
Abstract
Objectives
To evaluate postoperative venous haemodynamics and quality of life after treatment of great saphenous vein (GSV) incompetence.
Methods
Radiofrequency ablation and high ligation and stripping were performed in 62 patients (65 limbs) and 58 (65 limbs), respectively. Phlebectomies were performed in both modalities. Strain-gauge plethysmography on the foot combined with superficial venous occlusion was used to measure refilling time after knee bends. Strain-gauge plethysmography, duplex ultrasound and quality of life were assessed before and one month after treatment.
Results
Duplex ultrasound displayed successful intervention in all but two limbs. Refilling time increased similar in radiofrequency ablation and high ligation and stripping after treatment (p < 0.001). Postoperatively, strain-gauge plethysmography detected remaining reflux in 71% of the patients. Multivariate analysis showed that two or more incompetent calf branches were associated with remaining reflux (OR 4.82 (95% CI: 1.33–17.5), p = 0.02). No difference in quality of life was seen in patients with remaining reflux.
Conclusions
Despite successful treatment, a majority of the limbs showed remaining reflux, in which incompetent calf branches appear to play an important role.
Clinicaltials.gov: Lower Limb Venous Insufficiency and the Effect of Radiofrequency Treatment Versus Open Surgery. Nr: NCT02397226
Keywords
Introduction
Chronic venous disease is a common condition with clinical signs ranging from telangiectasias to varicose veins, which can lead to edema, eczema, lipodermatosclerosis and ultimately ulcers.1,2 Recommended treatment for superficial venous incompetence in the lower limb involve endovenous interventions and high ligation and stripping (HL/S),1–3 with the aim of improving the haemodynamic effect of the disease and to achieve symptom relief. However, despite advances in duplex ultrasound (DUS) diagnostics and more available treatment options, recurrence of varicose veins and relapse of symptoms continue to be a complex problem.3,4 DUS is excellent in describing the anatomical distribution of the reflux3–5 but does not permit an overall quantification of venous function. Plethysmographic methods are often used to determine whole limb venous haemodynamics.6–11 We have developed a new method of strain-gauge plethysmography (SGP) with standardized selective superficial occlusion, which has been validated by ascending phlebography.12,13 With our method, the components of superficial and deep venous refilling can be separated from each other. In patients with superficial venous incompetence, it is thus possible to compare each individual’s refilling time with their optimal state, i.e. during superficial occlusion when no component of superficial reflux affect the refilling time. Accordingly, the method allows a postoperative quantification of any possible sub-optimal haemodynamic treatment. This seems important because many patients have postoperative remaining reflux distal to the lowest access point of the intervention,14–16 and it is uncertain to what extent distal reflux in great saphenous vein (GSV) and/or small saphenous veins (SSV) segments and/or associated branch varicosities affect postoperative venous haemodynamics. It is further unknown whether the component of remaining superficial reflux is related to clinical signs or symptoms. This study was conducted to assess haemodynamic parameters using SGP and segmental venous reflux with DUS in the early postoperative state after treatment of GSV incompetence. The aim was further to evaluate if remaining reflux is related to clinical signs or symptoms in the early postoperative phase. We hypothesized that current methods are associated with remaining reflux, mainly due to incompetent veins below treated area.
Material and methods
Participants comprised of consecutive patients recruited between September 2014 and February 2019. They were referred to our polyclinics located in Norrköping and Linköping, Sweden. Diagnostic DUS was performed prior to referral. Inclusion criteria were GSV incompetence (C in CEAP, C2–C6) 17 and GSV suitable for treatment with both radiofrequency ablation (RFA) and high ligation and stripping (HL/S). Exclusion criteria were GSV anatomy not appropriate for both treatments, previous treatment in the limb, incompetent tributaries near the saphenofemoral junction, isolated SSV incompetence greater than 100 ml/min and/or greater SSV diameter than 6 mm and patients who were not considered able to perform the examinations. Bilateral treatment was permitted provided both limbs received the same treatment during the same operation. The patients was examined according to C in CEAP and Venous Clinical Severity Score (VCSS), and completed Aberdeen Varicose Vein Questionnaire (AVVQ).17,18 Patients were then referred to preoperative and follow-up investigations performed one-month after treatment with DUS and SGP performed by biomedical scientists at the Department of Clinical Physiology, Linköping, Sweden.
High ligation/stripping
HL/S was performed under general anesthesia. An incision was made in the groin with division and ligation at the saphenofemoral junction of the GSV and all tributaries in the area. The GSV was removed to below the knee. Local phlebectomies of prominent tributaries were performed.
Radiofrequency ablation
RFA was performed using the 7 cm ClosureFast radiofrequency catheter (Medtronic, Dublin, Ireland) during ultrasound guidance and tumescent anesthesia. Treatment was performed from below knee level to 1–2 cm from the saphenofemoral junction. Two cycles were used near the saphenofemoral junction, phlebectomies of prominent tributaries were performed. Both HL/S and RFA were performed by vascular surgeons employed at Linköping University hospital.
SGP with selective superficial occlusion
Our SGP protocol with two cuffs and selective occlusion of the superficial veins has been validated by ascending phlebology and allows a haemodynamic evaluation of the superficial and deep veins separated from each other.12,13 In short, a strain-gauge was placed around the forefoot, and compression cuffs were applied just over the malleoli and below the tibial condyles (Figure 1). Patients performed 20 knee bends at 1 s intervals, which activate the calf muscle pump as well as the foot pump by creating a weight transfer movement.
19
After completion, the patient remained still until a new steady


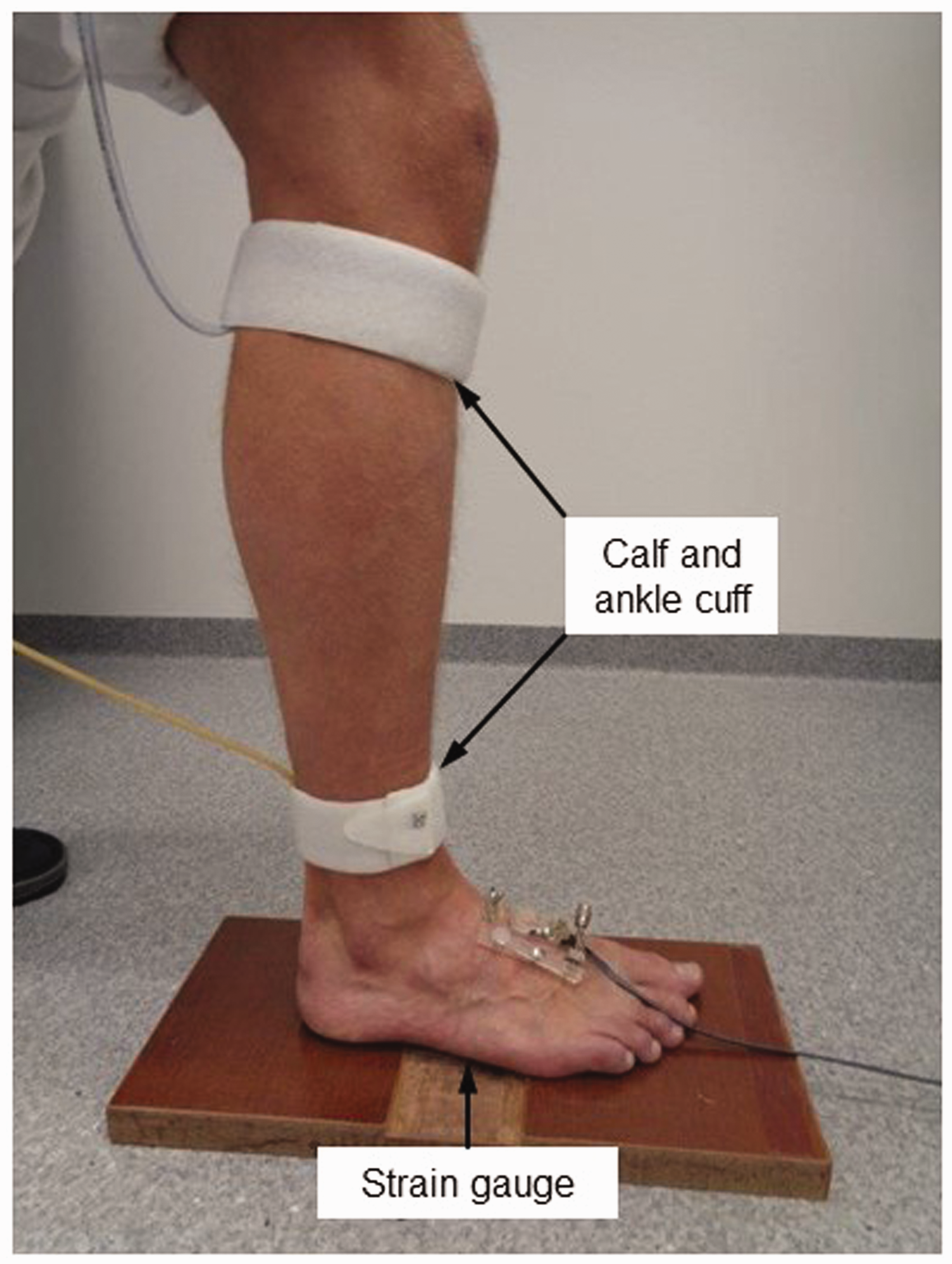
Arrangement of patient, calf cuff, ankle cuff and strain gauge for lower extremity venous plethysmography. As noted, it is possible to use a strain gauge on the calf as well in this setup.
The calculated pressure is the individual hydrostatic column (the distance between heart level and respective cuff) with the addition of a hydrostatic column of 30 cm and an ankle/calf pressure of 30/60 mmHg. The ankle and calf pressures were shown by Zachrisson et al. 13 to occlude the superficial system and because the experiments were conducted in the supine position with a measuring point 30 cm above heart level, a correction of this was conducted by adding a hydrostatic column of 30 cm. A conversion factor from cmH2O to mmHg of 0.76 was used. The same protocol was used pre- and postoperatively. Based on our previous determination of the methodological error of SGP measurements, patients were classified into two groups according to postoperative refilling times, i.e. no remaining reflux was defined as a difference in T50 ≤5 s between postoperative SGP with superficial occlusion and postoperative SGP without superficial occlusion, whereas remaining reflux was defined as a difference in T50 > 5 s between the measurements (Figure 2). All data were recorded, stored and analyzed using PeriVasc software (Ekman Biomedical Data AB, Gothenburg, Sweden).
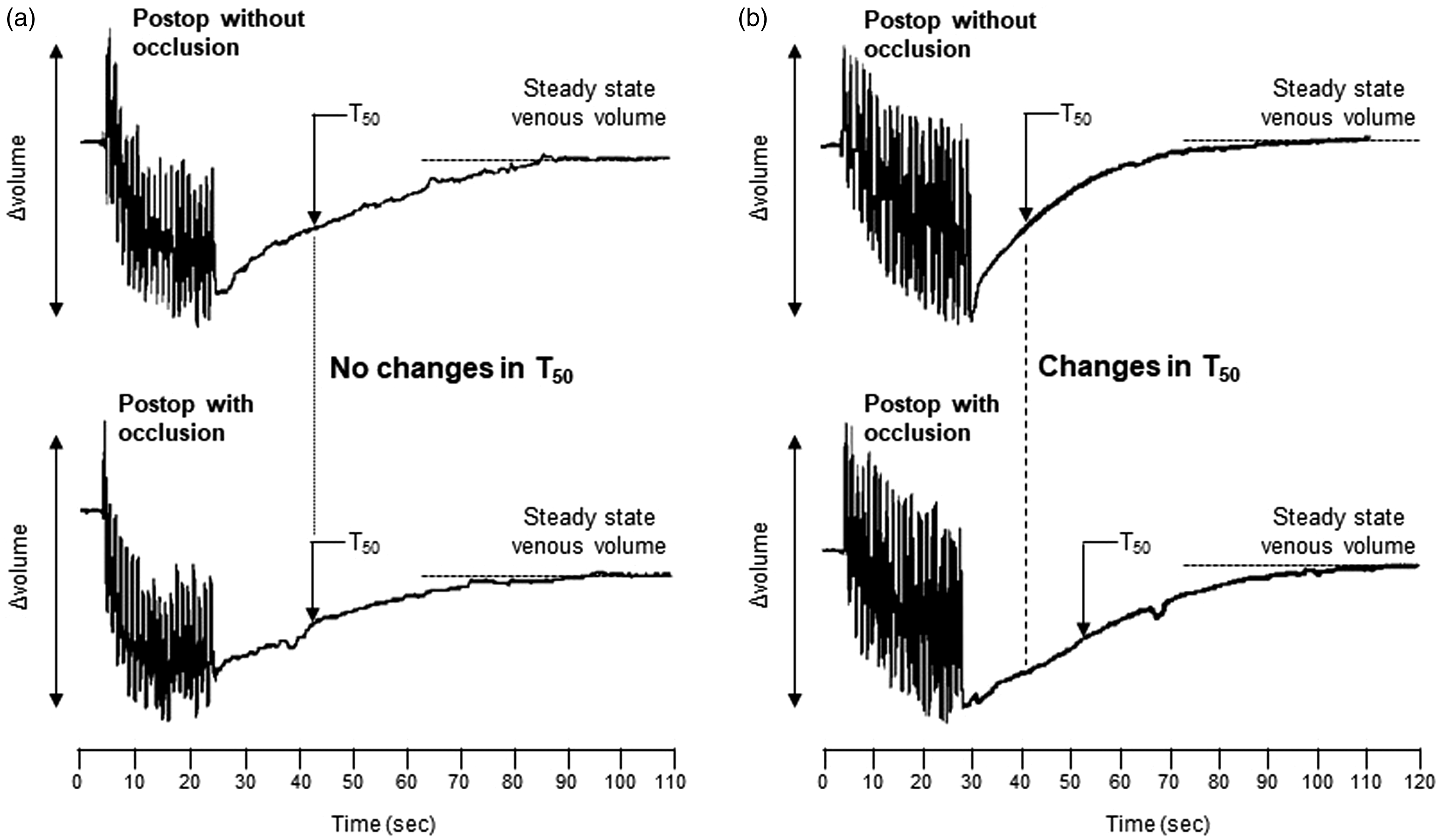
Representative tracings from two patients during postoperative SGP without, and with superficial occlusion. (a) Patient with no changes in T50 when superficial occlusion was applied. Based on no improvements in refilling time, this patient was characterized as no remaining reflux. (b) Patient with 12 s improvement in T50 when superficial occlusion was applied. Based on the improvement in refilling time of > 5 s, this patient was characterized as remaining reflux.
Duplex ultrasound
DUS examinations were performed with ACUSON S2000 system (Siemens Medical Solutions, Malvern, PA, USA) with 9 and 18 MHz transducers. The 9 MHz transducer was used for assessment of reflux. Both the 18 and 9 MHz transducer were used to exclude wall changes in the superficial and deep veins. The examination comprised of a standardized protocol to assess reflux in superficial, perforator and deep veins. A standardized cuff unit (Ekman Biochemical Data AB, Gothenburg, Sweden) inflated to 100 mmHg was used for distal compression and rapid release. Presence of normal phasic flow during breathing in the common femoral vein was mandatory in order to exclude significant central obstruction.
20
GSV incompetence was classified according to initial reflux flow during the first second after release of distal compression and measured in ml/min in the proximal part of the GSV. This classification is used at Linköping University Hospital and based on data correlating peak flow velocity and volume flow with venous haemodynamics.12,21,22 GSV incompetence was defined as severe (>100 ml/min and/or a maximal flow velocity of >30 cm/s), moderate (30–100 mL/min and/or <30 cm/s).
21
Diameter measurements were performed in the proximal part of GSV. In the follow
QoL measurements
Statistical evaluation
Values are expressed as mean ± SE unless otherwise stated. Normal distributed data was compared using Student’s t-test or Paired Student’s t-test as appropriate. Ordinal data or data demonstrating a non-normal distribution were compared with Wilcoxon test or Mann-Whitney U test. Subgroup analysis were conducted according to calculation of the methodological error of SGP measurements.12,24 Based on this, patients were classified into either two groups, ≤5 s (no remaining reflux) or >5 s (remaining reflux) between postoperative T50 with and without superficial occlusion, and QoL was compared. A multivariate logistic regression analysis was used to evaluate the association between the dependent factor (postoperative remaining reflux) and clinical relevant factors. Statistical analyses were carried out using SPSS 25.0 for windows (IBM, Armonk, NY, USA). p-values <0.05 were considered significant.
Results
A total of 120 patients (130 limbs) were recruited, in which 62 (65 limbs) were treated with RFA and 58 (65 limbs) with HL/S. Demographical data are presented in Table 1.
Demographic and clinical data.
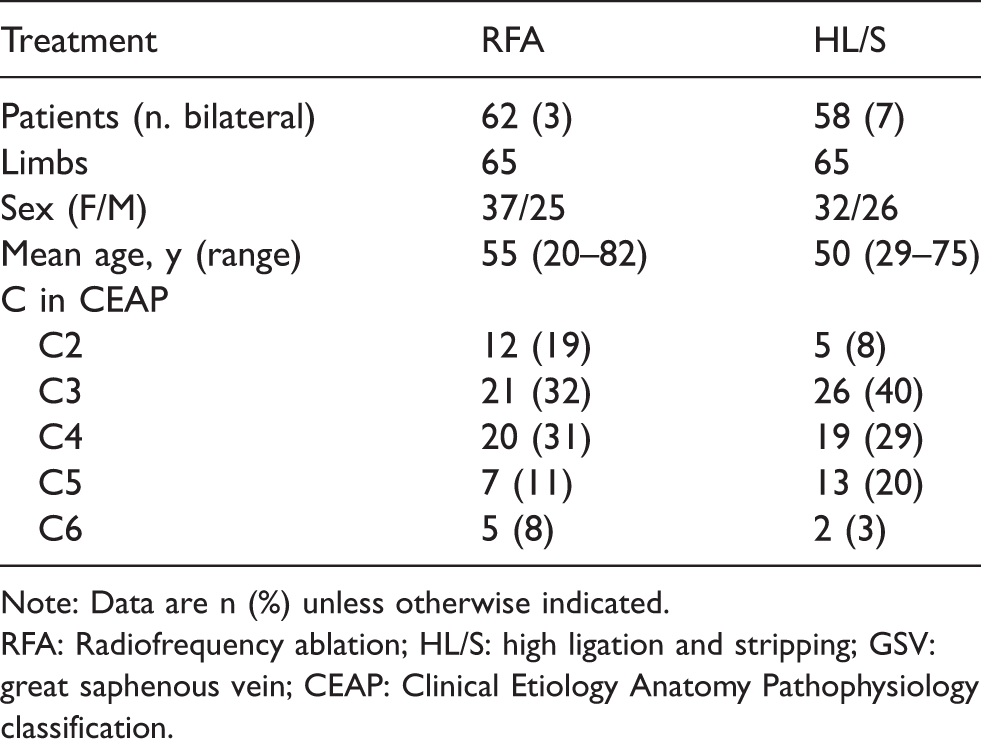
Note: Data are n (%) unless otherwise indicated.
RFA: Radiofrequency ablation; HL/S: high ligation and stripping; GSV: great saphenous vein; CEAP: Clinical Etiology Anatomy Pathophysiology classification.
Duplex ultrasound
Pre- and postoperative DUS are displayed in Tables 2 and 3. Axial GSV reflux from SFJ to the foot was detected in 32% and 26% of the limbs in RFA and HL/S, respectively. One limb in the RFA group had incompetence in the femoral vein, no patient in HL/S group had incompetence in deep veins. SSV incompetence was found in 25% of the limbs in RFA, compared to 6% in HL/S, and decreased marginally to 18% and 5% postoperatively. In both RFA and HL/S, approximately 50% of the limbs displayed two or more incompetent branches in the calf, and the percentage decreased similar to roughly 25% after intervention. Incompetent perforating veins were detected in 28% and 42% of the limbs in RFA and HL/S preoperatively, compared to 23% and 26% postoperatively. In RFA, no limb showed remaining reflux in treated GSV segment. One limb demonstrated reflux in the GSV stump, three new incompetent accessory branches in treated area as well as newly developed deep incompetence and one limb showed one new incompetent accessory branch in the treated area. In HL/S, stripping to mid-thigh was only possible in one limb due to a vein cluster, with reflux in the remaining GSV. One limb demonstrated a duplication of GSV with detected reflux from mid-thigh, and two limbs showed one new incompetent accessory branch in treated area. Below the treated area, 40% of the limbs in RFA and 45% of the limbs in HL/S displayed reflux in remaining GSV.
Preoperative DUS.
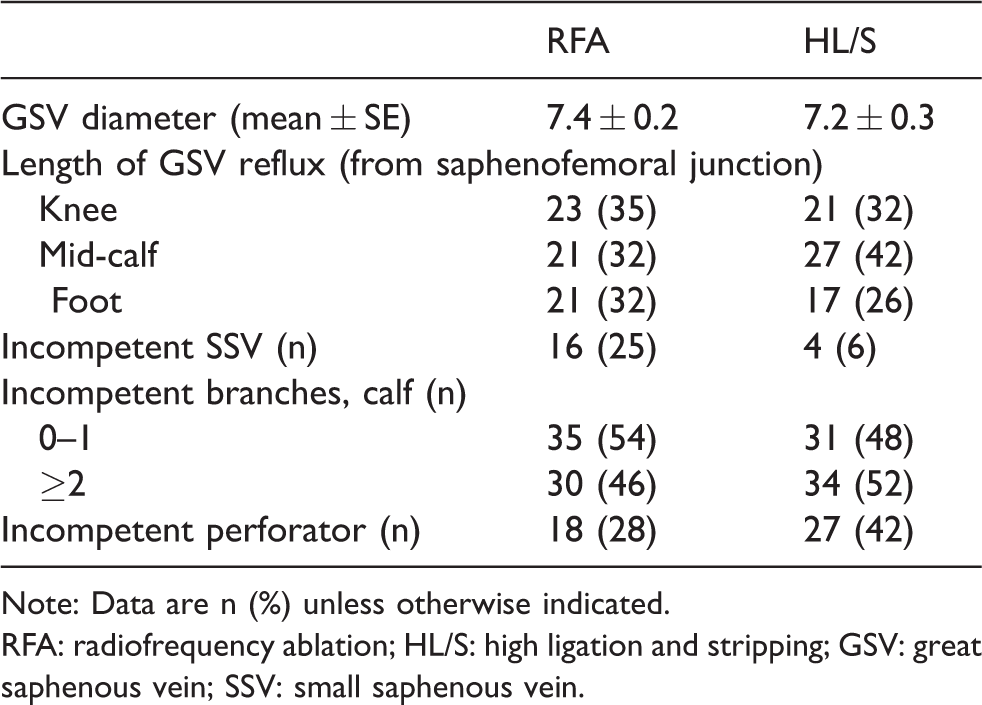
Note: Data are n (%) unless otherwise indicated.
RFA: radiofrequency ablation; HL/S: high ligation and stripping; GSV: great saphenous vein; SSV: small saphenous vein.
Postoperative DUS.

Note: Data are n (%) unless otherwise indicated.
RFA: radiofrequency ablation; HL/S: high ligation and stripping; GSV: great saphenous vein; SSV: small saphenous vein.
Strain-gauge plethysmography
T50 improved similar in the two groups when comparing pre- and postoperative SGP without superficial occlusion (Figure 3). In RFA, T50 increased from 9.4 ± 1.2 to 21.7 ± 1.4 s, and in HL/S, T50 increased from 9.9 ± 1.0 to 23.9 ± 1.5 s (both p < 0.001). In the two groups combined, T50 increased from 9.7 ± 0.8 to 22.8 ± 1.1 s (p < 0.001). Postoperatively, SGP with superficial occlusion demonstrated significant longer T50 compared to SGP without superficial occlusion, with no differences between RFA and HL/S (Figure 3). In RFA, T50 was 34.8 ± 2.5 compared to 21.7 ± 1.4 s (p < 0.001), and in HL/S, T50 was 34.9 ± 1.9 compared to 23.9 ± 1.5 s (p < 0.001). In the two groups combined, T50 decreased from 34.8 ± 1.6 to 22.8 ± 1.1 s (p < 0.001). Preoperative SGP with superficial occlusion was significantly longer compared to postoperative SGP without occlusion (Figure 3). In RFA, T50 was 26.9 ± 1.6 compared to 21.7 ± 1.4 s (p = 0.003), and in HL/S T50 was 30.8 ± 1.8 compared to 23.9 ± 1.5 s (p < 0.001). In the groups together, T50 decreased from 28.9 ± 1.2 to 22.8 ± 1.1 s (p < 0.001).

T50 from pre- and postoperative SGP without and with superficial venous occlusion. (a) RFA, (B) HL/S, (C) RFA and HL/S combined. **p < 0.01, ***p < 0.001. Paired Student’s t-test.
Factors associated with remaining reflux
No remaining reflux was defined as T50≤5 s between postoperative SGP with and without superficial occlusion, while remaining reflux was defined as a difference >5 s. In total, 36 limbs (29%) demonstrated no reflux based on T50 measurements, while 90 limbs (71%) demonstrated remaining reflux. In the multivariate regression analysis, only two or more incompetent calf branches was significantly associated with remaining reflux (OR 4.82 (95% CI: 1.33 – 17.5), p = 0.02, Table 4). Of the 36 limbs with no remaining reflux, 33 (92%) demonstrated less than two incompetent branches. However, 63 (70%) of the limbs with remaining reflux displayed less than two incompetent branches. A tendency for SSV incompetence to be associated with remaining reflux was seen, but the results were not significant (OR 3.40, (95% CI: 0.65–17.5), p = 0.15). No significant association were seen regarding preoperative factors such as sex and C in CEAP, type of intervention (HL/S versus RFA), or postoperative factors such as DUS detected GSV reflux below the treated area and incompetent perforators.
Multivariate logistic regression for all patients of considered influential factors associated to remaining reflux after intervention. Results are presented as odds ratios (OR) with confidence intervals of 95% (CI).

RFA: radiofrequency ablation; HL/S: high ligation and stripping; GSV: great saphenous vein; CEAP: Clinical Etiology Anatomy Pathophysiology classification.
aWomen compared to men.
bPatients categorized as C4–C6 compared to C2–C3.
Quality of life
In both RFA and HL/S, the severity of varicose disease assessed by VCSS was significantly reduced, and QoL evaluated by AVVQ was significantly improved with no differences between the groups (RFA, p < 0.001, HL/S, p < 0.001, Figure 4). Subgroup analysis of all patients with no remaining reflux demonstrated no significant improvement compared to patients with remaining reflux concerning both VCSS (p = 0.42) and AVVQ (p = 0.89).
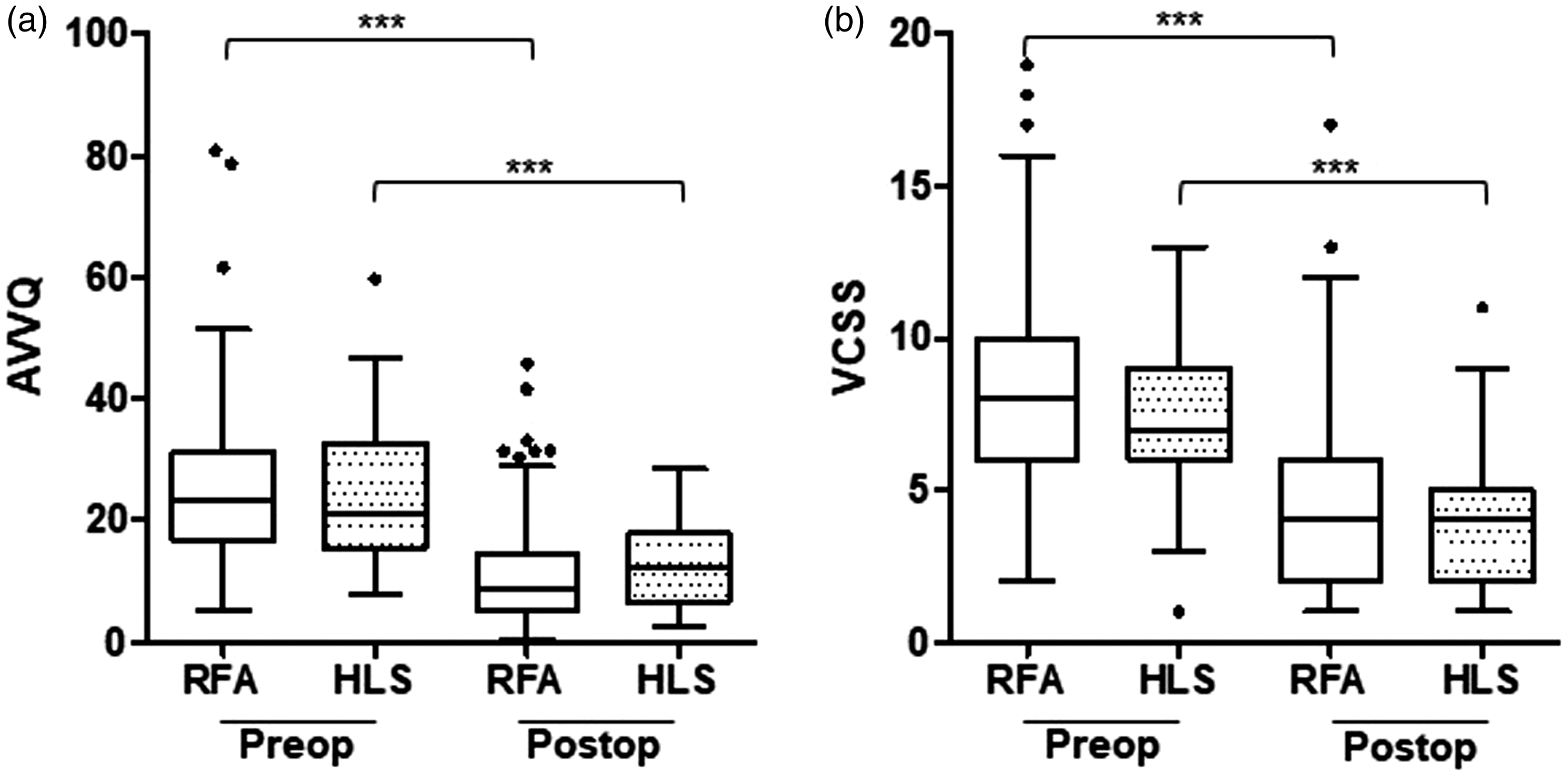
Pre- and postoperative AVVQ and VCSS in RFA and HL/S. ***p < 0.001. Mann-Whitney U test.
Discussion
Despite improvements in both pre-operative diagnostics and therapeutic interventions with a trend against more individual treatment strategies, recurrence of varicose veins remain a common as well as complex problem.25–27 Recurrence and relapse of symptoms may develop in spite of successful intervention and it is generally accepted that signs of recurrence become more apparent with additional years of follow-up.3–5 This study indicates that already one month after treatment of GSV incompetence with either RFA or HL/S, a large proportion of patients demonstrate signs of significant lower limb reflux despite successful intervention verified by DUS.
SGP was used in combination with DUS in the pre- and postoperative assessment. DUS provides diagnostic information on presence and anatomical distribution of the reflux,3–5 whereas plethysmographic measurements have the advantage of enabling quantitative evaluation of venous haemodynamics.6–11 Although the relationship between plethysmographic parameters and clinical severity of venous disease has varied across studies, it has been suggested that decreased venous refilling times (e.g. T50) are associated with both higher C class in CEAP and more specific values, such as skin changes.10,28,29 In this study, SGP measurements were conducted according to a standardized model for selective occlusion of the superficial veins.12,13 This model is validated by ascending phlebography and enable the components of superficial and deep venous refilling to be separated from each other.12,13 In patients with superficial venous incompetence, it is possible to compare each individuals current refilling time with their optimal state, i.e. during superficial occlusion when no superficial reflux affect the refilling time. Thus, our model can be used to isolate and quantify the effect of the superficial reflux component on the measured refilling time. This seems valuable since a large number of patients have remaining reflux below the lowest access point of the intervention.15,16 In our previous study, the methodological error was calculated, i.e. a value that can be used to estimate when a change in a T50 between two measurements is probable to reflect a true alteration. We found that a change in > 5 s is likely to indicate a real alteration and this seems to be similar to other data regarding SGP variability. 24 Accordingly, a difference in T50 ≤5 s between postoperative SGP with and without superficial occlusion was defined as no remaining reflux, whereas a difference in T50 > 5 s was defined as remaining reflux.
DUS one month postoperatively demonstrated successful intervention in all patients with the exception of two limbs in the HL/S group. These findings combined with a detailed preoperative evaluation containing both DUS and SGP implies that tactical and technical errors related to the treatment are unlikely. 30 Despite this, postoperative SGP with superficial occlusion, as a measure of venous function without any superficial reflux, demonstrated a significant longer T50 compared to SGP without superficial occlusion in both RFA and HL/S (Figure 3). The finding is further supported by preoperative T50 with superficial occlusion, which was found to be significantly longer than postoperative T50 without occlusion (Figure 2). This indicates that one month after treatment of GSV incompetence, a large proportion of patients show signs of lower limb reflux despite successful RFA or HL/S verified by DUS.
Postoperative DUS examinations showed that remaining reflux predominantly originated from below the treated area. This might be explained by the fact that both RFA and HL/S are performed from the groin to just below the knee in order to minimize damage to the sensory saphenous nerve. Although there are studies presenting that GSV below the knee can be safely treated with endovenous ablation, 16 no recommendation of this is yet incorporated in European or American Guidelines.3,4 In this study, preoperative below knee GSV reflux was present in 65% and 68% of the patients in RFA and HL/S, respectively. This is consistent with pervious data ranging from 41 to 81%. 15 However, we did not find GSV reflux below the treated area to be statistically related to remaining reflux after intervention. Only two or more incompetent calf branches were statistically significant associated with remaining reflux (Table 4). Ninety-two per cent of the limbs with no remaining reflux demonstrated less than two incompetent branches. However, since 70% of the limbs with remaining reflux displayed less than two incompetent branches, our results suggest that there are additional factors, beyond calf branches, that contribute to non-normalized refilling times after treatment. There was a tendency for SSV incompetence to be associated with remaining reflux, but the results were not significant. Further, no significant association was seen regarding other factors, such as sex, C in CEAP, type of intervention (HL/S versus RFA) or incompetent perforators. Although incompetent calf branches are likely to increase the total burden of reflux and conversely decrease SGP refilling, it remains unclear why this was the only statistically significant factor associated with remaining reflux. Further investigations of possible factors involved in non-normalized refilling times are needed.
As anticipated, AVVQ and VCSS improved in a similar fashion in both treatment groups (Figure 4). The clinical effect of distal remaining reflux after intervention is not settled. There are data indicating more significant improvement of AVVQ in patients undergoing complete ablation of the incompetent segment compared to ablation limited to the above knee segment, but these are short-term data (six weeks). 16 Distal DUS detected GSV reflux has also been observed to increase somewhat two years after surgery, but the same authors did not notice any increase in clinical visibly varicose veins below treated area. 15 Further, long-time follow-up has revealed the patients with DUS detected recurrence often reported excellent outcomes regarding symptom relief, cosmetic result and overall satisfaction. 31 In this study, the component of remaining reflux was measured as T50 by SGP in addition to DUS. No differences in AVVQ or VCSS were found in patients with SGP detected remaining reflux compared to those without. This may be explained by the general improvement in venous haemodynamics in all patients after one month.
Limitations of this study are worth mentioning. Methodological errors are inherent problems in both DUS and SGP. However, all DUS examinations were conducted following a strict pre- and postoperative protocol to minimize inter-observer error in the measurements; the coefficient of variation for T50 in our setting is 16%, which seems acceptable. 12 Although the standardized model for selective occlusion of superficial veins has been validated by ascending phlebography, it should be noted that incomplete superficial occlusion may occur in patients with severe obesity or in patients with severe skin changes.12,13 Refilling time is also affected by the arterial inflow and postoperative changes in arterial inflow cannot be excluded. 32 It is thus difficult to exactly compare refilling time between pre- and postoperative SGP with superficial occlusion. SGP measurements of volume changes require a cylindrical shape of the evaluated object. Based on this, no absolute quantitative volume measurement was possible on the foot. Nevertheless, it is possible with our method to calculate the relative maximal reflux in per cent of expelled volume, 12 and an advantage with distal evaluations of refilling time is the possibility to characterize the total impact of the reflux disease.8,13
In conclusion, remaining reflux evaluated with T50 was detected by SGP one month after treatment despite technically successful GSV treatment validated by postoperative DUS. The cause was mainly attributed to remaining reflux below treated area, most notably if the patient had two or more incompetent branches. This indicates that postoperative improvement of haemodynamic parameters measured by plethysmographic methods is not comparable to normal venous function in the majority of patients. However, no differences in severity of varicose disease or QoL were seen in patients with optimal and sub-optimal haemodynamic treatment. Further long-term follow-up needs to be conducted in order to evaluate if sub-optimal haemodynamic treatment detected by SGP in the initial postoperative phase is related to more severe clinical symptoms in a later stage.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from Linköping University Hospital Research Fund, Linköping, Sweden. ALF Grants, Region Östergötland, Linköping, Sweden.
Ethical approval
The study was approved by the regional ethical review board in Linköping (DNR2011/484-31), Sweden and written informed consent was provided by each participant.
Guarantor
POE Nelzén.
Contributorship
POE Nelzén and H Zachrisson were involved in patient recruitment and/or protocol development. J Skoog and POE Nelzén wrote the first draft of the article. POE Nelzén, J Skoog, M Öster and H Zachrisson were involved in data analysis. All authors reviewed and edited the article and approved the final version of the article.
Acknowledgements
We thank Mikael Ekman for technical support and Nora Östrup for linguistic corrections.