
Abstract
Introduction
In 2012, the Rouleaux Club published their survey claiming large deficits in venous training. Since then vascular surgery has become its own specialty with a dedicated section of the curriculum for superficial venous intervention. The aim of this study was to assess whether the introduction of the new curriculum has improved current Rouleaux Club members training in superficial venous intervention.
Method
A trainee designed survey was developed and distributed to UK vascular surgery trainees in summer 2017.
Results
We received 55 (41.0%) responses. Training in endovenous procedures was available to 100% of trainees, and open surgery was only available to 43.2% of trainees; 86.5% of centres used endovenous procedures as the default intervention Only 75.7% of respondents were timetabled for dedicated superficial venous intervention lists; 72.7% have not received any formal training in duplex ultrasonography. Higher self-reported procedural competence was associated with greater numbers of procedures rather than training grade seniority.
Conclusion
It seems that despite a separate curriculum there are still self-reported trainee deficits in competence and skills. Low respondent levels (41%) should be considered but there is a potential problem for future venous practice.
Introduction
Superficial venous incompetence (SVI) affects approximately 35–50% of the adult population.1,2 In 2014–15, 37,000 varicose vein interventions were performed by the NHS, 3 a significant but unknown number also undergo private treatment. Given the regularity of clinic attendances with symptomatic SVI and the frequency of procedures performed within the NHS alone, varicose veins intervention is an essential part of the vascular surgeon’s skill set. In 2012, vascular surgery separated from general surgery as a General Medical Council (GMC) defined specialty with a dedicated vascular curriculum. 4 It has been well documented that the introductions of modernizing medical careers (MMC-2008, 5 the New Deal (1998) 6 and the European Working Time Regulation (EWTR-2003) 7 have added to the difficult challenges to providing procedural training for surgical trainees within the training timeframe. Compounding these difficulties, Clinical Commissioning Groups (CCG) are making the criteria for SVI interventions increasingly stringent.8–10 This rationing is reducing procedure numbers and presents further barriers to training.
Evolution in the management of SVI has led to a huge expansion in the number of techniques available, traditional saphenofemoral ligation and strip being replaced by endovenous thermal ablation in accordance with published evidence.11,12 The National Institute for Health and Care Excellent (NICE) clinical guideline 168 recommends endothermal ablation as first line, followed by foam sclerotherapy (FS) and then surgical ligation and stripping. Recent endovenous developments have arisen in popularity and include non-tumescent non-thermal techniques (NTNT) such as cyanoacrylate adhesive (Glue) and mechanical occlusion with chemical assistance (mechanochemical ablation; MOCA) which have been adopted to varying degrees across the country. 13 The evidence base for these procedure is amongst the largest within vascular surgery and presents an intimidating variety for vascular surgeons in training to develop the wide range of skills required to provide these treatments, including the application of ultrasound, that has not traditionally been afforded time in the venous section of the curriculum.
In 2012, the Rouleaux Club (RC) 14 performed a survey of its members regarding venous training; they concluded trainees wanted more access to, and better-quality training in managing SVI. Similarly in 2015, the European Venous Forum conducted a survey of its training venous practitioners and phlebologists which also concluded more specialised venous training should be provided. 15 The new training programme has been running for four academic years and the first cohort of vascular surgery trainees is nearing completion of training, it was felt that this is the appropriate time to evaluate venous training opportunities available to UK vascular trainees with regard to the interventional management of SVI. Given that the syllabus is dedicated to the full spectrum of vascular disease, has this provided more opportunity for venous training and improved trainees’ perception of competence.
Methods
Between April and July 2017, an online survey was circulated to the members of the RC over three rounds.
The survey consisted of a questionnaire generated by the authors. This was reviewed by a consultant vascular surgeon (IKN) and president of the Royal Society of Medicine Venous Forum prior to dissemination.
The questionnaire interrogated four aspects of training: Local arrangements for venous training; formal and informal procedural training; dedicated allocation of training opportunities and self-reported procedural competence. The full survey is available in online Appendix 1.
Regular and repeated effort was made to encourage trainees to complete the survey with dedicated emails and personal communications. Trainees from all l6 UK local education training boards (LETB), formerly known as deanery’s were contacted. LETBs are responsible for the allocation of trainee rotations and placements across the institutions and hospitals providing a vascular surgical service.
Specific training information was collected on all NICE recommended treatments, including endovenous thermal ablations, open surgical ligation and strip of both the Great and Small axis, perforator ligation and phlebectomy.
Endovenous techniques assessed included radiofrequency ablation (RFA), endovenous laser ablation (EVLA) or steam ablation. Information on endovenous non-tumescent non-thermal ablation (NTNT) training opportunities were also collected; these include FS, cyanoacrylate adhesive (CA) and mechano-chemical ablation (MOCA).
Venous ultrasound (Duplex Ultrasound, DUS) competence was also evaluated for this survey. This is an essential skill within the curriculum and for the performance of endovenous procedures. Trainees are required to have competence in B-mode and colour Doppler imaging for diagnosis as per the international Union of Phlebology consensus docuemnt 16 and venous cannulation.
The Intercollegiate Surgical Curriculum Programme (ISCP) has a defined set of competence levels and this is outlined in Figure 1. 4 Level 4 is the highest achievable and in the context of surgical procedures indicates a trainee is able to perform the procedure independently and to deal with complications that arise. This system was used within the survey for grading self-reported level of venous competence.

Levels of competence as reported in the ISCP syllabus.
Basic demographic and statistical analysis was performed in SPSS v24. Chi-squared, t-test and one-sample median were used according to the type and distribution of data.
Results
Baseline demographics
RC trainee membership at the time of survey was 131 members (either with or without National Training Number (NTN)). A total of 55 (41.0%) responses were received, 51 (92.7%) of these were a currently in possession of an NTN. Mean age of respondent was 33.8 years (range 25–44). Number of years in NHS employment prior to gaining a national training number (NTN) was 4.9 years (0–9). The median number of LETBs for each trainee was 2 (1–5). Median year of training was ST5 with representation from all training years (Figure 2). Responses were received from 13 of the 16 LETB. There were no responses from any trainees based in Health Education Kent, Surrey and Sussex; Health Education Central and East London and Health Education Thames Valley. There was significant over representation from the West Midlands Deanery (15 responses; median for all others was 2 (range 0–5), p < 0.001) (Figure 3).

Bar chart representing number of survey responses by year in training.
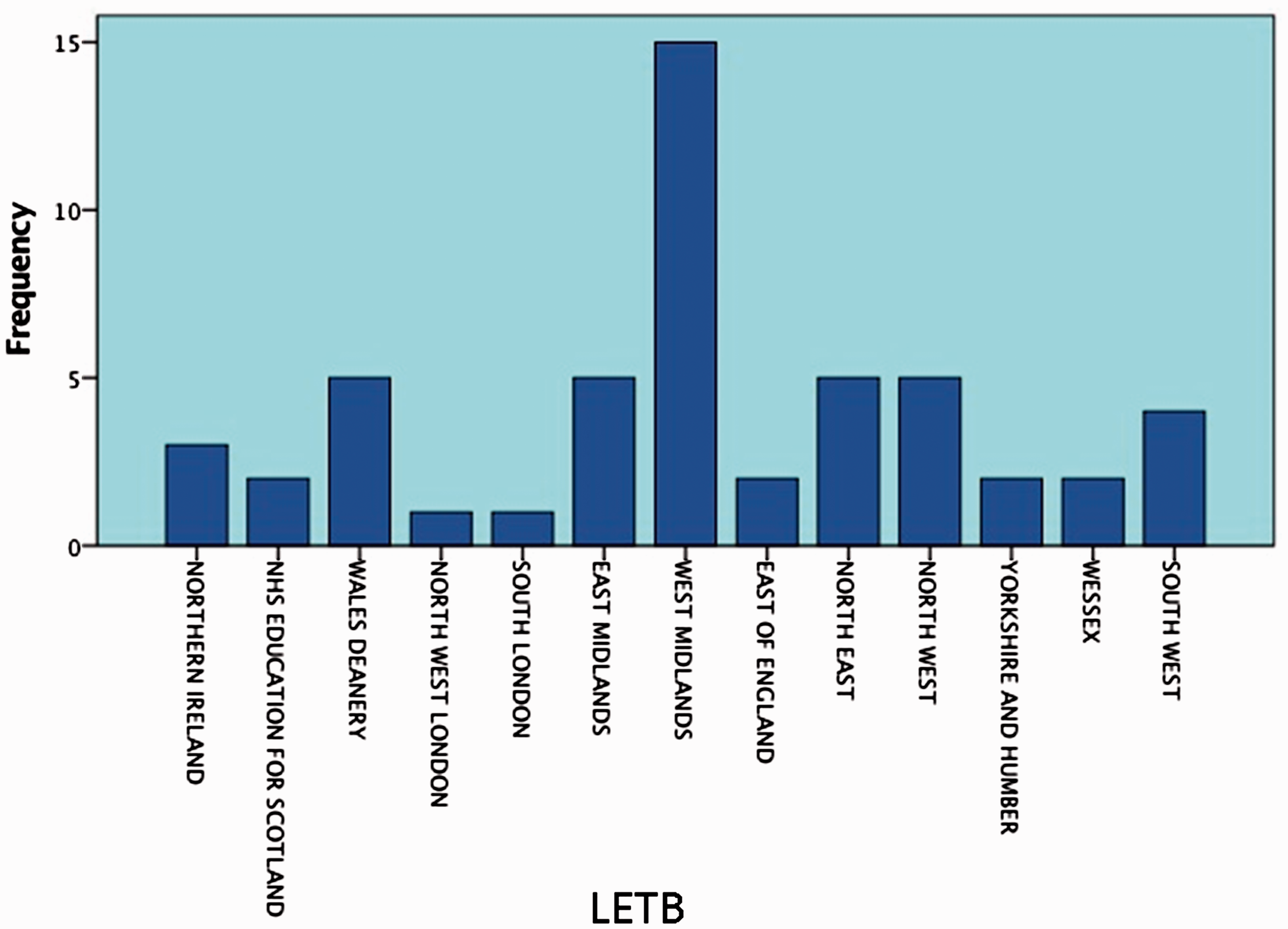
Number of responses to survey by deanery.
Training opportunities
Of the vascular units represented, the modalities of treatment available were; open surgery 100% (55), endothermal ablation 86.1% (47), and NTNT in 83.3% (46) of units. Training in endothermal ablation techniques for SVI was available to 81.1% (45) of members; NTNT techniques to 64.9% (36) (FS 62.2% (35), MOCA 5.5% (3), glue 1.8% (1)) and open surgery to 43.2% (24) of members during their rotational training (Table 1).
Availability of training by technique to treat SVI.

Note: Eighteen respondents did not answer this question of the survey.
SVI: superficial venous incompetence.
Open surgery for SVI although available universally was significantly less available for training (p ≤ 0.001), and a similar non-significant trend was observed for NTNT techniques (p = 0.057). When endothermal ablation was used it was also available for training (p = 0.324); 86.5% (11) of represented LETBs have an endovenous first approach to SVI treatment for suitable patients. Four years after NICE recommended an endothermal-first approach, 13.5% (2) use open surgery as first line treatment (86.5% vs. 13.5% p < 0.001).
Most vascular networks work in a hub and spoke model, 73.0% (27) of hubs perform interventions for SVI. Just over half, 56.8 (22) performed SVI intervention at their spoke hospitals. Only 10% (4) provided treatment at local independent treatment centres on behalf of the NHS. Less than half of vascular networks performed SVI interventions in main theatre (45.9%, 17); 64.9% (25) performed their interventions in day case theatres, 40.5% (15) in a treatment room and 10.8% (4) in clinic. Most vascular networks offer venous intervention using a combination of main theatres, day case theatres and treatment rooms.
In all, 75.7% (28) of respondents were timetabled for dedicated SVI interventions; 21.6% (8) of represented vascular networks performed SVI interventions on out of hours waiting list initiative lists. Only one trainee had access to training on SVI at a private hospital.
Training in venous ultrasound
The majority of responders (72.7%, 32) have not received any formal training outside that provided by deanery teaching programs in venous ultrasonography; 25% (11) had attended a one to two day course and only 2.3% (1) have completed a postgraduate certificate qualification. The majority of trainees (70.5%, 31) reported informal opportunities to gain ultrasound scanning experience. On specific questioning, 90.9% (40) of responders feel that training in DUS was either essential or very important.
Trainee opinion
To understand whether there was a perceived preference for training between techniques, trainees were asked if they felt training in open, endothermal and NTNT techniques was valuable. In general, trainees felt training in each technique was important. Specifically, 84.1% (37) feel training in open surgery is either very important or essential; 100% (44) feel that training in endothermal ablation is very important or essential and 86.3% (38) feel training in FS is very important or essential.
Current experience and competence
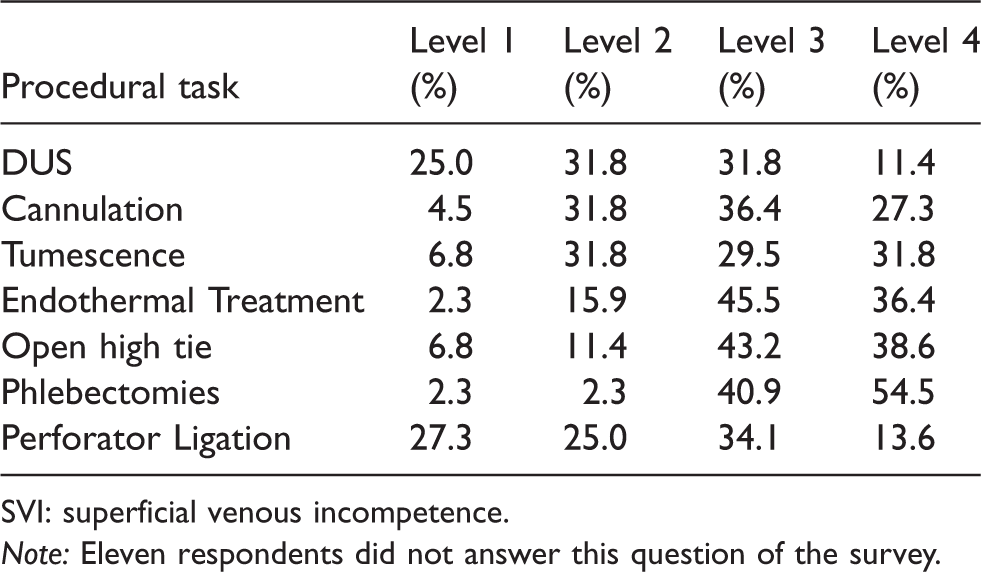
Trainees rated DUS as the aspect of endovenous management of SVI they found most challenging. Self-reported competence in a variety of steps required in open and endovenous interventions was recorded. Competence in non-ultrasound dependent tasks (delivering endothermic treatment, high tie and phlebectomies) was higher (median = Level 3) than those ultrasound dependent tasks (cannulation and tumescent anaesthesia) (median = level 2). The only exception was competence in perforator ligation which was a level lower than open high tie. The full response is detailed in Table 2. Significantly, fewer trainees are confident in performing ligation and stripping of the SSV than of the GSV (43.2% vs. 68.2% (19 vs. 30), p = 0.001).
Self-reported competence in key aspects of SVI procedures.
SVI: superficial venous incompetence.
Note: Eleven respondents did not answer this question of the survey.
For each technique, trainees were asked to provide the numbers recorded in their eLogbook (performed independently or with supervision). A full summary is provided in Table 3. There was large variation in number of cases in all techniques. No trainee had managed to gain experience in every available technique. Increasing training grade is not associated with increased numbers of procedures logged. Open surgery and RFA trended to increased procedural numbers with training years, however this was not significant.
Number of times each procedure performed by trainee according to eLogbook entry.
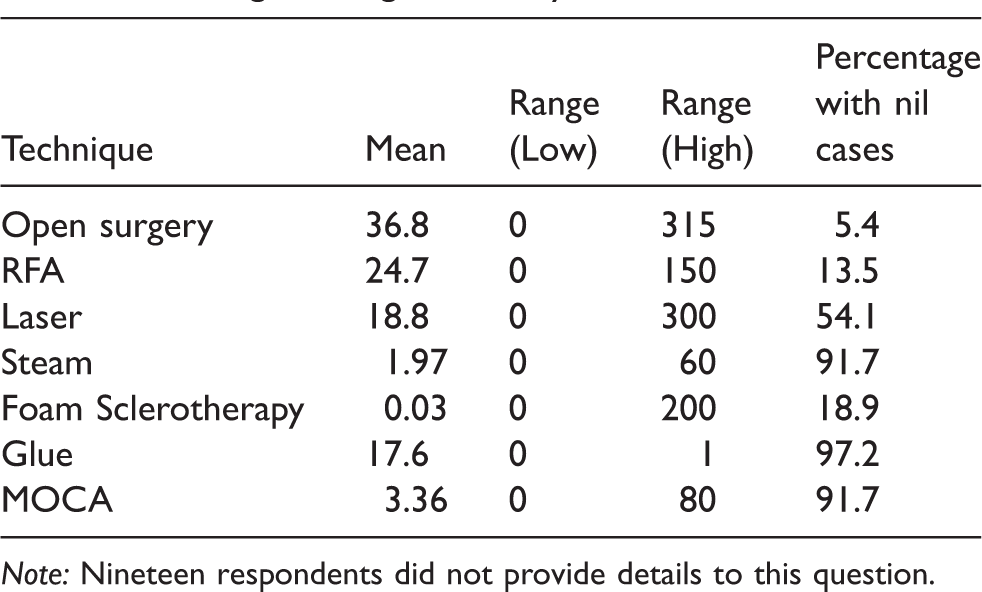
Note: Nineteen respondents did not provide details to this question.
Increased self-reported procedural competence is associated with increased number of logged procedures in the trainees’ eLogbook. For example, trainees reporting level 1 competence for cannulation had a mean of 10 endovenous cases in their eLogbook compared to 139.8 cases for those reporting a Level 4. This trend was consistent throughout with the exception of phlebectomies; this was as a result of so few rating themselves as a competence Level 1 or 2. Finally, there is no correlation between procedural numbers for both open and endovenous surgery (Pearson correlation 0.182, p = 0.280).
Discussion
The response rate of 41% for this survey is low especially compared to those of the 2012 RC survey. But, this is in keeping with other medical and venous disease surveys.9,17 When compared to the European Venous Forum survey, 15 here there were only 24% of trainees who responded. We also noted with interest the stark contrast between the response rate for this survey and a concurrent survey run by the RC on the provision of emergency endovascular aneurysm repair (EVAR) for ruptured aneurysm that received a 100% response rate after only two prompting emails. One could conclude from comparing these two surveys that training in SVI management does not appear to be as important to current vascular trainees in the UK. It is important to consider that members of the RC are asked to complete training-based questionnaires by the GMC and JCST on a yearly basis as a compulsory aspect of training, and it maybe that members experience survey fatigue as a result of these along with other surveys disseminated by organisations other than RC.
Most responding trainees worked in centres that offered open, endothermal and FS treatment for SVI. Where endovenous procedures were performed they were available for training. This was not the case with open surgery which although available was seldom performed. All trainees reported open procedures being performed in their institution if required; however, only 43.2% felt that open surgery was available for training. This is exemplified by the practice of the consultant author who has performed less than five open varicose veins procedures since 2010 despite undertaking over 200 procedures for SVI per year over the same period. It can be argued whether training in open surgery is important now that as endovenous interventions have become the gold standard for treating SV incompetence. 11 Furthermore, aspects of other vascular procedures such as GSV harvest in lower limb bypass surgery could be translated to attain the required skills for open venous surgery, perhaps there is a translational element of competence that the trainee participants are failing to recognise.
Currently, the vascular syllabus requires Level 4 competence in open saphenofemoral and saphenopopliteal disconnection and level 4 competence in open recurrent venous surgery. 15 These curriculum requirements for open surgery, particularly in recurrent surgery, may need modification as they are out of step with modern venous practice.
The hub and spoke model for prevalent in vascular centres presents an additional hurdle to venous training. Trainees are typically based at the hub site to cover the main vascular theatre lists, clinics and admissions while ambulatory vein lists are typically performed in the spoke hospital. With current understaffing levels and compulsory rest periods after on-calls, day case opportunities can be limited especially for lists provided in spoke sites. This survey found 73% of hubs performed interventions for SVI (45.9% of these interventions being performed in main theatres). This should mean that even within hub and spoke model, trainees have opportunities to gain experience in SVI intervention. With regard to NTNT techniques, there should be training opportunities for FS; however, our results indicate that trainees only receive training in glue and MOCA if they work in a unit that has real enthusiasm for the specific technology or is involved in research related to that device, perhaps at present this is acceptable given that the efficacy evidence Glue and MOCA is still evolving.
One way that training programmes can influence the number of trainee opportunities is to timetable trainees to lists dedicated to treatment of SVI. Currently, although 75.7% of trainees have this opportunity, it is unsatisfactory for a quarter of trainees to be gaining their experience on an ad hoc basis.
The aspects of SVI intervention that trainees find most difficult are those that require DUS. The vast majority (90.9%) felt that training in DUS skills is very important or essential; however, only 27.3% had received some form of formal training in DUS. This aspect of training is not covered in the formative years prior to obtaining a vascular surgery NTN. Also, many consultants are self-taught or have arranged their training and have no formal training accreditation in DUS. This is therefore a training requirement that has to be addressed centrally within the regional training programmes. The results of this survey indicate that if more trainees receive formal training in DUS they would be better equipped to perform the steps of endovenous procedures that require US. As the focus of vascular surgery becomes even more endovascular focused, DUS skills are becoming essential to functional practice in both the arterial and venous aspects of vascular surgery. It could be that making formal postgraduate qualification in DUS via specifically developed courses within the curriculum, with the approval and oversight of the Royal College of Radiologists, an essential requirement to achieve certificate of completion of training (CCT) (like ATLS and CCrISP), would address and resolve this issue. To make a comparison with arterial surgery, without the skills to interpret a CT Aortogram and accurately size an arterial graft, vascular surgeons would not dare proceed to endovascular aneurysm repair, yet the same is not translated for endovenous intervention for SVI.
As well as highlighting the importance of DUS training, the results of this survey suggest that responding trainees felt training in all aspects of SVI intervention to be important. This, however, contrasts with the survey response rate achieved and the poor trainee attendance at the Royal Society of Medicine Venous Forum (VF) training day 2017. Despite significant notice, multiple email correspondence and substantial subsidies only 11 trainees attended this training day.
Increased length of training should correlate with increased opportunity and exposure, along with improved competence and higher number of logged procedures. However, we found that number of procedures performed for SVI was not associated with increased training grade, in open surgery there was a trend towards greater numbers with increasing with years of training. Competence did correlate well with number of procedures. This indicates that number of procedures performed rather than years in training increased confidence and competence in performing the steps of the procedure. Perhaps therefore evidence that a dedicated short ‘SVI interventions’ block of training may address the training deficits.
Trainees that obtained high numbers of open procedures or endovenous procedures did not obtain high numbers in the other technique. This may be a sign of bias within their region to one particular type of treatment, or their institutional or workforce restrictions limiting the type of list that could be attended. It could also be that areas with a high number of trainees encourage trainees to attend day case endovenous lists as they have limited exposure to main theatres, while those with few trainees spend most of their time covering main theatres with corresponding exposure to open general anaesthetic procedures. This survey did not directly address this issue.
The underlying limitations of this study must be acknowledged.
Firstly, it must be questioned whether our 41% of response rate is representative of the training cohort. Secondly, over representation of one LETB may have skewed the results in favour of the practices of that region rather than reflecting training on a national level. In addition, many respondents skipped parts of the survey, leaving gaps in the data and reduced the power of the subsequent analysis. Finally, people who responded to this survey may have been enthusiasts and may reflect the body of trainees who are passionate about treatment of SVI. Despite these limitations, our survey has revealed a potential significant deficit in training of SVI interventions within the vascular surgery curriculum.
Perhaps, in order to address this, trainees are time-tabled to a regular training lists in SVI interventions as currently occurs for interventional radiology. With the majority of centres offering open and endovenous interventions, trainees would gain experience of both during their training. Secondly, the issue of access to open surgery (a decreasing number of open surgical procedures are performed each year for SVI) presents a challenge to trainees. Perhaps here the recognition of SFJ ligation in GSV harvest for bypass surgery, as a venous training opportunity will build trainee confidence. Perhaps the consideration of syllabus amendment to reflect the realities of modern training.
DUS training for vascular trainees appears to be limited. This survey has highlighted deficits in competence which will impact on DUS procedural competence. There is need for a course that enables trainees to attain the knowledge and practical experience required to be become confident users of DUS for assessment and management of SVI. It maybe, that in the future, if successive cohorts of trainees are unable to gain the sufficient expertise in the management of SVI and concurrent skills in DUS, post graduate accreditation will be required to assess these specific competencies. Either that or trainees maybe required to undergo post CCT fellowships in SVI prior to commencing in post as a consultant vascular surgeon.
The authors accept that training is a two-way process. There must be engagement from both parties and indeed as adult professional learners, vascular trainees do have to take responsibility for their own training deficits and seek out appropriate opportunities to meet the demands of the syllabus. Awareness and encouragement for the RSM Venous forum and the Vascular Society will of course always support trainee engagement.
Conclusion
Six years on from the initial RC survey of venous training and four years after implementation of a dedicated vascular curriculum, there are notable significant deficits with regard to training in SVI. Improving dedicated trainee access, training in duplex ultrasound and targeted exposure to open surgery are required for trainees to reach the required level of competence for completion of training. Trainees must take an active role to ensure they reach CCT competence in the management of SVI, but additional direct action at the SAC level will help to improve trainees’ engagement.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the Rouleaux Club and their membership for the support of this survey. We would also like to thank the Royal Society of Medicine Venous Forum for their support and providing the platform for dissemination of our results.
Ethical Approval
No ethical approval required.
Guarantor
L. Meecham
Contributorship
L. Meecham: Design/data collection/analysis and writing manuscript. S. Nandhra: Design/data collection and writing manuscript. I. Nyamekye: Design and writing manuscript.