
Abstract
Objective
In the Ziekenhuisgroep Twente Hospital, nurses from two community care organizations were trained to visit patients at home and provide adequate ulcer care. Furthermore, the one-stop clinic was introduced to set a diagnosis and treatment plan at the first visit in the hospital. The purpose of this study was to (a) evaluate if there is a difference in time to wound healing for patients with UCV treated by dedicated nurses compared to treatment by nurses in the Dermatology outpatient clinic and (b) determine if the one-stop clinic setting would lead to a difference in time to wound healing compared to the standard way of care.
Methods
In this retrospective cohort study, all files of patients with an ulcer in the Dermatology department of ZGT between 1 June 2010 and 1 June 2015 were studied.
Results
Out of a total of 385 new patients with an ulcer, 97 cases were included. Patients who were treated by dedicated nurses were significantly older (p = 0.002) and had larger wounds (p = 0.008). Age was not significantly related to time for wound closure (HR 0.99; 95% CI: 0.97–1.01, p = 0.226). After adjustment for confounders, there was no significant difference in time to wound closure between dedicated nurses (2.2 months (1.4–3.0)) versus hospital care (2.3 months (2.1–2.6)) (HR 1.01; 95% CI: 0.61–1.67, p = 0.961). The one-stop clinic led to a statistically shorter time to closure of the wound (1.8 versus 2.7 standard way of care, p = 0.007).
Conclusions
Time to wound closure is not statistically different between patients treated by dedicated nurses compared to hospital care when adjusted for the effects of the one-stop clinic. The one-stop clinic gives a significant better chance for faster time to wound closure controlled for both groups.
Introduction
Background
An ulcus cruris venosum (UCV) is the most prevalent cause of a leg ulcer. German studies show that the prevalence of general ulcer cruris in the general population is 1% and in individuals older than 80 years is between 4% and 5%. 1 Women are about three times more at risk of getting an ulcer compared to men. 2 Besides having an older age, there are other risk factors for UCV, which include varicose veins, vein abnormalities, multiple pregnancies, obesity, previous leg injuries (trauma), phlebitis, surgery and deep venous thrombosis (DVT). 3 Leg ulcers can be divided into categories such as venous, arterial and venous-arterial, also known as mixed ulcers. 4 The majority of lower limb ulcers are caused by venous disease. Some ulcers can be caused by trauma, skin malignancies, inflammatory skin diseases (e.g. Necrobiosis lipoidica, scratch wounds by eczema), infections (e.g. bullous erysipelas) and other factors. The Lothian and Forth Valley Study showed that among 600 patients with ulcer cruris, 76% were caused by venous disease and 22% by arterial disease. 5 Concerning the mechanism of ulceration, or in other words the process of ulceration, pericapillary fibrin cuff formation, trapping of white blood cells and growth factors have been proposed as possible mechanisms of ulcerations. 6 Venous ulcers can cause various symptoms: pain, itching, heaviness, leg-tiredness, cramps, burning and swelling. 7 Ulcers are debilitating and painful and can greatly reduce patients’ quality of life. 4 Ulcer healing has been shown to restore the quality of life. 4
The number of patients with UCV is increasing because of growing life expectancy and while more people develop obesity with its side effects. Moreover, since patients visit a hospital when the wound does not heal after a period of time, it is important to set the correct diagnosis as soon as possible. By setting a correct diagnosis, proper treatment can take place, resulting in a shorter time to wound healing and simultaneously cost reduction is expected.
Most patients with UCV are elderly, which requires significant effort for them to make frequent visits to the hospital. The dermatologists of the Ziekenhuisgroep Twente (ZGT) Hospital, i.e. Hengelo and Almelo, and the community care organizations Carintreggeland and ZorgAccent came up with a plan to train nurses of community care organizations with Dermatology department nurses who daily practice the wound care at the outpatient clinic of the Dermatology department in the ZGT. A Canadian study from 2011 already showed that the organization of care rather than the location or way of care delivery is more important. 8 This is why we trained the nurses the same method of wound care as in the hospital. This collaboration was implemented by the Dermatology department of the ZGT.
These trained community care nurses (dedicated nurses) visit the ulcer patients at home and give appropriate wound care and if necessary compression therapy. Patients can now be treated at home which makes the need for visits to the hospital no longer necessary. The quality of care is similar between care in a hospital setting and community care by dedicated nurses, but only if the care is well organized.8,9 Furthermore, at the ZGT, the one-stop clinic was introduced for faster diagnosis and identifying which patients could be treated at home rather than within the hospital setting. In one visit, the medical history, physical examination and additional (vascular) examinations are performed. After this and still during the first visit, the diagnosis and the individual ulcer treatment plan are made. This new method is unique in the Netherlands. Although not much evidence is available about this subject yet, we suspect that patients prefer care within their homes, and that through this approach (including faster diagnosis), wounds would heal faster and therefore makes this approach more cost-efficient.
Objectives
We performed this retrospective study to investigate if there is a difference in time to wound healing for patients with UCV treated by dedicated nurses compared to treatment by nurses in a Dermatology outpatient clinic. Another aim of this study was to assess if the one-stop clinic (faster diagnosis) leads to a faster time to wound closure.
Diagnosis of ulcer cruris in the ZGT
Besides the medical history and physical examination, additional examination will be performed. The tests which are used for the evaluation of the vascular functions are the ankle-brachial pressure index (ABPI), duplex ultrasound and on indication toe brachial index (TBI).
Diagnosis for superficial venosum reflux is available because of the duplex ultrasound scanning, which is the golden standard for accurate evaluation of the highest point of valve failure and extent of reflux.10,11 That is the best way to confirm or exclude the presence of venous dysfunction. Duplex can determine whether the deep veins or the greater or lesser saphenous veins and their tributaries are dilated, congested or incompetent. It can also detect the presence of incompetent perforating veins and if the problem is caused by anatomical obstruction, reflux or both. 12 Venous incompetence was identified by reverse flow lasting >0.5 s following the release of firm calf compression. 13 In the ZGT, the most common tools for diagnosing ulcers are medical history, physical examination and vascular examination such as Duplex scanning, ABPI and TBI. Laboratory tests are sometimes performed as well, which could include blood testing or cultures.
The ABPI is the ratio of the systolic blood pressure measured at the ankle to that measured at the brachial artery. 14 However, the ABPI may not always be reliable, particularly in patients with diabetes where vascular calcification can prevent arterial compression and falsely increase arterial systolic pressure and therefore the ABPI. 15 The ABPI may thus be confounded in diabetic patients, because of calcification of the arteries. In that case, the TBI can be performed. 15
After gathering all this information, the dermatologist makes a diagnosis/differential diagnosis. Sometimes additional tests are needed, for instance skin biopsy, blood samples and culture samples.
Methods of treatment for UCV
Treatment of patients with UCV is either conservative (compression therapy) or also with flebous intervention. In general, the goals of treatment are to reduce oedema, improve ulcer healing and prevent recurrence. 12 With appropriate treatment, most of these ulcers will heal within three to four months. 16
Compression therapy
Compression therapy aims to increase venous and lymphatic return, reducing oedema and venous pressure in the limb, by the application of an external force. Compression therapy is the standard care for venous ulcers. 17 Compression treatment increases the healing of ulcers compared with no compression. More ulcers were healed with high compression systems than with low compression systems, 18 but should only be used in the absence of significant arterial disease. No clear differences in the effectiveness of different types of compression systems (multilayer and short stretch bandages) have been shown. A meta-analysis showed that adequate compression therapy is not only important for the healing of venous insufficiency and ulcers but that continuing the compression after the ulcer has healed is also critical for the recurrence-free interval. 19
In addition to compression therapy, education is also important for both the healing process and to prevent recurrence, i.e. to inform the patient about the ulcer, the healing time and the importance of the treatments. 20 In addition to the UCV protocol, the patient is advised about their lifestyle: prevent immobility, stimulate to use the muscle calf pump, prevent obesity and discourage smoking. 21
(Venous) treatments
Different techniques are available in the ZGT, including ‘foam’-sclerotherapy, endovenous radiofrequent ablation for the incompetent veins and ambulant phlebectomy according to Muller. 22
Wound care and wound care materials
No level 1 evidence is available that any wound dressing confers specific benefit over another. 12 In the ZGT, alginate dressings, hydrofibres, hydrocolloids, hydrogels, wound edge protectors, foam and silver, paraffin and silicon dressings were used.
Ulcer care ZGT
The care path of patients with UCV before implementation of the dedicated nurses and the one-stop clinic is illustrated in Figure 1. This method led to delay while the appointments and additional tests took place on different days during the process, often within one week.

Old method. More visits were needed before a diagnosis was made. The patient receives care in the hospital. Additional tests took place on different day and patients had to come back to the outpatient clinic for the results. ABPI: ankle-brachial pressure index; TBI: toe brachial index; VNUS: endovenous radiofrequent ablation; ZGT: Ziekenhuisgroep Twente.
Until the year 2014, ZGT Almelo was using this ‘old method,’ and until the year 2004, ZGT Hengelo was using this ‘old method’. The old method is the procedure in which venous ulcer care in the Netherlands in most Dermatology departments is structured and therefore representative for the standard care of venous ulcer care.
Patients with UCV first went to the general practitioner (GP). If the wound did not heal, or when the GP had doubt about the diagnosis, the patient was referred to the hospital. After multiple outpatient visits, the diagnosis can be made (see Figure 1). After the diagnosis, a treatment plan was prepared by the dermatologist. After this, the patient has to visit the hospital each time for the treatment and care of the ulcer wound by the dermatologist (nurse).
ZGT introduction of the one-stop clinic and the dedicated nurses
The new method might be more time-saving by doing the different kinds of examinations and making the treatment plan during the first consult in the hospital. This is expected to save time because of fewer necessary consultations and thereby also less waiting time compared with the old method.
One-stop clinic
Since 1997, the Dermatology outpatient clinic of ZGT cooperates with nurses who are dedicated in taking care of ulcer patients. Since the year 2014 during the first consultation at the hospital, every ulcer patient receives a medical history, physical examination, additional examination, i.e. duplex ultrasound and ABPI and on indication TBI, laboratory tests and/or biopsy. After performing this, the diagnosis and the individual ulcer treatment plan are made. Information about the patient is (after informed consent is secured) exchanged with the dedicated nurses. Then information about the ulcer is given to the patient and a letter about the current state of the patient, the ulcer and the treatment plan is sent to the GP. Figure 2 illustrates the one-stop clinic in more detail.
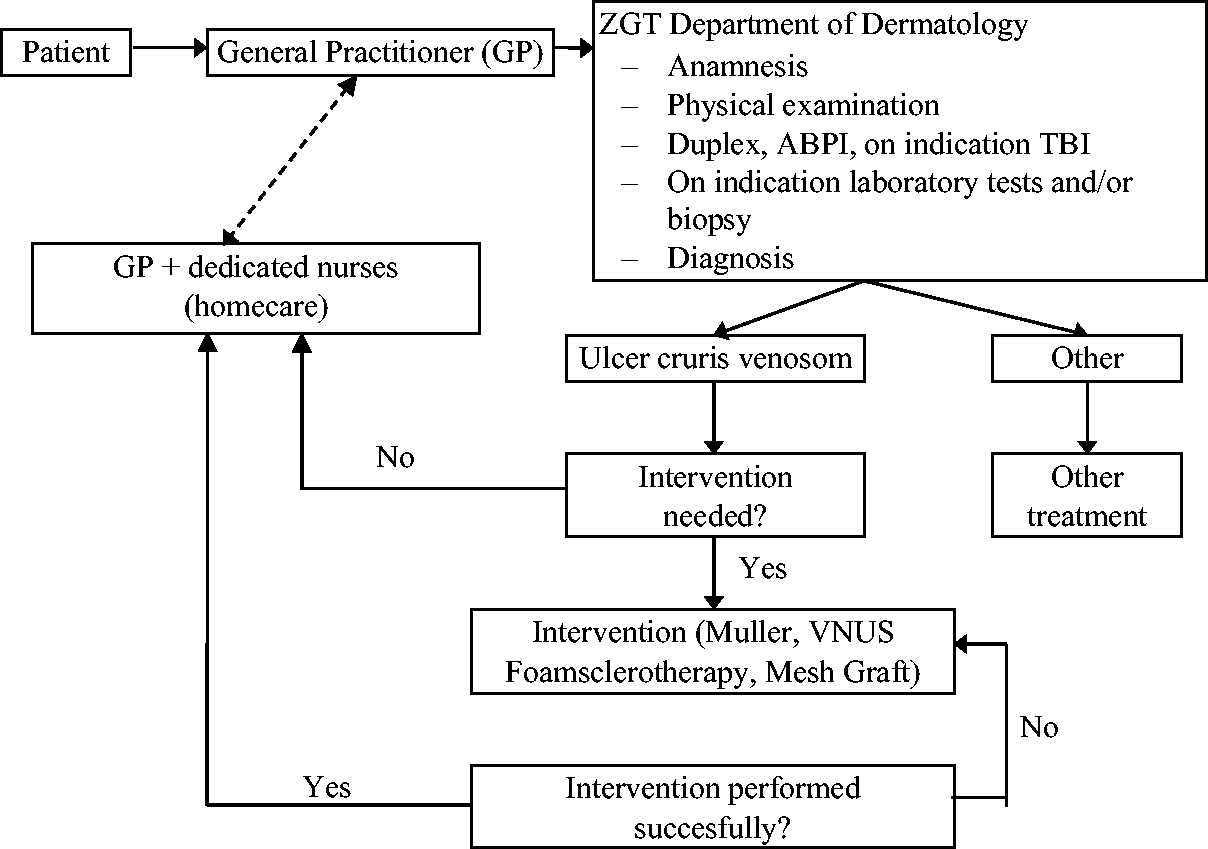
Overview of the one-stop clinic. During the ‘First consult’, the anamneses, physical examination, vascular research and the diagnosis are performed in one day. Sometimes, when laboratory test and biopsy are taken, the diagnosis comes later. ABPI: ankle-brachial pressure index; GP: general practitioner; TBI: toe brachial index; VNUS: endovenous radiofrequent ablation; ZGT: Ziekenhuisgroep Twente.
If the diagnosis during the first consult in the hospital shows that the ulcer is of venous origin, then two options of treatment are possible:
The nurse team with a dedicated nurse
Specific education and qualification requirements are required for a nurse to become a dedicated nurse.
The education requirements are:
To become a certified dedicated wound nurse, a nurse must follow a training that consists of eight sessions with an experienced dedicated nurse and two sessions at the ZGT with a dermatology nurse of the ZGT and with the dermatologist. Also the nurse must receive three sessions of theoretical training: two sessions (accredited by the dedicated nurse) and one session phlebological education by a dermatologist. The team of nurses is trained twice a year by a dedicated nurse (for ulcers) from Carintreggeland and once a year at an education course by a dermatologist of ZGT. The team has to participate two times a year in patient discussions. The education level of a nurse (for treating ulcers) must at least be level four of the secondary vocational education. The dedicated nurses must spend at least 10 hours a week on ulcer treatment and/or compression therapy.
The dedicated nurse in practice
Dedicated nurses are especially trained to treat ulcer patients with wound care and compression therapy. Because of these dedicated nurses, the ulcer patients do not have to go to the hospital to be taken care of, but instead these dedicated ulcer nurses go to the patients’ home. Usually a dedicated nurse visits the patients at home twice a week, but if necessary more often. The dedicated ulcer nurses have close communication with the dermatologist and nurses in the ZGT and with the GP. The nurses of ZGT, dedicated nurses of Carintreggeland and ZorgAccent cooperate together and use the same type of wound material to bind and clean the wound. So when in a case a nurse from Carintreggeland has to take over from a nurse from ZorgAccent or vice versa, then this can be done without problems. Also currently there is more economical use of wound materials. As an example, previously leg bandages would be used once and then they would be thrown away. Nowadays wound bandages can be washed and reused again for two or three times. Furthermore, the nurses also work according to the same guidelines, such as the way to bind wounds and which wound products to use. They also report their data according to standardized dossier compilation.
Summary of the advantage of one-stop clinic and the dedicated nurses
In summary, the advantage of the one-stop clinic and the dedicated nurses team in comparison to the old method of care is that the total care path from the beginning till the end takes less time, there is better communication between the nurses, there are special working guidelines and standardized medical records compilation for reporting data and there is more economical use of wound care products.
Research questions
The following are the aims of this study:
Is the time to wound healing for patients with UCV faster with the deployment of dermatologist nurses in the hospital compared to treatment by dedicated nurses? Does the one-stop clinic (faster diagnosis) lead to a faster time to wound closure?
Methods
Study design
This research study is a retrospective cohort study.
Setting
All the files of patients in the Dermatology department of ZGT in Almelo and Hengelo between 1 June 2010 and 1 June 2015 examined with a leg ulcer were studied. All cases were evaluated by one physician. After this, 385 patients were selected (see Figure 3).

Patient selection. UCV: ulcer cruris venosum; GP: general practitioner.
Participants
Patients were included when they had UCV and were 18 years or older. All ulcer sizes were included. Of patients with an ulcer on both legs, the largest ulcer was included for analysis.
Exclusion criteria were patients with other causes of leg ulcer, e.g. arterial leg ulcers, ulcer of Martorell, livedo vasculopathy, mixed ulcer: ulcer has both arterial and venous cause. Furthermore, patients with an ankle pressure <60 mm Hg and other causes of ulcers that did not have only a venous cause were excluded. Also patients under the age of 18 and also mentally disabled patients (for example dementia) were not included in the research study. Patients with multiple episodes of UCV were excluded. Other exclusion criteria were patients treated by family/GP or other community care organizations after visiting the ZGT.
Study variables
All files were searched and the following variables were identified: patient number, sex, date of birth, date of first visit, age at first visit, number of visits to the hospital, number of visits to a certain caretaker, ulcer side, ulcer size, type of ZGT method, type of treatment, state of closure of the wound, date of wound closure, first and last date of community care, number of treatments by community care and number of dedicated nurses at home. No differentiation was made between post thrombotic and superficial venous insufficiency.
Patient groups
The patients were assigned to groups based on clinical decision. The following are the group of patients belonging to different kind of ‘care methods’:
Patients who were treated via the one-stop clinic and treated with the dedicated nurses (One-stop+DDN) (New method) Patients who were treated oat the one-stop clinic and were treated only in the ZGT; therefore, no participation of the dedicated nurses (one-stop+ZGT) (Transitional phase old and new method) Patients who were not treated at the one-stop clinic, but by the dedicated nurses (no one-stop+DDN) (Transitional phase old and new method) Patients who were not treated at the one-stop clinic and were treated only in the ZGT (no one-stop+ZGT) (Old method)
To compare dedicated nurses to ulcer care in the hospital, we combined groups 1 and 3 and groups 2 and 4 due to small group sizes. Due to small group sizes, we combined groups 1 and 3, named DDN and groups 2 and 4, named ZGT.
Primary outcome variables
The first primary outcome variable is time to wound healing for patients with UCV treated by dedicated nurses compared to treatment by nurses in a hospital setting. The second primary outcome is the time to wound closure in patients treated via the one-stop clinic compared to treatment without the one-stop clinic pathway.
Statistical methods
Continuous variables are expressed as mean with standard deviation (SD) or median with interquartile range (IQR); categorical variables as counts with corresponding percentages.
Difference in baseline characteristics between groups was tested using independent t-test or Mann-Whitney U test (continuous variables) or chi-square (categorical). We analysed time to wound healing by Kaplan–Meier survival curves.
We used univariate and multivariate Cox proportional hazard regression models to establish the relationship of treatment (ZGT vs. DDN and one-stop clinic vs. no one-stop clinic) with time to wound healing.
Baseline characteristics that showed significant differences between groups were further analysed using univariate Cox proportional hazard regression to explore potential confounding effects on the relation between treatment group and time to wound healing. A p value of 0.150 or lower was included in the multivariate Cox regression model.
Results
Patient characteristics
Of the total 345 cases, 97 cases were included for analysis: group 1: n = 26 (male 12), group 2: n = 16 (male 8), group 3: n = 23 (male 8) and group 4: n = 32 (male 15). To compare dedicated nurses to ulcer care in the hospital, we combined groups 1 and 3, named DDN, and groups 2 and 4, named ZGT, due to small group sizes. From here, we will use DDN group and ZGT group.
Of these 97 cases (male n = 43, female n = 45) with median age 70.6 years (interquartile range 23.7, minimum 30.4, maximum 93.6 years), the median ulcer size was 2.0 cm2 (interquartile range 3.5 cm2, minimum 0.01 cm-165.0 cm) and the median time to wound closure was 2.4 months (95% CI 1.9–2.9 months).
Baseline characteristics of all initial groups are shown in Table 1. We combined the groups and compared them using descriptive statistics. These results are shown in Table 2. Patients treated by dedicated nurses were significantly older (p = 0.002) and had larger wounds (p = 0.008) compared to the ZGT group.
Baseline characteristics of the initial groups.

Male; F: female; IQR: Interquartile range; DDN: Dedicated dermatology nurse; ZGT: Ziekenhuisgroep Twente; 95 CI: 95% Confidence interval.. * The size of the wound was not known in all patients.
Descriptive data of the combined groups (1 + 3 and 2 + 4).
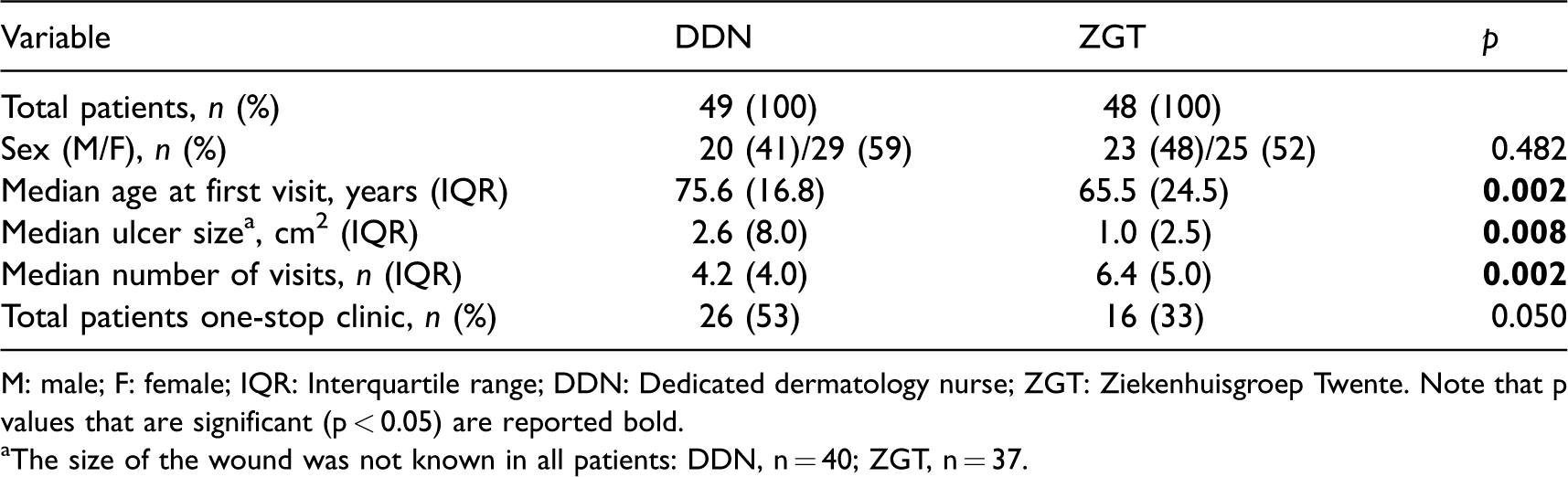
M: male; F: female; IQR: Interquartile range; DDN: Dedicated dermatology nurse; ZGT: Ziekenhuisgroep Twente. Note that p values that are significant (p < 0.05) are reported bold.
aThe size of the wound was not known in all patients: DDN, n = 40; ZGT, n = 37.
Primary results
The median time to wound closure in the Kaplan–Meier analysis was 2.2 (95% CI 1.4–3.0) months in the DDN group and 2.3 (95% CI 2.1–2.7) months in the ZGT group (p = 0.620). This was not a statistical difference. Survival analysis is shown in Figure 4.

Kaplan–Meier curve of survival in patients with UCV till wound closure. DDN consists of initial group 1 and 3 a ZGT consists of the initial group 2 and 4 (see ‘Methods’). ZGT: Ziekenhuisgroep Twente; DDN: dedicated dermatology nurse.
Treatment via the one-stop clinic led to a statistically shorter time to wound closure. No one-stop clinic had a median time to wound closure of 2.7 (95% CI 2.1–3.3) months versus a median time to wound healing of 1.8 (95% CI 1.4–2.6) months in the one-stop clinic (p = 0.007). After Cox regression analysis, this led to a greater chance of wound closure in patients treated via the one-stop clinic (HR 2.0; 95% CI 1.2–3.3, p = 0.008).
Secondary results
The median time to wound closure was 2.3 months, when no venous intervention occurred, with venous intervention, also 2.3 months.
The median time for wound healing was not statistically different between patients who had a venous intervention (p = 0.621) and patients without any of these interventional treatments.
There was no significant difference between both groups (DDN vs. ZGT) in the number of venous/mesh graft treatments (p = 0.476).We did not observe any confounding effect of the number of invasive treatment influencing the time of healing (p = 0.545) Regardless of number of treatment there was no confounding effect of invasive treatment on the time to wound closure (p = 0.356). Neither was age at first visit a confounder of time to wound healing (p = 0.358).
After adjustment for confounding factors at the one-stop clinic and ulcer size we did not find significant difference in chance of wound closure between dedicated nurses versus hospital care (HR 1.07; 95% CI: 0.6-2.0, p = 0.841) in the multivariate regression analysis. The one-stop clinic was significantly related to greater chance of wound closure (HR 2.36; 95% CI: 1.3--4.3, p = 0.005). Size of ulcer was not related to increased chance of wound closure (HR 1.0; 95% CI: 0.9--1.0, p = 0.255. Results ar listed in Table 3. The purpose of this first retrospective study was to investigate if there is difference in effectiveness in terms of timesaving: time to wound healing for patients with UCV treated by dedicated nurses compared to treatment by nurses in a hospital setting.
Multivariate regression analysis for time to wound closure.
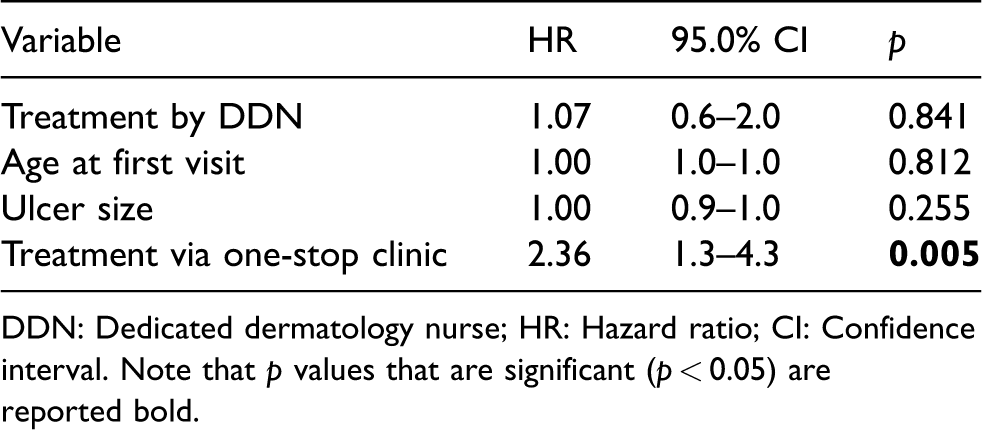
DDN: Dedicated dermatology nurse; HR: Hazard ratio; CI: Confidence interval. Note that p values that are significant (p < 0.05) are reported bold.
The answer to this question is that there was no difference in time to wound healing between these two groups; i.e. time to wound closure was not statistically different between patients treated by dedicated nurse compared to hospital care when adjusted for confounders.
The patients who were treated by dedicated nurses were significantly older and had larger wounds. This last finding is interesting, while Margolis et al. 23 reported already that ulcers of ≤6 month’s duration and ≤5 cm2 in area that are treated with compression are highly likely to heal within 24 weeks. Conversely, ulcers of >6 months’ duration and >5 cm2 in area are unlikely to heal within 24 weeks.
Overall, these patients were often not treated with venous intervention, due to comorbidity. Age at first visit and the size of the wounds did not confound results to wound closure time.
In conclusion, there was no significant difference in the time to wound healing between those treated by the dedicated nurses and the experienced nurses in the hospital.
The second purpose of this study was to examine if the one-stop clinic leads to faster time to wound closure.
In this retrospective study, we found that the one-stop clinic gives a significant shorter time to wound closure. This might be explained by the fact that while during the first visit to this one-stop clinic, duplex and arterial investigations were performed; sometimes, additional laboratory testing and a biopsy were needed. In the past, the additional tests were not always performed or these tests were performed when the ulcer did not heal in a short period of time. Because of this, there was some delay in the proper wound treatment. Nowadays, the correct diagnosis can mostly be stated during first visit, so the correct treatment is given directly.
The median time to wound healing was not statistically different between patients who had a venous intervention or mesh graft and patients without any of these treatments.
Discussion
Key results
The first outcome of this study is the effectivity in terms of timesaving: Is the time to wound healing for patients with UCV treated by dedicated nurses shorter, longer or equal compared to treatment by nurses in a hospital setting? This study showed that the time to wound closure is not statistically different between patients treated by dedicated nurses compared to hospital care when adjusted for the effects of the one-stop clinic. This finding is interesting. Most patients were old, for whom we assume it could be difficult to go to a hospital. Care inside their own homes gives more relief for the patients. Since there was no difference in time to wound closure, this suggests that the care can safely be arranged by dedicated nurses, which could be a benefit for these patients. We did observe a significant increased risk in faster time to wound healing in patients treated via the one-stop clinic, controlled for size of wound ulcer and group (dedicated nurse home treatment vs. in-hospital treatment).
Strengths
Between 1 June 2010 and 1 June 2015, 385 patients with a new ulcer were seen in the hospital. Only 140 out of 385 patients had a true UCV. The reason of this would be the strict inclusion criteria that were applied. Only patients with a single ulcer cruris venosum were included, and any underlying comorbidity as arterial dysfunction or diabetic mellitus was excluded.
Limitations
The biggest limitation is the study design. There are a lot of limitations, for example retrospective studies may need very large sample sizes for rare outcomes. 24 It is very difficult to make accurate comparisons between the groups and researchers cannot control exposure or outcome assessment, and instead must rely on others for accurate record keeping.
Also in this retrospective study, e.g. retrospective chart review, several known variables for ulcer healing were not taken into account.25,26 We did not perform research about the socio-economic differences in the groups. We did not know the chronicity of the wound before patients presented at the clinic. 23
This is a major predictive factor in ulcer healing and so a limitation of our study. Also in 15 cases, patients had multiple episodes of an ulcer, and these cases were excluded; however, we did not take into account the effect of this history of ulcer in the time to wound closure. This could have influenced the total time of healing in the investigated patients.
Because of the diverse pathways of care patients were classified to, four different patient groups were formed. This has led to the small sample sizes, making it difficult to compare groups and interpreting outcomes. Since the old method was not used at the moment of inclusion, these groups would not expand. Therefore, we chose to combine groups.
The whole cohort consisted of patients with a proven venous aetiology of the ulcer. Therefore we can not apply the outcome of the one-stop clinic to every patient with an ulcer, as every patient with an ulcer is nowadays seen via the one-stop clinic. In our cohort patients with multiple or reoccur ulcers were also excluded. Since ulcers have a great tendency to reoccur, this group is not an optimal reflection of the realistic population. These selection bias should been taken into account before generalizing the outcomes to all ulcer patients.
Our second primary outcome was time to ulcer healing in the one-stop clinic versus no one-stop clinic. This applies only for patients with proven venous insufficiency as a consequence of the ulcer. Therefore, we cannot apply the outcome of the one-stop clinic to every patient with an ulcer, as every patient with an ulcer is nowadays seen via the one-stop clinic. This selection bias has been taken into account before generalizing the outcomes to all ulcer patients.
Analysing the size of the wound was done by estimating the wounds on sight of previously taken pictures since in many cases a tape-measure was not used. Since the wound size was only measured two dimensionally, consequently the depth of the wound was not taken into account. However, since all wounds were assessed by the same physician, inter-observer variability was minimized.
Besides the time to wound healing, we planned to identify the cost-effectiveness in patients treated in the setting of hospital care, community care organizations and dedicated nurses. Information such as number of visits, the amount of wound dressings that were used, the number of times gauze was switched and the time (dedicated) nurses spent at the patients home would all be gathered. However, while the information systems of the community care organization were not yet equipped to collect such data, the information was not documented correctly in the records and was therefore limited. Consequently, in this retrospective study, we could not analyse these data accurately. In our daily practice, we find that dedicated nurses, through their extensive knowledge, are much more cost-effective on materials such as gauze, bandages and wound dressings. Identification of the costs of ulcers treated by dedicated nurses compared to the old method would allow health care workers and organizations to be more cost-efficient in the ulcer care. The total cost of ulcer care should be targeted for further research in an extensive multi-centre trial. This way a reduction of costs in ulcer care could be achieved.
We assume that people are more satisfied while receiving treatment at home. However, patient satisfaction has not been addressed in this study and future studies should examine the impact of preference of patients of the way of care on outcome. Furthermore, due to cost-efficiency in the health care nowadays, patients would see a lot of different nurses treating their wounds. In most cases where dedicated nurses were the main therapist, they would be the only one treating each patient. This could increase the patient satisfaction. We therefore suggest further research that includes patient satisfaction, preference of treatment and quality of life.
Interpretation
This kind of study had not been previously performed. To our knowledge this is the first study that shows that a one-stop clinic for ulcer cruris patients is very valuable. First, the one-stop clinic gives a significant better chance for faster time to wound closure for patients with a solitary venous ulcer, because a proper diagnosis is made and a correct treatment can be started directly. We expect this will result in lower costs for these ulcer treatments. Secondly by means of dedicated nurses, the treatment can be arranged at home as good as in the hospital, which must be a benefit for the mostly older patients. However, we suggest further research in a trial with a larger cohort with an intention to treat method since this would better reflect the realistic pathways and treatments of all ulcer patients.
Conclusion
The number of patients with an ulcer cruris venosum (UCV) is increasing and this mostly affects older people. The disease is often chronic and it has a large impact on the quality of life of patients. The wound healing process is a popular topic which has been studied extensively. In the Ziekenhuisgroep Twente (ZGT) Hospital, we have set up a new way of treating UCV. Nurses of the Dermatology department of the hospital who daily practice wound care trained a limited number of nurses from two community care organizations. These trained dedicated nurses then supplied proper ulcer care at home. Furthermore, the one-stop clinic was introduced at the outpatient clinic of the Dermatology department. In one visit, the medical history, physical examination, additional (vascular) examinations are performed. After this and still during the first visit, the diagnosis and the individual ulcer treatment plan are made. This new method is unique in the Netherlands. The purpose of our study was to evaluate if there is a difference in time for wound healing for patients with UCV treated by dedicated nurses compared to treatment by nurses in the Dermatology outpatient Clinic. Another purpose of this study is to assess if the one-stop clinic (faster diagnosis and treatment) leads to a faster time to wound closure. After studying the files of 385 patients with an ulcer for wound size, number of visits, date at first visit, date of wound closure, which method was used (one-stop or other), and ulcer care in the hospital or by dedicated nurses, 97 patients were included. Patients who were treated by dedicated nurses were significant older and had larger wounds. Age was not significantly related to time to wound closure. This study showed that the time to wound closure is not statistically different between patients treated by dedicated nurses compared to hospital care when adjusted for the effects of the one-stop clinic. The one-stop clinic gives a significant better chance for faster time to wound closure controlled for both groups, because a proper diagnosis is made and a correct treatment can be started directly. This will result in lower costs for these ulcer treatments. Second, by means of dedicated nurses, the treatment can be arranged at home as good as in the hospital, which could be a benefit for many patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M Wikkerink is an employee of Carrintreggeland. This company provides ulcer care to patients with ulcer venosum cruris who were initially treated by the ZGT Hospital. M Wikkerink is part of the research as an expert in the field and not as a representative of Carrintreggeland.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The medical ethics committee of the ZGT Hospital approved this study.
Guarantor
The guarantor of this research project is EBM Kroft.
Contributorship
EBM Kroft and B Rook researched the literature and conceived the study by gathering data from patient files and performed data analysis. M Wikkerink was involved in advising about the research protocol. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
The authors want to thank J Timmerman and M Vermeer, PhD (both epidemiologists of the ZGT), R Wijnsma (medical assistant Dermatology ZGT), M Huis in‘t Veld and A Broekmaat (nurses Dermatology ZGT) and M Beekman (dedicated nurse ZorgAccent) for their help in collecting and analysing the data of the files.