
Abstract
Objectives
To investigate whether radiofrequency endovenous ablation (RFA) of saphenous and perforating veins increases venous leg ulcer (VLU) healing rates and prevents ulcer recurrence.
Method
This prospective, open-label, randomized, controlled, single-center trial recruited 56 patients with VLU divided into: compression alone (CR, N = 29) and RFA plus compression (RF, N = 27). Primary endpoints were ulcer recurrence rate at 12 months; and ulcer healing rates at 6, 12, and 24 weeks. Secondary endpoints were ulcer healing velocity; and Venous Clinical Severity Score (VCSS).
Results
Recurrence was lower in the RF group (p < .001), as well as mean VCSS after treatment (p = .001). There were no significant between-group differences in healing rates. Healing velocity was faster in the RF group (p = 0.049). In the RF group, 2 participants had type 1 endovenous heat-induced thrombosis (EHIT).
Conclusions
RFA plus compression is an excellent treatment for VLU because of its safety, effectiveness, and impact on ulcer recurrence reduction and clinical outcome.
Introduction
Venous leg ulcers (VLU), whether healed or active, still affect about 1% of the adult population 1 despite recent advances in chronic venous insufficiency treatment. They are very important to healthcare providers because of high treatment costs and negative impact on quality of life. The cost of VLU treatment is estimated at over 1% of total healthcare costs in developed countries. 2 One study calculated mean cost of VLU treatment at US$86 per day up to healing and US$42 per day during follow-up, showing how reducing ulcer healing time and preventing ulcer recurrence is important to reduce healthcare expenditure. 3
VLUs can take several weeks, months, or even years to heal and typically have high recurrence rates, in the range of 28% to 38%, according to previous studies.4–6
Factors associated with VLU healing include ulcer location, area, and duration, and female gender. 7
The multicomponent compression bandage system is still the gold standard for treating venous ulceration, 8 since a previous randomized controlled trial (RCT) failed to show improvement in ulcer healing rates with open surgical treatment, although ulcer recurrence risk was reduced. 5 Nowadays, minimally invasive techniques, such as radiofrequency (RFA) and laser endovenous thermal ablation (EVLA) are replacing open surgical procedures, with equivalent efficacy and safety, but shorter recovery times. 9 A recent retrospective observational study reported low VLU recurrence rates in patients who underwent EVLA of saphenous veins.10,11 A recent trial 12 showed that early endovenous ablation of superficial venous reflux resulted in faster healing of venous leg ulcers and longer time free from ulcers than deferred endovenous ablation. Moreover, no other studies have selected patients with VLU for ablation of saphenous vein reflux concurrently with ablation of perforating veins. The impact of treating perforating vein reflux is not clear in recent studies.
The Venous Ulcer: Endovenous Radiofrequency Treatment of Saphenous and Perforating Veins Trial (VUERT trial) was designed to investigate whether RFA of insufficient saphenous and perforating veins could prevent VLU recurrence and increase healing rates.
Methods
Study design
We conducted a prospective, open-label, randomized controlled trial at a single center in Brazil. Consecutive patients referred for treatment of VLU were recruited at an outpatient vascular and endovascular clinic at the Hospital das Clínicas – University of São Paulo Medical School. The trial protocol was reviewed and approved by the local research ethics committee (CAPPesq, register 9725, number 489.142). All patients provided written informed consent before participating in the study, in accordance with the principles of the Helsinki Declaration. This study is registered at Clinicaltrials.gov (Identifier: NCT03293836).
Study subjects
Inclusion criteria were as follows: age 18 to 80 years; at least one active VLU (defined as any break in the skin between the knee and the malleolus that had been present for longer than 4 weeks in a person with chronic venous insufficiency); at least one saphenous and one perforating vein insufficiency in a previous duplex ultrasound; and ankle-brachial pressure index (ABPI) greater than 0.8.
Exclusion criteria were: evidence of significant arterial obstruction (ABPI less than 0.8); previous personal history or current evidence of occlusion; obstruction and previous deep venous thrombosis in the leg with the ulcer shown on ultrasound evaluation (simple deep vein reflux with no evidence of thrombosis and obstruction was not an exclusion criterion); evidence of previous superficial thrombophlebitis in the target saphenous vein; pregnancy; contraindications for surgery even under local anesthetic; suspicion of other causes of ulceration in legs (including inflammatory and malignant causes); inability to walk or severe ankle ankylosis; no evidence of insufficiency of at least one saphenous vein and one perforating vein in the leg with VLU; or saphenous vein diameter greater than 12 mm. For patients who presented with bilateral eligible leg ulcerations, the leg which declared as worse by the patient was considered for the analysis.
Baseline evaluation
Once eligibility had been confirmed, we recorded participants’ personal and clinical details at baseline, including focused physical examination, measurement of ABPI and Body Mass Index (BMI), Clinical, Etiology, Anatomy and Pathophysiology (CEAP) classification 13 and Venous Clinical Severity Score (VCSS). 14 Duplex ultrasound evaluation was performed for all participants.
The VLU area was calculated using Analyzing DigitalImages software (Global Systems Science, Lawrence Hall of Science at the University of California Berkeley, Berkeley, CA, USA) using a digital photograph showing the ulcer measured against a standard centimeter ruler.
An independent physician conducted Duplex ultrasound scans for all participants. Reflux in the deep and superficial veins was evaluated with the patient upright. We defined insufficiency as a reflux time exceeding 500 ms for the Great Saphenous Vein (GSV), the Small Saphenous Vein (SSV), the deep femoral vein, tibial veins, and perforating veins. Only clinically significant perforator veins were considered “pathologic”, with a reflux time exceeding 500 ms, with a diameter ≥3.5 mm, and located beneath a healed or open venous ulcer (CEAP class C5-C6), as proposed by the SVS/AFV Committee. 9 The cutoff value for the femoral and popliteal veins was 1 second. 9
Randomization and masking
We randomly allocated eligible participants to two treatment groups: compression treatment only (CR) or compression plus radiofrequency ablation of insufficient saphenous and perforating veins (RF). Participants were stratified according to ulcer duration (≥6 months or < 6 months) and ulcer area (≥5 cm2 or < 5 cm2) because these criteria are known predictors of ulcer healing. 15 Randomization was performed by an independent remote computerized randomization service run by the University of São Paulo Medical School and delivered in sequentially numbered envelopes. Assignment allocation was independent — in terms of time, place, and person — of assignment implementation.
We did not blind the outcome assessors. The ultrasound evaluations before and after treatment was performed by an independent physician who had no information about patients’ treatment or outcomes.
Procedures and devices
All surgeries were performed by one investigator, who was experienced with RFA and had performed more than one hundred RFA procedures previously.
Intervention group participants were treated in an outpatient setting with standard sterile technique and local tumescent anesthetics. Before skin preparation, all insufficient saphenous and perforating veins were mapped with duplex ultrasound (SonoSite MTurbo® L38 5–10 MHz; SonoSite, Bothell, Washington, USA) and the GSV access site was marked on the mid-leg. After standard sterile preparation, the saphenous vein was accessed by the Seldinger technique, and a 7-Fr Introducer (Cook Medical, Brisbane, Australia) was inserted. A ClosureFast™ catheter (Medtronic, Dublin Ireland) was introduced into the saphenous vein and its tip was positioned 2 cm below the saphenofemoral (distal to the vena epigastrica superficialis) or saphenopopliteal junction. After correct catheter placement, we proceed to treatment of perforating veins, to avoid vasospasm.
All pathological perforating veins (insufficient), regardless of diameter, were treated using ClosureRFS™ stylets (Medtronic, Dublin, Ireland). The perforating vein was located using ultrasound imaging, and a small incision was performed after local tumescent anesthesia with 1% lidocaine. The stylet was introduced and advanced into the perforating vein to fascial level. The ClosureRFG™ radiofrequency generator (Medtronic, Dublin, Ireland) was then connected. Correct stylet position was confirmed by an ultrasound image, blood backflow, and an impedance measurement below 400 ohms measured by the radiofrequency generator. Tumescent solution was infiltrated around the perforating vein to protect skin and the deep venous system. Radiofrequency energy was delivered to the vein wall for four minutes, one minute per quadrant. After ablation of the four quadrants, the stylet was drawn along the vein, performing an additional occlusion. After the procedure, occlusion of the perforating vein was confirmed by absence of blood flow on duplex ultrasound. If the vein had not been occluded, the procedure was repeated.
After treating perforating veins, we infiltrated tissues overlying the saphenous vein with tumescent solution under ultrasound guidance to provoke vein compression. Catheter tip position was confirmed, and the proximal end connected to the radiofrequency generator. The patient was placed in the Trendelenburg position and direct manual pressure was applied to the skin overlying the vein, to improve contact between the catheter electrode and the vein wall. Two 20-second ablation cycles were performed in the saphenofemoral or saphenopopliteal junction segment. Afterwards, one cycle was performed for each 7-cm-long segment. We also performed microphlebectomy of varicose subcutaneous tributaries close to and directly related to the VLU. After the intervention, crepe bandaging was applied to the whole leg and replaced with a compression bandage after 48 hours. Patients were encouraged to walk as frequently as possible and to return to normal activities when they felt able to do so. No peri-procedure anticoagulation was administered.
Patients underwent duplex ultrasound assessment after one week, thirty days, three months, and one year. If perforating vein insufficiency was detected after 30 days, further ablation procedures were performed until all incompetent perforating veins had been occluded.
Both intervention and control groups patients received two-layer compressive bandages (Ktwo™, Urgo Medical, Chenôve, France). Bandages were applied every week until ulcers healed. 8
Clinical assessment and photographic measurement of VLU area were conducted weekly until the ulcer was fully healed. After ulcers healed, patients were given 30–40 mmHg compressive stockings and were advised to use them daily, during standing hours. They were followed-up every two months for one year.
Outcome measures
Our primary endpoints were ulcer recurrence rate at twelve-month follow-up and ulcer healing rates at six, twelve, and twenty-four weeks after starting treatment. We defined healing as complete epithelial cover, free from eschar, with no dressing needed and ulcer recurrence as any break in the skin between knee and malleolus after ulcer healing.
Secondary endpoints were ulcer healing velocity (defined as area reduction in square centimeters per week), improvement in VCSS (before treatment vs. 12-month follow-up) and adverse events.
Statistical analysis
The power calculation was based on ulcer recurrence. The sample size was calculated based on 25% ulcer recurrence at 52 weeks and 15% difference in recurrence between surgical and conservative treatments, according to previous studies.5,16,17Thirty-four participants in each group would give 90% power to detect difference between groups with an alpha error of 5%. Assuming 10% losses to follow-up, we estimated a sample size of 75 participants.
Analyses were conducted by intention to treat and SPSS version 25 was used for all tests. Categorical variables were analyzed using the chi-squared test. Measures of risk, such as hazard ratios (HR), are presented with 95% confidence intervals. We investigated differences in healing and recurrence rates with a Kaplan-Meier plot and, for the primary analysis, we estimated HRs with the Cox model. Ulcer healing velocity (cm2 per week) and post-treatment VCSS were compared using Student’s t test. Statistical tests were two-tailed with a significance level of p = .05.
Role of the funding source
The study sponsor is a government research funding agency (São Paulo Research Foundation – FAPESP) and had no direct role in study design, data collection, data analysis, data interpretation, or writing of this report. The corresponding author has full access to all the data and has final responsibility for the decision to submit for publication.
Results
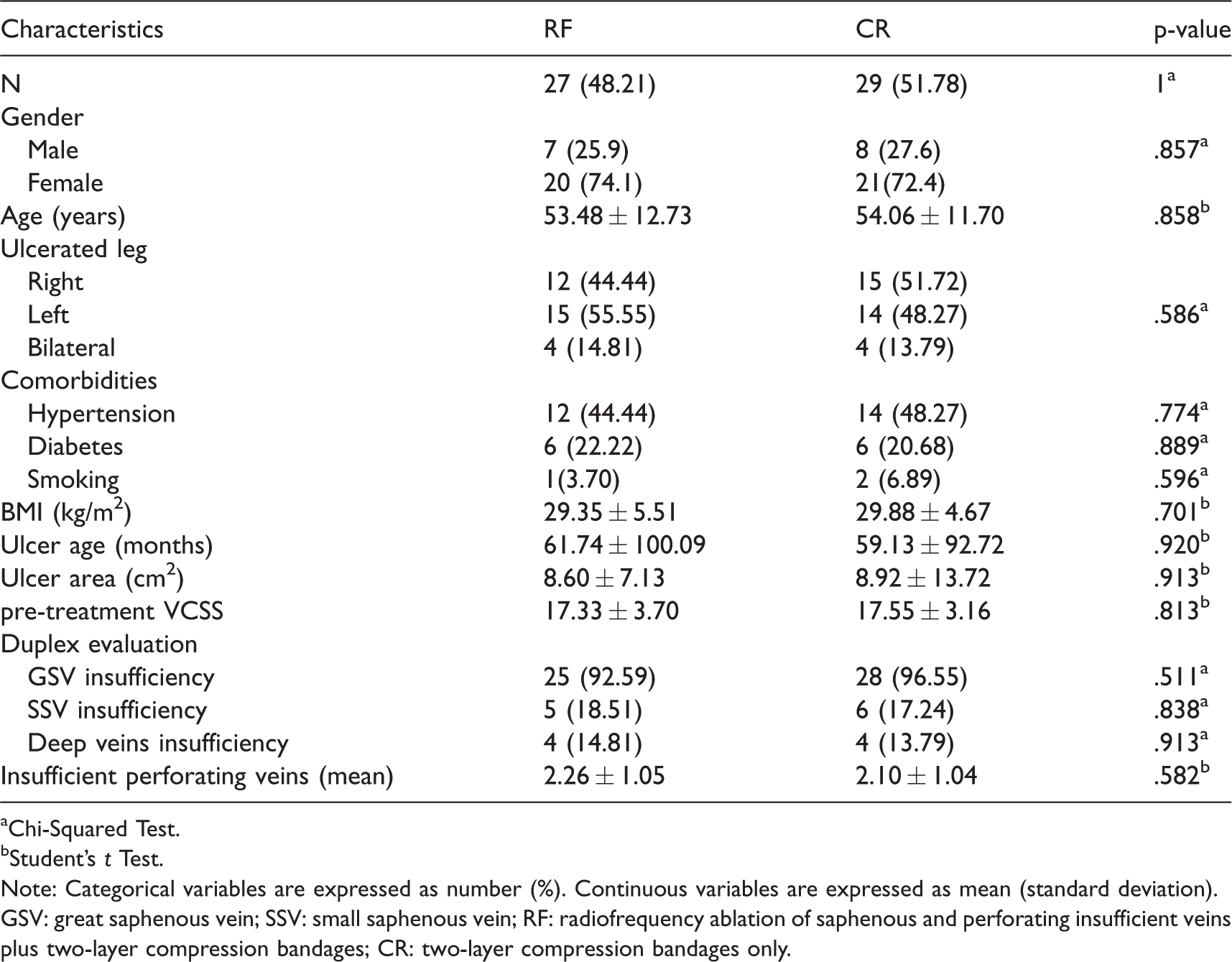
From January 2015 to August 2017, we screened 77 people who were considered eligible for the study, but 21 participants were excluded before randomization for treatment abandonment, pretreatment wound healing, ultrasound evidence of previously unknown deep venous thrombosis, or clinical deterioration. We randomly allocated 56 participants, 27 to the RF group and 29 to the CR group (Figure 1). Baseline characteristics were similar in both groups and are summarized in Table 1.
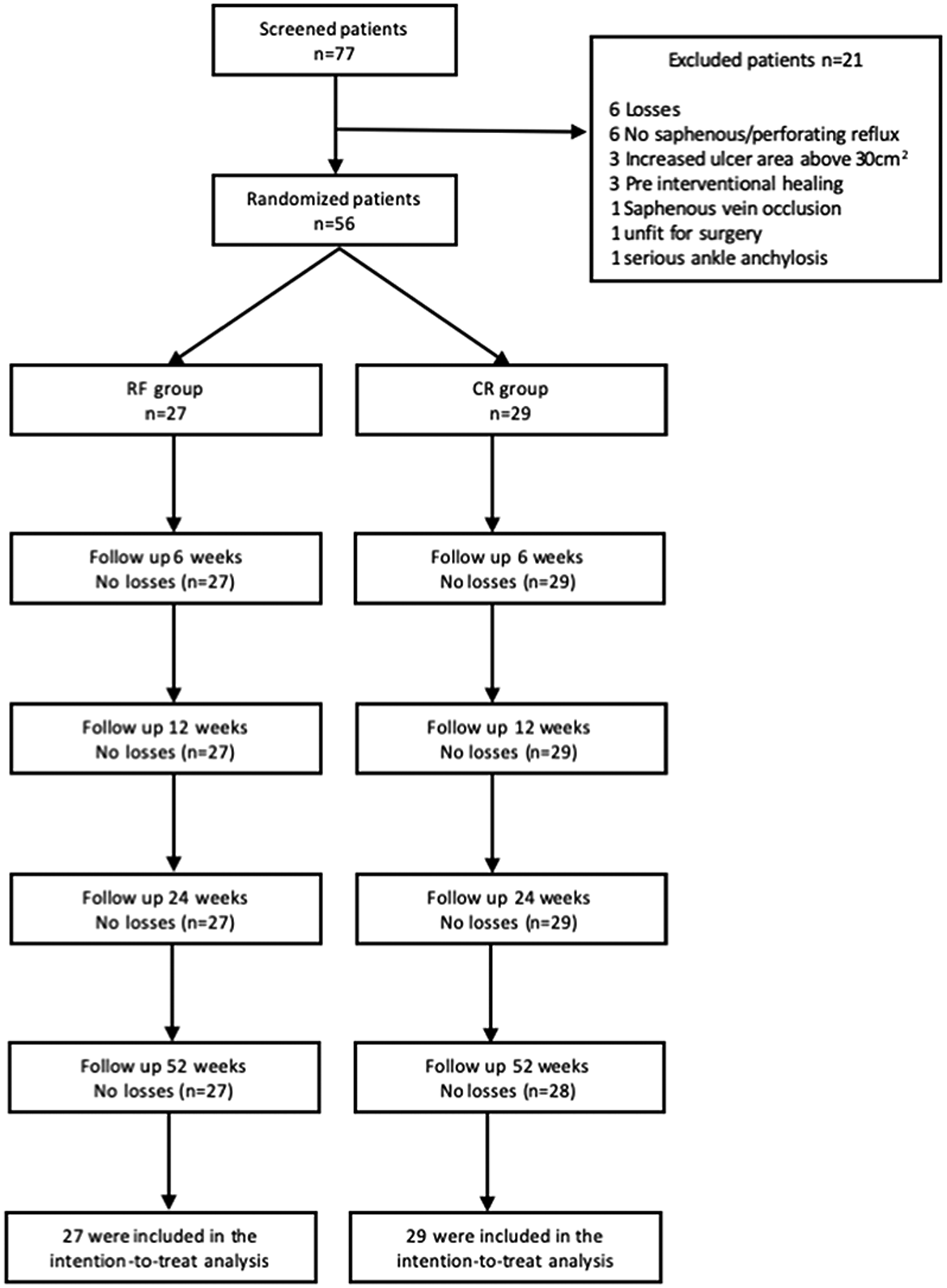
Consolidated Standards of Reporting Trials (CONSORT) flow diagram for subjects involved in the VUERT trial. The patients’ progress through the trial is indicated in the diagram, including final N values for each study group. RF, Radiofrequency ablation of saphenous and perforating insufficient veins plus two-layer compression bandages; CR, treatment with two-layer compression bandages only.
Baseline demographic characteristics of the VUERT trial participants.
aChi-Squared Test.
bStudent's t Test.
Note: Categorical variables are expressed as number (%). Continuous variables are expressed as mean (standard deviation).
GSV: great saphenous vein; SSV: small saphenous vein; RF: radiofrequency ablation of saphenous and perforating insufficient veins plus two-layer compression bandages; CR: two-layer compression bandages only.
Mean follow-up time was 74 weeks for the RF group and 67 weeks for the CR group (p = 0.566). We lost 1 participant to follow-up before 12 months because of death from a comorbid condition (pulmonary insufficiency).
There was just one case of ulcer recurrence over 12 months of follow-up in the RF group (3.7%). However, ulcers had recurred in 44.8% of the CR group after the same follow-up period (HR 0.083; 95% CI 0.011 – 0.0632; p < .001).
There were no significant differences in ulcer healing rates between the groups after 6 weeks (HR 1.176; 95% CI 0.412 – 3.353; p = .762), 12 weeks (HR 1.259; 95% CI 0.649 – 2.444; p = .496), or 24 weeks (HR 1.390; 95% CI 0.768 – 2.516; p = .277). Figures 2 and 3 show Kaplan-Meier survival curves for ulcer recurrence and ulcer healing.
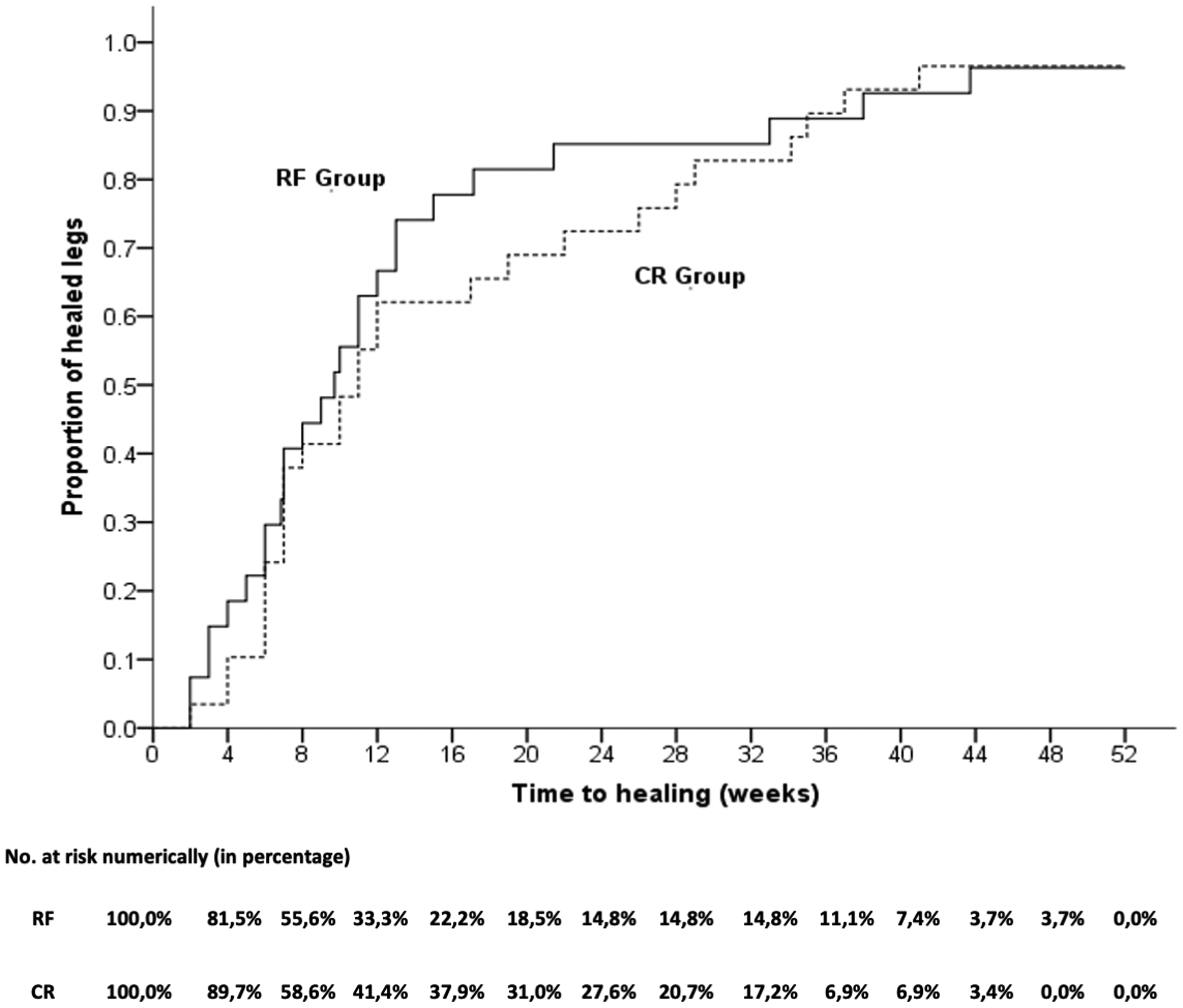
Kaplan-Meier Curves for Time to Ulcer Healing for each treatment group. RF, Radiofrequency ablation of saphenous and perforating insufficient veins plus two-layer compression bandages; CR, treatment with twolayer compression bandages only.

Kaplan-Meier Curves for Ulcer Recurrence for each treatment group. RF, Radiofrequency ablation of saphenous and perforating insufficient veins plus two-layer compression bandages; CR, treatment with twolayer compression bandages only.
However, ulcer healing velocity was higher in the RF group, at 0.739 ± 0.498 cm2 per week, than the control group, at 0.495 ± 0.409 cm2 per week (p = .049).
Mean post-treatment VCSS for the RF group was 8.74 ± 3.04, compared with 11.79 ± 3.47 for CR group (p = .001), showing a better clinical outcome in the group of participants who underwent surgery.
We performed 27 primary radiofrequency ablation procedures in the RF group, treating 25 GSVs, 5 SSVs, and 61 perforating veins. Regarding surgical success rates, 8 participants underwent a second surgical procedure during follow-up prior to ulcer healing. Seven participants were re-operated to perform ablation of 12 perforating veins, which equates to a primary closure rate of 80.32% for perforating veins. One patient had GSV recanalization after 3 months follow-up and underwent another GSV ablation procedure. Therefore, the primary GSV closure rate was 96% (Table 2).
Numbers of radiofrequency ablation procedures performed, including primary surgical procedure and reinterventions, which occurred due to procedure primary failure or early recanalization.
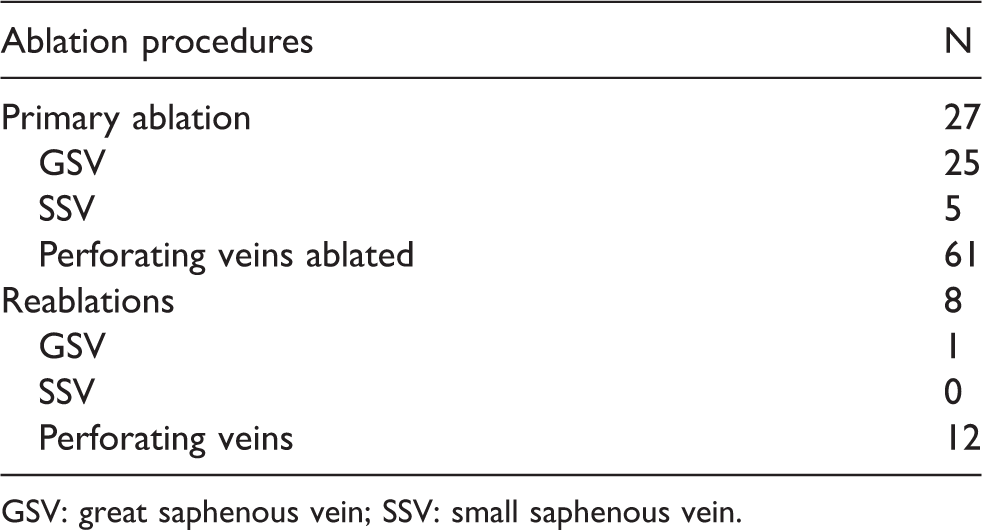
GSV: great saphenous vein; SSV: small saphenous vein.
During follow-up until ulcer healing, 37.93% (N = 11) of the CR group and 25.93% (N = 7) of the RF group participants had clinical signs of ulcer infection (p = .336), all treated with systemic antibiotics. One of these participants, in the CR group, needed hospitalization for intravenous antibiotic infusion. There were no thromboembolic events in the CR group. In 2 participants in the RF group, post-ablation duplex ultrasound examination identified endovenous heat-induced thrombosis (EHIT) involving the saphenofemoral junction but not extending to deep veins (type 1). These participants were treated with oral anticoagulation for 1 month with no complications. One participant who was treated with ablation of the GSV and 3 perforating veins reported persistent paresthesia in the ankle.
Discussion
We found a 91.7% lower risk of recurrence in the surgical group (RF) compared to the compression only group (CR) over the 12-month follow-up period. The difference in ulcer healing between the RF group and the CR group was not statistically significant. However, ulcer healing velocity was significantly faster in the RF than in the CR group.
In addition to the faster healing rate, RFA also caused, as expected, a significant reduction in the signs and symptoms of chronic venous disease, as demonstrated by lower VCSS at the end of follow-up. We had two cases of type 1 EHIT. Although this observation was not significant due to sample size, the potential added risk of DVT with perforator and saphenous RF intervention should be considered when selecting the best treatment.
Several studies have reported results of surgical procedures for venous ulcer healing rates.10,12,16,18–21 A systematic review and meta-analysis comparing surgical intervention and conservative therapy for venous ulcers has shown that venous surgery may improve healing, but the quality of evidence is low because the analysis was based mostly on nonrandomized and small RCTs. 22
As a large and multicenter RCT, the ESCHAR trial 5 offers the best quality evidence for CEAP C6 patients treated surgically. This study provided evidence of how important it is to treat venous reflux to avoid VLU recurrence. However, it was unable to identify the impact of open venous surgery on ulcer healing rates, despite this impact being widely observed in daily clinical practice. The current study design is very similar to the ESCHAR design. However, our population was more homogeneous, including only patients with both superficial and perforating insufficiency. This resulted in similar surgeries for all participants, unlike the previous study, in which several different types of procedures were employed, such as high ligation and stripping of saphenous veins side by side with isolated perforator ligation. This may explain why RFA of saphenous and perforating veins resulted in higher healing rates and faster healing velocity when compared with compression alone.
Furthermore, percutaneous ablation of insufficient perforators enables access to veins found in areas of profoundly damaged skin, which are often neglected in treatment with open surgery, where there is difficulty with dissection and a higher rate of wound complications. 23
Therefore, ultrasound-guided minimally invasive therapies have been recommended in current guidelines for ablation of both insufficient saphenous and perforating veins in patients with open or healed ulcers.9,24 These recommendations were based on a few observational cohorts, case-control studies, and small RCTs.25–28
A large RCT of minimally invasive venous surgery options was only published recently. 12 The EVRA trial showed faster VLU healing time and longer ulcer-free time after early ablation of superficial axial veins with reflux using ultrasound-guided foam sclerotherapy, EVLA, RFA, cyanoacrylate closure, mechanochemical ablation, or a combination of these techniques followed by an effective leg compression treatment. These findings are similar to our results. However, they had a shorter median time to healing, 56 days versus 105 days (15 weeks), which may be because of the higher average size (2.4 cm2 versus 8.6 cm2) and longer duration of ulcers (3.2 months versus 61.74 months) in our patients, and could be related to demographic differences in our population. This shows that endovenous ablation is an outstanding method for improving ulcer healing rates, even in people who have had their ulcers for a very long time.
The key strengths of this trial are, first, its stratified randomized design, resulting in very similar baseline characteristics in both groups, particularly ulcer size and duration. Second, its careful patient selection, including only those with both saphenous and perforating veins with pathological reflux. Lastly, we tested one specific technique (radiofrequency ablation), not several different minimally invasive procedures, and had minimal loss of participants over the follow-up period.
Our trial also has several limitations. We used dual primary end points, as described (ulcer recurrence and ulcer healing), but our power calculation was based on recurrence only. A significantly larger sample size would have been needed to attain the statistical power required to analyze ulcer healing. It is, therefore, a small trial and there were also several dropouts between screening and randomization because of pre-treatment ulcer healing and differences between prior duplex findings and the scans performed for enrollment on the study, such as evidence of a previous DVT. These losses caused a smaller number of participants than recommended by the sample calculation, which can significantly reduce the power of the trial.
Moreover, blinding of patients was impossible because we chose not to perform placebo surgical procedures in the control group, to avoid unnecessary complications related to venous manipulation, following the ethical principle of primum non-nocere. Blinding of physicians was also impossible because clinical signs of surgical treatment are obvious.
Conclusion
Radiofrequency endovenous ablation of insufficient saphenous and perforating veins plus multilayer compressive bandaging is an excellent treatment protocol for venous ulcer patients, because it is safe, effective, applicable to highly damage skin areas, and shows improved ulcer healing velocity and a massive impact on ulcer recurrence reduction and on symptom severity measured by the VCSS.
Footnotes
Authors’ note
The preliminary results were delivered as a podium presentation to the 30th American Venous Forum Annual Meeting, Tucson, AZ, 20–23 February 2018. The mid-term report was presented and won the first prize for Best Scientific Presentation at the 9th Annual Venous Symposium, New York, NY, 5–7 April 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the FAPESP [2015/170044], São Paulo, SP, Brazil. Regsitration NCT03293836 (clinicaltrials.gov).
Ethical approval
This trial protocol was reviewed and approved by the local research ethics committee (CAPPesq, register 9725, number 489.142). All patients provided written informed consent before participating in the study, according to the principles of the Declaration of Helsinki. This study was registered at Clinicaltrials.gov (Identifier: NCT03293836).
Guarantor
IRS.
Contributorship
IRS, JP, WC Jr, FBC, ESS, and FBC designed and conceived the study. IRS, JP, WC Jr, FBC, ESS, and JBS were involved in data collection, interpretation and analysis. JRS, JP, WC Jr, FBC, and ESS were involved in statistical analysis. IRS, JP, WC Jr, FBC, ESS, and FBC wrote the first draft of the manuscript. IRS, JP, WC Jr, FBC, ESS, NDL, PP, and FBC revised the manuscript. IRS, JP, WC Jr, FBC, ESS, NDL, RMPP, JBS and PP approved the final version of the manuscript.
Acknowledgement
We thank Daniel de Almeida M. M. Silvestre for assistance with randomization and preliminary statistical analyzes, Débora Yumi F. Kamikava for the psychological evaluation of the participants and Débora Nolli for the tireless and extremely affectionate way to treat the participants and their ulcers