
Abstract
Objective
the aim of this study was to assess the results of mechanochemical endovenous ablation either in the primary or recurrent saphenous vein insufficiency, including only patients with veno-venous shunt type III.
Methods
retrospective analysis of a prospective study of patients with symptomatic chronic venous insufficiency who underwent ClariVein® technique. A total of 134 saphenous veins were included between August 2017 and August 2018. Follow-up was performed by Duplex ultrasound at 1, 6 and 12 months. Primary endpoints were technical and anatomical success. Secondary endpoints were the need for further treatment of varicose collateral veins by sclerotherapy, outcomes regarding recurrent insufficiency and clinical success.
Results
A total of 111 great saphenous veins and 23 small saphenous veins were treated with a technical success of 95.6%. The overall anatomical success rates at 1, 6 and 12 month were 96.2%, 88.8% and 84.4%, respectively, without differences between primary and recurrent insufficiency. Deferred sclerotherapy over varicose collaterals was carried out in 28% of the patients with anatomical success. Clinical improvement was achieved in 87.3%.
Conclusions
MOCA technique has proven to be an effective technique, although additional treatment over varicose collaterals could be necessary in up to one-third. Atrophy of the saphenous vein and the lack of persistent varicose collateral veins during follow-up seem to be indicators of successful therapy.
Introduction
The prevalence of chronic venous disease (CVD) has been reported to be as high as 60%. It is an important cause of patient discomfort and has a significant impact on quality of life and healthcare resources. The advanced stages of CVD (CEAP clinical stages C3 to C6) appear to affect about 5% of the population, with an estimated prevalence of 1 to 2% of the end stages of CVD (CEAP clinical stages C5 to C6). 1
For decades the gold standard for the treatment of CVD was surgery. Recently, a new technique named Mechanochemical Ablation (MOCA) has been developed. In this technique a mechanical damage to the endothelial cells of the vein is produced by the tip of a rotating catheter while sclerosant is released through the catheter-wire. 1 MOCA of the great saphenous vein (GSV) and small saphenous vein (SSV) does not requires tumescent anesthesia. High occlusion rates with significant clinical improvement at short-mid term have been described,2,3 with a low rate of post-procedural pain and a fast resumption to daily activities, 4 although the NICE guidelines still recommend endothermal ablation as first line strategy if feasible. 5
Up to now, there are not studies addressing the behavior of MOCA based on the type of veno-venous shunt of the CHIVA strategy. The aim of this study is to analyze the results of MOCA either in the primary or recurrent GSV/SSV insufficiency, including just patients with veno-venous shunt type III, which is also de most frequent. 6
Methods
Patients with symptomatic CVD with CEAP clinical stages ≥C2 that underwent MOCA of saphenous veins (SV) using the ClariVein® (Vascular Insights LLC, Quincy, MA) device. They were prospectively collected in a computerized database. The assessment included age, sex, height, weight, BMI, baseline comorbidities, previous venous procedures, DUS examination and antiplatelet/anticoagulation regimen (when applicable). Only patients treated between August 2017 and August 2018 were included in order to achieve a 1-year follow-up in every single case.
A Duplex-ultrasound (DUS) examination was carried-out to assess venous insufficiency. Inclusion criteria were as follows:
GSV or small SSV insufficiency. Rectilinear pathway of at least 10 cm from the saphenofemoral (SFJ) or saphenopopliteal (SPJ) junction. GSV or SSV diameter <10 mm.
Patients were excluded if one of the following situations were noted:
Veno-venous shunt different to type III according to CHIVA (the French abbreviation for ‘cure conservatrice et hemodynamique de l'Insufficience veineuse en ambulatoire’) European Association. Deep venous insufficiency. Deep or superficial venous thrombosis. Peripheral artery disease (Rutherford classification ≥3).
7
Target limb infection. Pregnancy or lactating. Recorded allergy to Polidocanol. Disulfiram use.
DUS was performed not only to prove the insufficiency of the GSV or SSV and assess inclusion/exclusion criteria, but also to create a map of the venous anatomy and blood flow. Thus, escape point, reflux course, re-entry point, as well as origin and features of varicose collateral veins (VCV) were examined.
Escape point is defined as blood flow from an internal venous compartment (from now on femoral vein if we refer to GSV or popliteal vein if we refer to SSV) to an external venous compartment (GSV or SSV). Reflux is defined as retrograde flow > 0.5 seconds at the SFJ (and/or over the GSV course) or at the SPJ (and/or over the SSV course), in the standing position after the provocation of a Valsalva manoeuver or manual calf compression respectively. Re-entry point is where reflux flows back to the deep venous system after its superficial course.
Based on these findings, the type of veno-venous shunt was written down. A veno-venous shunt is defined as a flow diversion with direction opposite to physiological. The classification of the shunts represents a hemodynamic categorization of the varicose syndrome, which gives information about the clinical repercussion and the best approach to deal with (Figure 1). Just patients with type III shunt (escape point between deep venous system and GSV/SSV with a collateral along its course of reflux with sustained reflux) were included. We decided not to include type I shunts (escape point between the deep venous system and GSV/SSV, without VCV interposition) in order to avoid generating biased results due to shunt’s type.
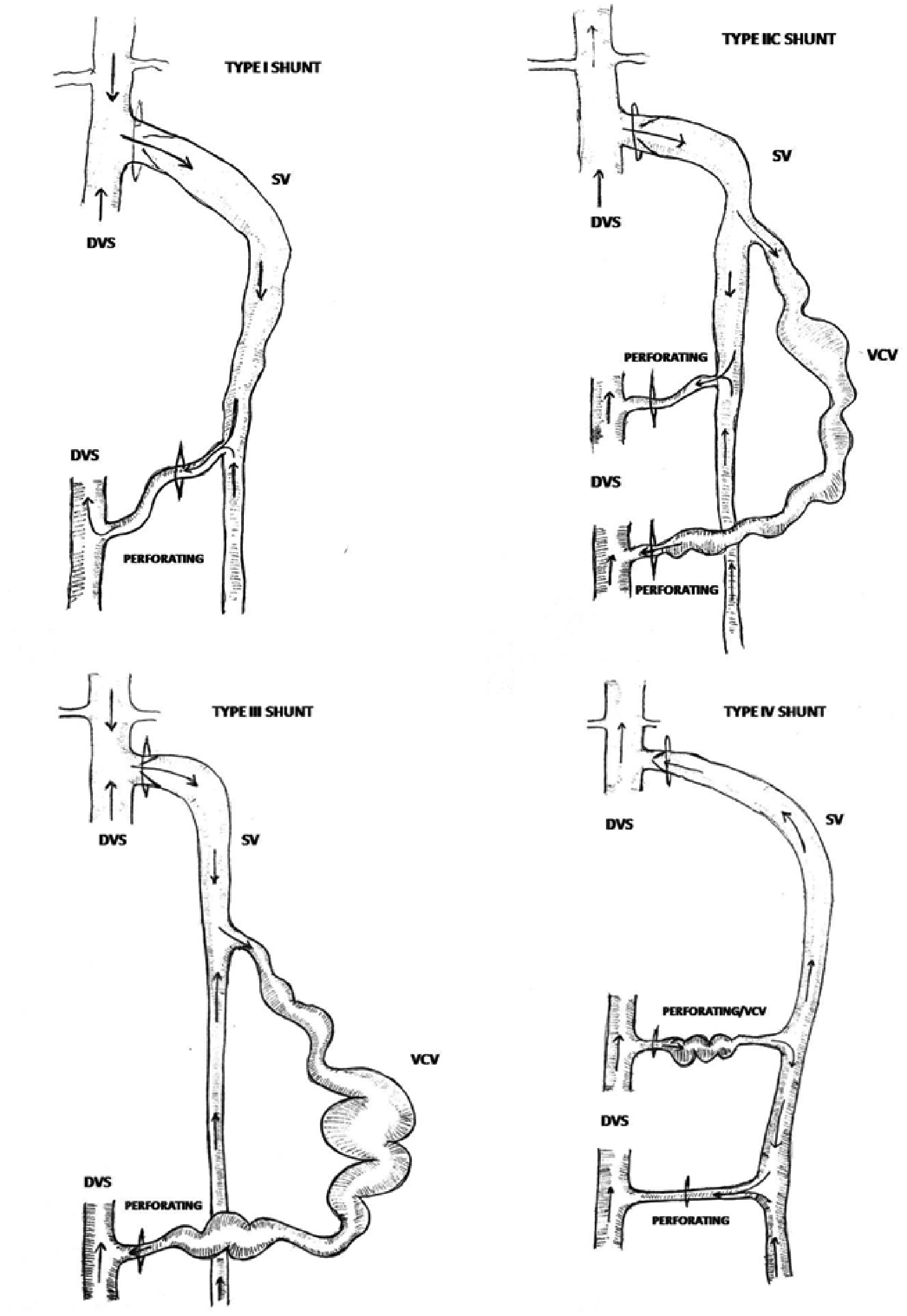
Hemodynamic classification of the veno-venous shunts (not all the shunts are included).
The procedure was performed under local anaesthesia and percutaneous ultrasound guidance access. Through a 4 F sheath, the ClariVein® device is advanced up to 2 cm below the SFJ or SPJ. Wire rotation is activated prior to sclerosant injection with continuous catheter withdrawn. Four Polidocanol sclerosant vials were used for GSV and 2-3 vials for SSV (from practitioner point of view according to target vein length and diameter). Each vial contains 2 ml with 2.0% Polidocanol and the maximum recommended volume per treatment session should not exceed 10 ml, according to the instructions for use. No concomitant treatment over VCV was performed during the same procedure.
Routinely DUS check for deep venous system patency and lack of SV compressibility was performed after the procedure. A compressive bandage was applied prior to discharge from the forefoot to the groin whether GSV was the target vein or from the forefoot to the knee in case of SSV. The bandage is replaced to compression stockings 24 hours later and maintained during daytime for fifteen days from then on. Patients were instructed to administrate Fraxiparine 5700 IU/0.6 ml daily during three days in order to reduce deep venous thrombosis risk. Follow-up visits with a DUS assessment and clinical examination were carried-out at 1, 6 and 12 months. There was no loss of follow-up.
Primary endpoints were technical success and anatomical success. Secondary endpoints were the need for further treatment of VCV with sclerotherapy using Polidocanol foam (Aetoxisclerol®, Kreussler, Germany), outcomes regarding recurrent varicose veins after any previous open treatment (stripping or CHIVA), clinical success and complications. Technical success is defined as completed procedure as planned and achievement of immediate and complete SV occlusion after the ablation. Anatomical success during the follow-up was defined as SV atrophy (narrowing with a diameter of less than 3 mm and absence of either blood flow and thrombus) or occlusion (of at least 85% of its length).
VCV status on follow-up was assessed and classified as persistent, occluded or drained. We defined during the follow-up ‘drained VCV’ as that with flow towards deep venous system when walking. In order to assess the VCV, the patient was ordered to walk for 2 minutes. The VCV was straight away evaluated. We considered a ‘drained’ VCV if flow within moved towards deep venous system, becoming empty. A ‘persistent VCV’ was considered as that which remains insufficient. We used the duplex color and 2D mode to determine these measurements.
SPSS® v.20.0 statistical package (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Continuous variables are presented with mean and standard deviation. Categorical data were compared using de Chi-square or Fischer exact test for parametric and non-parametric studies respectively. Comparisons between a categorical and a continuous variable were analysed using T-Student or Mann–Whitney U test for parametric and non-parametric data. Statistical significance was assumed at p < 0.05.
Results
A total of 116 patients (62.7% females) and 134 legs were treated during this period of time. The mean age was 55 ± 11.5 year-old and the mean body mass index was 27.42. Within this sample there were 111 GSV (82.8%) and 23 SSV (17.2%). The vast majority (94.8%) had a CVD clinical stage ≥3. Baseline comorbidities are summarized in Table 1. Average SV diameter was 6.83 mm but no differences were found between GSV and SSV (6.85 ± 1.44 vs 6.82 ± 1.55 mm; p = 0.875).
Baseline characteristics.

Technical success was achieved in 95.5% of the patients. Regarding patients with technical failure, 1 (0.75%) was unable to be treated and 5 (3.75%) had a suboptimal result due to inability to advance the device to the most proximal vein segment; therefore, only partial treatment was completed. The reason why technical success could not be accomplished was the presence of spasm or venous tortuosity, which was unnoticed during preoperative DUS. None of these patients (unable and sub-optimal) got anatomical success, but clinical improvement at 12 months was noticed in 3 of them (3/6), nevertheless.
Anatomical success at 1, 6 and 12 months were 96.2%, 88.8% and 84.4%, respectively. Interestingly, there were not statistical differences between GSV and SSV at 1 and 6 months, but there were actually at 12 months: 95.0% vs. 96.4% (p = 0.8), 90.1% vs 82.6% (p = 0.3) and 88.3% vs. 69.6% (p = 0.02), respectively (Figure 2). A subgroup analysis arose that SSV with diameters > 8 mm were associated to a higher recanalization rate than SSV < 8 mm at 1-year follow-up (p = 0.033). No associations were found between diameter (p = 0.86), age (p = 0.46), body mass index (p = 0.63) or CVD clinical score (p = 0.16) and anatomical success.
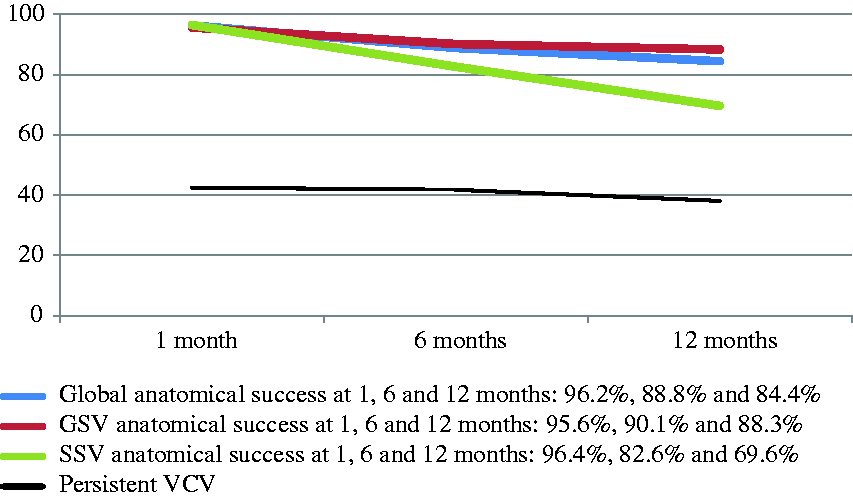
Global, GSV and SSV anatomical success, as well as varicose collateral veins (VCV) persistence at 1, 6 and 12 months of follow up.
On DUS examination, VCV were persistent in 42.5%, 41.8% and 38.1% (51 patients) at 1, 6 and 12 months (Figure 2). Up to 28% of patients with anatomical success (32 out of 113) at 12 months still had persistent VCV (Table 2). Although most experienced clinical improvement, a total of 39 out of 134 patients (29%) required a secondary treatment over the VCV. Some persistent VCV were not treated as they were present in elderly population with clinical improvement and an aesthetic result was not the goal.
Analysis of varicose collateral vein (VCV) status in patients with anatomical success (saphenous vein occlusion or atrophy) at 12 months of follow-up.
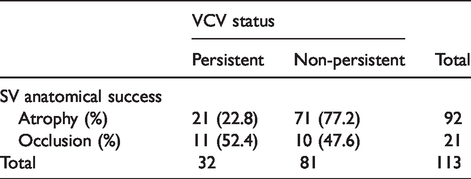
We carried out another subgroup analysis among patients with anatomical success and the VCV status at 12 months. Cases with anatomical success were split between patients with SV occlusion (18.5% of the cohort) and SV atrophy (81.5% of the cohort). SV atrophy was associated to a higher number of non-persistent VCV (77.2%) than those with SV occlusion (47.6%), which was more associated to persistent VCV relatively (Table 2).
Sclerotherapy was performed by direct vision, using 2% Polidocanol foam. None of these cases were treated within the first postoperative month. Twenty-five cases received sclerotherapy at 6 months, achieving a 68% occlusion rate (17 patients) in the next control (12 months). At 12 months, 15 patients were treated, but there is still no available data regarding this group.
ClariVein® was performed in 12 (8.9%) patients with recurrent chronic venous insufficiency after a previous open treatment. Results show an anatomical success of 91.6% and a VCV persistence of 40% at 12 months.
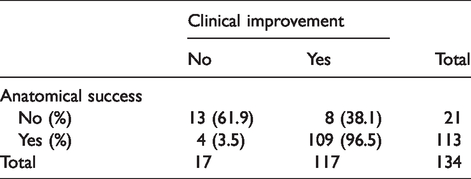
Overall, 117 patients (87.3%) reported clinical improvement after MOCA. Worth to mention that 109 out of 113 patients with anatomical success at 12 months reported clinical improvement but all (100%) in whom either an occluded or a drained VCV was achieved reported clinical improvement (Tables 3 and 4). There were no major complications. Skin staining occurred in 14.9% of the patients, thrombophlebitis in 2.9%, oral paresthesia (a slight tingling sensation) in 2.2% and aura during the procedure in just one patient.
Analysis of clinical status in patients with or without anatomical success at 12 months of follow-up.
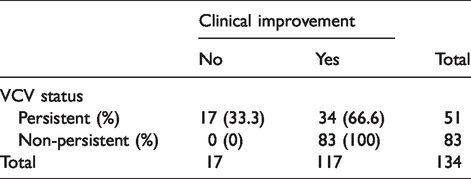
Analysis of clinical status in patients with or without varicose collateral vein persistence at 12 months of follow-up.
Discussion
The lack of technical success rate was 4.5%. In our experience, key points while performing an endovascular treatment of the SV are puncturing and advancing the device through the vessel. Tortuosity, small diameter at the access point, spasm due to repeated puncture attempts and the presence of several collateral veins are some issues that may complicate the device navigation.8,9 A thorough DUS exam, surgeon’s experience and the compliance within the device instructions for use minimize the possibility of an unsuccessful treatment.
Our anatomical success, influenced by the technical success, was 96.2%, 88.8% and 84.4% at one, six and twelve months respectively. These outcomes are lightly inferior compared to other similar published studies regarding MOCA technique,3,10 but we included GSV and SSV, as well as cases with previous failed treatments. In addition, there are different criteria8,11 or lack of accurate criteria12,13 when defining what is considered to be anatomical success, making comparison difficult to perform.
Comparing to endovenous thermal techniques, non-thermal seems to be at least as effective at one year, 14 and is associated with shorter operating times,15,16 as no tumescent anesthesia is needed. The MARADONA trial is a multicentre study that compared the treatment of the GSV disease between MOCA (105 patients) and radio-frequency (104 patients). 17 This study reported a lower anatomical success rate at one and two years in the MOCA group (83.5% and 80% vs 94.2% and 88.3%; p = 0.025 and p = 0.066 respectively) due to partial recanalization. Nevertheless, clinical success rates at one and two years were similar (88.7% and 93% vs 93.2% and 90.4%; p = 0.315 and 0.2 vs p = 0.010 and 0.5) with a faster improvement in the Venous Clinical Severity Score (VCSS). In a similar line, the LAMA trial, comparing EVLA (endovenous laser ablation) with ClariVein® at 12 months, reported a GSV occlusion rate of 91% vs 77% (p = 0.020), but there was no difference in clinical improvement between the two techniques. 18
More recently, the ablation with cyanocrilate (CAVA) has expanded the therapeutic options, although MOCA achieved anatomical results at least non-inferior at 6 and 12 months (94.7 for MOCA vs 94.8% for CAVA and 94.1% for MOCA vs 89% for CAVA) 19 and is more cost effective than CAVA. 20
After a subgroup analysis, we did not find differences between vein diameter or advanced CVD stages and a higher rate of recanalization in accordance to previous published studies.4,8,9,21 However, we found that SSV with diameters larger than 8 mm were associated with lower anatomical success rate. We have not found studies addressing this issue but worse results at 6-12 weeks are reported when treating SSV (92% vs 84%). 8
One important factor that may determine the result of MOCA is the amount of sclerosant used, as well as its concentration. Following the manufacturer instructions, we use 4-6 ml of 2% Polidocanol for the treatment of SSV and 8 ml for the GSV. Some authors recommend using 2 ml of 3% Polidocanol along the first few centimetres of the GSV in order to prevent from early recanalization as most of these occur in the proximal segment.4,8 The mechanism of this is unclear but it is stated that flexion-extension forces present at this point could play an important role in the foreseeable results. 22
In a RCT regarding MOCA using Polidocanol at 1% (foam), 2% and 3% (liquid) concentration, GSV occlusion rates at 6 weeks were 56.5%, 100% and 96.4% respectively. 23 As Polidocanol concentration increases, the recommended length of treatment is shortened in order to not exceed the maximum dose. 23 Even thought Sodium tetradecyl sulphate (STD) is an alternative sclerosant agent with better results than Polidocanol in in-vitro studies, there is no evidence supporting a significant difference in humans. 10 STD allows up to 15 ml of 2% to be used in a single treatment, instead of 10 ml of 2% Polidocanol. 13
As seen in our study, up to one third of the patients treated by ablation may need additional procedures over VCV during follow-up,24,25 despite achieving anatomical success. Nowadays, there is still no consensus about when and which VCV should be treated. In our study a persistent VCV was the criteria to perform sclerotherapy, unless elderly population referring clinical improvement in whom an aesthetic result were not a goal. We assessed the behaviour of the SV and its relation with VCV status during FU. We noticed that the natural evolution of the successfully treated SV changed from an early phase of occlusion to a late phase of atrophy. Interestingly, atrophic SV are more associated to non-persistent VCV (77.2%) than those occluded SV (47.6%). This may indicate that the SV evolution towards atrophy is closely related to a positive effect over the VCV and thus, less prone to a secondary treatment with sclerotherapy.
Some authors say that all VCV are a contributing factor for lacking of clinical success and thus, they advise to treat them in a systematic way. 26 From our point of view, deferred VCV treatment when necessary rather than a systematic sclerotherapy in the same stage as MOCA avoid overtreatment. Performing a concomitant approach in the same stage leads to overtreat patients who would not need it. We also base this approach on the theory that sclerosant agent during MOCA is supposed to flow trough the VCV, treating them in an indirect way.4,27 Moreover, a successful treatment of the SV may reduce the pressure column as much to become an incompetent VCV into a drained one while walking. However, a prospective observational study have shown that concomitant treatment of VCV improves quality of life, pain score, and reduces the risk of postoperative thrombophlebitis. 28
We have not found data analysing the results of the ClariVein® for the treatment of recurrent varicose veins, where fibrosis and neovascularization may increase the risk of an open re-intervention. Our results regarding this issue are similar to those obtained for the treatment of primary disease, with an anatomical success rate of 91.6% at 12 months. Although promising, these results need further and statistical empowered studies that could confirm the effectiveness in such cases.
The clinical success rate after 12 months was 87.3%, slightly superior to the anatomical success rate of 84.4%. This shows that some patients improve clinically despite the lack of a complete successful result. The study by Ekeeren in 2014 was unable to prove differences in the clinical status referred by patients between those with a successful result and those with recanalization. 4 The latter favors endovascular treatment versus open repair, as lack of technical success in open repair is associated to an absence of clinical improvement. 28
Worth a mention that all the patients with a successful treatment of VCV (occluded/drained when walking) had clinical improvement at 12 months in comparison with a 96.5% (109/113 patients) of those with anatomical success. Although the correlation between both groups is high, the finding in DUS during follow-up of an occluded VCV or a drained when walking VCV is more associated to clinical success than the SV status, as far as our experience is concerned.
The patients were instructed to wear compression stockings for fifteen days and to administrate Fraxiparine 5700 IU/0.6 ml daily during three days in order to reduce deep venous thrombosis risk. Currently, there is not solid evidence-based justification, but a recent consensus in UK and Ireland concluded that prophylaxis with low-molecular-weight heparin following superficial endovenous treatment is recommended. 29
This study arises some questions as the different behaviour and results that ClariVein® could arise in patients with type I vs. type III shunts, or which patients benefit most from an associated VCV treatment. This study has also several limitations, as there is no control group and data was retrospectively analyzed. We may also have missed a deep venous thrombosis as we did not check the deep venous system routinely. Clinical comparisons with other studies are difficult as no clinical scales, like VCSS or AVVQ, were used. Finally, long-term data is still not available.
Conclusions
MOCA has proven to be a safe and effective technique according to our results for the treatment of primary varicose veins as well as recurrent disease, although complimentary treatment of VCV could be necessary in up to one-third of the cases. SV atrophy and the lack of persistent VCV during follow-up seem to be DUS indicators of a successful therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approved by ethical committee from Hospital Universitario Central de Asturias (Oviedo).
Guarantor
VMR.
Contributorship
Literature search: Vicente Mosquera-Rey, Jose Antonio del Castro, Manuel Alonso, Rubén Ansorena, Ángeles Menéndez.
Design: Vicente Mosquera-Rey, Jose Antonio del Castro, Ángeles Menéndez.
Data acquisition: Rubén Ansorena, Ernesto Arenas, Jose Antonio Del Castro.
Treatment: Ángeles Menéndez, Jose Antonio del Castro, Manuel Alonso, Vicente Mosquera-Rey, Ernesto Arenas.
Follow-up: Rubén Ansorena, Vicente Mosquera-Rey, Ernesto Arenas.
Data analysis: Vicente Mosquera-Rey, Ernesto Arenas, Rubén Ansorena, Manuel Alonso.
Manuscript writing: Vicente Mosquera-Rey, Jose Antonio Del Castro, Ángeles Menéndez.
Manuscript review: Vicente Mosquera-Rey, Jose Antonio Del Castro, Ángeles Menéndez, Manuel Alonso, Ernesto Arenas.
Acknowledgements
The authors would like to thank their colleagues LA Camblor and Mónica Pandavenes for assistance in carrying out this research project.