
Abstract

COVID19 infects cells binding to the angiotensin-converting enzyme 2 receptor. The type 2 transmembrane serine protease facilitates viral infection by cleaving ACE2 and activating the COVID19 structural protein which determines its high virulence. 1 The virulence is increased by the action of COVID19 on the immune system with severe lymphopenia. In later stages of infection, epithelial-endothelial barrier integrity is compromised. Dysfunctional alveolar-capillary oxygen transmission and impaired oxygen diffusion capacity are characteristic features of COVID-19. In severe COVID-19, activation of coagulation and consumption of clotting factors occur. Patients who develop acute deep vein thrombosis during COVID19 infection are in a critical condition, in which deep vein thrombosis represents the iceberg of a general hemostatic derangement.1–3 The aim of our study was to analyze the risk factors and clinical outcomes of COVID19 patients who developed deep vein thrombosis during hospitalization in the acute phase of the outbreak in our region (Lombardia-Italy). From March 1th to April 28th, 942 COVID19 patients with severe symptoms were admitted to our hospital. Patients who developed deep vein thrombosis before admission were not included into the study. Patients with probable immune deficiency (history of tumor diagnosis, previous organ transplant) were not include into the study. Thirty-two patients developed clinical evidence of deep vein thrombosis during hospitalization (mean 393 hours after admission) and they were prospectively evaluated. Nine patients died in a condition of multiple organ failure, 23 patients survived and left the hospital in good general conditions. At 1 month follow-up none of the 23 patients complained of major symptoms. Table 1 shows the clinical characteristics and the laboratory parameters at admission, at diagnosis and 5 days after full anticoagulation and aggressive anti-inflammatory therapy of the patients. All patients were in critical conditions. Treatment included supportive management of acute hypoxic respiratory failure and of hemodynamic instability, antibiotic therapy, correction of the fluid–electrolyte and metabolic unbalances. All patients received prophylaxis with LMWH and anti-inflammatory therapy. At the time of diagnosis full anticoagulation was started and the dosage of anti-inflammatory therapy was increased. All patients had significant alterations of hemostatic and inflammatory parameters at admission. In univariate analysis advanced age (70 years of age or more) and associated specific comorbidities (CAD, diabetes, renal failure) were significant clinical risk factors for mortality (p < 0.0001). High levels of D-Dimers (15.000 or more), Fibrinogen, LDH, and CK were significant risk factors for mortality (p < 0.0001). However, aggressive therapy allowed a 72% survival, including also for patients in critical clinical conditions and with high risk parameters. The most important risk factors were reduced or no change of several laboratory parameters after therapy, including increased CRP values after initial treatment, high levels of D-Dimers and Fibrinogen after full anticoagulation and aggressive anti-inflammatory therapy, persistence of high levels of LDH and CK in all stages of therapy (p < 0.001). The persistence of altered laboratory parameters despite aggressive therapy was more evident in patients 70 years of age or older, with associated diabetes and/or renal failure, who might have had reduced immunologic defenses. The analysis of time-related changes in our study supports the theory that COVID19 infection is mainly related to hemostatic changes in patients with probable immune deficiency. These hemostatic changes may trigger an inflammatory storm which aggravate the hemostatic changes in a vicious circle. There is a high risk group for mortality, characterized by persistence of laboratory changes despite optimal standard therapy, in whom additional therapy should be taken into consideration. Ongoing trials are testing antiviral therapies, immune modulators, and anticoagulants. Monoclonal antibodies and hyperimmune globulin may provide additional strategies. Randomized trial of 103 patients with COVID-19, convalescent plasma did not shorten time to recovery.4,5
Mortality in hospitalized covid19 patients with deep vein thrombosis.
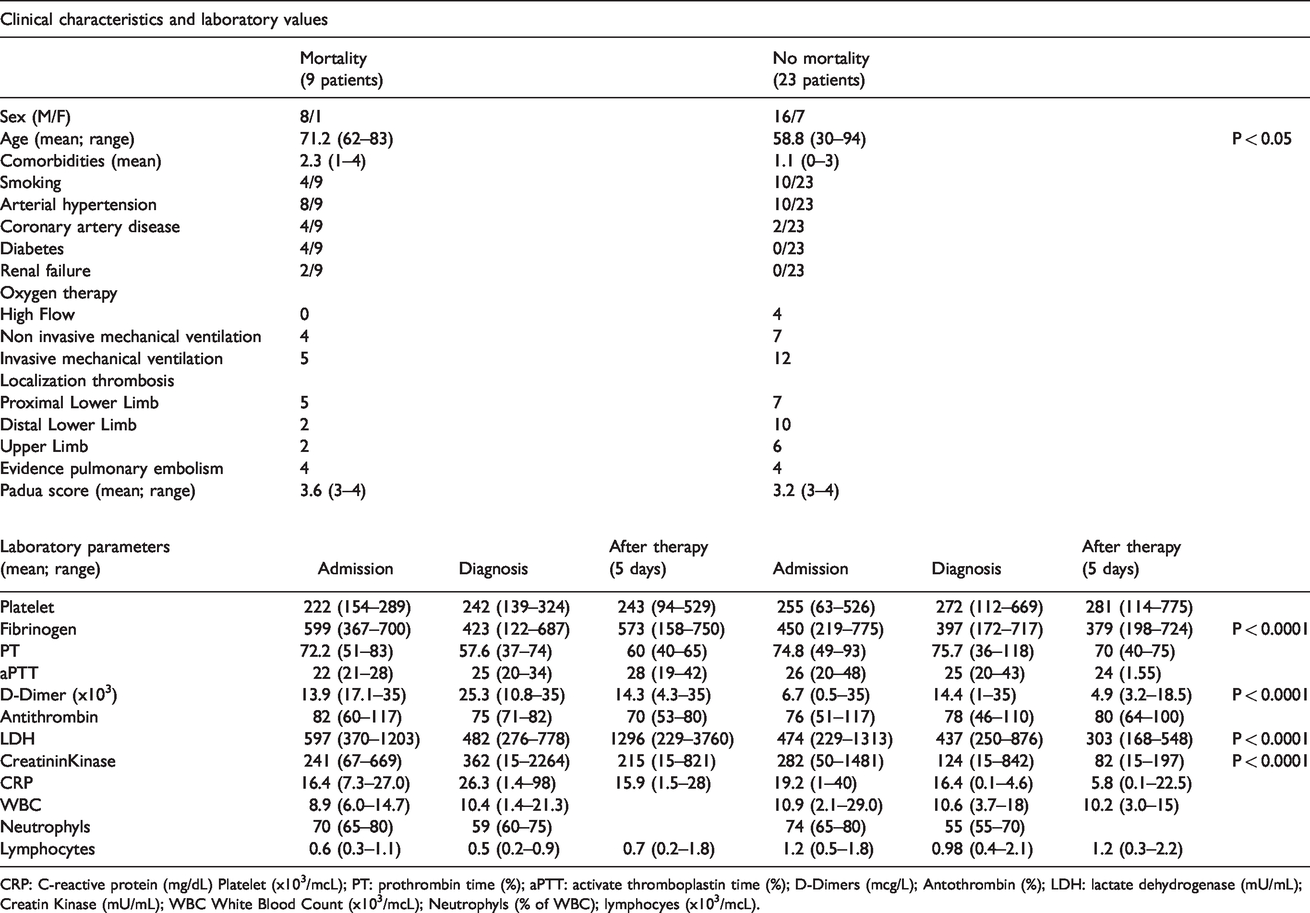
CRP: C-reactive protein (mg/dL) Platelet (x103/mcL); PT: prothrombin time (%); aPTT: activate thromboplastin time (%); D-Dimers (mcg/L); Antothrombin (%); LDH: lactate dehydrogenase (mU/mL); Creatin Kinase (mU/mL); WBC White Blood Count (x103/mcL); Neutrophyls (% of WBC); lymphocyes (x103/mcL).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Institutional Review Board (IRB) approval has been obtained.
Guarantor
FR.
Contributorship
AB, GT, VA and AVS researched literature and conceived the study. ER, FM, RB and FR was involved in protocol development, gaining ethical approval, patient recruitment and data analysis. AB, GT, VA and AVS wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
None.