
Abstract
Background
To review long-term outcomes and saphenous vein (SV) occlusion rate after endovenous ablation (EVA) for symptomatic varicose veins.
Methods
A review of our EVA database (1998–2018) with at least 3-years of clinical and sonographic follow-up. The primary end point was SV closure rate.
Results
542 limbs were evaluated. 358 limbs had radiofrequency and 323 limbs had laser ablations; 542 great saphenous veins (GSV), 106 small saphenous veins (SSV) and 33 anterior accessory saphenous veins (AASV) were treated. Follow-up was 5.6 ± 2.3 years; 508 (74.6%) veins were occluded, 53 (7.8%) partially occluded and 120 (17.6%) were patent. On multivariable Cox regression analysis, male sex (HR 1.6, 95% CI [0.46–018], p = 0.012) and use anticoagulation (HR 2.0, 95% CI [0.69–0.34], p = 0.044) were predictors of long-term failure. On Kaplan-Meier curve, we had an 86.3% occlusion rate.
Conclusion
Our experience revealed a 5-year closure rate of 86.3%. Ablations have satisfactory occlusion rate.
Introduction
Endovenous ablation (EVA) is a minimally invasive procedure used to treat symptomatic superficial venous disease. 1 Prior to their Federal Drug Administration approval in 1999 (radiofrequency ablation – RFA) and 2002 (laser ablation – LA), high ligation of the saphenofemoral junction with great saphenous vein (GSV) stripping and phlebectomy of varices was considered the first line of surgical treatment for symptomatic varicose veins. 2 Both RFA and LA use thermal energy to occlude the insufficient veins from the inside in order to redirect blood flow. 3 On short-term follow-up, patients present with satisfactory results. Therefore, these techniques have risen as the preferred method for the treatment of symptomatic varicose veins with increases of 450-fold in volume of procedures performed in the last decade.4–11
Evidence regarding long-term RFA and LA failure and varicose vein recurrence following these procedures is limited. 12 In this study we aim to present our multi-center experience with RFA and LA, especially regarding outcomes at long-term follow up.
Methods
We identified all patients from our three regional sites (Florida, Arizona, and Minnesota), who underwent EVA of the superficial venous system between January 1998 and December 2018. Data collection included details of each patient’s clinical presentation, comorbidities, medications, surgical management and follow-up through a retrospective chart review. Only those individuals with primary venous reflux disease were included. No patients with concomitant deep venous interventions and outflow iliac venous stents were part of our cohort. Furthermore, a minimum of clinical and ultrasound imaging of at least three years was required for inclusion in this study. In terms of surveillance, local patients did undergo at least a yearly surveillance ultrasound. However, ultrasound and clinical examination was prompted by the patients facing new complaints or concerns. This study was approved by the Mayo Clinic Institutional Review Board (IRB#18-010958). Informed consent was waived by the IRB as this study was deemed minimal risk to patients.
Definitions
Occluded vessels were defined as no flow per ultrasound examination within the lumen of the superficial vein.
Partially occluded vessels were defined as vessels with partial flow per ultrasound examination within the lumen of the superficial vein. The ultrasound evaluation may include scarring and webbing within the vessel with blood flow.
Patent vessels were defined as free flow of blood through the superficial vein being evaluated.
Methods of thermal ablation
The procedure of thermal ablation is performed by accessing the GSV, small saphenous veins (SSV) and the anterior accessory saphenous veins (AASV). Either the RFA or the LA probes are placed 3–5 cm away from the saphenofemoral junction. Subsequently, tumescent solution (1gram of lidocaine and 1 mg of epinephrine in 100 mL + 10mEq sodium bicarbonate in 10 mL added in 1000 mL of 0.9% physiologic saline) is applied around and within the fascia of the vein to be ablated. Finally, the RFA probe is used to heat the vein at a 7 cm vein segment in 20-s intervals. The LA probe is used to heat the vein at a 1 cm vein segment interval every 10 seconds. Once the veins are ablated, the patient undergoes wrapping of the lower extremity with elastic bandages, which remain in place for 24 h. Our primary end point was to determine the closure rate of EVA on long-term follow-up. Our secondary end points included the rate of endovenous heat induced thrombosis (EHIT) in these patients with long-term follow-up and clinical manifestation, etiologic factors, anatomic distribution, pathophysiologic dysfunction (CEAP)/venous clinical severity score (VCSS) scores at time of ablation and on follow-up. Data are reported using means and standard deviations for continuous variables or as frequencies for categorical variables. Differences between categorical variables were tested using χ2 test and differences between continuous variables were tested using Student t-test when deemed appropriate. Multivariable Cox regression models were utilized to assess the risk of superficial veins ablated to remain occluded on long-term follow-up. Differences were considered significant if p was ≤0.05. All statistical analyses were performed using SAS statistical software (SAS Institute, Cary, NC).
Results
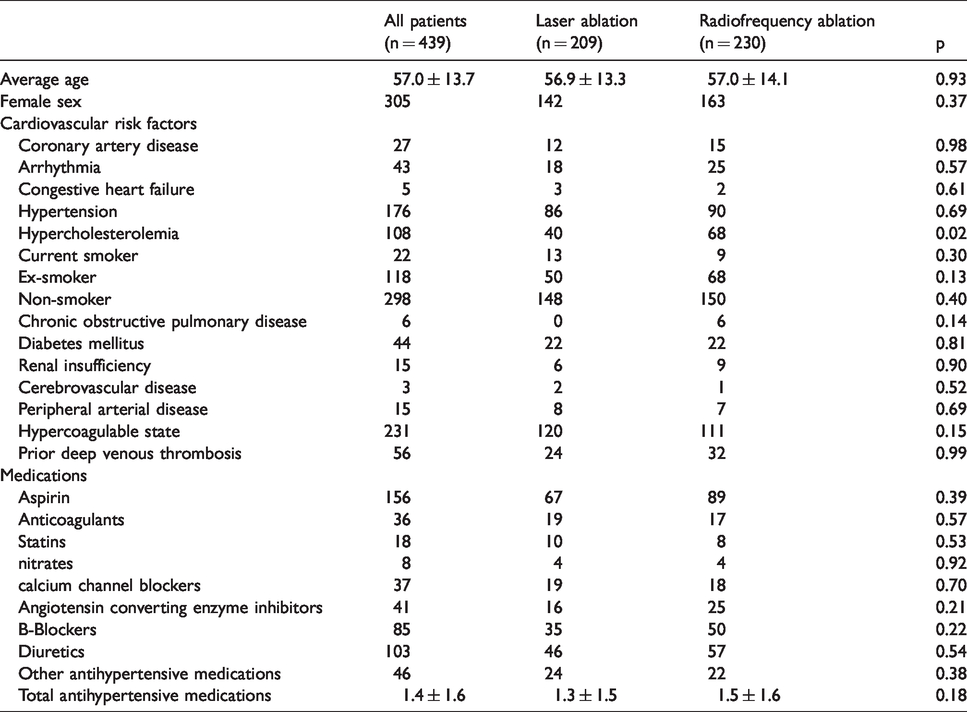
There were 439 patients with 542 limbs were evaluated. 305 (70%) patients were female. Mean age was 57.0 ± 13.8 years. From the demographic data collected, which is shown in Table 1, the only difference among groups undergoing RFA and LA is the number of patients with hypercholesterolemia (68 in the RFA and 40 in the LA group, respectively, p = 0.02). Otherwise, both groups are very similar in terms of risk factor profile and medications. There were 542 GSV, 106 SSV and 33 AASV treated. Mean diameter of the vein treated was 8.4 ± 6.4 mm for GSV, 4.6 ± 1.9 mm for SSV and 6.9 ± 3.0 for AASV. Mean reflux time of vein treated was 6481.4 ± 4103.3 ms for GSV, 4491.9 ± 3421.2 ms for SSV and 5706.9 ± 3364.6 ms for AASV. CEAP classification included 59 limbs CEAP class 6, 31 limbs CEAP class 5, 88 limbs CEAP 4, 148 limbs CEAP 3, 213 limbs CEAP 2 and 3 limbs CEAP 1. Mean VCSS score was 7.7 ± 3.3 prior to ablation.
Demographic data on endovenous ablation patients.
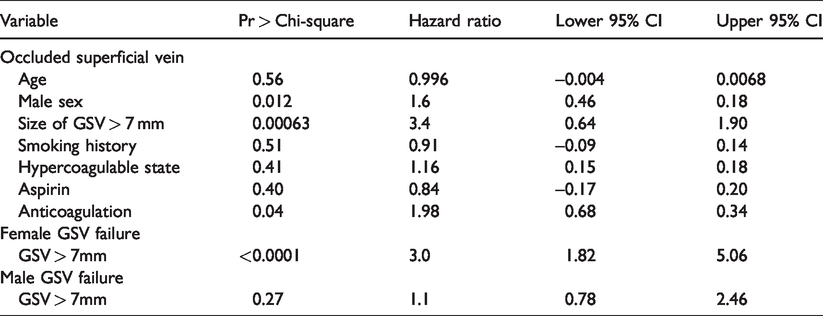
From the 542 limbs evaluated and treated, 292 also underwent stab phlebectomies at the time of intervention and these included 681 veins in total treated including 358 using RFA and 323 using LA. Following ablation, EHIT was identified in 11 (2%) legs with protrusion of the thrombus into the deep venous system without occluding the deep venous system and was managed with oral anticoagulation for 76.9 ± 53.3 days. Postoperative complications were rare: pain was reported in 27 (5.0%) limbs (as per visual analog scale) and hematoma in 5 (0.9%). Follow-up was 5.6 ± 2.3 years; 508 (74.6%) veins were occluded, 53 (7.8%) partially occluded and 120 (17.6%) were patent. There was no difference between patients treated with RFA and LA (Table 2). On follow-up, there were 53 limbs with CEAP class 1, 161 limbs with CEAP class 2, 136 limbs with CEAP class 3, 60 limbs with CEAP class 4, 22 limbs with CEAP class 5 and 39 limbs with CEAP class 6 (Figure 1) with a VCSS score of 5.8 ± 3.7 (p < 0.05). Ulcerations healed in 20 patients. However, there were an additional 14 patients whose ulcerations healed and recurred multiple times during the follow-up period. From those limbs with patent superficial veins on follow-up, 47 limbs were symptomatic and 17 were treated with RFA and 13 with LA, respectively. An additional 17 limbs were offered high ligation of the insufficient vein. On multivariable Cox regression analysis, male sex (HR 1.6, 95% CI [0.46–018], p = 0.012) and use of anticoagulation (HR 2.0, 95% CI [0.69–0.34], p = 0.044) were predictors of long-term failure to occlude superficial veins using EVA (Table 3). Because of potential influence of the size of the veins within the male versus female patients (i.e. male patients having larger veins overall at presentation), we conducted a second regression analysis of the veins according to size and for the great saphenous vein only, a size greater than 7 mm is a predictor of long-term failure (HR 3.4, 95% CI [0.64–1.90], p = 0.00063) (Table 3). Furthermore, this association is only sustained within the female patient population only (HR 3.0, 95% CI [1.82–5.06], p = <0.0001). Finally, on Kaplan-Meyer curve, the rate of occlusion by year five is calculated to be 86.3% (Figure 2).
Veins treated and patency.


CEAP scores before ablation and on long-term follow-up.
Multivariable Cox-regression analysis for factors affecting superficial vein occlusion.
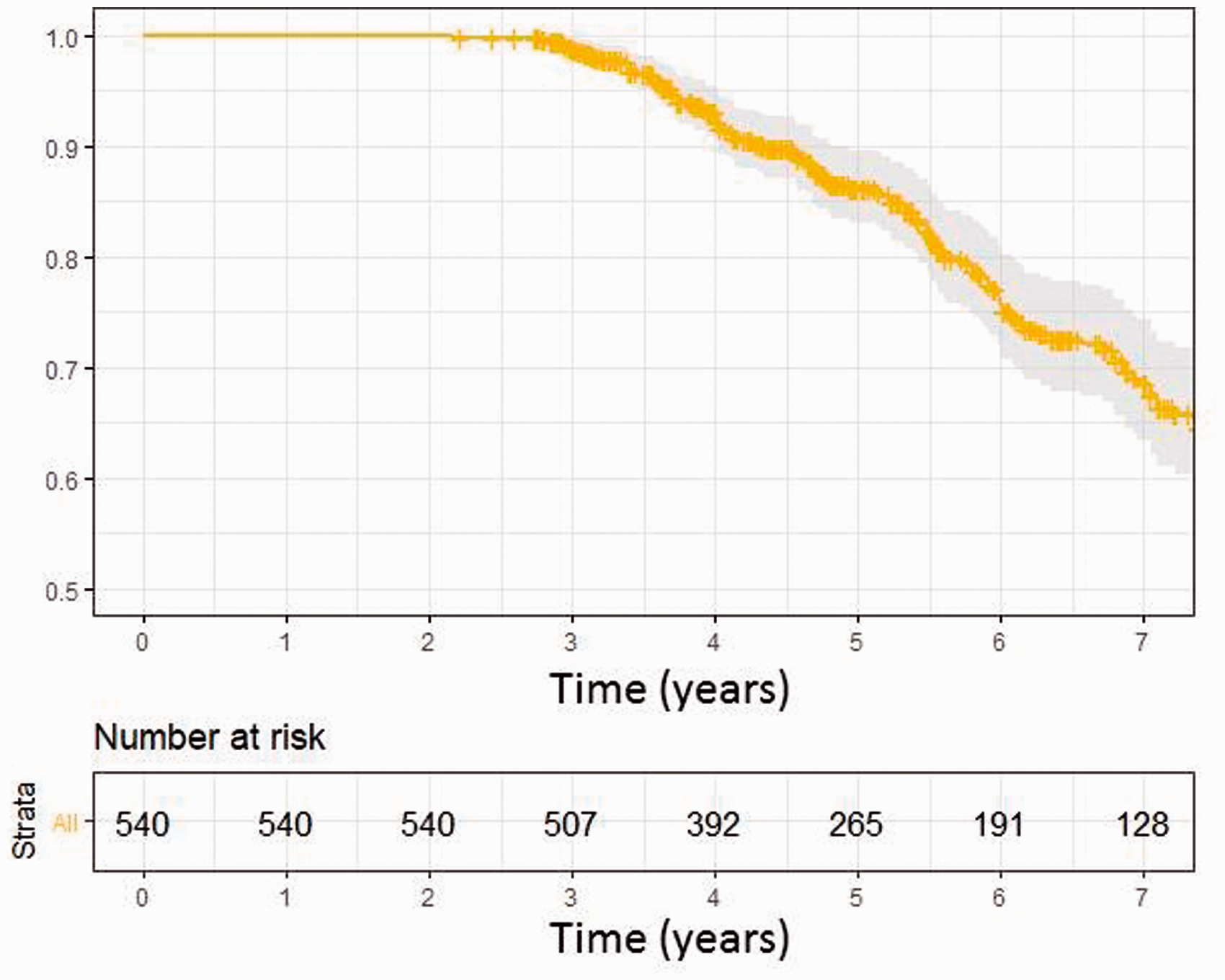
Kaplan-Meyer occlusion curve over time.
Discussion
EVA has become the preferred method for the treatment of symptomatic insufficiency of superficial veins of the lower extremities. In fact, there is a noted 450-fold increase in volume of these procedures performed within the last decade.9,11 However, focus on long-term outcomes is lacking. The few studies available report a successful occlusion rate of 6.2%–33%.13–15 In our current multi-center review, we have a five-year occlusion rate of 86.3%, which is concordant with the available literature; and although success rate is not 100%, patients’ symptoms are significantly improved noting an increase in proportion of patients with lower CEAP class as noted in Figure 1.
The rate of immediate post-operative complications was noted to be low with only 5% reporting any pain (as per visual analog scale), 2% EHIT and 0.9% hematomas; which are very similar to previously published data. 16 Overall, EVA is considered both safe and efficacious with low morbidity even in octogenarians, nonagenarians and centenarians. 17 Reasons for failure of occlusion of the superficial veins was noted to be significantly correlated to the sex of the patient and the use of anticoagulation. We did not appreciate a significant number of patients on novel anticoagulants that it could have made a difference in the outcomes since our cohort reviewed included patients from 1998 to 2018. However, this does not preclude that in the future, the number of patients prescribed novel anticoagulants may be significantly high enough that, it might make a difference in outcome. The short-term outcomes literature does not reveal any correlation between anticoagulation and rate of recanalization. 18 However, on long term follow-up, we were able to demonstrate that the use of Coumadin does have a significant correlation with failure of occlusion of symptomatic superficial veins. Furthermore, there is no sex difference reported in the literature regarding the failure of EVA.19,20 In our cohort, we noticed also a difference due to the difference in size of the great saphenous vein ablated larger than 7 mm in diameter to be a predictor of long-term failure. One could imagine that our male patient population with larger diameter great saphenous veins was at risk for recanalization on long-term follow-up. Finally, although these differences were noted, still the clinical improvement was sustained on follow-up of our patient cohort, as reflected in the CEAP class and VCSS scores improvement (Figure 1).
Limitations
This is a retrospective review of patients undergoing an elective procedure for which most clinicians would not inherently screen and follow-up on a long-term basis as the initial presenting symptomatology has been dealt with a significant improvement noted. Therefore, careful assessment of these patients returning for a follow-up visit greater than one year after the initial presentation represent a biased cohort that could have returned for follow-up possibly as a result of symptom recurrence. Therefore, cautious interpretation of these data is recommended.
Conclusion
Our real-world multicenter experience with saphenous vein ablations revealed a 5-year closure rate of 86.3%. Perioperative thrombotic complications were minor and resolved after anticoagulation therapy. Saphenous ablation for varicose veins using either RFA or LA is safe, effective and results in a durable clinical improvement in symptomatic patients and has a satisfactory occlusion rate. Male sex and use of anticoagulation were predictors of long-term failure.
Article highlights
Type of research: Retrospective review of long-term endovenous superficial venous ablation follow-up from January 1998 to December 2018 at three different institutions.
Key findings: Male sex and use of anticoagulation are predictors of long-term failure of endovenous superficial venous occlusion.
Take home message: Ablation using either RFA or LA is safe, effective and results in a durable clinical improvement in symptomatic patients and has a satisfactory occlusion rate. Male sex and use of anticoagulation are predictors of long-term failure.
Table of contents summary: There is satisfactory occlusion rate in long-term endovenous superficial venous ablation follow-up from January 1998 to December 2018 at three different institutions. On multivariable regression analysis, male sex and use of anticoagulation are predictors of long-term failure of endovenous superficial venous occlusion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Yes obtained through IRB
Guarantor
None.
Contributorship
| Name | Conception and Design | Analysis and Interpretation | Data collection | Writing of manuscript | Critical revision | Agreement of accountable | Approval of Manuscript | Statistical analysis |
|---|---|---|---|---|---|---|---|---|
| Young Erben | x | x | x | x | x | x | x | x |
| Isabel Vasquez | x | x | x | x | x | x | ||
| Yupeng Li | x | x | x | x | x | X | X | |
| Peter Gloviczki | x | x | x | x | x | x | ||
| Manju Kalra | x | x | x | x | x | x | ||
| Randall De Martino | x | x | x | x | x | x | ||
| Haraldur Bjarnason | x | x | x | x | x | x | ||
| Melissa Neisen | x | x | x | x | x | x | ||
| January Moore | x | x | x | x | x | x | ||
| Joao Da Rocha Franco | x | x | x | x | x | x | ||
| Maria Sanchez | x | x | x | x | x | x | ||
| Gregory Frey | x | x | x | x | x | x | ||
| Beau Toskich | x | x | x | x | x | x | ||
| Zlatko Devcic | x | x | x | x | x | x | ||
| Warner Oldenbug | x | x | x | x | x | x | ||
| Jessica Gomez | x | x | x | x | x | x | ||
| Justin Yarbrough | x | x | x | x | x | x | ||
| Michael Adalia | x | x | x | x | x | x | ||
| William Stone | x | x | x | x | x | x | ||
| Andrew Meltzer | x | x | x | x | x | x | ||
| Albert Hakaim | x | x | x | x | x | x |