
Abstract
Objective
To assess the efficacy and safety of once-daily 10 mg rivaroxaban for venous thromboembolism prophylaxis after ClosureFast radiofrequency ablation (RFA) of saphenous veins.
Method
The medical records of patients, who had a Caprini score of ≥3, underwent RFA, received prophylactic rivaroxaban for five days, and completed follow up at one month were reviewed for efficacy (a combination of endovenous heat-induced thrombosis [EHIT] grade of 2–4, any symptomatic or asymptomatic deep vein thrombosis [DVT], and symptomatic pulmonary embolism [PE]) and safety (a combination of major and clinically relevant non-major [CRNM] bleeding) outcomes.
Results
The results of RFA for 248 great saphenous and 24 small saphenous veins with the concomitant miniphlebectomy (63.8%) and sclerotherapy (16.5%) were analyzed. The primary efficacy outcome occurred in 5 of 218 (2.3%; 95%CI, 1.0–5.3%) patients: three EHITs and two symptomatic DVTs. The CRNM bleeding was reported in two patients (0.9%; 95% CI, 0.2–3.3%). No difference was observed in comparison with 79 similar patients who received 40 mg of subcutaneous enoxaparin during the same time period.
Conclusion
Once-daily 10 mg rivaroxaban is suitable for VTE prophylaxis after RFA of saphenous veins.
Introduction
Radiofrequency ablation (RFA) is a well-established method for thermal obliteration of refluxing saphenous veins with technical and clinical outcomes comparable with open surgery and laser treatmnet. 1 The incidence of major complications after RFA, particularly venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is low and does not exceed one percent. 2 Someone can place a high value for endovenous heat-induced thrombosis (EHIT) of types 2–4, which represents a thrombus propagation from the superficial venous system into the deep veins proximally to a site of recent obliteration. It takes most of VTE events after thermal ablation and accounts for about 1.4%. 3 The clinical significance of the EHIT is debatable, and the current European and recent American guidelines do not support the routine pharmacological prophylaxis to avoid it.1,2,4 However, in the absence of clear consensus, some local and National guidelines suggest prophylactic anticoagulation for patients undergoing venous surgery.
In Russia between 2015 and 2018, the National clinical recommendations for VTE prevention and treatment, which were complimentary with ACCP guidelines of 2012, 5 suggested pharmacological prophylaxis for all patients at intermediate to high risk for VTE. The individual risk could be assessed by the Caprini score (a version of 2005). 6 Considering that the Caprini model was not validated for venous surgery, the indications for prophylactic anticoagulation were extrapolated from the general surgical population: the individuals with three to four scores (intermediate risk) and ≥5 scores (high risk) had to receive it. Taking into account that all relevant patients have varicose veins and minor surgery (1 + 1 scores) they quickly can get one additional score (age over 40, edema, or another risk factor) and be stratified into the group of intermediate risk for VTE. So clinical centers following these guidelines were obliged to prescribe pharmacological prophylaxis for most patients after venous surgery. In 2018 the new National clinical recommendations on diagnostic and treatment of chronic venous disease were published, removing the necessity of routine use of anticoagulants after venous surgery.
Low-molecular-weight heparins (LMWH) are preferable for VTE prophylaxis in non-orthopedic surgery. 5 However, subcutaneous injections are not comfortable for patients after venous interventions in outpatient settings or single-day surgical facilities. Direct oral anticoagulants (DOACs) appeared to be an attractive option after their introduction. Their efficacy and safety were assessed after total hip and knee arthroplasty. 7 Unlike the other DOACs, the direct oral factor Xa inhibitor rivaroxaban showed superiority over enoxaparin after major and non-major orthopedic surgery.7,8 The once-daily 10 mg rivaroxaban became popular for VTE prevention after endovenous laser treatment, even in the absence of legal indications (off-label use).9–11 However, of our best knowledge, it has not been assessed after endovenous radiofrequency ablation.
The aim of this study was to report the efficacy and safety once-daily 10 mg rivaroxaban for venous thromboembolism prophylaxis after ClosureFast radiofrequency ablation of saphenous veins concomitant with miniphlebectomy, sclerotherapy or no treatment of varicose tributaries in patients formally having intermediate to high risk for VTE according to the Caprini score.
Methods
This study is a retrospective analysis of prospectively collected data obtained from medical records of patients treated for varicose veins using RFA at one clinical center (Hospital “Neftyanik” of Tyumen, Russian Federation). In 2012–2018, radiofrequency ablation was predominantly used for the treatment of refluxing great saphenous (GSV) and small saphenous (SSV) veins at the referred clinical center. Since 2018 the cyanoacrylate embolization by VenaSeal technology replaced the RFA. Between 2015 and 2018, patients were assessed by the Caprini score, and those at a score of ≥3 were prescribed with subcutaneous enoxaparin of 40 mg starting 12 h before, 12 h after the intervention, and then every 24 h for five days. For all patients with a personal history of VTE who had already finished anticoagulation prior to surgery, the duration of pharmacological prophylaxis was extended to 30 days. Those who had not finished anticoagulation to the moment of intervention were not included in the analysis.
Individuals, who rejected subcutaneous injections, were advised to use direct oral anticoagulant rivaroxaban. The reasons for LMWH refusal were: discomfort with subcutaneous injections, inability to perform them in outpatient facilities, and awareness of oral anticoagulants. Informed consent on off-label use was signed in advance. Rivaroxaban (Bayer AG, Leverkusen, Germany) of 10 mg was prescribed in the same manner as enoxaparin (12 h before, 12 h after the intervention, and then every 24 h) for five days.
Since 2018 the routine use of pharmacological prophylaxis after venous surgery was abandoned, so enoxaparin and rivaroxaban were prescribed only for individuals with a personal history of VTE or higher Caprini score (without an established threshold and on the personal decision of surgeon). The protocol for using anticoagulants did not change. The same approach was used for VenaSeal embolization that replaced RFA in 2018. The results of VTE prevention after cyanoacrylate embolization are out of the scope of this report and are being under investigation within the ongoing prospective registry study CAPSIVS. 12
The radiofrequency ablation with ClosureFast (Medtronic, San Jose, USA) was performed in patients with symptomatic chronic venous disease of C2–C5 clinical classes by CEAP classification (revision of 2004) 13 and with reflux on the GSV and/or SSV trunks of >0.5 s as detected by duplex ultrasound scan (DUS). 14 The technique of ClosureFast procedure was complimentary to well-known descriptions 15 with some deviations based on the surgeon’s personal experience. Briefly, the vein was assessed closely to the distal point of reflux (not lower mid-calf for SSV), the catheter tip (distal heating element of 7 cm in length) advanced towards the junction and placed at 2 cm below it. The tumescent anesthesia under ultrasound guidance was applied with modified Klein’s solution, 16 containing 1000 ml of normal saline, 20 ml of 2% lidocaine (400 mg), 1 ml of 0.1% epinephrine (1 mg), and 10 ml of 8.4% sodium bicarbonate (10 mEq). Three heating cycles were applied at the junction, either sapheno-femoral or sapheno-popliteal. The number of cycles at the lower levels was adjusted to the vessel diameter. For GSV of <8 mm one cycle was applied; for GSV of 8–12 mm – two cycles; for GSV >12 mm – three cycles at every segment. For SSV one, two or three cycles were used in the case of a vein diameter of <6 mm, 6–8 mm, and >8 mm, respectively. All sizes are related to the measuring in standing position. The truncal ablation could be supplemented by simultaneously miniphlebectomy or sclerotherapy. Miniphlebectomy was performed under tumescent anesthesia or enhanced by general anesthesia through a laryngeal mask. The last option was suggested in the case of excessive tributaries or anxious patients. Sclerotherapy was made with physician-compounded foam, based on the ambient air and polidocanol of 1–3% adjusted by the vein diameter. The proportion of air and liquid sclerosant was 4:1. The decision to treat varicose tributaries and treatment approach choice were based on the surgeon’s and patient’s preferences. In general, miniphlebectomy was preferred in the case of large tributaries or patients concerned more about a quick resolution of visible varicosity. Sclerotherapy was used for smaller veins in patients more concerned about aesthetic results. The tributaries were left for spontaneous regression in those concerned about venous insufficiency symptoms more than for visible varicosities or aesthetics and in cases of smallest varicosity.
Elastic compression with above-knee medical stocking (pressure at the ankle of 23–32 mm Hg) was applied just after the procedure, and the patient was ambulated in the absence of general anesthesia. He was advised walking for 30–40 min inside the surgical department. If tumescent anesthesia was enhanced by general anesthesia, the ambulation was delayed for 30–60 min. Referred stockings were recommended to use on an everyday basis during the first month after surgery.
According to the internal protocol, patients were followed at 1 and 7 days, 1, 3, and 12 months after RFA with clinical examination and DUS. The operating surgeon made a duplex ultrasound with Mindray M7 (Guangdong, China) scanner and linear transducer of 8–12 MHz (in Russia, only physicians are allowed to perform ultrasound investigation). DUS is routinely performed in a horizontal position to assess the compressibility of deep and superficial veins and in a vertical position to detect the superficial venous reflux. The standard report is being made under established rules 17 and documented in the medical record. It includes the patency (compressibility) of the deep veins at the calf and thigh level; the occlusion of the target superficial vein; the proximal level of occlusion in relation with neighbor deep vein or superficial tributary (epigastric vein); the presence of EHIT; the persistence of the residual superficial reflux. The EHIT was reported only in the case of grade 2 (thrombus propagation into deep veins with a cross-sectional area obstruction <50%), grade 3 (>50% cross-sectional area obstruction), or grade 4 (total occlusion of the deep vein). 3 In Russia, EHIT of grade 1 (thrombus propagation to the junction) does not interpret as a complication and is not being reported. The recanalization of the target vein was suggested in the case of its length >5 cm. The vein thrombosis was considered if any incompressibility of a deep vein or untreated superficial vein was detected and reported.
Follow-up medical records also contain standard medical information on complaints, objective status, and possible complications after treatment. They allowed identifying the efficacy and safety outcomes.
The investigators evaluated the medical records of eligible patients. The inclusion criteria for analysis were as follows: performed ClosureFast radiofrequency ablation of the GSV or SSV, Caprini score of ≥3, prescribed pharmacological prophylaxis with rivaroxaban due to rejection of subcutaneous injections. A group of similar patients who received prophylactic subcutaneous enoxaparin during the same time period was used for the comparison. The exclusion criteria were: therapeutic anticoagulation or dual antiplatelet therapy at the time of intervention (history of VTE, atrial fibrillation, percutaneous coronary intervention), lack of follow-up medical record in one month.
The primary efficacy endpoint of the study was designed as a combination of EHIT (grade of 2–4), any symptomatic or asymptomatic DVT, and symptomatic PE within the first month after the intervention. The EHIT should be detected by DUS and reported, as mentioned above. The symptomatic DVT suggested the presence of typical symptoms and signs (pain, swelling, cyanosis, prominent subcutaneous veins) as indicated in the medical record and should be confirmed by DUS. The asymptomatic DVT suggested a lesion of the deep vein without a direct connection with the obliterated vein as detected by DUS. The symptomatic PE indicated the presence of typical symptoms and signs (cough, shortness of breath, hemoptysis, chest pain, collapse) and confirmed by appropriate imaging. The secondary efficacy endpoints contained components of the primary one with the recanalization of the target vein at 1 and 12 months after the intervention.
The primary safety endpoint was designed as a combination of major and clinically relevant non-major (CRNM) bleeding within the first month after the intervention, as defined by the International Society of Thrombosis and Hemostasis. The definition of major bleeding included fatal bleeding, and/or symptomatic bleeding in the critical area (intracranial, intraspinal, intraocular, retroperitoneal, pericardial, in a non-operated joint, or intramuscular with compartment syndrome), and/or extrasurgical site bleeding causing a fall in hemoglobin level of ≥20 g/L or leading to transfusion of two or more units of whole blood or red cells, and/or surgical site bleeding that requires a second intervention of sufficient size to delay mobilization or wound healing, to prolong hospitalization or to result in deep wound infection, and/or surgical site bleeding that is unexpected and prolonged and/or sufficiently large to cause hemodynamic instability. 18 The CRNM bleeding should require medical intervention, and/or lead to hospitalization or increased level of care, and/or promote face-to-face evaluation. 19 The secondary safety endpoint contained components of the primary one and other adverse events (AEs) that were reported within the first month and could be related to rivaroxaban or enoxaparin. An adverse event was defined as any unfavorable and unintended sign (including an abnormal laboratory finding), symptom, or disease temporally associated with the use of rivaroxaban or enoxaparin, whether or not it was considered related to rivaroxaban or enoxaparin. The two experienced in vascular surgery investigators assessed the relationship of any reported AE to the administration of rivaroxaban or enoxaparin.
The demographic data, preoperative risk factors according to the Caprini score, vein characteristics, procedural data, including concomitant miniphlebectomy and sclerotherapy, and outcome data, including ultrasound findings and complications, were collected from the reliable medical records. The study follows the principles outlined in the Declaration of Helsinki. It did not require any additional informed consent due to retrospective character, as had been confirmed by the Institutional Review Board of the Pirogov Russian National Research Medical University.
Statistical analysis
The descriptive statistic was used for data analysis. The patient is the main analyzed unit unless otherwise stated. The absolute variables are expressed as mean with standard deviation and the relative variables as percents. The outcomes are reported in absolute and relative numbers, including a 95% confidence interval (CI), calculated by Wilson. The t-test for independent samples compared absolute variables, and two-tailed Fisher’s exact test or chi-squared test compared the relative values. Logistic regression was used to find significant predictors for specified outcomes. Propensity score matching was performed by sex, age, CEAP clinical class, side of the affected limb, target vein, Caprini score, type of intervention on tributaries, and type of anesthesia. A P-value of <0.05 was considered statistically significant. The analysis was performed using SPSS version 26 software package (IBM Corp, Armonk, NY). The power test was done by the online calculator Sealed Envelope (Sealed Envelope Ltd, London, UK). 20
Results
The data for the period of 2015–2020 were extracted in April 2020 and updated in October 2020. A total of 375 RFAs in 297 symptomatic patients were analyzed (Figure 1): 272 procedures in 218 subjects were carried out with the prescription of rivaroxaban, and 103 procedures in 79 subjects were performed with the use of enoxaparin for VTE prophylaxis. In total, 177 women and 120 men in the age of 21–73 years (mean age of 45.1 ± 11.7 years) were treated predominantly between 2015 and 2018. The distribution of the higher CEAP clinical class was as follows: C2 – 113 (38.0%), C3 – 119 (40.1%), C4 – 55 (18.5%), and C5 – 10 (3.4%). The left leg was treated in 108 (36.4%) patients, right leg – in 122 (41.1%), and simultaneous bilateral intervention was performed in 67 cases (22.5%). In total, 333 GSV trunks and 42 SSV trunks were obliterated. The maximal diameter of treated GSV ranged from 4.2 to 24.0 mm (mean of 9.2 ± 2.9 mm), and the SSV – from 3.7 to 13.0 mm (mean of 7.8 ± 2.3 mm). In 275 (92.6%) patients, the treatment was done under local anesthesia, and only 22 (7.4%) subjects required inhalational enhancement. Varicose tributaries were removed by miniphlebectomy in 161 (54.2%) patients, treated with foam-form sclerotherapy in 62 (20.9%) subjects, and were left for further spontaneous regression in the last 74 (24.9%) cases. The patients who received rivaroxaban, or enoxaparin were comparable according to the main demographical and clinical criteria (Table 1). However, in the enoxaparin group were observed more interventions on the SSV trunk and more varicose tributaries were left without treatment (39.2% vs. 19.7%, p = 0.001).
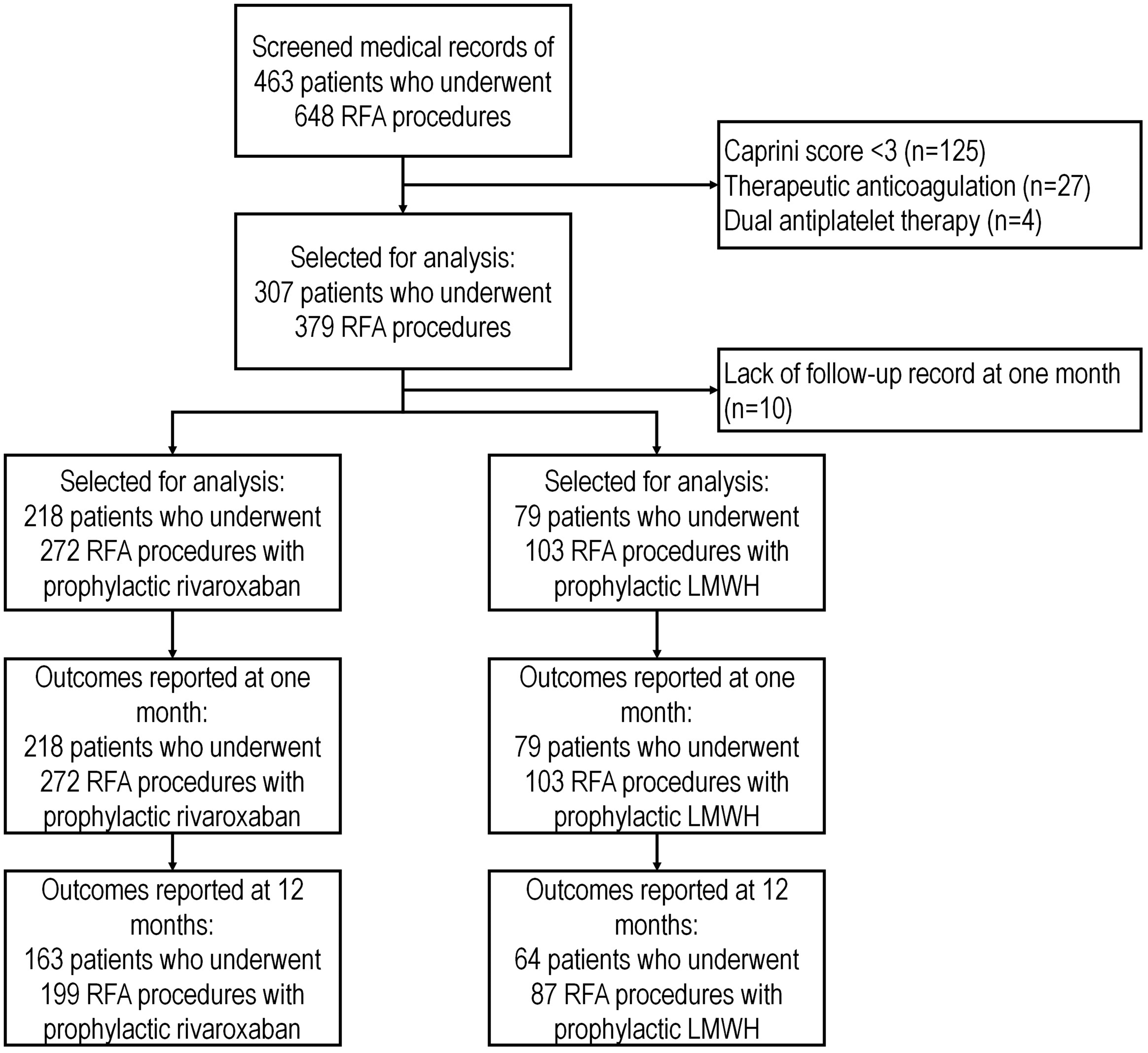
The study flowchart.
Demographical and clinical characteristics of treated patients who received either rivaroxaban or enoxaparin for VTE prophylaxis.
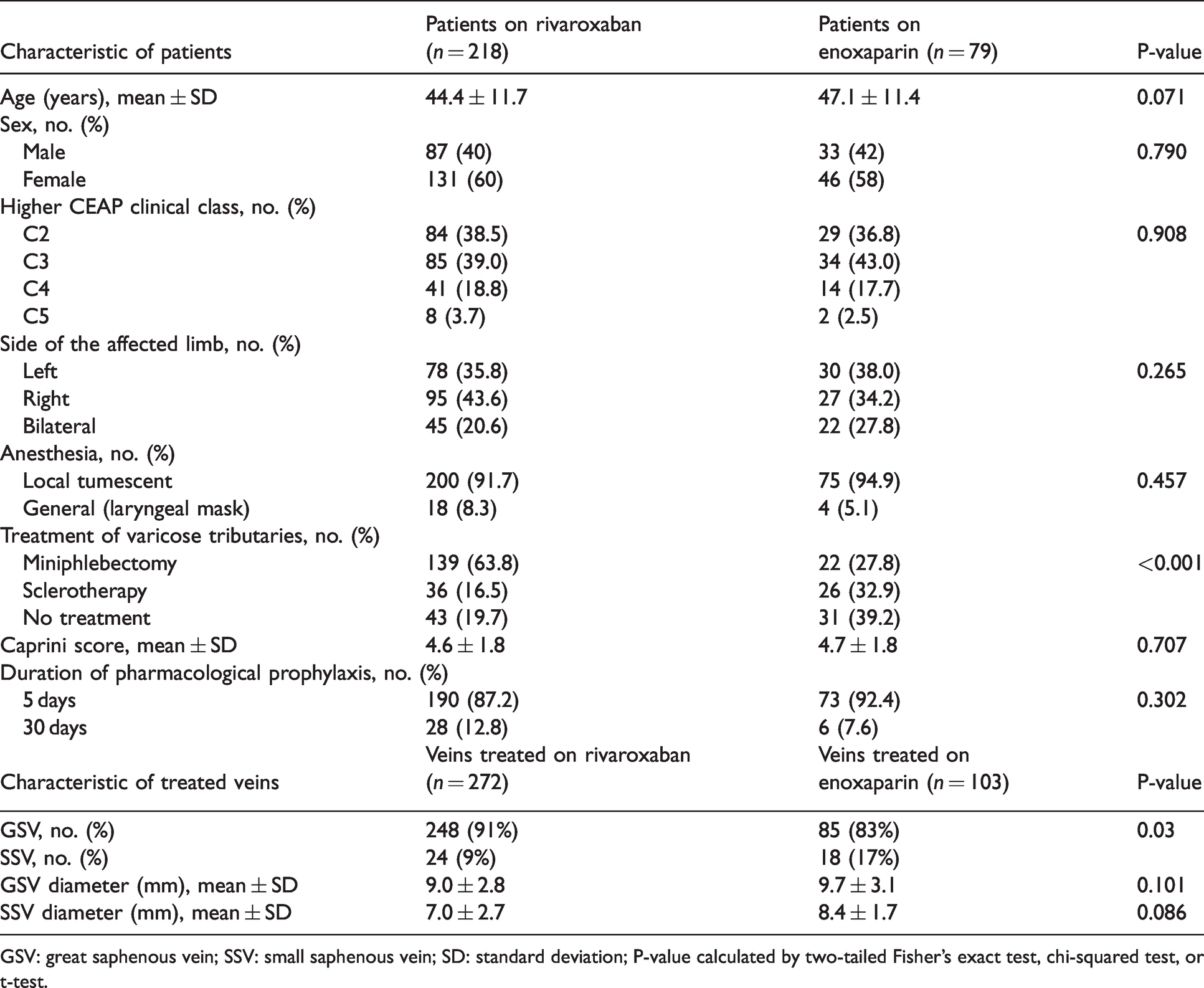
GSV: great saphenous vein; SSV: small saphenous vein; SD: standard deviation; P-value calculated by two-tailed Fisher’s exact test, chi-squared test, or t-test.
The Caprini score varied from 3 to 10, with a mean value of 4.6 ± 1.8. The distribution of individual risk factors for VTE is represented in Table 2. No significant difference was found between patients who received rivaroxaban or enoxaparin. The mean Caprini score in the rivaroxaban group was 4.6 ± 1.8 compared with 4.7 ± 1.8 in the enoxaparin group. In 53 patients who were treated after 2018 and received pharmacological prophylaxis, the Caprini score varied from 3 to 10, with a mean value of 7.0 ± 1.6. Prophylactic anticoagulation was limited to five days in 263 (88.6%) patients and prolonged for one month in 34 (11.4%) subjects with a personal history of VTE without any difference between groups (Table 1).
The distribution of individual risk factors for VTE according to the Caprini score (a version of 2005) 6 in patients who received either rivaroxaban or enoxaparin for VTE prevention.
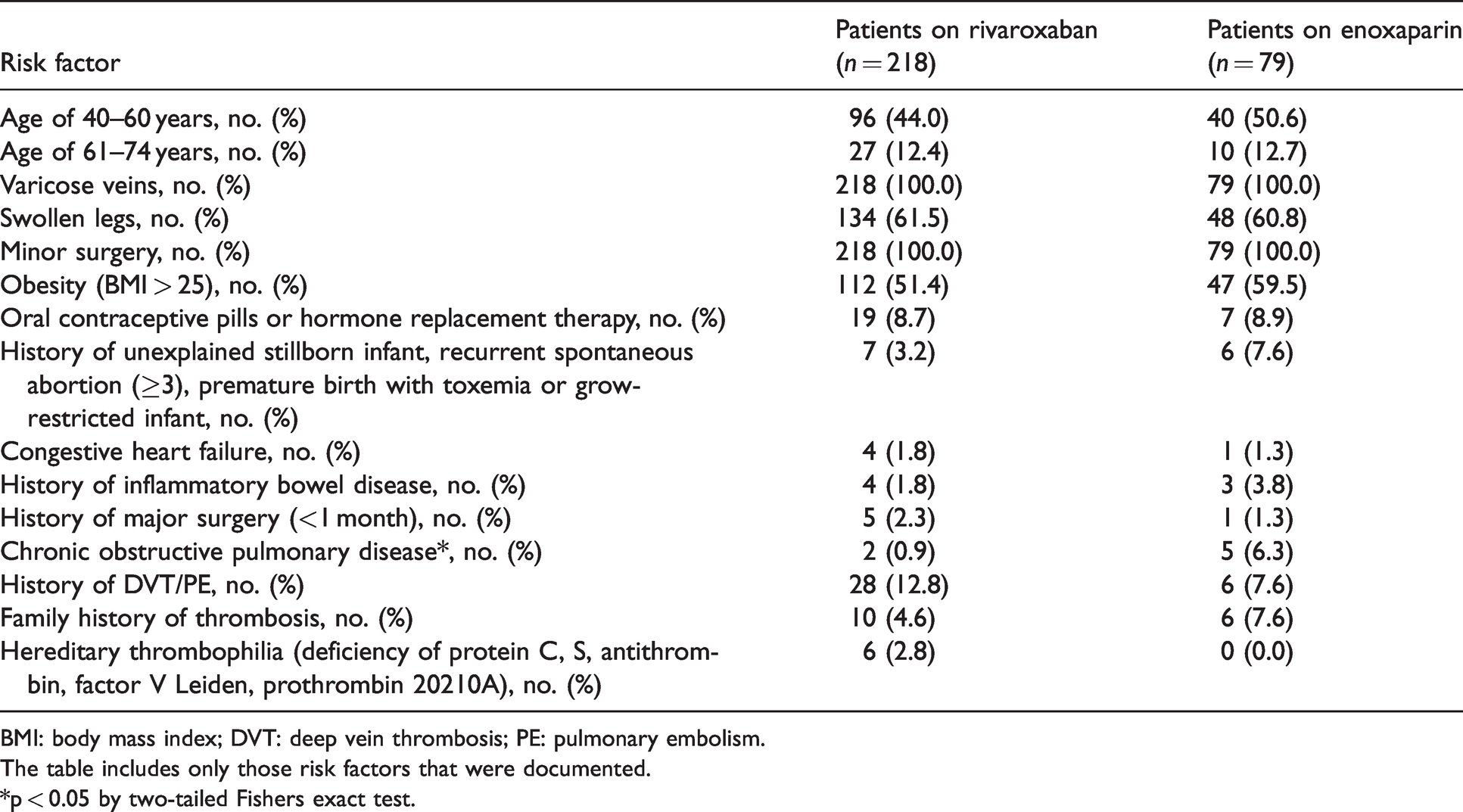
BMI: body mass index; DVT: deep vein thrombosis; PE: pulmonary embolism.
The table includes only those risk factors that were documented.
*p < 0.05 by two-tailed Fishers exact test.
The results of the observation are represented in Table 3. The primary efficacy endpoint in patients who received rivaroxaban was detected in 5 of 218 (2.3%; 95% CI, 1.0–5.3%) patients and contained of 3 (1.4%; 95% CI, 0.5–4.0%) EHITs and 2 (0.9%; 95% CI, 0.2–3.3%) DVTs. In the enoxaparin group, EHIT was observed in 2 of 79 patients (2.5%; 95% CI, 0.7–8.7%) without any DVT. No case of symptomatic PE was reported in both groups. No difference was found for the primary efficacy endpoint between patients received either rivaroxaban or enoxaparin (relative risk [RR], 0.91; 95% CI, 0.18–4.58).
Efficacy and safety outcomes in patients who received either rivaroxaban or enoxaparin for VTE prophylaxis.
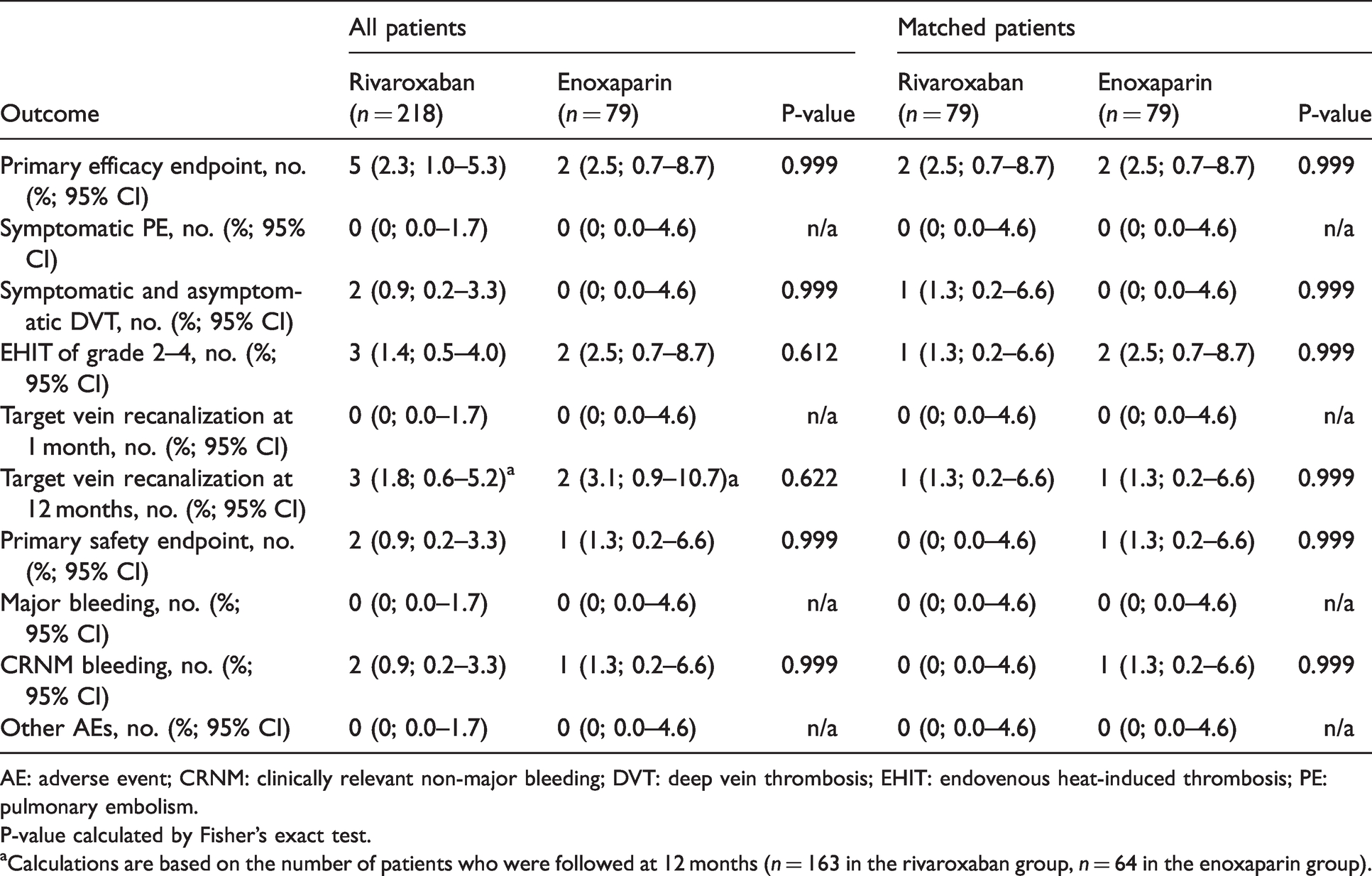
AE: adverse event; CRNM: clinically relevant non-major bleeding; DVT: deep vein thrombosis; EHIT: endovenous heat-induced thrombosis; PE: pulmonary embolism.
P-value calculated by Fisher’s exact test.
aCalculations are based on the number of patients who were followed at 12 months (n = 163 in the rivaroxaban group, n = 64 in the enoxaparin group).
All EHITs were classified as grade 2 as detected by DUS on the next day after GSV ablation. No new EHIT was observed at seven days or later after the intervention. In the rivaroxaban group, women of 3, 4, and 10 Caprini scores developed EHIT. One man plus one woman in the enoxaparin group, both of three Caprini scores, developed EHIT. In two cases (one in each group), RFA was accompanied by miniphlebectomy, and in the other three cases, no treatment for varicose tributaries was performed. The maximal diameter of GSV was 8.9, 9.5, and 9.7 mm in the rivaroxaban group, similar to 9.5 mm and 7.5 mm in the enoxaparin group. All patients were switched to rivaroxaban of 20 mg once daily for three weeks with full resorption of thrombotic masses in the common femoral vein.
Both deep vein thromboses in the rivaroxaban group were symptomatic and confirmed by DUS. The first one occurred in a male with the Caprini score of 7 at two weeks after GSV ablation with concomitant miniphlebectomy. At 10 days after the intervention and at five days after cessation of anticoagulation, he jumped with a parachute, broke the calcaneus, and was immobilized by plaster cast without further pharmacological prophylaxis for VTE. One week after that, he was diagnosed with popliteal DVT and received therapeutic doses of rivaroxaban for three months. The second DVT occurred in a female with the Caprini score of 6, who restarted her hormonal replacement therapy at two weeks after GSV ablation. One week after that, she was diagnosed with calf DVT and received therapeutic anticoagulation with rivaroxaban for three months. Thus, all reported DVTs were provoked and occurred after cessation of standard five-day VTE prophylaxis.
At one month of observation, the target vein recanalization was observed in none of 218 (0%; 95% CI, 0.0–1.7%) patients who received rivaroxaban and in none of 79 patients (0%; 95% CI, 0.0–4.6%) who received enoxaparin. At 12 months, 163 patients in the rivaroxaban group and 64 patients in the enoxaparin group were followed. Recanalization was detected in in 3 (1.8%; 95% CI, 0.6–5.2%) and 2 (3.1%; 95% CI 0.9–10.7%) cases, respectively without significant differences.
The primary safety endpoint was reported in 2 of 218 (0.9%; 95% CI, 0.2–3.3%) patients who received rivaroxaban compared to 1 of 79 (1.3%; 95% CI, 0.2–6.9%) persons who received enoxaparin without any differences (RR, 0.73; 95% CI, 0.07–7.88). All three cases were represented by a subcutaneous hematoma in the zone of miniphlebectomy, which required an additional draining and was classified as CRNM bleeding. No other AEs potentially attributed to rivaroxaban or enoxaparin were documented in the medical records.
The results obtained from the propensity score matched population (79 patients who received rivaroxaban and 79 patients who received enoxaparin) were similar to the total sample; they did not show any significant difference between the groups (Table 3).
Multiple factor logistic regression including age, sex, CEAP clinical class, side of the affected limb, treated vein, Caprini score, type of anesthesia, type of intervention on varicose tributaries, type of prophylactic anticoagulation, duration of prophylactic anticoagulation was performed for the primary efficacy endpoint. The results are represented in Table 4. Only age and Caprini score predicted the postoperative VTE.
The results of logistic regression analysis for the predictors of postoperative VTE (a combination of EHIT grade of 2–4, symptomatic and asymptomatic DVT, symptomatic PE).
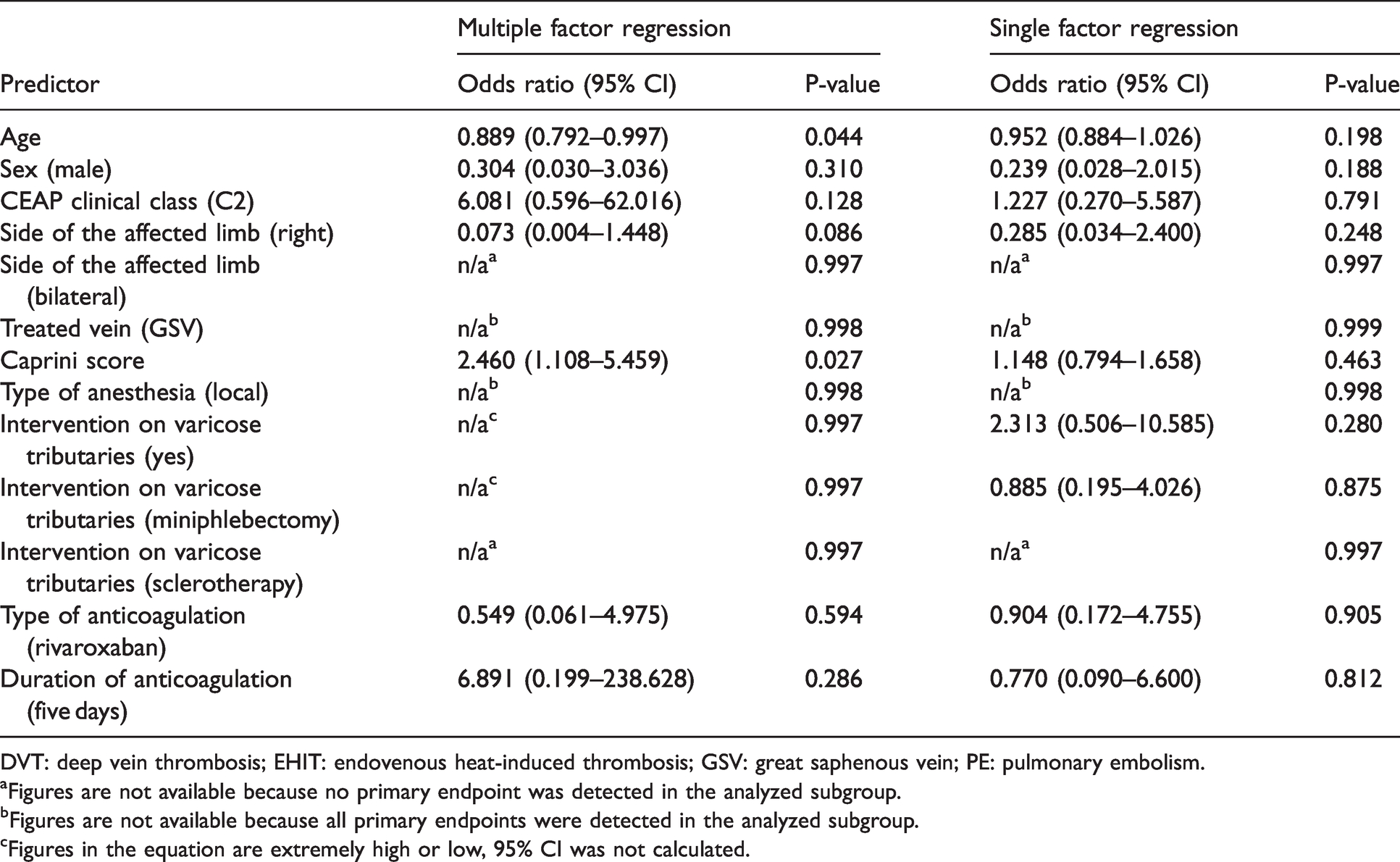
DVT: deep vein thrombosis; EHIT: endovenous heat-induced thrombosis; GSV: great saphenous vein; PE: pulmonary embolism.
aFigures are not available because no primary endpoint was detected in the analyzed subgroup.
bFigures are not available because all primary endpoints were detected in the analyzed subgroup.
cFigures in the equation are extremely high or low, 95% CI was not calculated.
Power analysis with a significance level of 5% and a power of 80% showed that our study is underpowered for demonstrating non-inferiority to the anticipated frequency of VTE events and bleeding rate in patients receiving 10 mg rivaroxaban. A recent meta-analysis 3 showed that the expected frequency of DVT (including EHIT) after endovenous thermal ablation is 1.7% with a 95% CI of 0.9–2.7%. The actual incidence of VTE events is 2.3%, the anticipated rate is 1.7%, and the non-inferiority limit is 1.0%; thus, the required sample size is 947 patients. The preliminary results of the ongoing registry trial CAPSIVS showed the 30-day incidence of symptomatic and asymptomatic VTE after modern vein surgery (predominantly laser treatment) of 3.8% in those who did not receive pharmacological prophylaxis. 12 Thus, showing the superiority of rivaroxaban over no prophylaxis will require a sample of 4120 patients. The expected bleeding rate may be extracted from the recent PRONOMOS study that evaluated the efficacy and safety of prophylactic rivaroxaban in non-major orthopedic surgery. 8 The rate of major and CRNM bleedings on rivaroxaban was 1.1% with a 95% CI of 0.7–1.7%. The required sample size is 851 patients with the actual incidence of major and CRNM bleedings of 0.9%, the anticipated rate of 1.1%, and the non-inferiority limit of 1.0%. According to the current trial findings, showing non-inferiority of rivaroxaban to enoxaparin (bleeding rate of 0.9 and 1.3%; the non-inferiority limit of 1.0%) will require a sample of 1374 patients. To demonstrate superior safety of rivaroxaban, a study enrolling 21,346 patients needs to be conducted.
Discussion
Here we present a report on once-daily 10 mg rivaroxaban use after ClosureFast radiofrequency ablation of the great and small saphenous veins with concomitant miniphlebectomy, sclerotherapy, or no treatment for varicose tributaries in patients formally having intermediate to high risk of VTE according to the Caprini score. Previously once-daily 10 mg oral rivaroxaban has already demonstrated superiority over subcutaneous once-daily 40 mg and twice-daily 30 mg enoxaparin after major arthroplasty21–24 and after non-major orthopedic surgery. 8 After laser ablation of superficial veins, it has demonstrated expected efficacy and safety comparable with fondaparinux of 2.5 mg regardless of the duration of prophylaxis (Table 5).9–11 The choice of rivaroxaban after RFA was based on the scientific evidence in the orthopedic population as well as a comfortable regimen of dosing, requiring just one tablet once daily. In contrast with other publications, we started prophylaxis before the intervention extrapolating the recommendations for general surgery. However, this approach did not affect the bleeding rate in comparison with enoxaparin and other trials, even with the concomitant miniphlebectomy. Generally, our data appeared to be complimentary with previously published, suggesting high efficacy and safety of once-daily 10 mg rivaroxaban after endovenous thermal ablation (Table 5).
The efficacy and safety of once-daily 10 mg rivaroxaban after endovenous thermal ablation.
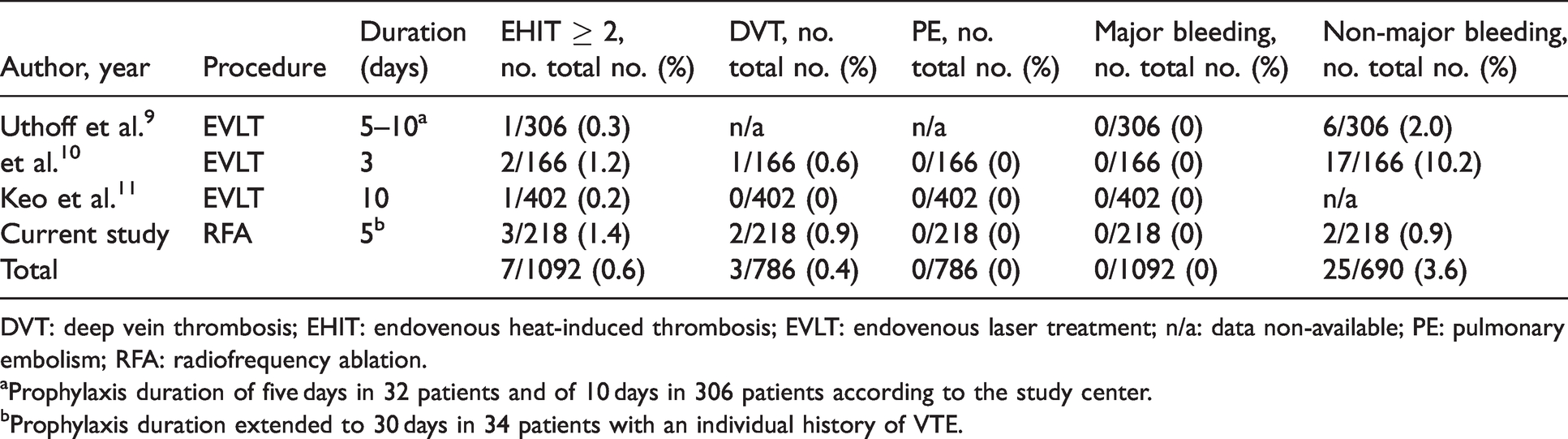
DVT: deep vein thrombosis; EHIT: endovenous heat-induced thrombosis; EVLT: endovenous laser treatment; n/a: data non-available; PE: pulmonary embolism; RFA: radiofrequency ablation.
aProphylaxis duration of five days in 32 patients and of 10 days in 306 patients according to the study center.
bProphylaxis duration extended to 30 days in 34 patients with an individual history of VTE.
The duration and indication for pharmacological prophylaxis after endovenous thermal ablation are still under debate. In our practice, we prefer using anticoagulants for at least five days after the intervention, extrapolating recommendations for the general surgical population. However, the current evidence suggests that the duration may be limited to three days. 11 In the absence of quality studies, someone can assume that three-day prophylaxis with anticoagulants does not affect the real incidence of VTE events. The small number of DVT and PE that were observed in the available reports could be related to the objectively low incidence of clinically significant thrombotic complications after modern venous surgery.12,25,26 Thus, the pharmacologic prophylaxis may not be required routinely and should be used case-to-case in subjects at increased risk (e.g. previous VTE, documented thrombophilia, obesity, immobilization, cancer, older age).1,2,4 We have observed two cases of delayed DVT after RFA that were provoked by major (leg fracture with immobilization) and minor (restarting of hormonal replacement therapy) transient risk factors. We believe that these episodes were more related to the established provoking factors than venous intervention and could occur without previous RFA. However, prolonged prophylactic anticoagulation might have prevented these episodes, so individual risk assessment for VTE is essential.
For today there is no validated risk assessment model for patients undergoing venous surgery. Despite the fact that the Caprini score was assessed in about three million surgical patients,27,28 it has not been studied in modern venous interventions. In this report, we used a threshold of ≥3 scores as an indication for obligatory pharmacological prophylaxis, as was recommended for general surgery. But it seems that it was excessive. The recent meta-analysis suggests that the benefits of prophylactic anticoagulation may be achieved only in patients with a score of 7 and higher. 27 However, in venous surgery, this threshold may be elevated due to the presence of varicose veins in every patient and the possible presence of venous edema. These risk factors provide two additional points but are to be treated at the same time. Thus we believe that the benefit of prophylactic anticoagulation starts at the Caprini score of 8–10 in patients undergoing venous surgery. The first results of the ongoing prospective registry study CAPSIVS demonstrated a significant correlation between the Caprini score and the risk of asymptomatic VTE after modern venous intervention. 12 However, it was impossible to identify the appropriate threshold for VTE prediction.
It is essential to mention that our local protocol for RFA with ClosureFast has some differences from the international protocols and manufacturer’s instruction. 29 Mainly we routinely position the catheter more closely to the junction (2 cm in contrast to recommended 3 cm) and perform more heating cycles for significantly dilated veins (three cycles at the junction and one to three cycles along the trunk in comparison with two cycles at the junction and one cycle along the trunk). The rationale is based on the previously published experimental data suggesting that the depth of vein wall injury depends on the number of cycles and three cycles that damage all layers. 30 In Russia, the concern for vein recanalization is more significant than for EHIT and postoperative pain or discomfort. Thus most physicians prefer aggressive regimes of endothermal ablation.
Undoubtedly, this study has serious limitations to make a strong conclusion on the efficacy and safety of once-daily 10 mg rivaroxaban after endovenous radiofrequency ablation. It was retrospective, observational, without compliance measurement, and underpowered to provide any statistically significant results. Routinely we did not assess the disease severity by VCSS, did not evaluate the quality of life, did not report the incidence of EHIT 1, did not measure the bruising, so these data were unavailable for extraction. However, this study gives some additional information that, in combination with previously published, allows suggesting the efficacy and safety VTE prophylaxis after venous surgery with oral rivaroxaban. This hypothesis should be confirmed in more powerful randomized clinical trials assessing the benefits of pharmacological prophylaxis, particularly with direct oral anticoagulants, after modern interventions for varicose veins.
Conclusion
This study suggests that once-daily 10 mg oral rivaroxaban may be suitable for VTE prophylaxis in ClosureFast radiofrequency ablation of saphenous veins.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EM received honoraria for master-classes from Medtronic, travel grants from Bayer, KL received honoraria for lectures and travel grants from Bayer, LL, AD, and IP nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study follows the principles outlined in the Declaration of Helsinki. It did not require any additional informed consent due to retrospective character, as had been confirmed by the Institutional Review Board of the Pirogov Russian National Research Medical University.
Guarantor
KL.
Contributorship
KL, LL, AD, and IP researched literature and conceived the study. EM and IP collected the data. KL made statistical analyses. EM, KL, LL, AD, and IP interpreted the results. KL wrote the first draft of the manuscript. All authors reviewed the manuscript critically for important intellectual content and approved the final version of it.