
Abstract
Background
Totally implantable venous access port (TIVAP) is a completely closed intravenous infusion system that stays in the human body for a long time. It is used for the infusion of strong irritating or hyperosmotic drugs, nutritional support treatment, blood transfusion and blood specimen collection, and other purposes. There are two common ways of TIVAP: internal jugular vein implantation and subclavian vein implantation. However, the postoperative complications of the two implantation methods are quite different, and there is no recommended implantation method in the relevant guidelines. Therefore, we conducted a meta-analysis to evaluate the difference in complications of the two implantation methods, and choose the better implantation method.
Methods
Computer search in PubMed, Embase, Web of Science, and Cochrane Library database was conducted for randomized controlled trials (RCTs) from the establishment of the database to October 2021. Two researchers independently screened the literature according to the inclusion and exclusion criteria, extracted data, and evaluated the risk of bias in the included studies. RevMan5.4 software was used for meta-analysis.
Results
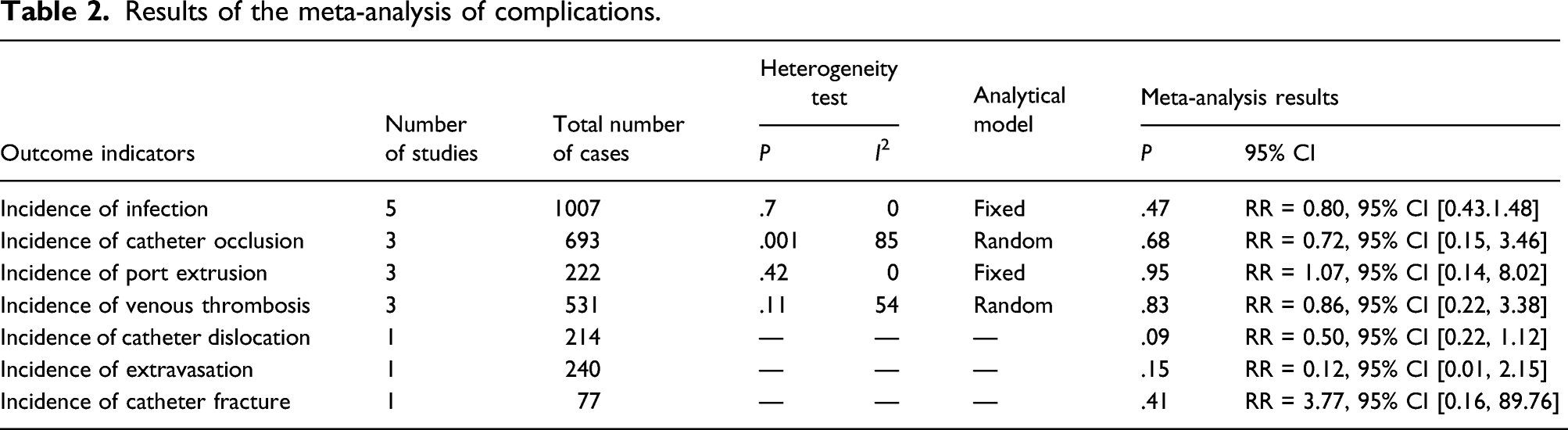
A total of 1086 patients in five studies were finally included. The results of meta-analysis showed that there was no significant difference in the incidence of infection (RR = 0.80, 95% CI: 0.43–1.48, p = .47), catheter blockage (RR = 0.72, 95% CI: 0.15–3.46, p = .68), port squeeze (RR = 1.07, 95% CI: 0.14–8.02, p = .95), catheter-related thrombosis (RR = 0.86, 95% CI: 0.22–3.38, p = 0.83), catheter displacement (RR = 0.50, 95% CI: 0.22–1.12, p = .09), extravasation (RR = 0.12, 95% CI: 0.01–2.15, p = .15), and catheter rupture (RR = 3.77, 95% CI: 0.16–89.76, p = .41) between the two implantation paths.
Conclusions
There is little difference in the complication rate of TIVAP between internal jugular vein insertion and subclavian vein insertion. Due to the small number of included studies, there are certain limitations, and more studies need to be included for analysis in the future.
Keywords
Introduction
Totally implantable venous access port (TIVAP) is a closed venous access infusion device that can be completely implanted in the human body, which is mainly composed of an injection seat for puncture and a venous catheter system.1,2 It can be used for infusion of various irritating or high permeability drugs, rehydration, nutritional support, blood product infusion, blood sample collection, etc., to provide patients with long-term venous access, especially for patients with poor peripheral veins. TIVAP implantation has the advantages of simple operation, low complication rate, and convenient use for patients. 3 At present, TIVAP has become the prior choice for cancer chemotherapy and patients who need long-term infusion.4,5 The American Society of Infusion Nursing recommends that patients with tumor infusion should use a central venous infusion device, of which TIVAP is preferred. 6
The puncture path of TIVAP mainly includes internal jugular vein, subclavian vein, axillary vein, femoral vein, and so on. The common insertion routes are internal jugular vein and subclavian vein. 7 The use of subclavian vein approach to implant infusion ports is rare in literature, but authoritative journals have reported that this method is a simple and safe deep vein route with low complications. 8 In addition, it is reported in the literature that the subclavian vein approach has a high incidence of pneumothorax, and has unique complications of clipping syndrome, while the internal jugular vein approach has lower symptomatic thrombosis. 9
At present, the published randomized controlled trials (RCTs) showed that the postoperative complications of the two implantation methods were quite different.10–14 At the same time, there is no recommended placement method in the relevant guidelines. 15 Therefore, this study analyzed the differences in the occurrence of different complications after subclavian implantation and transcervical implantation of TIVAP through a systematic review, and provided evidence-based basis for clinical medical staff to choose the path of TIVAP implantation.
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and the recommendations of the Cochrane Collaboration. 16
Data Sources and Searches
Computer search in PubMed, Embase, Web of Science, and Cochrane Library database was conducted from the establishment of the database to October 2021. RCTs were retrieved and collected for complications of internal jugular and subclavian vein placement of TIVAP. The combinations of free words and MeSH words which were used to search include TIVAPs, totally implantable venous device, Port-A-Cath, TIVA, port, ports, TIAP/TIVAP, jugular vein, Subclavian vein, complications.
Study Selection
(1) Research type: RCTs. (2) Research objects: patients who need to be placed in the infusion port. (3) Intervention measures: TIVAP was inserted into the internal jugular vein or the subclavian vein was inserted into the patient. (4) Outcome indicators: The occurrence of complications of TIVAP implantation, including the incidence of infection, catheter blockage, port extrusion, catheter-related thrombosis, catheter displacement, extravasation, and catheter fracture.
Data Extraction
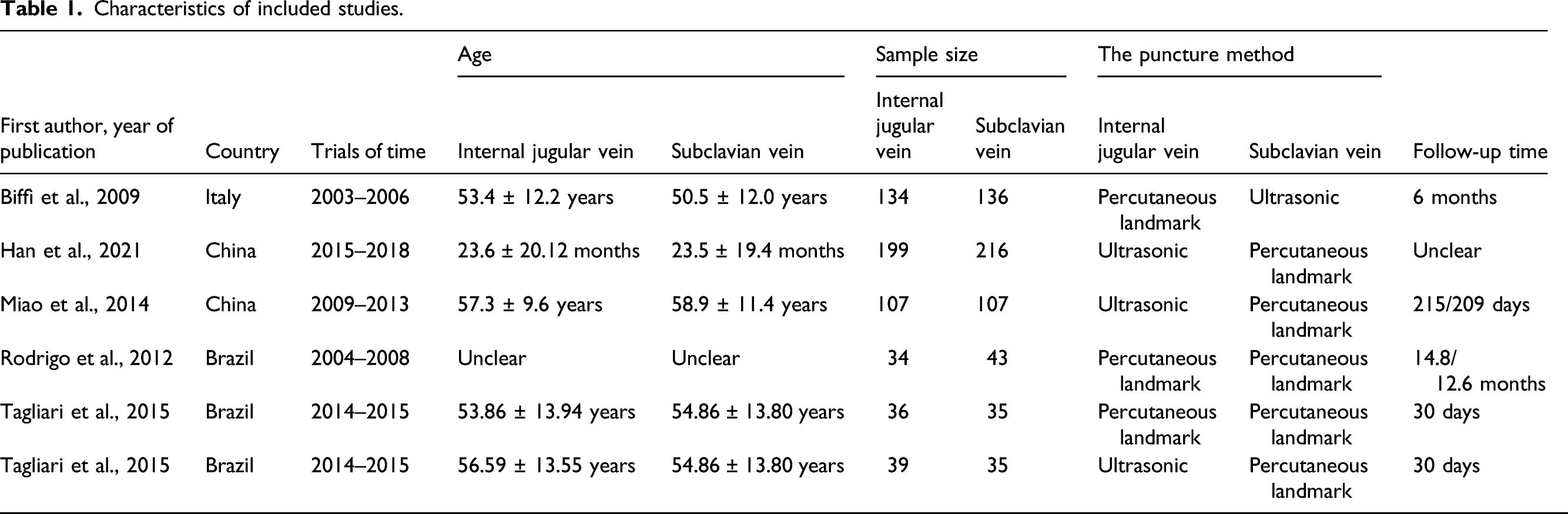
Two reviewers independently screened the literature, extracted data and assessed the risk bias of the included studies, and cross-checked them. If there was a disagreement, it would be resolved through discussion or negotiation with a third-party researcher. For literatures with missing full text or partial information, contact the original research authors via email to obtain information. The extracted content includes: first author, year of publication, country, age of research object, intervention measures, sample size, puncture method, follow-up time, and outcome indicators.
Quality Assessment
The RCT bias risk assessment tool recommended by the Cochrane Handbook was used to assess the bias risk of RCT, including: (1) random method; (2) allocation concealment; (3) blinding of patients and interveners; (4) outcome evaluation; (5) lost to follow-up; (6) selective reporting; and (7) other biases. The evaluation results are expressed as “high risk,” “low risk,” and “unclear.”
Statistical Analysis
Meta-analysis was performed using RevMan 5.4 software. The data type of this study is a binary variable, and the relative risk ratio (RR) and its 95% CI are used as the effect analysis statistics. The heterogeneity among the results of the included studies was analyzed by the χ2 test (the test level is α = 0.1), and I2 was used to quantitatively judge the size of the heterogeneity. When p < .1 and/or I2 > 50%, the random effects model was used for the combined analysis, otherwise, the fixed effects model was used for the combined analysis. Sensitivity analysis was applied for heterogeneity sources. A funnel chart was used to assess possible publication bias and small sample bias.
Results
Literature search results and basic characteristics
Characteristics of included studies.

Flowchart of literature selection.
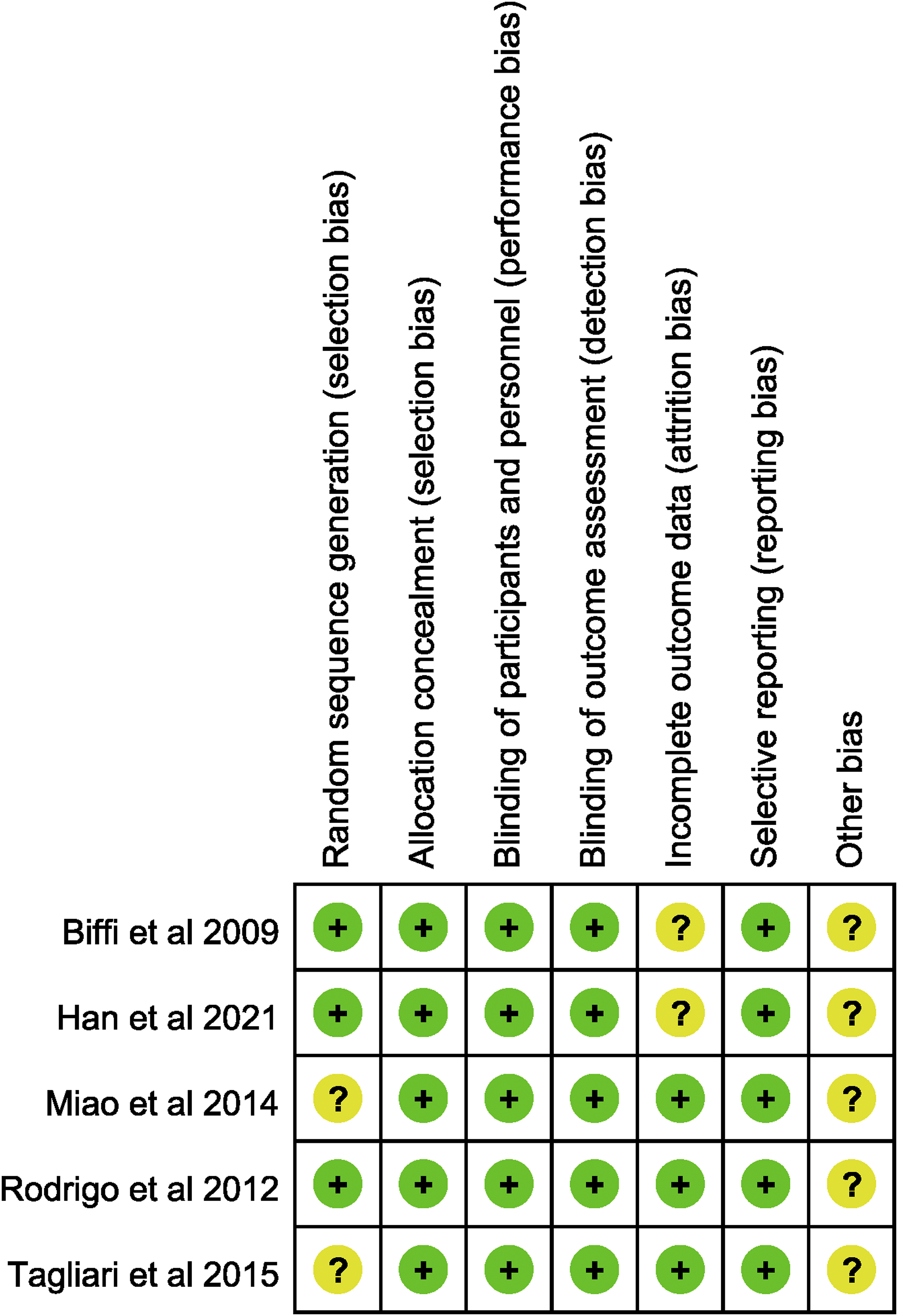
Risk of bias summary.
Meta-analysis of results
Incidence of infection
Results of the meta-analysis of complications.
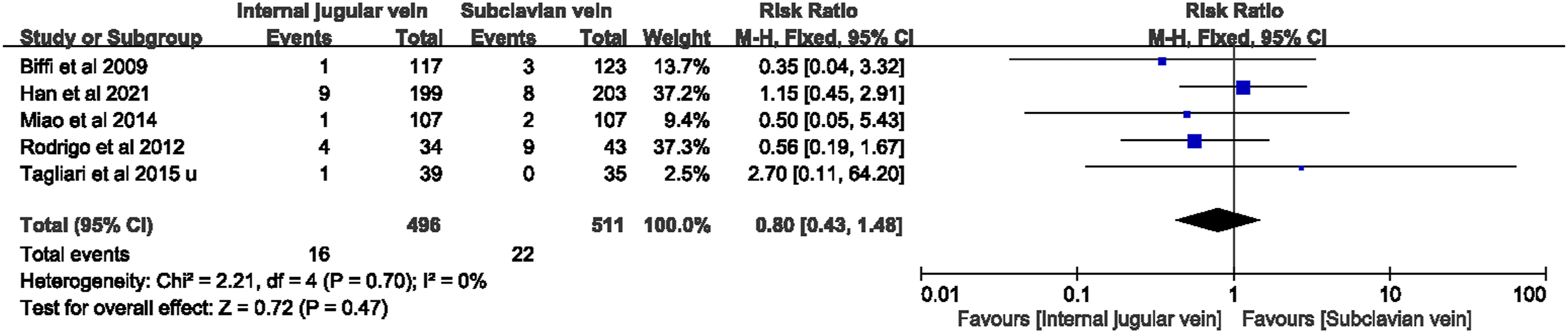
Forest plot of incidence of infection.
Incidence of catheter occlusion
There were three studies included.11–13 The heterogeneity between studies was not statistically significant (I2 = 85%, p = .001), and the random effects model was used for analysis. The results showed that there was no statistically significant difference in the incidence of catheter blockage between the internal jugular vein catheterization group and the subclavian vein catheterization group (RR = 0.72, 95% CI: 0.15–3.46, p = .68) (Table 2, Figure 4). Use one-by-one elimination method for sensitivity analysis. The results showed that when Han et al.
11
literature was excluded, the heterogeneity decreased, and the combined effect size was (RR = 0.32, 95% CI: 0.15–0.69, p = .003). This might be related to the large sample size studied by Han et al.
11
Forest plot of incidence of catheter occlusion.
Incidence of port extrusion
Two studies were included.13,14 The heterogeneity between studies was not statistically significant (I2 = 0, p = .42), and the fixed effects model was used for analysis. The results showed that there was no significant difference in the incidence of port compression between the internal jugular vein catheterization group and the subclavian vein catheterization group (RR = 1.07, 95% CI: 0.14–8.02, p = .95) (Table 2, Figure 5). The sensitivity analysis was carried out by the one-by-one elimination method, and the change of the combined effect size was not obvious, and the result was relatively stable. Forest plot of incidence of port extrusion.
Incidence of venous thrombosis
Three studies were included.10,12,13 The heterogeneity between studies was not statistically significant (I2 = 54, p = .11), and the random effects model was used for analysis. The results showed that there was no significant difference in the incidence of venous thrombosis between the internal jugular vein catheterization group and the subclavian vein catheterization group (RR = 0.86, 95% CI: 0.22–3.38, p = .83) (Table 2, Figure 6). The sensitivity analysis was carried out by the one-by-one elimination method, and the change of the combined effect size was not obvious, and the result was relatively stable. Forest plot of incidence of venous thrombosis.
Incidence of catheter dislocation
One study 12 was included. The results showed that there was no significant difference in the incidence of catheter displacement between the internal jugular vein catheterization group and the subclavian vein catheterization group (RR = 0.50, 95% CI: 0.22–1.12, p = .09) (Table 2).
Incidence of extravasation
One study 10 was included. The results showed that there was no significant difference in the incidence of extravasation between the internal jugular vein catheterization group and the subclavian vein catheterization group (RR = 0.12, 95% CI: 0.01–2.15, p = .15) (Table 2).
Incidence of catheter fracture
One study 13 was included. The results showed that there was no significant difference in the incidence of catheter rupture between the internal jugular vein catheterization group and the subclavian vein catheterization group (RR = 3.77, 95% CI: 0.16–89.76, p = .41) (Table 2).
Publication bias
Since less than 10 articles were included, the publication bias analysis could not be performed.
Discussion
The application of TIVAP can be regarded as a leap-forward development of infusion technology. It could greatly reduce the risk of drug infusion, especially chemotherapy drugs. 17 At the same time, it could improve the quality of life of cancer patients and patients who need long-term intravenous therapy.18,19 TIVAP is completely implanted under the skin and can be left in the body for a long time, with the advantages of little impact on patients, easy to carry and easy to maintain.20,21 At present, internal jugular vein and subclavian vein implantation are mostly used in clinical practice. However, the complications of the two implantation routes are quite different. Therefore, we collected relevant RCTs and conducted a meta-analysis to provide evidence for clinical application.
This meta-analysis compared the occurrence of complications in the port of infusion after catheterization through the internal jugular vein and through the subclavian vein. The results showed that there was no statistically significant difference in the incidence of infection, catheter blockage, port compression, catheter-related thrombosis, catheter displacement, extravasation, and catheter rupture between the two implantation routes.
Infection is the most common complication of infusion ports. The main causes are long catheterization time, frequent puncture, irregular butterfly wing replacement, long-term total parenteral nutrition, neutropenia and hematological malignancies. There are literatures introducing the “antibacterial lock” technology. 22 To a certain extent, the occurrence of infection can be reduced, but there are also certain limitations.18,23,24 Catheter-associated infections are the most frequent complication after TIVAP implantation. Related studies have shown that puncture technique is associated with catheter-associated infections and that ultrasound guidance could reduce the incidence of catheter-associated infections. 25 Several guidelines also recommend the use of ultrasound-guided cannulation techniques to reduce the incidence of catheter-related infections.26–28 The puncture modalities in those included studies were divided into direct percutaneous puncture and percutaneous puncture under ultrasound guidance. Puncturing the vein according to the body markers is prone to corresponding complications such as pneumothorax, hematoma, vascular injury, and clamping syndrome, and the success of puncture depends largely on the operator’s technique and experience. The use of ultrasound-guided venipuncture, on the other hand, allows accurate localization, significantly improves the success rate of cannulation, and reduces the complications caused by puncture.27–29 Therefore, ultrasound-guided percutaneous puncture placement is highly recommended.30,31Related guidelines suggest that the prevention of catheter-associated infections should begin with the education and training of healthcare workers. 26 Emphasis on training and quality control can reduce the incidence of catheter-associated bloodstream infections and it is also an effective measure to reduce morbidity and mortality.32,33 Standardization will greatly reduce the risk of infection. 34 For healthcare professionals, maximum sterile barrier should be recommended.34,35 For catheter placement and care, sterile gloves and strict aseptic principles should be used.28,35 Also, before and after palpation, implantation, viewing, adjustment of infusion ports or dressing changes, strict hand hygiene practices should be applied.27,36 In general, the use and maintenance of TIVAP must strictly abide by the principle of aseptic operation, which is the key to preventing infection.36,37
Catheter blockage is manifested by blood disorders in bolus injection and withdrawal. The main reasons are the formation of fibrin sheath, long-term infusion of high concentration, strong irritant drugs, total parenteral nutrition, irregular tube flushing, and tube sealing. The prevention of the obstruction of the infusion port catheter is to use heparin sodium solution before and after each infusion and to use positive pressure technology to flush and seal the tube for regular maintenance.6,17 Once the catheter is blocked, first perform a chest X-ray to confirm the position of the intravenous infusion port, 38 and detect the cause of the blockage of the catheter.
Port squeeze is mainly due to the occurrence of catheter clamping syndrome, which is common in transclavicular catheterization.39,40 The catheter enters the narrow gap between the first rib and the clavicle when the catheter is inserted through the subclavian vein puncture, and it is squeezed by the gap to produce stenosis or clip, which makes the catheter blocked.
Studies have shown that the incidence of catheter-associated thrombosis due to TIVAP was 1.06%–11.4%.41,42 In contrast, other central venous placements resulted in an incidence of 2–75%. 43 The incidence of symptomatic thrombosis due to TIVAP is significantly lower than that of other central venous placements, but the incidence of asymptomatic thrombosis due to TIVAP has not been reported in the literature. In severe cases, it can cause pulmonary embolism. Fibrin sheath formation, history of thrombosis, history of pulmonary embolism, history of blood system diseases, type and stage of cancer, type and frequency of chemotherapy, type and location of catheter, D-dimer quantification, and fibrinogen quantification abnormalities are related factors of infusion port-related thrombosis. In addition, the technique of cannulation may play a role in the induction of thrombosis. Studies have shown an association between minimal damage to the venous wall by ultrasound-guided cannulation techniques and a lower incidence of subsequent thrombotic events. 34 Ultrasound-guided venipuncture for TIVAP implantation, with high puncture success rate, few complications, is easy to master and suitable for clinical implementation. If it is clear that it is a catheter-related venous thrombosis, anticoagulation treatment should be given first. 18 For patients contraindicated to anticoagulation, unplanned port withdrawal should be considered. If there is no anticoagulation taboo, the port body can be retained temporarily, but long-term anticoagulation therapy is needed. 44 Preventive anticoagulation is not routinely recommended at present, for the results of relevant literature data are inconsistent, and the efficacy and adverse reactions are not clear.18,45,46
Insufficient catheterization depth, excessive movement of the upper arm of the patient, neck flexion, and increased chest and abdomen pressures such as coughing and vomiting can cause catheter displacement. Therefore, after catheterization, the catheter should be properly fixed and checked regularly to avoid displacement twists and turns to ensure patency. Also, health education is needed to guide patients to lead a correct life. 6
Loosening of butterfly needle, shedding of catheter lock, disconnection of interface and displacement of catheter can all lead to extravasation. After the butterfly wing needle puncture, the patients should be taught to pay attention to protect the puncture place, to avoid collision and strenuous abduction activities and chest expansion, and to avoid damage caused by extravasation. 47
The catheter breaks are mainly in the following locations: (1) the infusion port-catheter connection part; (2) the subcutaneous tunnel part; (3) the catheter insertion vein; and (4) the intravenous part. Severe catheter clamping syndrome, 39 strenuous abduction movements of the upper limbs, extraction of heavy objects, and catheter materials are all factors that cause the catheter to break. Regular inspection and maintenance can detect pipe breaks in time. 48
Due to the incidence of catheter displacement, extravasation, and catheter rupture, only one article was included. Such complications need more research to discuss in the future.
Limitations
This study has certain limitations: (1) All the literatures retrieved were in English, which may be biased; (2) the number of included studies was small, and further analysis of multi-center, large sample, high-quality studies is still needed in the later period; (3) part of the outcome indicators could not be combined for analysis due to few studies; (4) there were too few included studies to perform subgroup analysis; (4) each research was carried out in different countries and hospitals, and doctors were in different professional levels.
Conclusions
In summary, there is little difference in the complication rate of TIVAD between internal jugular vein insertion and subclavian vein insertion, and both are safe, effective, and reliable venous access. Medical staff can choose either, according to the actual situation of patients, so as to reduce the occurrence of related complications. However, the occurrence of complications is affected by many factors. This meta-analysis includes fewer RCT studies and lacks more sample sizes. Therefore, it is necessary to obtain multi-sample and high-quality studies to further explore the advantages and disadvantages of the two implant pathway technologies.
Footnotes
Acknowledgments
The authors thank the authors of the included studies who shared the important data.
Author contributions
Data collection: Qiang Zhang and Jifang Song. Literature retrieval: Juan He and Na Peng. Software operating: Qiang Zhang and Jifang Song. Supervision: Xinxin Yang; Writing—original draft: Ya Zhou, Yanqiu Lan, and Xinxin Yang. Writing—review and editing: Ya Zhou, Yanqiu Lan, Xingqiao Peng, and Xinxin Yang.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
XY.