiological consequences are poorly understood.
Method
We reviewed the existing literature as well as present a unique anecdotal case of a patient presenting with a very large portal vein aneurysm that was successfully managed conservatively and non-operatively without anticoagulation, with close follow-up and routine surveillance.
Result
The rising prevalence of abdominal imaging in clinical practice has increased rates of portal vein aneurysm detection. While asymptomatic aneurysms less than 3 cm can be clinically observed, surgical intervention may be necessary in large asymptomatic aneurysms (>3 cm) with or without thrombus, or small aneurysms with evidence of evolving mural thrombus formation on imaging.
Conclusion
Portal vein aneurysms present a diagnostic challenge for any surgeon, and the goal for surgical therapy is based on repairing the portal vein aneurysm, and if portal hypertension is present decompressing via surgically constructed shunts.
Introduction
Portal vein aneurysms (PVAs) are rare dilations in the portal venous system, with a reported prevalence of less than 0.5%.1,2 About 3% of these aneurysms occur in the venous vasculature, often extrahepatic in location, and in many cases, associated with different complications. 2 The complications, although variable, include thrombosis, rupture (either spontaneous or as a consequence of progressive aneurysmal dilation), portal hypertension, and in certain scenarios, compression of adjacent vessels or visceral structures.1,3 Despite the rise and improvement in abdominal imaging techniques in recent years to detect the presence of PVAs (either incidental or symptom based), the etiology and pathophysiological consequences of these aneurysms remain poorly understood. Moreover, management particularly of asymptomatic, large PVA, which are also extremely uncommon, remains unclear and varied. Here, we highlight a unique case of a 62-year-old man who presented with a very large, incidentally diagnosed, asymptomatic PVA, which was managed conservatively with routine surveillance. This report reviews the literature to assess current practice patterns and offer insight into treatment strategies for the management of PVA.
Case report
A 62-year-old male Veteran with a history of Parkinson's disease, hypertension, type II diabetes mellitus and prior alcohol use disorder who presented with a four-week history of vague right-sided back pain. He described the pain as sharp and shooting in nature, more severe in the lumbar region, and worsened by movement, especially when trying to push himself up from a chair or reaching for objects with his right hand. He otherwise denied any surgical history, fevers, lightheadedness or dizziness, shortness of breath, chest pain, abdominal pain, nausea, vomiting, diarrhea, dysuria, or any associated symptoms concerning for infection, trauma, portal hypertension, liver disease, or malignancy. Apart from his hypertension, which was well controlled, his vitals were within normal limits. His physical examination revealed mild right-sided paraspinal muscle tenderness but no associated bony deformities or point tenderness along his spine, as well as bradyphonia, resting tremor and shuffling gait, all baseline and attributable to his known Parkinson's disease. Workup involved a computed tomography (CT) of the abdomen with contrast, which was unremarkable except for an incidentally found aneurysm of the extrahepatic portal vein measuring approximately 5 cm in its greatest diameter, without any evidence of thrombus formation, or upstream intrahepatic portal vein dilation (Figure 1). There was mild fatty infiltration of the liver, but no evidence of cirrhosis, ascites, splenomegaly, bowel distension, hydronephrosis, or any obvious abnormalities in the pancreas or adrenal glands. All his labs, including liver function tests, were also within normal limits.
Representative computed tomography (CT) images demonstrating the size of the portal vein aneurysm and associated structures. (a) Axial images with adjacent vasculature and (b) coronal image demonstrating a well-circumscribed large aneurysm.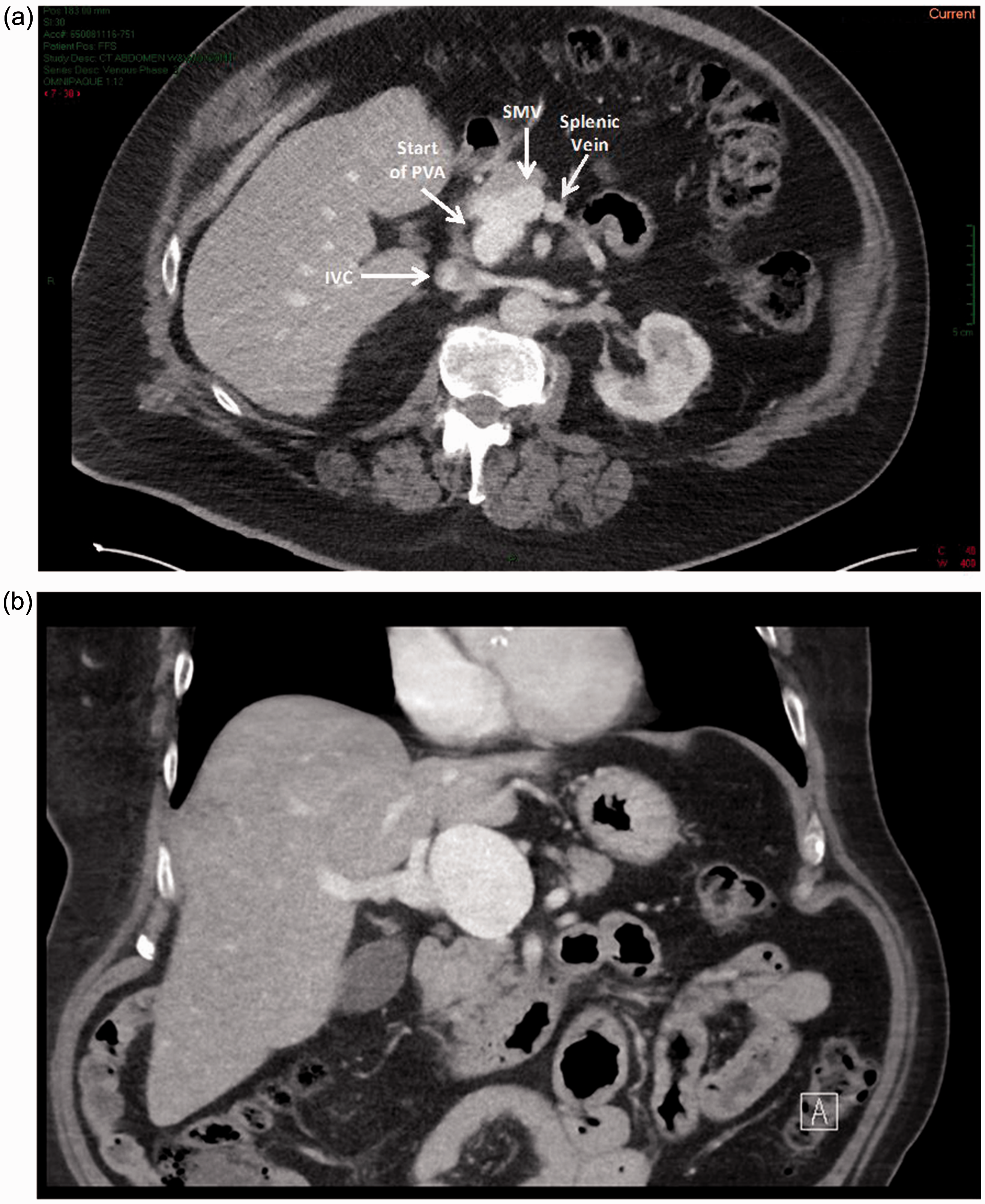
Given the patient's symptoms and the relative large diameter of the PVA, the patient was admitted for close monitoring and pain control. The patient remained hemodynamically stable with a relatively quick resolution of his back-pain symptoms. Although surgical options were considered during hospitalization, the spontaneous resolution of his symptoms more likely favored the etiology of the back pain to be musculoskeletal in nature rather than secondary to the aneurysm itself. The patient was eventually discharged after a short hospital course and without any anticoagulation treatment given his history of falls and at increased risk due to his Parkinson's disease. At three- and six-month follow-up, the patient remained asymptomatic with a stable PVA on imaging and no change in size.
Discussion
PVA are extremely rare, but present unique diagnostic and surgical challenges. These PVAs are generally characterized by portal vein dilatation greater than 20 mm in diameter, exceeding the normal 15 mm diameter of healthy individuals, and 19 mm average in cirrhotic patients. First described by Barzilai and Kleckner, 4 only about 200 cases of PVA have been reported in the literature.5,6 Our patient was unique, presenting with a very large, asymptomatic 50 mm extrahepatic PVA, incidentally found during a workup for vague back pain.
PVAs are distinguished by whether they are congenital or acquired, and intrahepatic or extrahepatic. Demographically, the mean age of diagnosis approximates to 52 years, and there appears to be no association with gender.2,5 Acquired PVA is most commonly seen in patients with cirrhosis or portal hypertension. However, in certain scenarios, there have been published reports of PVAs attributed to pancreatitis, prior abdominal surgery, trauma, infrequently due to progressive enlargement of a diverticular remnant of the vitelline vein, and hereditary hemorrhagic telangiectasias (Osler-Weber-Rendu syndrome), an autosomal dominant vascular disorder.2,5,7 While mycotic aneurysms and portal vein septic thrombophlebitis are common in the mesenteric vasculature, there is no known association to PVA that has been previously reported.8,9 Although poorly understood, we suspect that the absence of association may be due to the absence of septic physiology, age at presentation, and different pathophysiology.
Moreover, intrahepatic aneurysms are often found at vessel bifurcations, while extrahepatic dilatation frequently involves the main portal vein or the spleno-mesenteric venous junction, which accounts for about 3% of the aneurysms.1–3 A systematic review on 198 visceral venous aneurysms by Sfyroeras et al. 10 found that the extrahepatic portal vein is the most common site, with a prevalence of 26.2%, followed by the superior mesenteric-splenic venous confluence (18.6%).2,5
The primary presentation of portal vein aneurysm is extremely variable and can depend upon the size and related complications. These complications often include thrombosis, rupture, portal hypertension, and in certain scenarios, compression of adjacent vessels or visceral structures.1,3 Although quite uncommon, a minority of patients can present with gastrointestinal bleeding (7.3%). 10 The etiology of these symptoms is typically elucidated with ultrasound, CT scans or magnetic resonance angiography. 11 However, many PVA patients are asymptomatic and are incidentally discovered, as in our case. For instance, a review of 4186 consecutive patients who underwent abdominal CT scans found a 0.43% prevalence of PVAs with most patients (72%) being asymptomatic. Interestingly, four of the seven symptomatic patients with thrombosis secondary to PVA were noted to have underlying thrombophillic defect. While an association was difficult to determine, given the small sample size, the authors suspected that a thrombophillic defect probably played a role in the development of PVA thrombosis. Hence, these patients should be further investigated for underlying thrombophilia. 2 In contrast, a recent systematic review by Laurenzi et al. 5 reported that one-third of cases are usually asymptomatic (50% presented with abdominal pain). 5 Another study found the prevalence of incidentally discovered PVAs ranging between 25% and 38%. 10
Symptomatic or not, the etiology and pathophysiological consequences of these aneurysms remain poorly understood. Moreover, the optimal approach for the management of PVAs remains uncertain, with lack of clarity primarily over the indications and timing for surgery. Some clinicians propose medical management with either anticoagulation and/or close observation with or without beta-blocker therapy, although also controversial.10,12 Surgical intervention is employed to prevent severe complications including local compression, portal hypertension, or rupture, which carries a high mortality. The decision for operative repair is more easily justified in patients with clear symptoms related to the PVA, as opposed to incidentally found PVAs.
The goals for surgical therapy are to repair the PVA, and if portal hypertension is present, to decompress via surgically constructed shunts. 5 Open surgical procedures include aneurysmorrhaphy (in which the aneurysmal wall is laterally sutured, leaving it normal in size and contour), portocaval, or mesocaval shunt in the setting of portal hypertension, resection of the PVA and a polytetrafluoroethylene bypass, or vein graft interposition bypass. Lateral venorrhaphy and venous plication are also utilized in the surgical treatment. The choice of surgical reconstruction performed will depend on the anatomic location of the PVA and relative feasibility of the operation itself, with variable outcomes based on scattered case reports.5,10,13 In one large reported series of 40 patients who underwent surgery for symptomatic PVAs, the post-operative mortality was 17.5% over a median follow-up of 10.5 months. 5 Patients with portal hypertension and/or portal vein thrombosis are usually candidates for surgical bypass, either portocaval or mesocaval shunts to reduce portal pressures. 14 If thrombosis is present in the superior mesenteric and splenic veins, thrombectomy may be necessary. 14 In patients presenting with absence of portal hyptertension, an aneurysmorrhaphy procedure could be performed for an isolated lesion in order to preserve portal circulation flow while restoring laminar flow in the portal vein. In some cases, patch angioplasty could be considered if the relative integrity and size of the vessel wall is affected by the expanding aneurysm. The utility of endovascular approaches in the management of PVAs has not been reported. Although this technique is performed as a hybrid open and endovascular procedure, it could be employed potentially in high-risk patients if the anatomy is favorable.
Existing guidelines in this area of rare vascular pathologies encompassing PVAs remain unclear, so care must be individualized. Current guidelines recommend surgical intervention in cases of complicated PVA, i.e. with rupture, thrombosis, symptomatic aneurysms, or in patients presenting with progressively enlarging aneurysms and impending risk of spontaneous rupture. 5 While asymptomatic aneurysms less than 3 cm can be clinically observed, based on our institutional and surgeon experience, surgical intervention may be necessary in large asymptomatic aneurysms (>3 cm) with or without thrombus, or small aneurysms with evidence of evolving mural thrombus formation on imaging.10,13 In our case, even though the size of the aneurysm was significant (i.e. >5 cm), the patient's lack of symptoms, overall risk profile, and reassuring imaging findings on admission CT justified our decision for routine surveillance. We performed CT venograms at three and six months, and interval scans are planned every 6–12 months thereafter unless there were new symptoms or rapid expansion of the PVA, in which case the need for operative management would require reassessment.
PVA remains a diagnostic and management dilemma for any surgeon, with treatment options variable depending on the anatomy, presentation and existing co-morbidities of the patient. The timing and type of treatment itself are unclear, and often based on the relative judgment of the clinician as one weighs the relative risks of complications from the aneurysm to the overall morbidity of the procedure itself. Our patient was successfully managed conservatively and non-operatively without anticoagulation, with close follow-up and routine surveillance demonstrating a stable non-enlarging PVA.
Footnotes
Contributorship
SH and FR researched literature and conceived the study. SH and FR wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.