
Abstract
Objective
The aim of this study is to evaluate chronic venous disease symptoms by using the Venous Insufficiency Epidemiological and Economic Study-Quality of Life/Symptoms (VEINES-QoL/Sym) questionnaire in varicocele patients.
Material and methods
The study was designed as a prospective, case controlled study and conducted in four hospitals from Turkey. A total of 600 patients who admitted to urology outpatient clinic were enrolled to the study. After the exclusion of 44 patients who do not match the inclusion criteria, the remaining 556 patients were examined for the presence and grade of varicocele and subsequently examined clinically for the presence of chronic venous disease findings. Finally, patients were asked to answer the VEINES-Sym questionnaire consisting of 10 items. All patients’ demographic parameters, cardiovascular risk factors, other co-morbid diseases and drug usage were noted.
Results
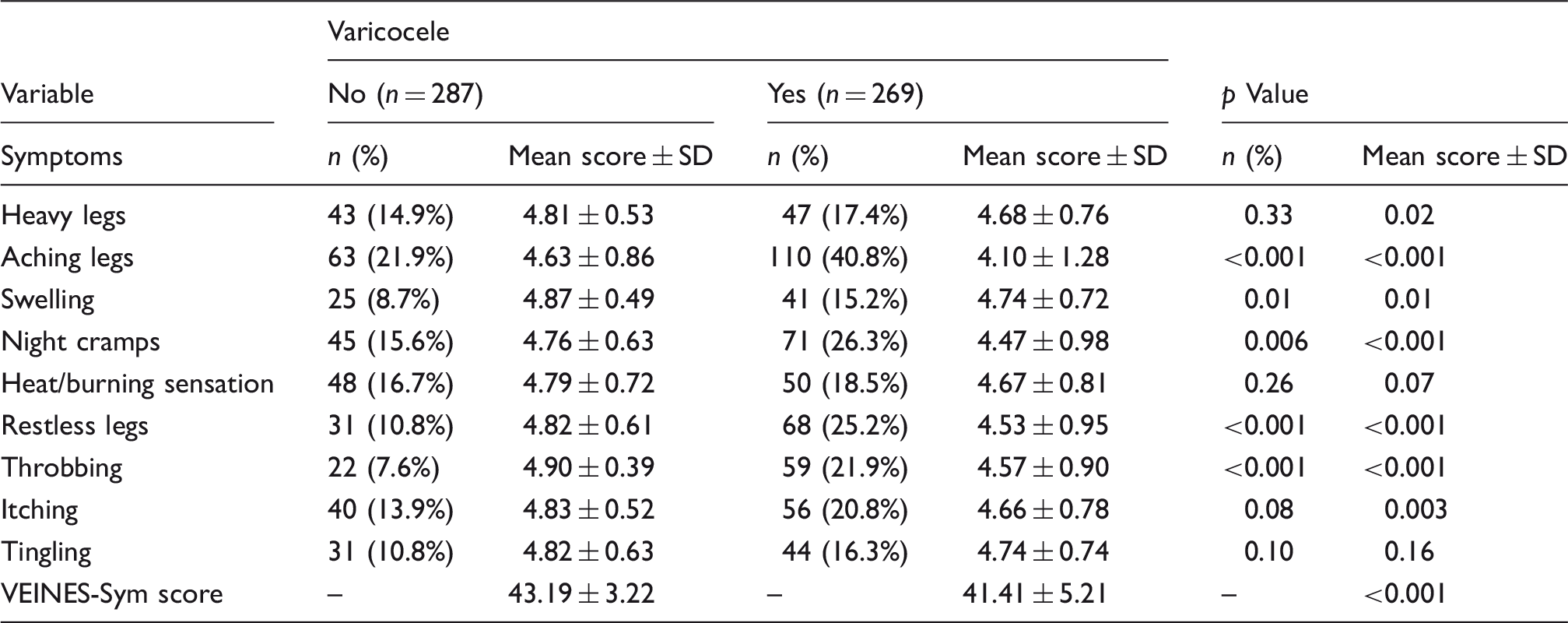
Patients were classified into two groups: varicocele (+) group (n = 269) and varicocele (−) group (n = 287). VEINES-Sym scores of varicocele patients were lower compared to patients without varicocele (41.41 ± 5.21, 43.19 ± 3.22, respectively, p < 0.001). Grades of varicocele significantly but inversely correlated with VEINES-Sym score (r = 0, −206, p = 0.001). Logistic regression analysis revealed that presence of varicocele irrespective of grading significantly and independently associated with the presence of aching (odds ratio: 2.054, 95% confidence interval: 1.265–3.338, p = 0.004) and throbbing (odds ratio: 2.586, 95% confidence interval: 1.353–4.943, p = 0.004).
Conclusion
Varicocele patients have lower VEINES-Sym scores compared to patients without varicocele and this finding is inversely correlated with the degree of the varicocele. This association supports the hypothesis that there may be a systemic vessel wall abnormality in venous disease patients. Patients with symptoms related to vascular dilatation in any territory may deserve to be assessed systematically with the support of further clinical studies.
Introduction
Chronic venous disease (CVD) is very common in the Western countries 1 and an important mortality and morbidity factor depending on the effected vascular region. 2 It is often overlooked by healthcare professionals due to the underestimation of the prevalence and impact of the disease. Besides, variations in clinical presentations of CVD contribute to underdiagnosis of the disease. It represents a spectrum of conditions varying from simple telangiectasia or reticular veins to skin fibrosis and venous ulceration. The main clinical characteristics are dilated veins, edema, leg pain, and cutaneous alterations in the legs. Varicose veins are dilating superficial veins, which become more tortuous and enlarged, continuously.2,3
Varicocele is defined as the dilatation, elongation and tortuosity of the scrotal portion of the internal spermatic venous system, which drains the testicle. 4 Its prevalence varies between 7% and 20% in healthy adolescents and young men and 75% and 90% of varicocele is left sided. It is associated with male infertility and it can be treated surgically. Diagnosis of varicocele can be made by physical examination easily. 5 Absence or deficiency of venous valves, increased venous pressure, and vascular wall pathologies are suspected pathophysiological mechanisms for varicocele formation. 2
Besides affecting the morbidity and mortality, CVD have an impact on the life quality of patients suffering from the disease, which can be measured with quality-of-life (QoL) reports. These questionnaires are important for the clinicians to evaluate the symptom severity, its impacts on daily life and response to treatment.1,6 Venous Insufficiency Epidemiological and Economic Study-Quality of Life/Symptoms (VEINES-QoL/Sym) questionnaire is patient based, designed for self-completion instrument to measure both the symptom severity and quality of life. VEINES-QOL measures life quality and VEINES-Sym provides an overall estimate of CVD symptom frequency. Lower VEINES-Sym scores indicate more severe symptoms and higher VEINES-QoL/Sym scores indicate better QoL.7,8
Recently, chronic venous diseases such as varicocele and varicose veins have been defined as ‘Dilating venous diseases’ by Yetkin et al. due to the fact that they have similar pathophysiological mechanisms. 2 Besides, presence of peripheral varicose veins was shown to be associated with varicocele in a study published by Kılıç et al., previously. 5 However, CVD symptoms, which are also included in the VEINES-Sym questionnaire, have never been evaluated in varicocele patients. In this context, in this study we have aimed to investigate the CVD symptoms in varicocele patients.
Materials and methods
Study design
This study was designed as a prospective, case controlled study. The study consisted of patients admitted in the urology clinic with varying complaints between June 2015 and October 2016. The patients were enrolled to the study in four clinics in Turkey: Başkent University Ankara Hospital, Başkent University Konya Hospital, Private Malatya Gözde Hospital, Private Batman Dünya Hospital.
The Ethics Committee of Başkent University Faculty of Medicine approved the study protocol (KA15/297). All study procedures were conducted according to the principles of Good Clinical Practice and Helsinki Declaration. Written informed consent was obtained from the patients who accepted to participate in the study.
Study population
The study group consisted of 600 consecutive patients who admitted the outpatient urology clinic with any symptom regardless of associated with varicocele. The main inclusion criterion was the willingness of patients to be involved in the study. Exclusion criteria were the history of malignancy, active infection or drug usage for infection at the time of enrollment, hematological disease, collagen tissue disease, history of heart failure, atrial fibrillation, history of a respiratory disease, rheumatic disease, history of lower extremity orthopedic disease/surgery and elephantiasis. The flow chart diagram of the study including exclusion criteria is also shown in Figure 1.
Flow-chart diagram of the study.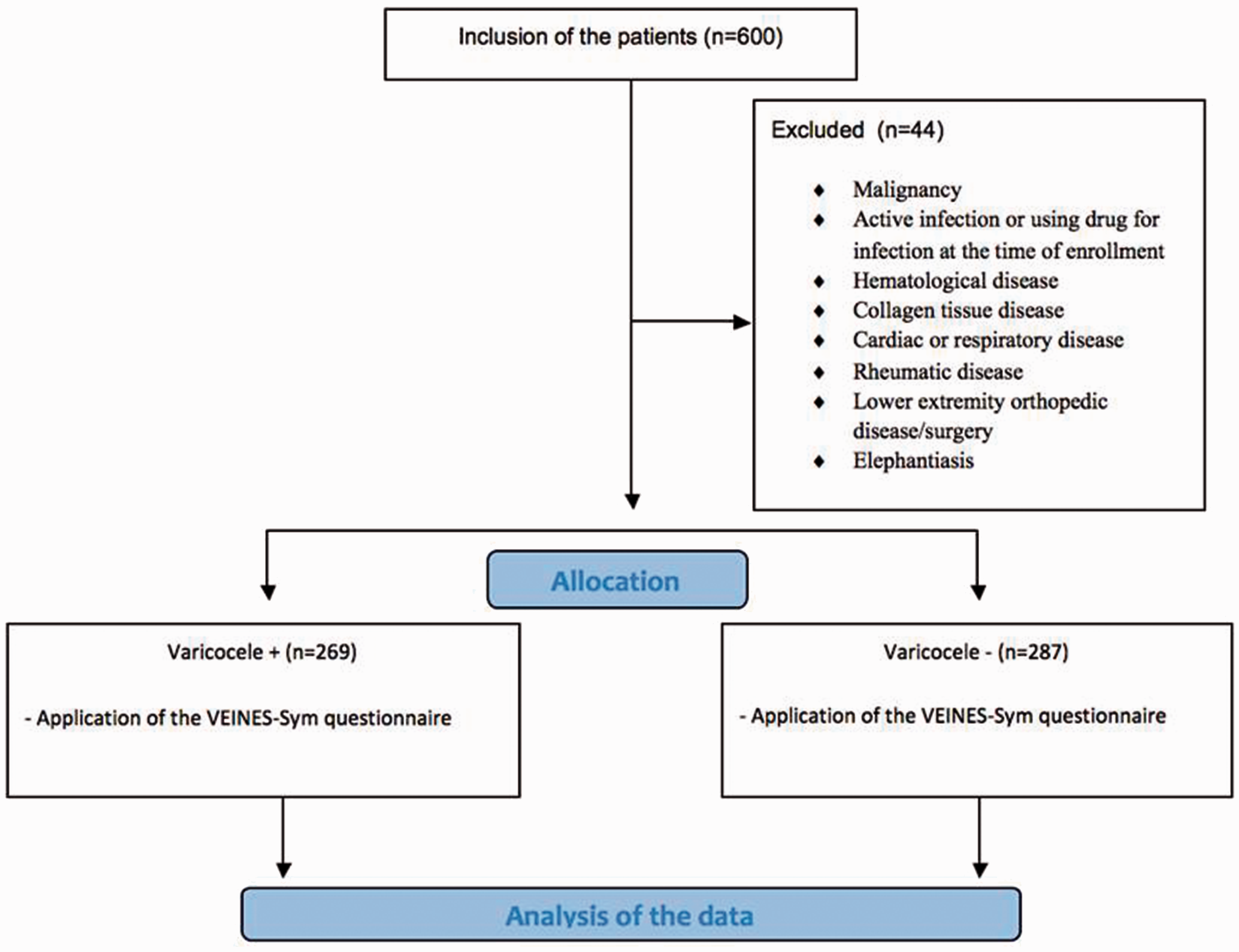
Physical examination of the patients
All the patients included in the study were examined for the presence of varicocele by an experienced urologist in each clinic. Patients were examined in a warm room after a 5-min resting. The scrotum was examined with palpation and each spermatic cord in the supine and upright positions with and without the Valsalva maneuver. The varicocele was graded according to the Dubin and Amelar system: Grade 1, varicocele palpable only during the Valsalva maneuver; grade 2, varicocele palpable in standing position; and grade 3, varicocele detectable by visual scrutiny alone. 9
The patients were then examined clinically for lower extremity venous system according to CVD guidelines and categorized according to clinical component of CEAP (clinical, etiological, anatomical and pathological) classification as follows: grade 0, no visible signs of venous disease; grade 1, telangiectasias or reticular veins; grade 2, varicose veins; grade 3, edema; grade 4, skin changes due to CVD; grade 5, skin changes with healed ulceration; and grade 6, skin changes with active ulceration. 10 Patients with CEAP ≥ 2 were considered as positive for the peripheral varicose vein. All patients’ demographic parameters, cardiovascular risk factors, venous diseases, occlusive diseases and drug usage were recorded on our database. Duplex ultrasonography for the assessment of CVD and ultrasonographic grading of varicocele were not performed in all patients due to design of study. On the other hand, further ultrasonographic evaluation of varicocele was performed when clinically needed in selected patients. Finally, patients were asked to answer the VEINES-Sym questionnaire. VEINES-Sym consists of 10 items including nine venous symptoms (heavy legs, aching legs, swelling, night cramps, heat/burning sensation, restless legs, throbbing, itching and tingling sensation) in five different frequencies (1 = everyday, 2 = several times a week, 3 = about once a week, 4 = less than once a week, 5 = never). The tenth question concerning at what time of the day these symptoms are most intense is not included in calculation and is only used for descriptive information. Kutlu and her colleagues studied the validity and reliability of the VEINES-QoL/Sym questionnaire in the Turkish population. 7
Statistical analysis
All statistical analyses were performed using SPSS version 16.0 (SPSS, Inc., Chicago, IL, USA). Categorical variables were determined as counts and percentages and compared between the groups using the chi-squared test. Continuous variables were expressed as mean value ± standard deviation for parametric variables. The Kolmogorov–Smirnov test was applied for the assessment of normality. Differences between the means were compared by unpaired t-test when the continuous variables showed normal distribution or by the Mann–Whitney U-test when they did not. Relationship between the varicocele grade and VEINES-Sym score was tested by Spearman’s correlation analysis. One-way ANOVA and post-hoc Bonferroni test was performed to compare the VEINES-Sym scores according to the grade of varicocele. Logistic regression analysis was applied to identify the possible association of venous leg symptoms and mean VEINES-Sym scores with varicocele. All of the venous leg symptoms mentioned in the VEINES-Sym questionnaire were included in the regression analysis. Two-tailed p < 0.05 was considered as statistically significant in all tests.
Results
A total of 600 consecutive male patients who admitted to the urology clinic were enrolled in the study prospectively. Among them, 44 patients who do not match the inclusion criteria were excluded from the analysis. Patients were classified into two groups: Varicocele (+) group (n = 269) and varicocele (−) group (n = 287).
Baseline demographics, clinical characteristics and admission complaints of the study population.

Symptom evaluation and VEINES-Sym score assessment of the study population.
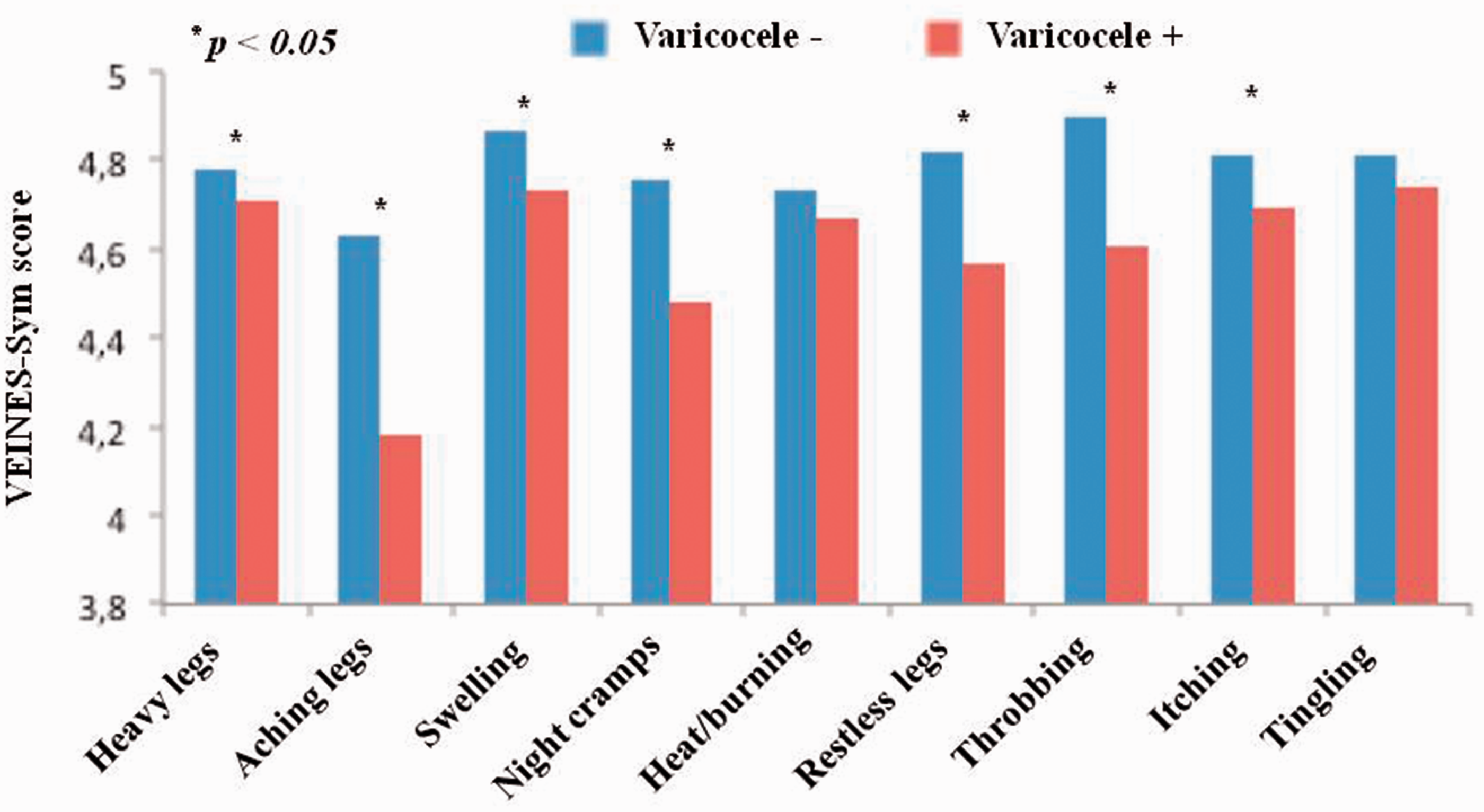
Mean VEINES-Sym score of symptoms in patients with and without varicocele. Lower VEINES-Sym scores indicate more severe symptoms.
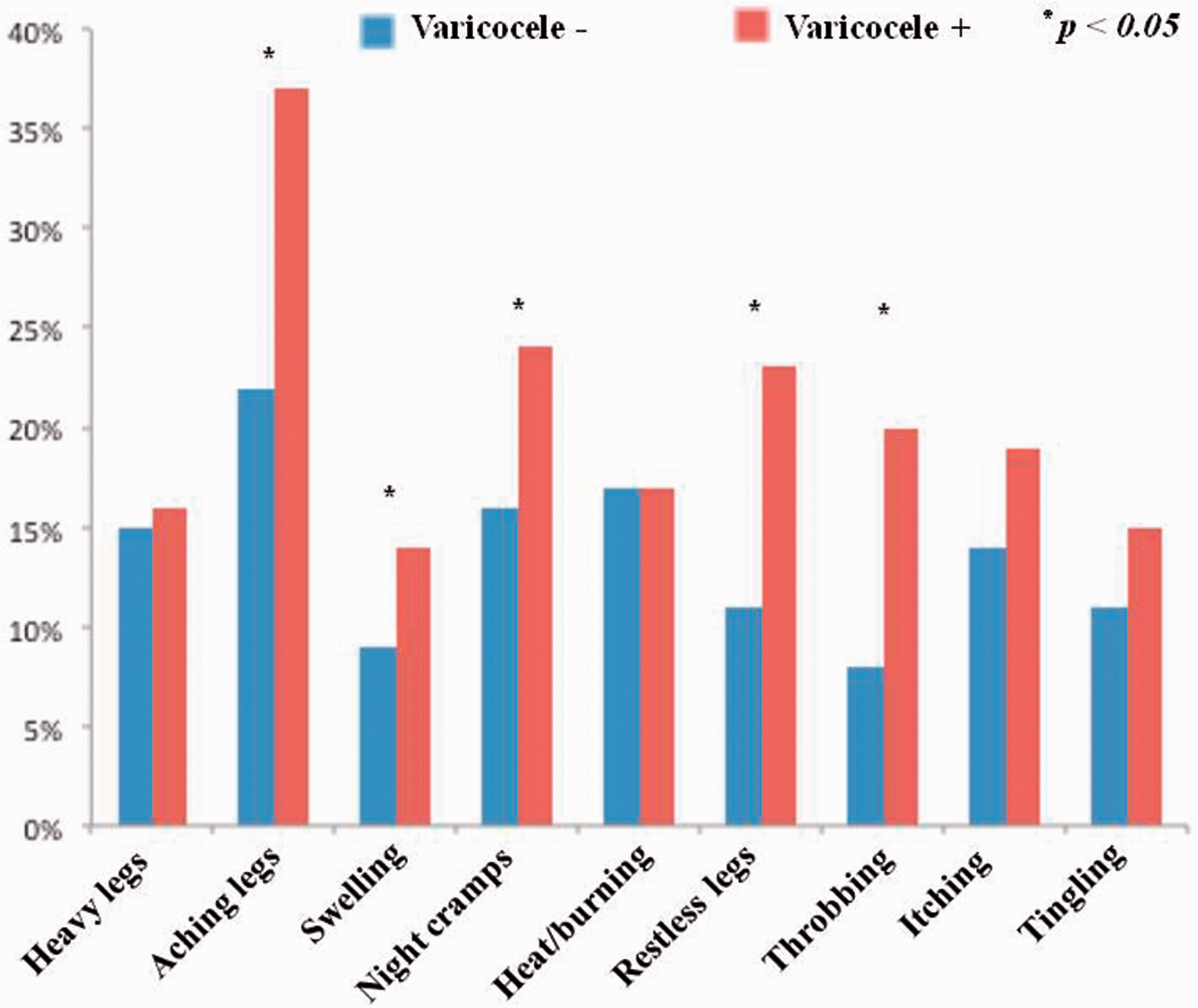
Proportion of patient reported symptoms among patients with and without varicocele.
Variance analysis of symptoms regarding the grade of varicocele.
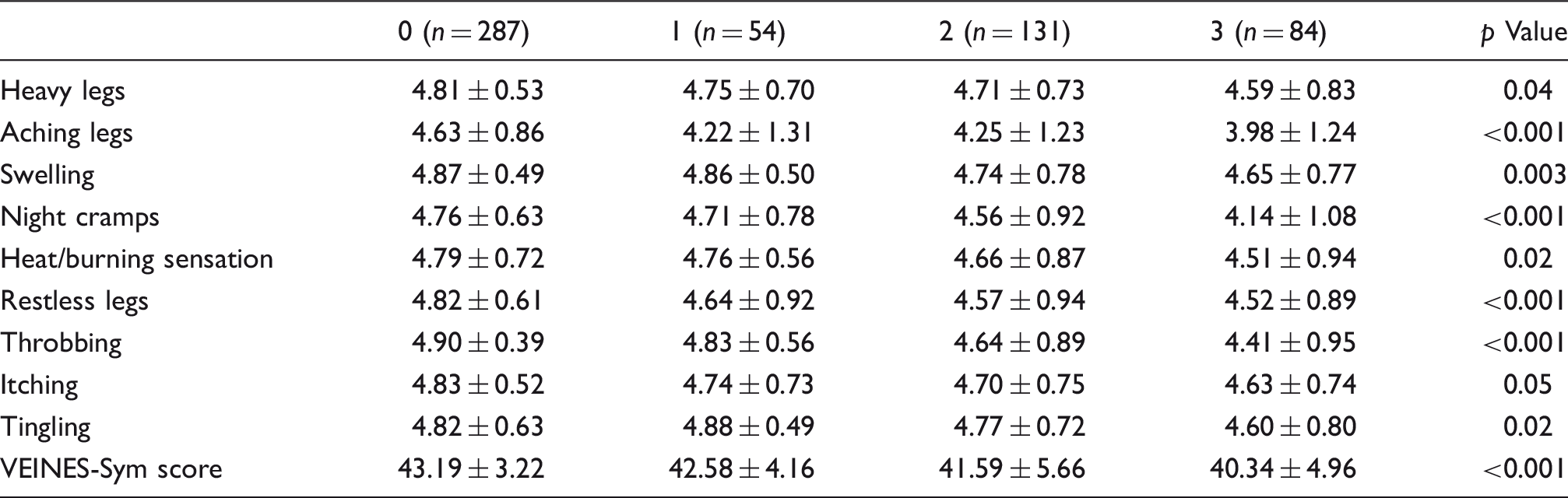

Error bar graphic of VEINES-Sym score of patients without varicocele and patients with different grades of varicocele. “r” represents the correlation coefficient between the VEINES-Sym scores and varicocele grades.
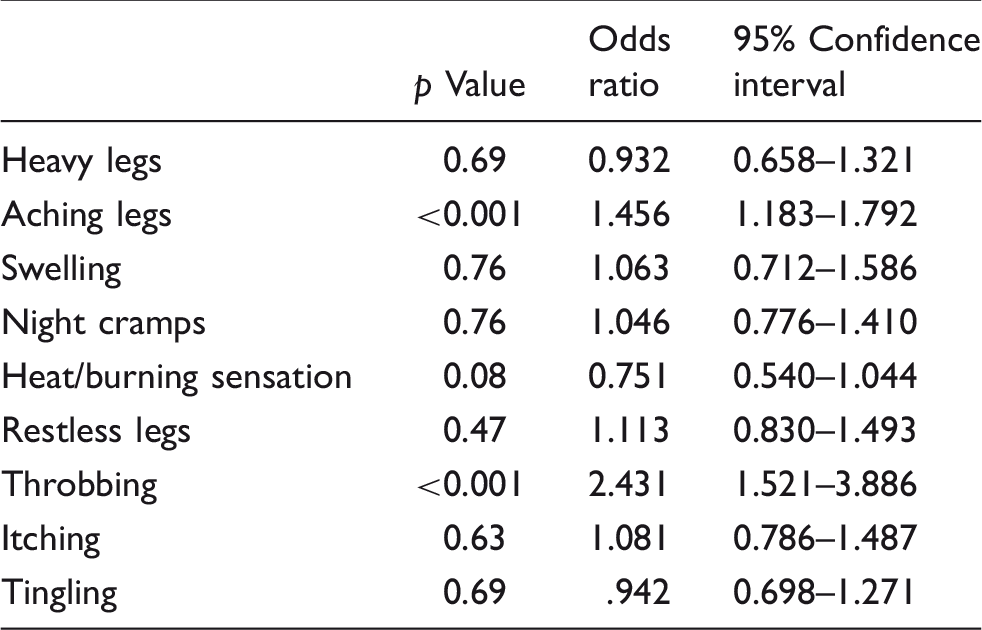
Logistic regression analysis of venous leg symptoms for varicocele.

Logistic regression analysis of VEINES-Sym scores for the presence of varicocele.
Discussion
To the best of our knowledge, this is the first study in the literature evaluating the CVD symptoms with VEINES-Sym questionnaire in varicocele patients. In the present study, we have demonstrated for the first time that score is significantly low in patients with varicocele and independently associated with the presence of varicocele. Besides, we have shown that varicocele grade significantly correlated with the VEINES-Sym score.
CVD is a widespread but overlooked problem of lower extremity veins and is frequently linked with varicose veins. 3 The spectrum of CVD ranges from varicose veins to leg edema and serious skin changes such as hyper-pigmentation, eczema, lipodermatosclerosis, and venous ulceration. 11 In the Western populations, the prevalence of varicose veins varies between 25% and 33% in females and 10–20% in males.2,12 CVD is a very common problem affecting the Western adult population with a prevalence of up to 57% and 77% in men and women, respectively. It may also be associated with other clinical manifestations.12–15 Symptoms of varicose vein patients vary between aching, burning, pain, cramps, heaviness, swelling, throbbing, tiredness, leg ulcers, tightness, and ecchymosis.6,8,16,17 Interestingly, ecchymosis has been shown to be a sign of varicose vein and associated with muscle cramps. 18 Aging, female gender, race differences, pregnancy, family history, obesity, limited physical activity, prolong standing, genetic and chromosomal abnormalities are traditional risk factors.3,19 Although various mechanisms have been proposed, the main mechanism causing varicose vein and CVD is not fully understood. Varicocele, which is a life debilitating disease and associated with male infertility, is abnormal dilatation of the veins within the scrotum and shares similar pathophysiological mechanisms with varicose veins. 2 Besides having similar pathogenetic mechanisms, a high coexistence of these diseases was shown, previously. In their study, Kılıç et al. showed that the prevalence of peripheral varicose veins in patients suffering from varicocele is significantly higher than patients without varicocele. 5 In our study, we have found a symptomatic association between these two diseases, which was also related with the degree of the disease. Although prevalence of CVD is lower in male patients regarding the female counterpart, significant association of VEINES-Sym score with varicocele in our case control study underlines the common pathophysiological mechanism on two distinct vascular territories.
Venous diseases which were proven to share similar pathophysiological mechanisms such as peripheral varicose veins, varicocele, hemorrhoids, and pelvic congestion syndrome have been named as ‘Dilating venous diseases’ by Yetkin et al., recently. 2 Besides, it is known from previous reports that there is a close linkage between these diseases. Sakamoto found that men with bilateral varicoceles have increased mean diameter, and peak retrograde and antegrade flow velocity in the prostatic venous plexus. 20 Besides, Holdstock et al. found that there is a frequent association between pelvic vein varices and hemorrhoids. 21 Kilciler et al. reported an association between varicocele and hemorrhoids. 22 According to these reports, it is reasonable to suggest that dilating venous diseases are closely linked to each other and venous reflux or dilatation of the venous vessels in different vascular systems might have originated from a systemic vascular wall pathology rather than being a local disease.2,23 Surprisingly, similar association has also been demonstrated between dilating venous and arterial vessel diseases. This association has been demonstrated between coronary artery ectasia and varicocele, 24 and coronary artery ectasia and varicose veins 25 in previous studies. In light of these studies, we can speculate that venous reflux or dilatation in various vascular regions share a common pathogenetic mechanism, which causes all vessels prone to dilate or reflux.
VEINES-QoL/Sym questionnaire measures the effect of CVD on the life quality of patients and is currently the most appropriate and applicable choice for patient evaluation. It is the only self-reported test that covers the whole spectrum of patients’ considerations about leg-related venous disease, varying in a wide spectrum from uncomplicated varicose vein dilatations to deep venous thrombosis. Its psychometric and statistical characteristics seem to be scientific for translation to various demographic environments. VEINES-QoL provides an overall prediction of QoL, and the VEINES-Sym gives information about symptom frequency. 26 Therefore, the validity and reliability of this questionnaire in varicose vein and CVD patients has been studied in different countries.7,27,28 However, symptoms, which are also present in this questionnaire, have not been studied in varicocele patients previously. Due to the fact that VEINES-Sym is the most extensive and complete questionnaire on symptom type and frequency, 26 we have preferred to apply this questionnaire in our study. Even so, there are some contrary reports about the feasibility of VEINES-Sym questionnaire in some studies. Van der Velden et al. found that existence of venous symptoms was slightly more often in CVD patients but the difference was small and statistically non-significant. They concluded that symptoms, which are present in VEINES-Sym questionnaire, are less specific for patients suffering from CVD and refluxing veins than is usually thought and the VEINES-QOL/Sym questionnaire is not suitable to use as a diagnostic or screening tool. 29
CVD represents a wide spectrum of clinical conditions depending on the effected vascular region.2,3 Therefore, symptoms of these patients and clinical presentations may vary. In some studies, it has been concluded that patient-reported lower limb symptoms are not specific to CVD. The Bonn Vein Study, which is a population-based trial, indicated that 62.1% of women and 49.1% of men complained from leg symptoms; however, only 27.8% of men and 34.1% of women had CVD above clinical classification C2 and only 35.3% had pathological reflux in the duplex sonographic examination. 30 According to the results of the Edinburgh Vein Study, only certain lower limb symptoms such as swelling, cramps, itching in men, and aching and cramps in women were related to the venous reflux on duplex ultrasound examination. The authors concluded that using duplex ultrasound scanning is not suitable to identify the patients with real venous symptoms. 31 In our study, the percentage of patients suffering from aching, swelling, night cramps, restless legs, and throbbing were found to be higher and mean VEINES-Sym score of these symptoms was found to be significantly lower in varicocele patients. In addition, as previously demonstrated by Kılıç and his colleguaes, 5 frequency of patients with peripheral varicose vein was higher in varicocele patients compared to patient group without varicocele. However, such an association was not observed in terms of hemorrhoids in our study. We think this contrary result originates from insufficient patient reports. Due to the fact that this is a symptom-based study, we did not perform rectal examination to the patients. Moreover, independent association between varicocele grade and VEINES-Sym has been documented. On the other hand, it is difficult to make a conclusive or definite pathophysiological statement on the causal relationship between the varicocele and CVD. This clinical and symptomatical association between the varicocele and CVD underlines the presence of population who are prone to dilate due to vascular wall abnormality. Since considerable number of patients without varicocele has also CVD and leg symptoms in our study, contributing factors3,19 such as race differences, family history, obesity, limited physical activity, prolong standing, genetic and chromosomal abnormalities should also be considered in the pathophysiologic course and presentation of venous diseases. Likewise, hip pain due to pelvic venous reflux has been described without leg varicose veins. 32 Additionally, any superficial venous reflux without clear clinical signs and non-saphenous leg vein reflux from sources including the pelvic veins32,33 might have led us to overlook the diagnosis of CVD.
The present study has a few limitations. First, due to the fact that this is a symptom and clinical examination-based study, we did not perform ultrasonographic examination in our study population. Since we did not examine the patients with venous duplex ultrasound, silent superficial venous reflux without any clinical signs might have been missed. Second, our patient group comprised partially younger patients. So these results cannot be attributed to older populations.
In conclusion, we have demonstrated for the first time that varicocele patients have lower VEINES-Sym scores compared to patients without varicocele and this is inversely correlated with the degree of the varicocele. This association supports the hypothesis that there may be a systemic vessel wall abnormality in venous disease patients and warrants further studies to elucidate the pathophysiologic mechanisms. Patients with symptoms related to vascular dilatation in any territory may deserve to be assessed systematically with the support of further clinical studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Vascular and Molecular Cardiology Society.
Ethical approval
The study protocol was approved by The Ethics Committee of Baskent University Faculty of Medicine.
Guarantor
EY.
Authors’ contributions
SO, KTA, EY, SK, LP, MI, IT contributed to the conception and design; EY, KTA, SK, TC, LP, IT, AG, OA, MI were involved in acquisition, analysis and interpretation of data; SO, EY, KTA, TC, LP, IT, AG, SK, OA, MI, EY were involved in drafting the article; SO, EY, LP, IT, KTA, TC, MI were involved in revising it critically for important intellectual content.
Acknowledgements
We would like to thank Ebru Kayadelen for her skillful help on collecting and editing data of patients enrolled in the study.