
Abstract
Objective
Puig types 2 through 4 venous malformations (VMs) are challenging to treat with sclerotherapy given their robust systemic outflow. Endovenous balloon occlusion offers a means of temporarily occluding systemic venous outflow to allow for more complete sclerotherapy. This study reviews our experience of implementing this technique in patients with Puig advanced (types 2 through 4) VMs.
Methods
An IRB approved review of treated venous malformations from 2013–2016 revealed 10 patients fitting inclusion criteria. Patient demographics, pre-procedural imaging, intra-procedural technical parameters, and post-procedural follow-up outcomes were recorded. All patients underwent temporary balloon occlusion of a systemic or major draining vein during sclerotherapy. Embolic agents included n-butyl cyanoacrylate glue, sodium tetradecyl sulfate foam, and coils. Standard 5 French angioplasty balloons ranged from 4 to 8 mm diameter and 2 to 8 cm length depending on vessel requiring occlusion. All patients underwent minimum 3-year follow-up questionnaire administration re-assessing resolution of lesion symptomology and post-procedural quality of life (QoL) measures.
Results
Of the 10 VMs treated, 2 were Type 2, 6 were Type 3, and 2 were Type 4. More than one sclerotherapy session was required in 7/10 patients (mean: 2, range: 1–4). Most common sites of VM systemic drainage included subclavian, popliteal, internal/external jugular, and basilic veins. All patients had no indication for further sclerotherapy following adjunctive balloon occlusion. No non-target embolization or immediate post-procedural complications occurred. Follow-up questionnaires (mean interval: 3 years 6 months, range: 3 years–3 years 11 months) confirmed the persistence of embolization effects, improved QoL, and no additional sclerotherapy sessions for all patients in the cohort.
Conclusions
Endovenous balloon occlusion as an adjunct to sclerotherapy can be considered when treating patients with types 2–4 venous malformations. This technique lowers the risk of non-target systemic venous embolization, allowing for operator-driven deeper intralesional sclerosant penetration and subsequently maintained treatment efficacy.
Keywords
Introduction
In 1982, Mulliken and Glowacki published the landmark manuscript characterizing histologic differences between vascular neoplasia (such as hemangiomas) and errors in vasculogenesis (vascular malformations). 1 This soon became the basis of the International Society for Study of Vascular Anomalies (ISSVA). This classification schema divides vascular anomalies first into two major categories: vascular tumors and vascular malformations. Vascular tumors are divided into benign, locally aggressive or borderline, or malignant. Benign vascular tumors include lesions such as infantile hemangiomas, congenital hemangiomas, and pyogenic granulomas. Locally aggressive or borderline tumors include various hemangioendotheliomas (such as kaposiform, retiform pseudomyogenic, composite) as well as Kaposi sarcoma and Dabska tumors. The two main types of malignant vascular tumors are angiosarcomas and epithelioid hemangioendotheliomas. Vascular malformations are subclassified simple (a lesion with only one type of vascular malformation), combined (a lesion with two or more vascular malformations), originating from major named vessels, or associated with other anomalies. Simple malformations are subdivided into capillary lesions (such as nevus simplex and port-wine stains), lymphatic malformations (such as common cysts and generalized lymphatic anomaly), venous malformations (such as common venous malformations or glomuvenous malformations), and arteriovenous malformations and fistulas (such as sporadic or HHT-associated). Combined vascular malformations are any combination of capillary, venous, arteriovenous, and/or lymphatic formations. Malformations of major named vessels, also known as “channel type” or “truncal” vascular malformations, can be anomalies of various aspects of vessels such as their origin, course, length, or communications. Finally, malformations associated with other anomalies are those associated with clinical syndromes such as Klippel-Trenaunay and Sturge-Weber. 2
Puig et al. developed a classification schema dividing venous malformations on the basis of drainage. 3 Type 1 malformations are isolated without peripheral drainage, and can be sclerosed with essentially zero risk. Type 2 malformations drain into normal caliber veins. Type 3 malformations drain into dysplastic veins. Type 4 malformations represent total dysplasia with central drainage elements. 4 Types 2, 3, and 4 malformations are complex given their innate risk of sclerosant embolization into central venous drainage pathways (Figure 1). As such, achieving complete sclerosis in patients with higher-grade lesions is considered more challenging.
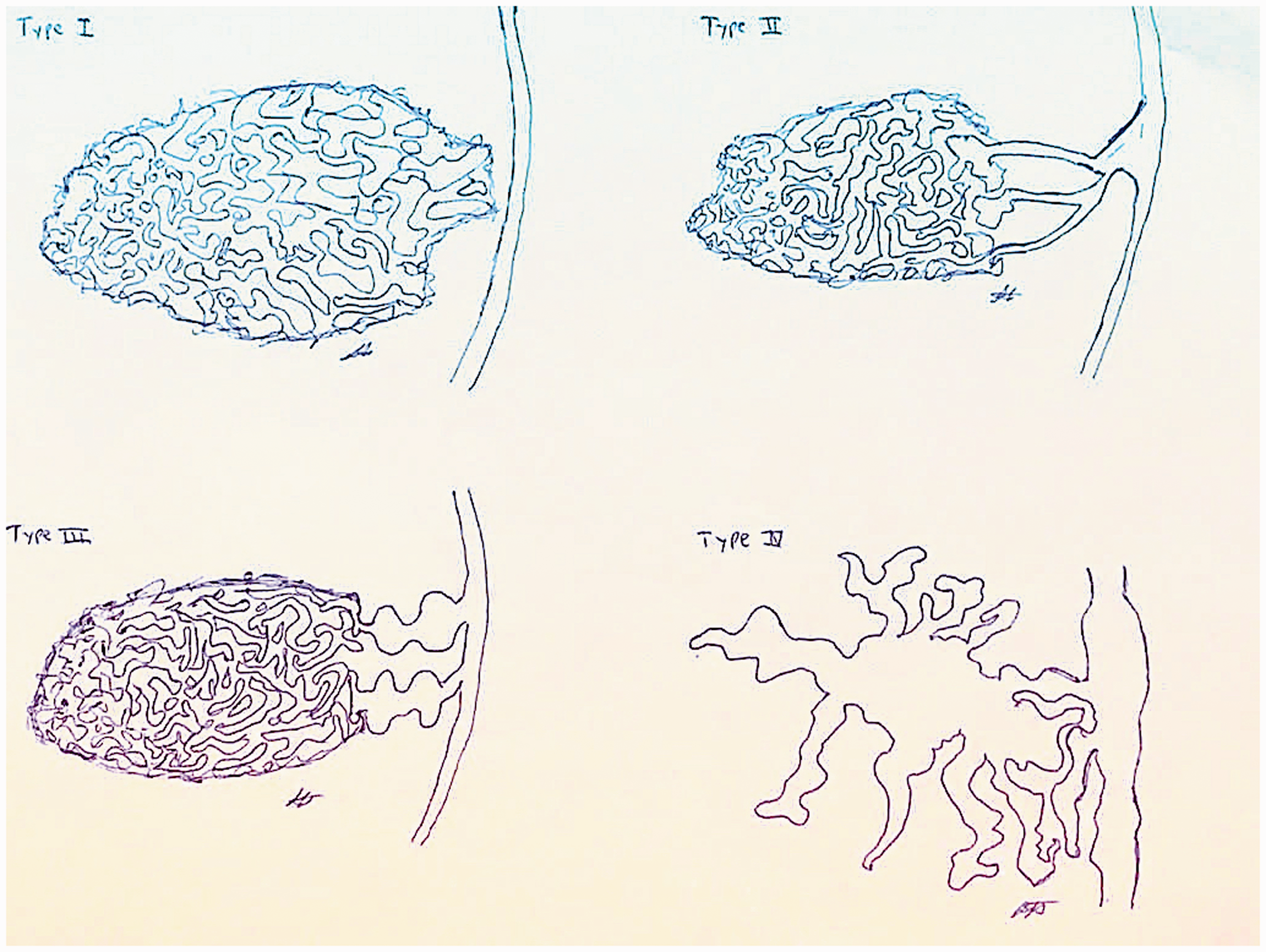
Artist renditions of Puig’s types 1 through 4 venous malformations. Type 1 malformations are isolated without peripheral drainage, and can be sclerosed with essentially zero risk. Type 2 malformations drain into normal caliber veins. Type 3 malformations drain into dysplastic veins. Type 4 malformations represent total dysplasia with central drainage elements.
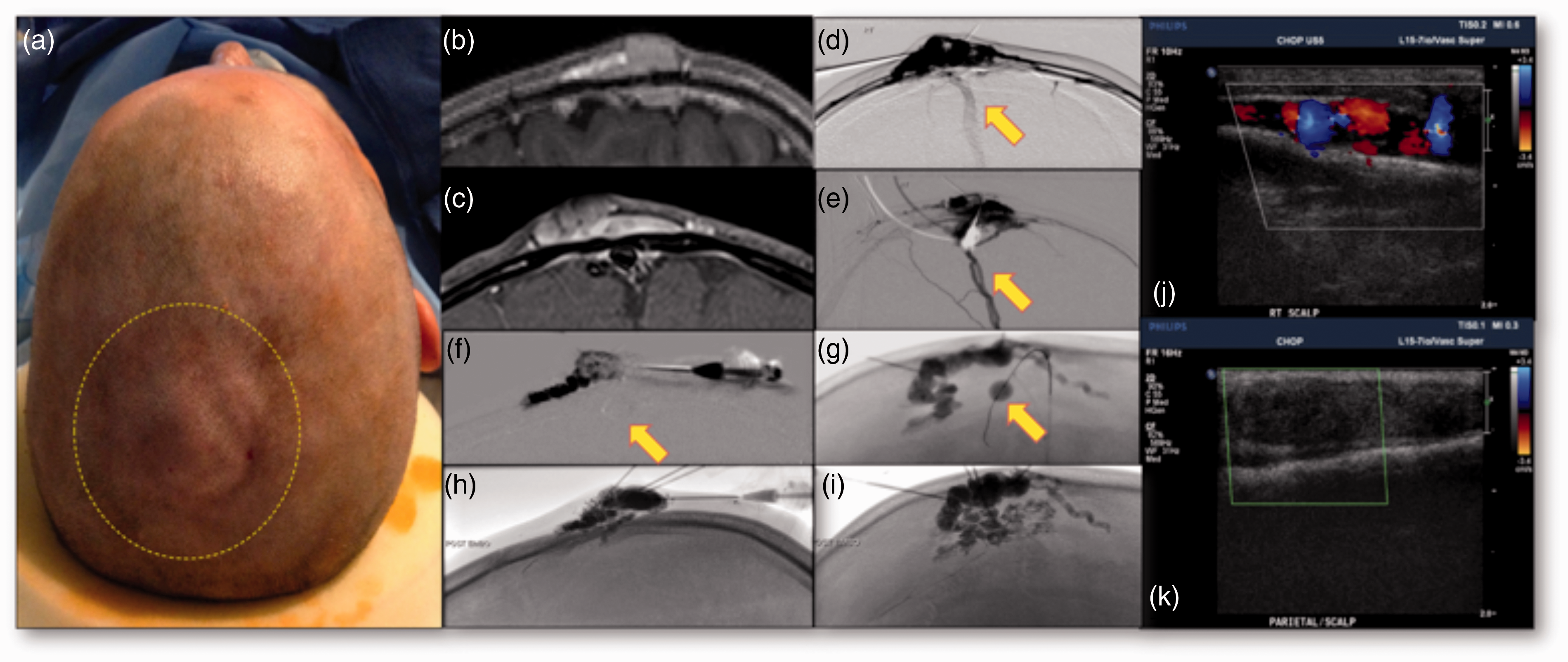
Cohort patient number 5. 8 year old male incidentally found to have focal scalp swelling during participation in contact sports. Fluctuant mass noted in the right parietal vertex scalp (Figure 2a), suspected to be a venous malformation on imaging (Figure 2b: sagittal post-contrast T1, Figure 2c: coronal post-contrast T1). During direct stick angiography of the malformation, opacification of the superior sagittal sinus (Figure 2d, yellow arrow) and its tributaries (Figure 2e, yellow arrow) were noted, consistent with a Puig type 2 malformation. Following deployment of a 7 mm x 7 cm balloon in the superior sagittal sinus at the point of malformation communication (Figure 2f and g, yellow arrows), the malformation was sclerosed to completion with 30% nBCA glue (Figure 2h and i). Comparison of color Doppler ultrasound images pre-procedure (Figure 2j) and 12 months post-procedure (Figure 2k) confirmed maintained embolization effects with lack of color Doppler flow in the malformation.
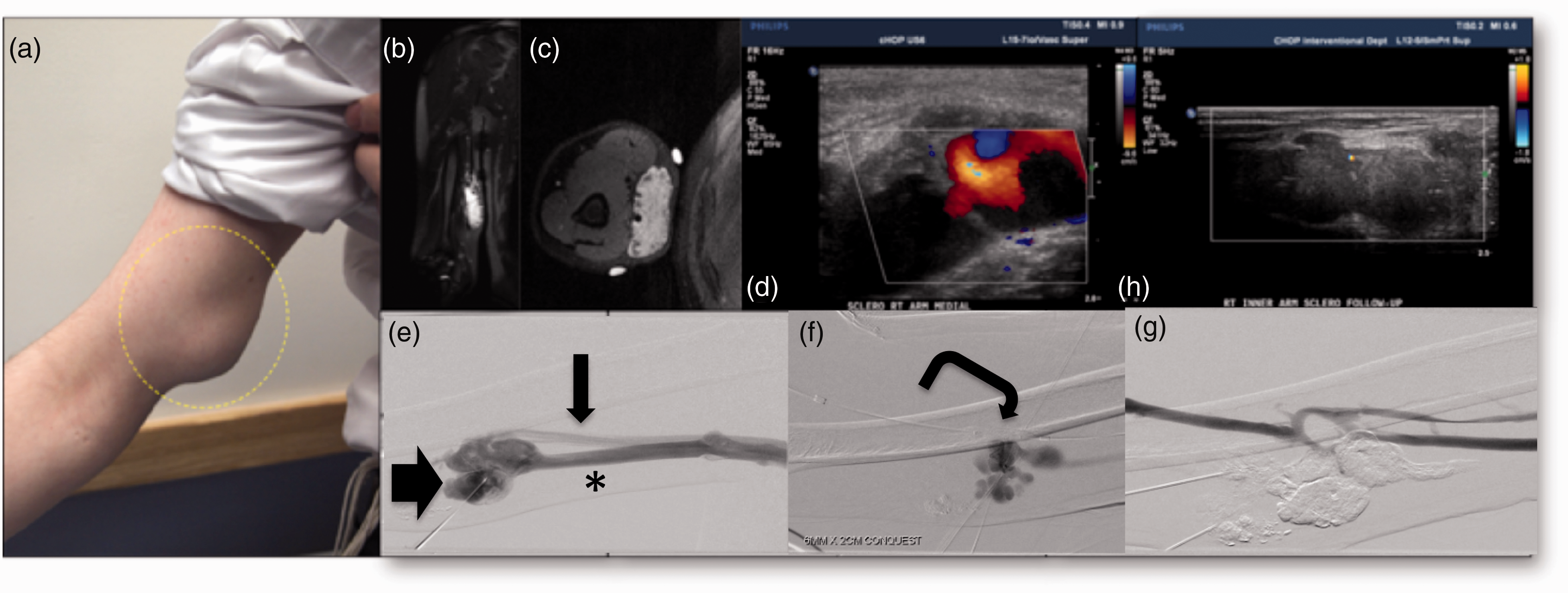
Cohort patient number 8. 17 year old male with right upper extremity heaviness and mild limitation in range of motion, found to have a fluctuant mass in the medial right upper extremity (Figure 3a). Soft tissue mass with ectatic vascularity and phleboliths was confirmed in the medial right upper extremity on MRI and ultrasound, demonstrating imaging features consistent with venous malformation. Figure 3b: coronal T2 STIR, Figure 3c: axial T2 STIR with overlying vitamin E markers, Figure 3d: color Doppler ultrasound confirming vascular non-pulsatile flow within the fluctuant mass. Direct-puncture angiography of the venous malformation confirmed a dysplastic draining vein (Figure 3e, asterisk) connecting the malformation (Figure 3e, short arrow) to the basilic vein (Figure 3e, long arrow), consistent with Puig type 3 malformation. Following balloon occlusion of the basilic vein with a 6 mm x 2 cm balloon (Figure 3f, curved arrow), direct puncture sclerotherapy was subsequently performed with nBCA glue. Post sclerotherapy angiography through basilic vein confirmed successful sclerotherapy, noting no opacification of the malformation or its draining vein (Figure 3g). One month follow-up confirmed maintained embolization with lack of color Doppler flow in the malformation (Figure 3h).
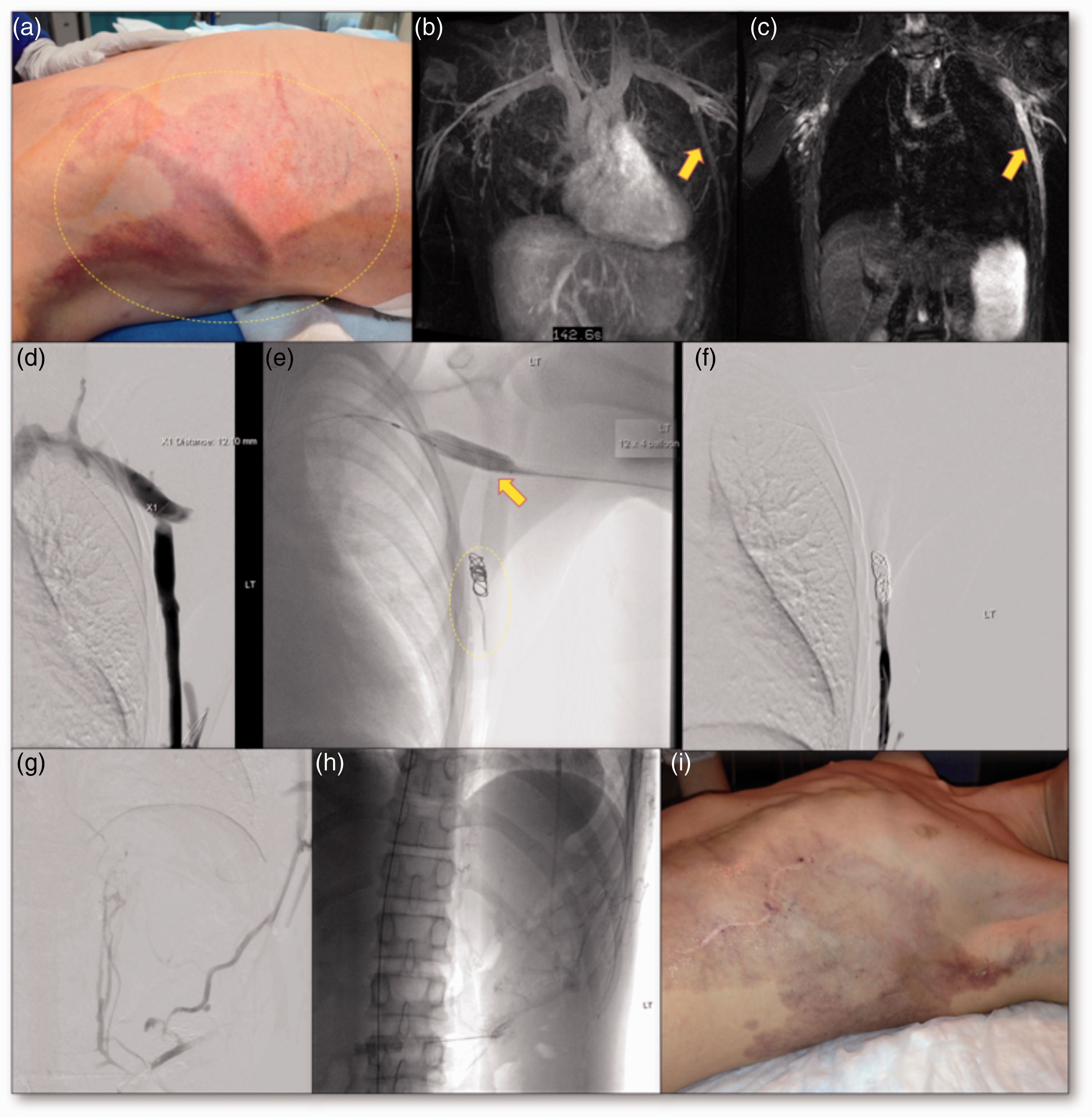
Cohort patient number 9. 14 year old male with Klippel Trenaunay syndrome and with broad left chest-abdominal wall draining vein associated with underlying Puig type 4 venous malformation contributing to discomfort and swelling (Figure 4a). MR venography confirmed connection of the prominent draining to the subclavian vein (yellow arrows in Figure 4(b): 3D reconstruction venographic image, and Figure 4(c): Coronal T1 post contrast single image). Venography of the draining vein and left subclavian vein allowed for appropriate measurement calculations (Figure 4d). As shown in Figure 4(e), a 12 mm x 4 cm balloon was inflated in the left subclavian vein (yellow arrow), allowing for safe coil embolization of the draining with 4 Nester metallic coils (two 14 cm x 10 mm coils and two 14 cm x 8 mm coils) without fear of systemic coil embolization (yellow dashed oval). Post coil embolization of draining vein angiography performed, confirming complete embolization of the draining vein with absence of left subclavian opacification (Figure 4f). Attention was then given to the malformation in the lower chest, for which embolization to stasis was performed with 3% STS (Figure 4g and h). At the time of four month clinical follow-up, patient had described resolution of previous symptomology, noting that previously seen prominent draining vein was no longer evident (Figure 4i).
Sclerotherapy is defined as the injection of an agent that acts as an irritant to the given vascular target’s lining walls. Foam sclerosants such as sodium tetradecyl sulfate (STS) have less of a chance for migration compared to ethanol given its expansile nature leading to increased surface tension and contact surface area with target vascular endothelium. 5 Embolotherapy is defined as use of coils, or liquid embolics - such as n-butyl cyanoacrylate (nBCA) and ethylene vinyl alcohol copolymer (Onyx) – to physically occlude a target vessel. 6 Combined utilization of sclerotherapy and embolotherapy techniques during treatment of peripheral vascular malformations has the potential to achieve zero occurrences of non-target embolization in experienced operators’ hands.7,8 Nevertheless, no sclerosing agent is immune to the potential risk of non-target embolization, especially in the setting of larger caliber draining veins. 9 Balloon occlusion offers a means of temporarily blocking these connections to the systemic circulation to allow for more complete sclerotherapy in addition to reducing the risk of non-target venous occlusion. This manuscript retrospectively reviews the procedural efficacy and outcomes of implementing this technique in a vascular anomaly patient population with primarily Types 2, 3, and 4 VMs.
Methods
Following institutional IRB approval, a retrospective review of patients who underwent venous malformation sclerotherapy utilizing balloon occlusion was performed. Parameters reviewed and collated included patient demographics, pre-procedural referral and imaging, intra-procedural technical parameters, post-procedural follow-up outcomes, and complications.
All patients identified underwent temporary balloon occlusion of a systemic or major draining vein during percutaneous sclerotherapy. All procedures were performed under general anesthesia. General anesthesia was utilized to minimize the risk of non-target embolization during sclerotherapy and adjunct embolotherapy of multiple access sites. Additionally, given the complexity of each patient’s respective venous malformation, absolute minimization of patient movement with general anesthesia allowed for precise balloon catheter navigation alongside coordinated inflation and deflation during times of sclerotherapy. The potential for confounding performance bias was limited through identification and incorporation of patients only treated with a balloon-occlusion technique by the same set of two interventionalists (or neurointerventionalists) respectively. Standard angioplasty balloons used ranged from 4 to 8 mm diameter and 2 to 8 cm length depending on vessel requiring occlusion (Conquest® Balloon Catheters, BD Bard, Arizona, USA). All instances of balloon occlusion were performed with inflation devices for gentle insufflation and below burst pressure to avoid venous angioplasty. Once the balloon was noted to accommodate the diameter of the vein using road mapping imaging, insufflation was ceased. Successful occlusion was confirmed in each case with dedicated fluoroscopic contrast injection of the lesion.
Agents used included, n-butyl-cyanoacrylate (TRUFILL® nBCA, Codman & Shurtleff Inc., Massachusetts, USA) mixed with ethiodol for a 30% concentration and 3% STS (SOTRADECOL®, Mylan®, Nevada, USA) mixed with lipiodol and air as per the Tessari method to create a foam. 10 Coiling or nBCA glue embolotherapy was performed for occlusion of the outflow vein. STS foam was utilized for primary sclerosis of the malformation. The lesions were injected using subtraction roadmapping visualizing the sclerotherapy agent reaching the outflow veins but not extending systemically, the goal being to treat the outflow veins and lesion. Where possible 30% concentration nBCA was injected close to the origin of the outflow vein with the remainder of the lesion treated with STS foam. Systemic heparanization was routinely performed with a 50–75 units per kilogram protocol, modified depending on patient’s body habitus, additional comorbidities and medication history. If the patient was already on low molecular weight heparin for localized intravascular coagulopathy, this was not stopped pre procedure.
Charts highlighting patient demographics, venous malformation at time of imaging diagnosis and procedure, number of sclerotherapy sessions, sites treated, and numbers of sites treated with balloon adjunctive sclerosis were created. Data collection was performed under an institutional IRB approved protocol. All patients underwent outpatient follow-up after their final sclerotherapy intervention. Dedicated post-procedural questionnaires were created and administered to all patients during their short-term follow-up appointments and at a minimum of 3 years following last intervention (Supplementary Figure).
Results
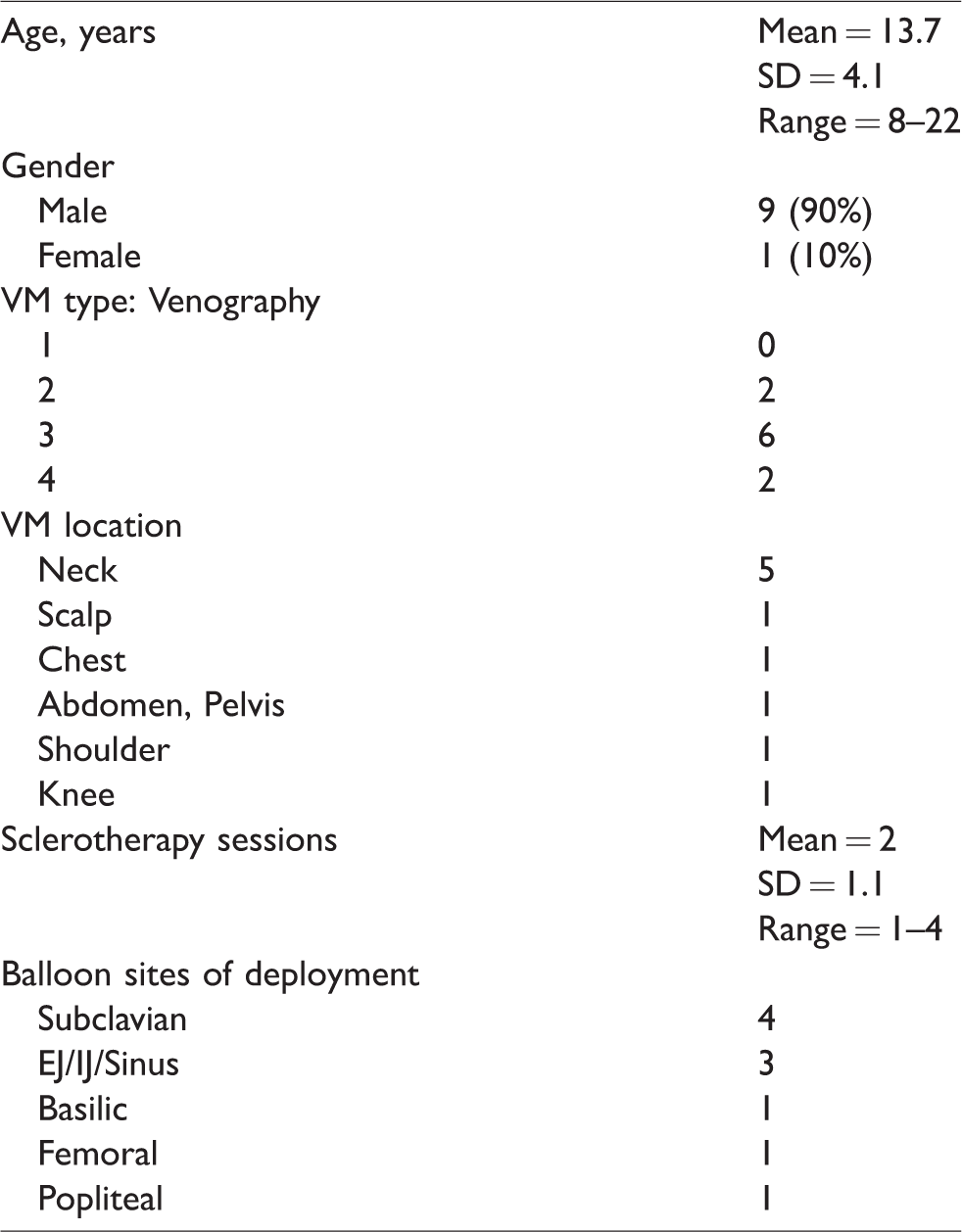
Demographics of the venous malformations’ cohort are summarized in Table 1. Ten patients were identified, consisting of 9 males and 1 female. Mean patient age was 13.7 years, noting a standard deviation of 4.1 years and range of 8–22 years.
Cohort demographics.
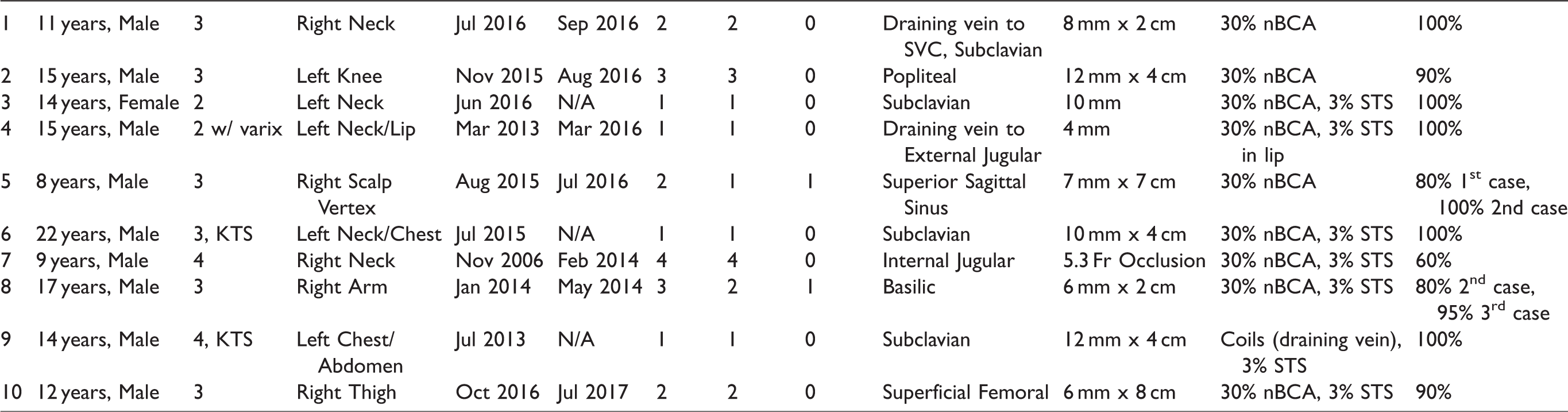
The majority of treated venous malformations with adjunct balloon occlusion were type 3, with an otherwise equal distribution of type 2 and type 4 venous malformations. Case specifics – including malformation type at time of imaging and intra-procedure, total number of sessions, sites treated with assistance of balloon occlusion, and specific sclerotherapy agent are summarized in Table 2. The cohort consisted of 6 patients with type 3 VMs, 2 patients with type 2 VMs, and 2 patients with type 4 malformations.
Session and occlusion Conquest® balloon parameters.
More than one sclerotherapy session was required in 7 of 10 patients, as the number of sclerotherapy sessions depended on lesion extent and presence and size of draining veins. Clinical and imaging follow-up was obtained in all patients, noting a mean imaging follow up of 16.4 months (range 1–62 months) and mean clinical follow up of 44.5 months (range 39–62 months). Majority of endovenous balloons were deployed in the subclavian vein (40%) and jugular venous systems (30%). Remaining 30% were evenly distributed across femoral, popliteal, and basilic veins. Representative case presentations of a type 2, a type 3, and a type 4 malformation are depicted in Figures 2 to 4, respectively.
One immediate post-procedural complication was noted in patient #10, within whom popliteal and superficial femoral vein deep vein thrombosis was identified during the patient’s overnight hospital admission, warranting subsequent mechanical thrombectomy with aspiration (Penumbra Inc, Almeda, CA, USA) and short-term therapeutic anticoagulation. This presumably occurred due to a combination of prolonged balloon inflation, subtherapeutic heparanization, and potential nontarget STS egress into the outflow vein. No additional complications (short-term or long-term) were noted in any of the other patients.
Following the session at which endovenous balloon occlusion was used in adjunct with sclerotherapy, this was the definitive therapy with no further sclerotherapy sessions needed in 8 of the 10. For two patients (patient numbers 5 and 8), the balloon occlusion intervention was the penultimate session in their respective managements. Two patients with type 4 lesions continued concomitant management with oral Rapamycin. Two patients with type 2 lesions in the knee and neck respectively electively chose to undergo cosmetic debulking of asymptomatic residual tissue. All patients had symptom relief at the minimum 3 years following completion of staged sclerotherapy sessions, as noted in Table 3.
Post-procedural follow-up.
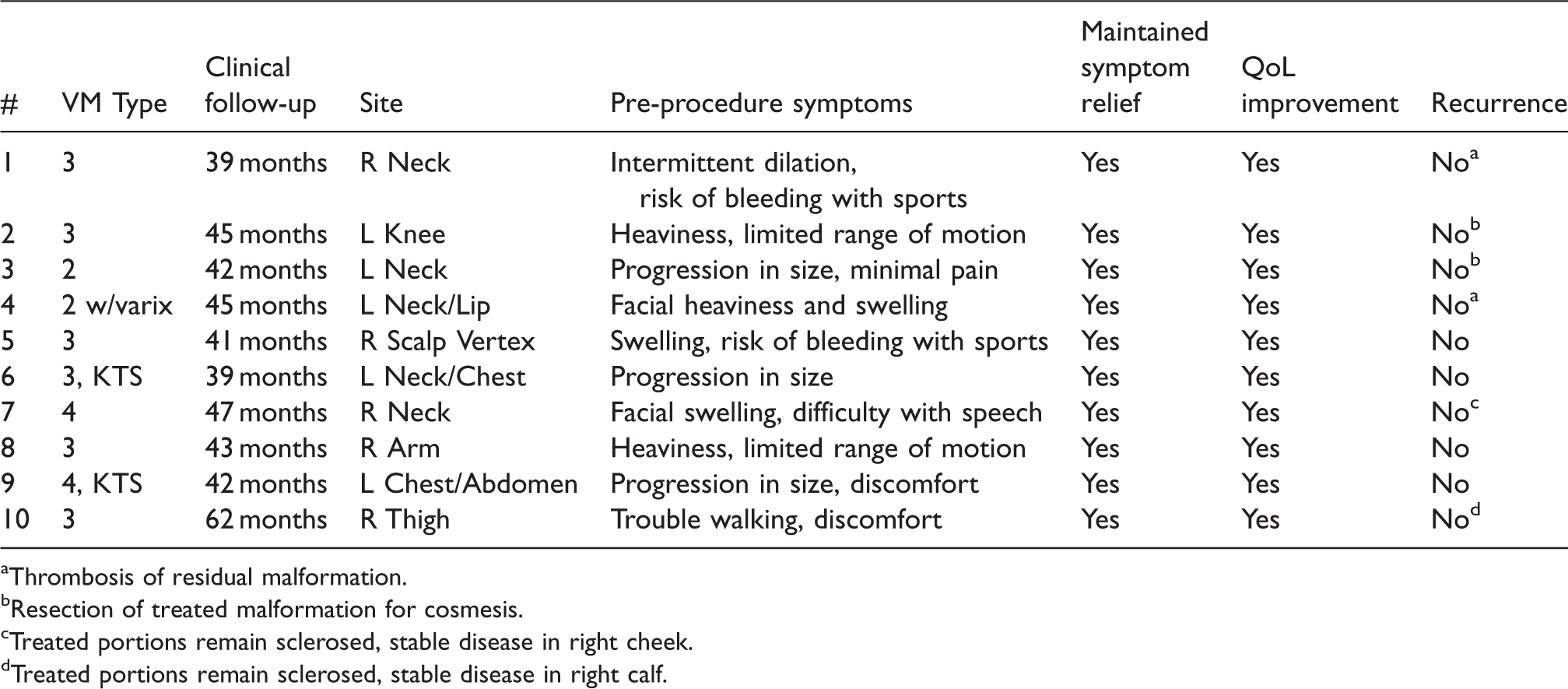
aThrombosis of residual malformation.
bResection of treated malformation for cosmesis.
cTreated portions remain sclerosed, stable disease in right cheek.
dTreated portions remain sclerosed, stable disease in right calf.
Discussion
Venous malformations remain the most common type of vascular malformation, affecting approximately 1%–4% of the population. 11 While these are present since birth, their penetrance and age of presentation are dependent on physiologic (such as hormonal alterations in puberty) and environmental (such as infection) factors. Symptoms are highly variable, ranging from discomfort to pain thought to derive from their tendency to thrombose and form phleboliths in the setting of inflammation and vascular stasis. 12 Percutaneous sclerotherapy provides a minimally invasive means of reducing lesion volume and improving associated symptoms. 11 Multiple sessions are often necessary due to lesion size, location, and presence or absence of systemic drainage. 13
Puig et al. developed a classification schema dividing VMs on the basis of drainage. 3 Type 1 malformations are isolated and without peripheral drainage. Type 2 malformations drain into normal veins. Sclerotherapy of type 1 and 2 malformations yield high rates of cure and satisfactory results, noting 92-94% complication-free predictive values following successful staged sclerotherapy sessions.14–16 However, as type 3 malformations drain into ectatic dysplastic veins and type 4 malformations include regions of generalized venous ectasia, sclerotherapy of these malformation types are known to result in higher risk of complications and achieve only 50–60% exclusion from systemic venous outflow rates despite staged sclerotherapy sessions.14–16 A primary reason for such low exclusion from systemic venous outflow rates of type 3 and 4 malformations stems from these malformations possessing draining veins of larger caliber that allow sclerosants to embolize into the central venous system, thereby limiting an operator’s ability to safely achieve complete sclerosis of such lesions. 17 Li et al recently reported a 70% efficacy following combined ethanol and n-butyl cyanoacrylate sclerotherapy of their cohorts’ Puig type VMs, higher than 55% curative rates previously reported in the literature. 18
The aim of sclerotherapy is to induce mural irritation of its respective target with subsequent sclerosis, collapse, and eventual pruning of the malformation. In contrast, as embolotherapy results in primary mechanical occlusion while otherwise maintaining the structural integrity of its target, its minimal utilization is preferred to avoid creation of large areas of firm or potentially palpable lumps in the respective regions of the given malformation. Given that a major risk of sclerotherapy for vascular malformations is nontarget distal embolization of the sclerosant, it is essential to use techniques that achieve successful stasis of efflux.
One of the most widely used temporary efflux restriction techniques is simply manual compression. This can be accomplished via an inflatable cuff, tourniquet, or physical clamping or gauze application. The major advantage of this method is its simplicity and ease of implementation. It also allows for more rapid adjustments of pressure regionally, facilitating for real-time focal control. 14 However, manual compression only works so long as the target venous structure is accessible superficially. This is not feasible for deeper malformations, such as those located in the head and neck, deep compartments of the upper and lower extremities, and deep spaces of the chest, abdomen, and pelvis. 19 Moreover, if one too tightly and acutely compresses a vein during sclerotherapy administration, there is a risk of embolization and/or reflux of the sclerosant into regional arteriolar beds. This can lead to eventual tissue and nerve injury. 15
Aside from nBCA glue, a commonly employed outflow occlusion technique is coiling. Although the concept and implementation is very similar at a broad level to balloon occlusion, there are key distinctions. Foremost, the coil is a permanent measure. This inherently increases the risk for complications such as infection, bleeding, and thrombosis. Moreover, coil placement necessitates precise and correct sizing due to the inherently compliant nature of venous structures. In pediatric patients especially, continued growth of venous diameter as these patients age increases the risk of coil migration and eventual dislodgement. Dislodgment can lead to complications such as deep vein thrombosis and pulmonary embolism. Venous size is also very easily influenced by factors such as position, spasm, metabolic demand, and the surrounding muscular environment. These constantly and rapidly changing conditions further increase the risk for dislodgement and embolization. Another consideration is that coils must be deployed within the vein centrally so as to not interfere with normal inflow veins and create significant stasis and eventual thrombosis. 19
Such permanent occlusions are in contrast to the benefits provided by the balloon occlusion technique, noting that its efficacy in embolization of head and neck vascular anomalies are well documented in the neurointerventional literature. 3 The extrapolation of such techniques outside head and neck vasculature is either not routinely performed or not well reported in the literature. This to our knowledge is the first reported series demonstrating successful implementation of adjunct venous balloon occlusion technique in conjunction with sclerotherapy. Temporary occlusion of major venous channels allowed for complete to near-complete sclerotherapy of the malformation with greater penetration and persistence of the sclerotherapy agent in the lesion. Systemic risks such as pulmonary artery embolization or systemic arterial embolization in the setting of right to left heart shunting are also reduced.
Eight of the 10 reviewed patients required no further sclerotherapy sessions following use of balloon occlusion. Balloon size selection was based on angiographic appearance of the dominant draining vein and/or native venous outflow path. In the two patients for whom an additional session was needed (patient 5 and patient 8), the post-balloon occlusion session was performed for sclerosis of minimal residual malformation contributing to pain and achiness in their respective malformation locations, noting that the majority of their respective malformations were embolized at the time of balloon utilization. In 8 of the 10 cases, the balloon was situated in the anatomic venous outflow path (such as popliteal vein, subclavian vein, etc), the balloon length being determined by the luminal insertions of the draining veins. Balloon size was calculated according to angiographic diameter of the vessel within which it was to be inflated. Patient number’s 1 and 4 cases were unique in that balloons were situated within the pathologic draining vein themselves rather than within the outflow native vein. Specifically, caution was taken to avoid temporarily occluding the superior vena cava and external jugular vein in these cases respectively.
Venous malformations typically possess activating mutations in two angiogenesis proliferating genes: tyrosine kinase (TIE2) and phosphatidylinositol 3-kinase (PIK3). Rapamycin has been effective in decreasing pain and improving functional limitations in patients with venous malformations. Such improvement in quality-of-life metrics is achieved, as rapamycin is an inhibitor of the eponymously named P13K-mechanistic target of rapamycin (mTOR) axis that mediates aberrant proliferation of venous malformations. 20 This leads to the authors’ special mention of patient number 7 with a broad right neck Puig type 4 venous malformation. While this patient underwent four sclerotherapy sessions beginning 6 years prior, in combination with rapamycin therapy, each session only achieved 5–10% total malformation sclerosis given the need to cease further embolization due to brisk systemic venous drainage from the malformation into the ipsilateral internal jugular vein. It was only following the fourth session utilizing balloon occlusion that up to 60% of the extensive submandibular malformation's total volume could be embolized in one session.
Although a curative efficacy of 93.5% averaged across our cohort’s Puig type VMs is greater than the 70% reported in recent literature, our small cohort is insufficient to establish true statistical significance correlating the ability of balloon implementation in achieving more total sclerosis in type 2 to 4 VMs. 18 Nevertheless, such a trend towards reducing the total number of sclerotherapy sessions due to more complete outflow vein occlusion via balloon inflation should not be overlooked.
Lastly, patient symptomology should be taken into account prior to treatment consideration. In a retrospective review of 410 patients with Klippel-Trenanay syndrome, 63% of the cohort reported quality of life afflicting pain levels. Debilitating psychosocial stigmata associated with venous malformations were equally emphasized, noting a statistically significant correlation between venous malformation presence and depression, anxiety, and similar psychiatric conditions.21–23 As summarized in Table 3, all cohort patients demonstrated maintained symptom improvement alongside satisfactory curative results following completion of sclerotherapy sessions at their 3-year follow-up.
Conclusion
Balloon occlusion of systemic or outflow venous drainage pathways in type 2–4 venous malformations provides an effective temporary means of increasing the penetrance of the sclerotherapy agent in a given lesion. The combination with STS and glue sclerotherapy can provide a means of both mechanically treating the outflow veins and the lesion simultaneously. The incorporation of this adjunctive technique, in our experience, allowed for more complete embolization and was the definitive technique within our follow up period of a minimum of 3 years and maximum up to 5 years post procedure.
Supplemental Material
sj-pdf-1-phl-10.1177_02683555211015565 - Supplemental material for Balloon occlusion as an adjunctive technique during sclerotherapy of Puig's classified advanced venous malformations
Supplemental material, sj-pdf-1-phl-10.1177_02683555211015565 for Balloon occlusion as an adjunctive technique during sclerotherapy of Puig's classified advanced venous malformations by Sri Hari Sundararajan, Srirajkumar Ranganathan, Sphoorti Shellikeri, Abhay Srinivasan, David W Low, Bryan Pukenas, Robert Hurst and Anne Marie Cahill in Phlebology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent
This single center retrospective study was approved by our IRB, and informed written consent was obtained at the time of initial procedural consent.
Guarantor
Not applicable.
Contributorship
Sri Hari Sundararajan is the primary author who analyzed and interpreted data from the study and was a major contributor in writing and editing the manuscript. Srirajkumar Ranganathan hand-drew Figure 1 of the manuscript, analyzed and interpreted data from the study, and was a major contributor in writing and editing the manuscript. Sphoorti Shellikeri performed the initial search and collection of the study's primary data, analyzed and interpreted data from the study, and was a major contributor in writing and editing the manuscript. Abhay Srinivasan performed Pediatric Interventional Radiology clinical duties for the manuscripts' patient cohort and was a contributor in editing the manuscript. David Low performed Plastic Surgery clinical duties for the manuscripts' patient cohort and was a contributor in editing the manuscript. Bryan Pukenas performed Interventional Neuroradiology clinical duties for the manuscripts' patient cohort and was a contributor in editing the manuscript. Robert Hurst performed Interventional Neuroradiology clinical duties for the manuscripts' patient cohort and was a contributor in editing the manuscript. Anne Marie Cahill is the principal investigator of the study who performed Pediatric Interventional Radiology clinical duties for the manuscripts' patient cohort, analyzed and interpreted data from the study, and was a major contributor in writing and editing the manuscript.
Consent for publication
Consent for publication was obtained at the time of initial procedural content.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.