
Abstract
Objective
To investigate the risk factors, predilection sites in pulmonary embolism (PE) patients caused by deep venous thrombosis (DVT) and explore the value of scoring systems in assessing the risk of PE in DVT patients.
Methods
A total of 692 DVT patients were enrolled, and divided into no pulmonary embolism (NPE, 226, 32.66%), silent pulmonary embolism (SPE, 330, 47.67%) and featuring pulmonary embolism (FPE, 136, 19.65%) groups. For each group, the differences of clinical data and PE locations were compared, and the risk factors of PE secondary to DVT were analyzed. The predictive value of the scoring system for the diagnosis of PE and FPE was evaluated.
Results
PE presented more in the bilateral pulmonary arteries (PAs) (249, 53.43%) and has no significant difference in PESI scores in different locations. Gender, DVT locations, and previous surgery were the independent risk factors of PE. DVT locations, previous history of COPD, and previous surgical interventions were the independent risk factors of FPE. The results for areas under the ROC curves were: AUC(Wells) = 0.675, AUC (Revised Geneva) = 0.601, AUC(D-dimer) = 0.595 in the PE group; AUC(Wells) = 0.722, AUC (Revised Geneva) = 0.643, AUC(D-dimer) = 0.557 in the FPE group.
Conclusions
PE secondary to DVT mostly occurs in the bilateral PAs. Male gender, DVT locations, and previous surgery increased the risk of PE. The Wells scoring system was more advantageous for evaluating the diagnosis of PE in patients with DVT.
Introduction
Venous thromboembolism (VTE) is a common clinical disease with an incidence of 100–200 cases per 100,000 people. It mainly manifests as deep venous thrombosis (DVT) and pulmonary embolism (PE). VTE is the most common cardiovascular disease underlying acute myocardial infarction and stroke.1,2 PE is a concealed high mortality disease and is generally considered to be the result of DVT. The risk factors of PE include two main categories: inherited and acquired. One of the strongest risk factors for VTE is a history of prior VTE. 3 Approximately 10% of symptomatic acute PE patients die within 1 h of the first presentation of symptoms; the mortality rate of untreated PE patients is high at 15%. 4 Meanwhile, DVT and PE, which are secondary to DVT, also cause a huge economic burden to the social medical system.
The clinical presentation of DVT and PE varies according to the size of the thrombus and the degree of embolization. The typical clinical manifestations of DVT include swelling, pain, fever, and redness of the affected limb. PE lacks typical clinical presentation, the most common signs and symptoms include dyspnea, chest pain, shortness of breath, syncope, and cough. It may also manifest as fever, hemoptysis, cyanosis, hypotension, and shock. 5
Thrombus can be distributed into two major areas in PE, the central vascular area (the main pulmonary artery (PA) and the left or right PA) and the peripheral vascular area (segmental or subsegmental PA, not in the main PA). 6 Peripheral PE is defined as thrombus only in lobar. Clinical manifestations of PE in the peripheral vascular area are usually mild and atypical; therefore, diagnosis of VTE based only on clinical manifestations and signs has great limitations. Currently, the diagnosis of PE mainly depends on pulmonary angiography and computed tomography pulmonary angiography (CTPA). However, the extensive use of pulmonary angiography or CTPA not only increases the economic burden, but can also cause adverse reactions such as unnecessary radiation and contrast nephropathy. 7 Some patients in basic-level hospitals cannot undergo CTPA examination due to the limited access in developing countries, so long distance travel to a more specialized hospital is needed to undergo CTPA, however, transportation is risky due to their condition. Therefore, carrying out effective clinical evaluations of DVT patients as a reliable alternative to imaging examination for those at high risk of PE is warranted to avoid unnecessary injury and excessive waste of medical resources caused by extensive imaging diagnosis technology.
In this study, PE patients with DVT symptoms as the first manifestation, analyzing PE locations, risk factors, and the clinical possibility assessments’ score system was studied, then the possible methods of risk stratification of PE were discussed.
Patients and methods
Study objects and groups
This was a retrospective and observational study. The consecutive patients diagnosed with DVT in the First Affiliated Hospital of Chongqing Medical University from July 2013 to August 2018 were selected as study objects. The inclusive criteria were: 1) patients had the clinical manifestations of DVT (swelling, pain, fever, and redness of the affected limb), whether followed by the characteristic clinical manifestations (chest pain, dyspnea, and hemoptysis) of PE at admission; 2) patients were diagnosed with DVT by Doppler ultrasound at admission; 3) CTPA examination was performed in DVT patients, the cases without CTPA examination were excluded after admission. The color Doppler ultrasound and CTPA examination were conducted and interpreted by the ultrasound doctor and the radiologist, respectively. Whether to conduct CTPA examination was decided by the clinician, rather than the researcher. Chest pain, dyspnea, and hemoptysis were defined as the featured clinical presentations of PE. According to CTPA and the clinical presentation, all of the patients were divided into three groups: no PE group (NPE) where no PE was found by CTPA; silent PE group (SPE) where CTPA confirmed the presence of PE but it did not have any of the characteristic manifestations of PE; featuring PE group (FPE) where CTPA diagnosed the presence of PE and it presented with one or more of the characteristic clinical manifestations of PE.
Clinical data collection
General data such as age, gender, and survival status after 30 days was collected, and the previous medical history of all patients was recorded. In addition, electrocardiogram, cardiac enzyme levels, pulmonary arterial systolic pressure (PASP), D-dimer, DVT, and PE locations were recorded in all patients. The Wells score, Revised Geneva score, and pulmonary embolism severity index (PESI) were performed on all enrolled patients, and these score systems were calculated by two attending doctors among the researchers.
Statistical analysis
Statistical analysis and drawings were performed with the SPSS 17.0 statistical package software and GraphPad Prism 5 software. The sample descriptive statistics data were expressed as means ± standard deviation (x ± s), and analyzed with the t-test; the chi-square test was used to analyze the count data. Using a binary logistic regression model to analyze risk factors, an ROC curve was used to evaluate the possibility of PE. The statistical significance was defined by P < 0.05.
Results
General clinical data of the VTE patients
Of the 2470 consecutive DVT patients screened, there were 1770 DVT patients without CTPA examination and eight patients with incomplete clinical data were excluded. However, 692 patients met the inclusion criteria (Figure 1). The average age of the 692 DVT patients was 59.59 ± 15.51 years; the number of males was 373 (53.90%). Among the 692 patients, 226 (32.66%) patients were in the NPE group, 330 (47.69%) cases in the SPE group, and 136 (19.65%) cases in the FPE group. Four patients died within 30 days in the FPE group.

Patient flow diagram.
In this study, there was no significant difference in age distribution among the three groups. Male patients accounted for 40.71% (92/226), 60.30% (199/330) and 60.29% (82/136) in the NPE, SPE and FPE groups, respectively, and there were more male cases than female cases. Moreover, the proportion of DVT in the right lower extremity was higher in the SPE group than in the FPE and NPE groups (28.79% > 24.26% > 17.26%); the difference was statistically significant compared with the NPE group (P < 0.05). In patients with coronary heart disease, chronic obstructive pulmonary disease (COPD), arrhythmia, and other underlying diseases, PE was more likely to manifest clinical symptoms. The incidence of pulmonary hypertension in the FPE group was significantly higher than that in the NPE and SPE groups (Table 1).
Clinical features and outcome of patients with VTE.

aRepresents comparison with NPE group, P < 0.05.
bRepresents comparison with SPE group, P < 0.05.
COPD: chronic obstructive pulmonary disease.
Diagnosis of pulmonary hypertension: echocardiography showed PASP > 35 mmHg. 8
Risk factors analysis of PE in patients with DVT
Binary logistic regression analysis was used to identify independent risk factors for PE and FPE. The results showed that males (odds ratio (OR) 1.977, 95% confidence interval (CI) 1.404–2.784) with DVT in left lower limbs (OR 2.078, 95% CI 1.171–3.687) and a surgical history (OR 2.100, 95% CI 1.220–3.687) (P < 0.05) were independent risk factors for PE (Table 2). However, DVT in right lower limbs (OR 1.966, 95% CI 1.005–3.846) with a surgical history (OR 3.092, 95% CI 1.553–6.158) and previous history of COPD (OR 0.187, 95% CI 0.085–0.410) were independent risk factors for FPE (P < 0.05) (Table 3).
Risk factors for PE in patients with DVT by binary analysis.
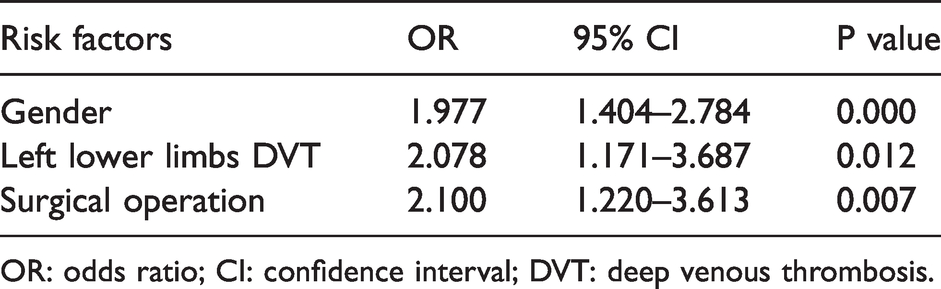
OR: odds ratio; CI: confidence interval; DVT: deep venous thrombosis.
Risk factors for FPE in patients with DVT by binary analysis.
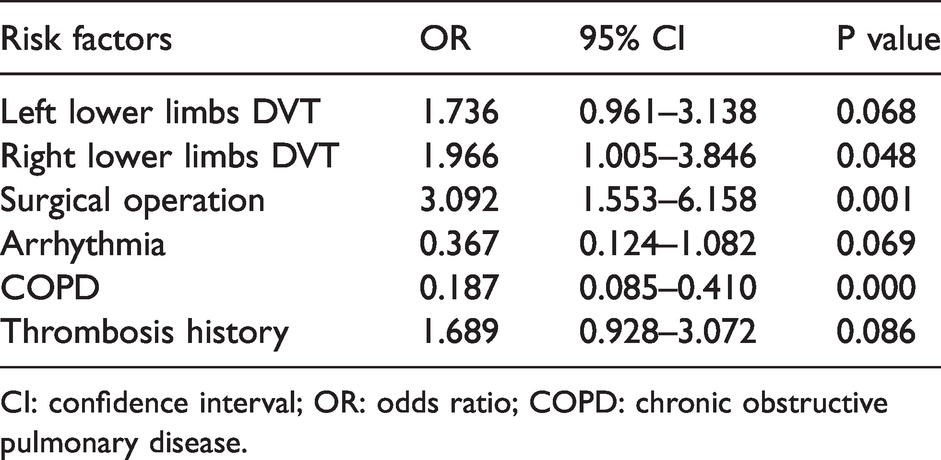
CI: confidence interval; OR: odds ratio; COPD: chronic obstructive pulmonary disease.
Analysis of embolism locations in PE patients with DVT
Among all PE patients, embolism occurring in bilateral pulmonary arteries (PAs) was the most common (249, 53.43%), followed by unilateral right PA (158, 33.91%), and the least common was unilateral left PA (59, 12.66%). This distribution pattern appeared in both the SPE and FPE groups (Figure 2). In the SPE group, 174 cases (52.73%) had bilateral embolism, 118 cases (35.76%) had right embolism, and 38 cases (11.52%) had left embolism. In the FPE group, bilateral embolism occurred in 75 cases (55.15%). 40 cases (29.41%) had right-sided embolism, and 21 cases (15.44%) had left-sided embolism.
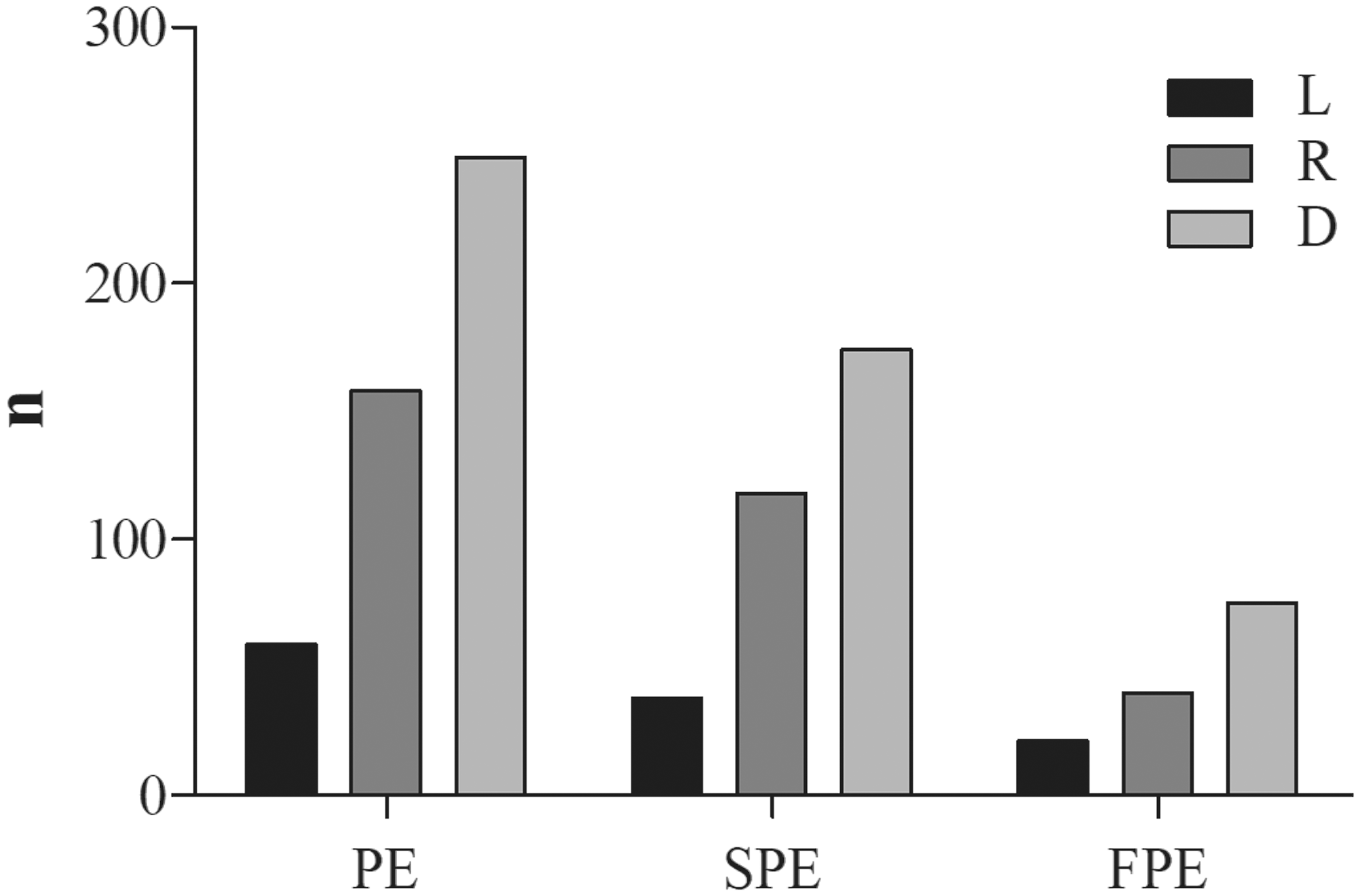
The number of PE locations in different group.
The accurate locations (central and peripheral PAs) of PE was further analyzed. Results showed that the embolized areas were mainly distributed in the inferior lobe of the left lung (50.22%) and the inferior lobe of right lung (69.74%) in the PE group. The SPE group embolized areas were also more distributed in the inferior lobe of lung. However, in the FPE group, embolism was in the superior lobe of the left lung (42.65%) and the superior lobe of right lung (53.68%). Compared with the SPE group, the FPE group’s emboli occurred more in the pulmonary trunk and upper lobe of the lung, and less in the lower lobe; the differences were statistically significant (Table 4).
The locations of PE in different groups.

PA: pulmonary artery; PE: pulmonary embolism; NPE: no pulmonary embolism; SPE: silent pulmonary embolism; FPE: featuring pulmonary embolism; DVT: deep venous thrombosis.
Severity levels of PE patients with DVT
In this study, PESI was used to assess the severity and prognosis of PE patients. It was graded into three risk classes; I–II – low risk, III–IV – moderate risk, and V – high-risk. The average PESI scores in all PE patients were 76.47 ± 27.64, with a large proportion of low-risk patients (I–II class) (Table 5). PESI scores for the FPE group were significantly higher than those of the SPE group (86.10 ± 37.20 vs. 70.33 ± 19.82, P = 0.000).
The PESI class of PE in different groups.
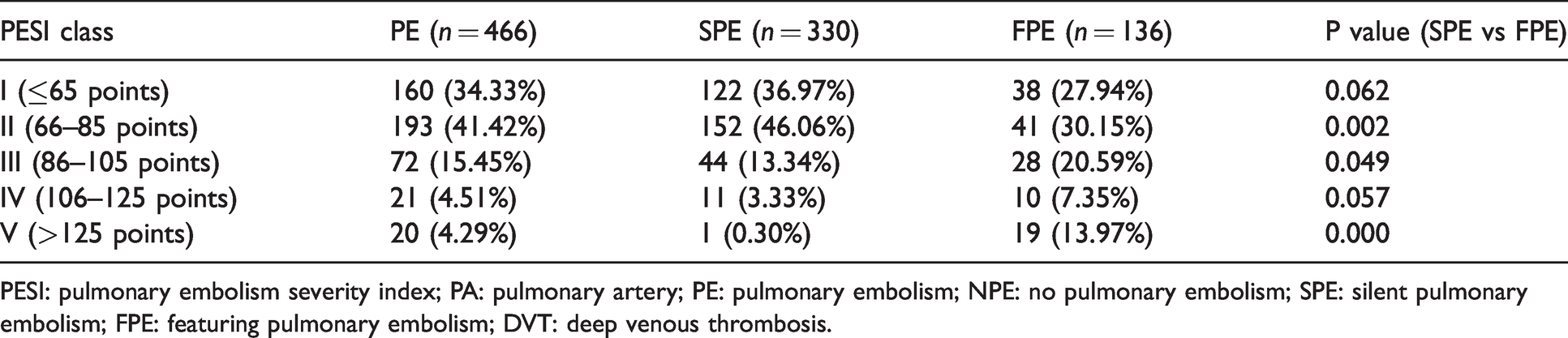
PESI: pulmonary embolism severity index; PA: pulmonary artery; PE: pulmonary embolism; NPE: no pulmonary embolism; SPE: silent pulmonary embolism; FPE: featuring pulmonary embolism; DVT: deep venous thrombosis.
We further analysis of the relationship between PE locations and PESI showed that PESI scoring had no statistically significant difference in all PE patients, regardless of whether the embolization location was unilateral or bilateral. Although the PESI of right PE was higher in the SPE group than the bilateral PE (71.88 ± 17.77 vs 69.77 ± 19.57, P = 0.029), they were all low risk (class II). There was no statistically significant difference in PESI scores in the FPE group when PE occurred on the left, right, or both sides (Figure 3).
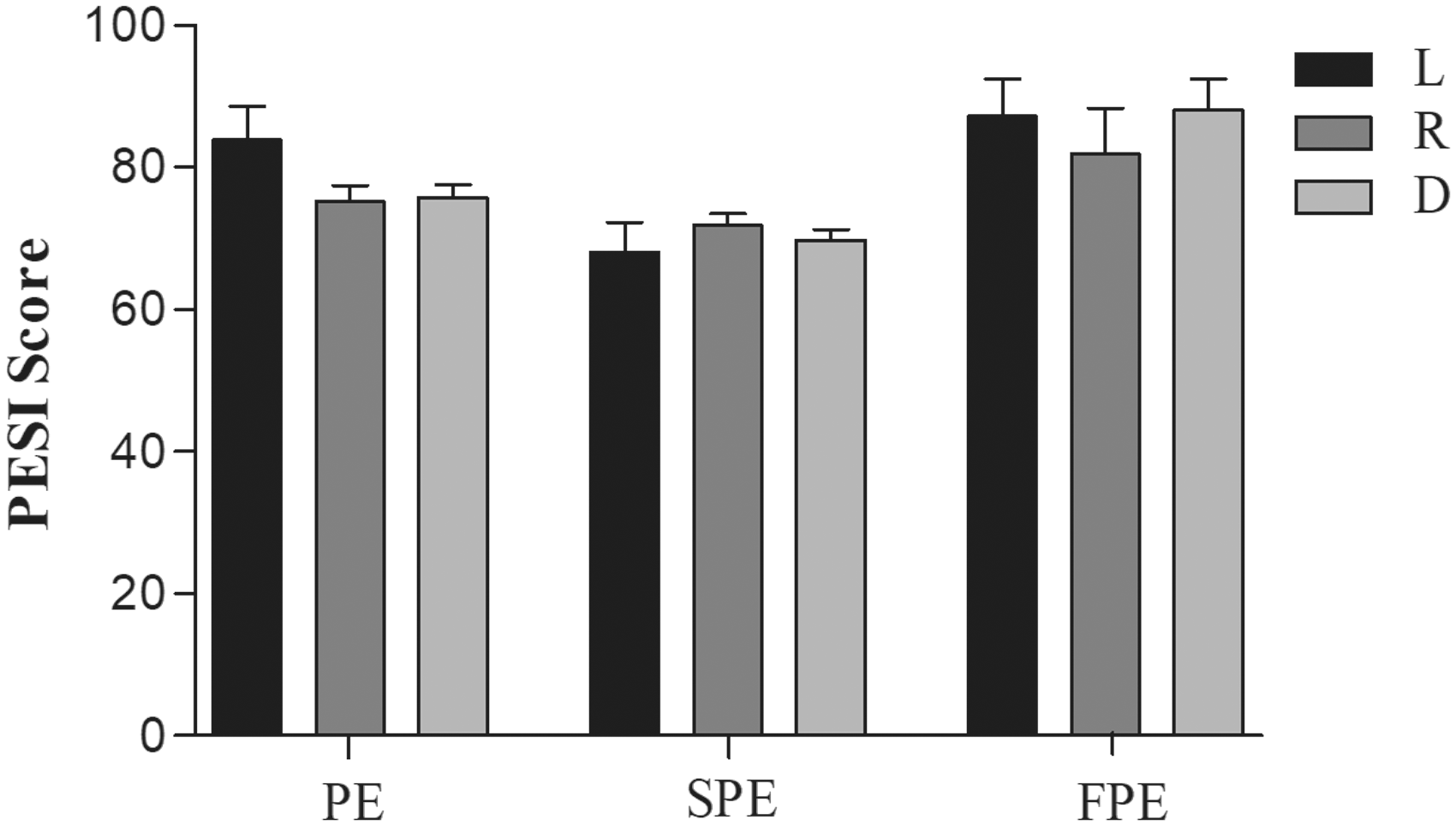
PESI score in different groups.
The ability of various scoring systems to predict PE in patients with DVT
A relative operating characteristic curve was used to analyze the predictable values of Wells score, Revised Geneva score, D-dimer, and age for PE and FPE groups (Table 6, Figure 4). The results showed that the Area Under The Curve (AUC) of PE were: Wells score 0.675 > D-dimer 0.601 > Revised Geneva score 0.595 > age 0.506; Cut-off values were: Wells score 5, D-dimer 7.5, Revised Geneva score 10.5, and the age 52.50. The AUC of FPE were: Wells score 0.722 > Revised Geneva score 0.643 > D-dimer 0.557 > age 0.514; Cut-off value were: Wells score 5, Revised Geneva score 11.5, D-dimer 8.5 and the age 58.50.
Wells and revised Geneva scores in different groups.

NPE: no pulmonary embolism; SPE: silent pulmonary embolism; FPE: featuring pulmonary embolism.
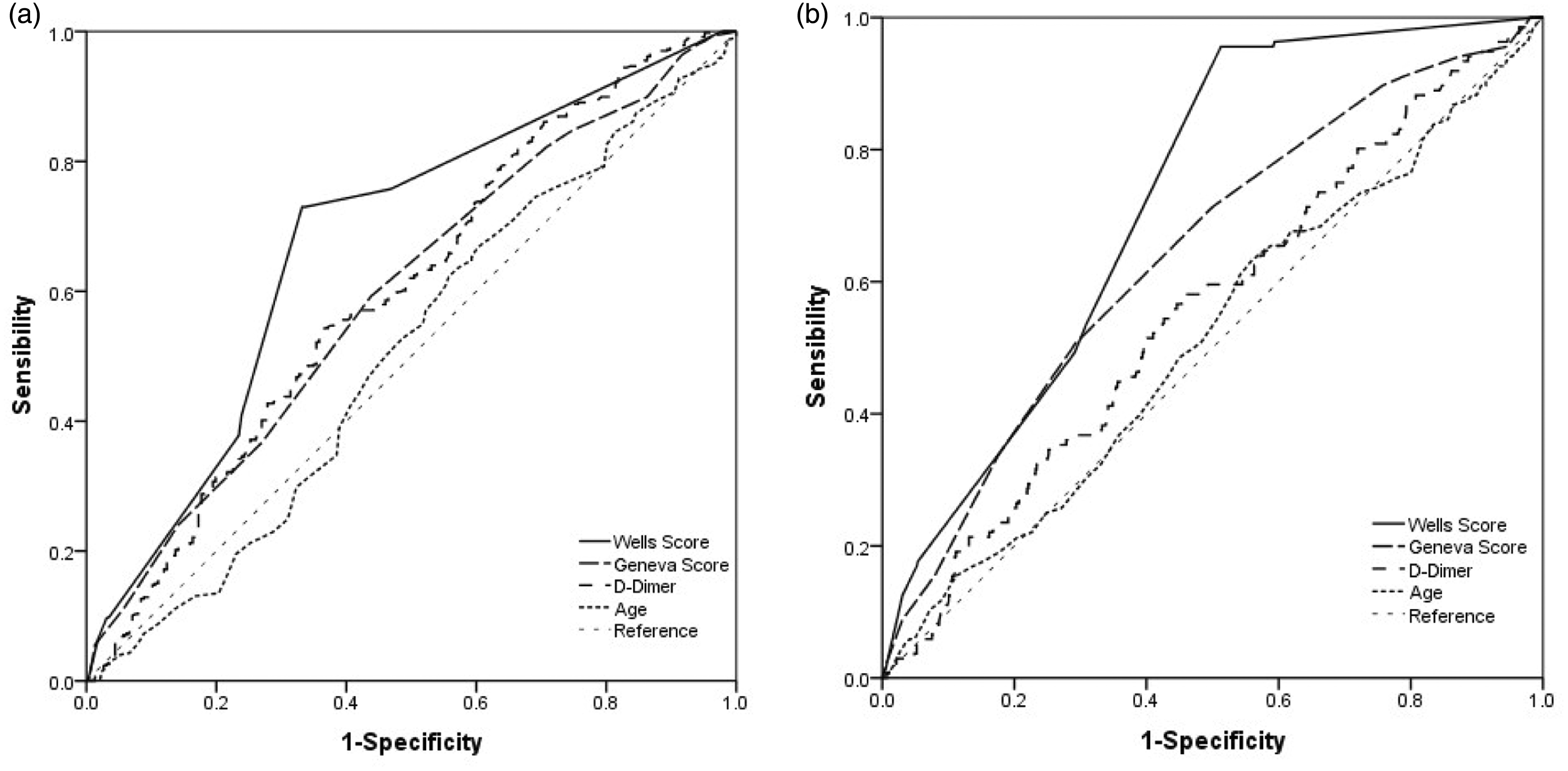
Receiver-operating characteristic curve of PE(a) and FPE(b).
Discussion
VTE, including DVT and PE, causes many cases, and even deaths, every year. It can occur in all races, ages, and genders, and is an important and increasingly serious medical problem. 9 Because PE often lacks a typical clinical manifestations and occurs in the peripheral PAs in most cases, 10 patients can have no clinical symptoms or signs, therefore, it is difficult to make a diagnosis based on clinical manifestations alone. Once misdiagnosed, PE patients have some potentially serious consequences. The three-month all-cause mortality rate of acute PE can reach up to 5.4–17%.11,12 Currently, CTPA is one of the best gold standard tests for the diagnosis of PE, which can clearly display multistage and small branches of PA, further improving the diagnostic accuracy of PE. However, patients with severe renal insufficiency, those with allergies to contrast agents, and pregnant females13,14 should be careful when tested with CTPA. Access limitations of primary hospitals in many developing countries requires long-distance transportation for CTPA examination, which may further aggravate the disease. Therefore, screening DVT patients with a high PE risk by using risk factors or scoring systems can reduce the adverse reactions and socio-economic burdens caused by generalized CTPA examination.
In this study, the clinical features of PE patients caused by DVT were specifically studied. Exclude active bleeding, malignant hypertension and other conditions, all DVT patients received anticoagulant therapy, limb elevation and local immobilization, and PE patients also accepted anticoagulant therapy under the condition of stable respiration and circulation.1,12 692 DVT patients were enrolled where approximately 2/3 (67.34%) were diagnosed with PE by CTPA; the frequency was higher to the data of Prandoni, P. who conducted a study to investigate the prevalence of PE among patients hospitalized for syncope. 15 The ratio of FPE to SPE was 1:2.44, and the overall mortality ratio at 30 days was 0.57%. The ratio of male patients with PE was higher than female patients, and the incidence of PE was associated with DVT locations. Moreover, PE patients with coronary heart disease, COPD, arrhythmia, and other basic diseases were more likely to develop the characteristic clinical symptoms. These results indicated that FPE was more likely to occur in male patients, right unilateral or bilateral DVT patients, and therefore, may require close observation and further examination to determine the presence of PE.
There are few studies on the distribution of PE sites and whether the embolization sites increase the severity of PE, so the relationship between embolism location and severity in PE was focused on in this study. The results showed that PE secondary to DVT occurred more in bilateral PAs, followed by the right side, and then the left side. It was speculated that the cause of this phenomenon might be due to the initiation of coagulation, by shedding procoagulant lipid microparticles, or by impairing blood flow in patients with DVT. It is a process of multiple shedding, and the caducous thrombosis may be randomly drifted to different PAs on both sides. Because of the heart’s location in the left chest cavity, it leads to the anatomical position of the left PA becoming higher than the right PA at the PA bifurcation. When the thrombus detached from a deep vein in the lower extremity and entered the left ventricle from the inferior vena cava, it is more likely to enter the right PA first. Since the right lung is divided into three lobes while the left lung is divided into two lobes, the blood flow in the right lung is higher than that in the left lung. All of the above reasons cause embolism to occur more frequently in the right PA than in the left PA.
The study also showed that FPE occurred more frequently in the upper lobe of the lung, while SPE was mainly in the lower lobe of the lung, which is considered to be related to the anatomy and functional structure of the lung.16,17 Ventilation in the upper lobe of the lung is higher than the lower lobe, and blood flow is lower in the lower lobe, therefore, embolism occurs more frequently in the lower lobes of the lung. When embolism occurs in the upper lobe of the lung, the ventilation function is greatly affected which manifests as dyspnea as well as other clinical symptoms. However, the specific reasons need to be further studied.
PESI is a new tool for PE risk and prognosis assessment, and its effectiveness has been widely verified.17,18 Therefore, PESI was chosen as the tool to evaluate the severity of PE patients in this study. In this research, the FPE group had more distribution at PESI class III–IV. In addition, the study results showed that no significant difference in PESI score was observed whether the PE locations were bilateral or unilateral; this is consistent with the research results conducted by Valle et al. 19 of 269 patients with PE. The result also reflects the severity assessment of PE requires comprehensive consideration of the size, number, location of emboli, and the presence of underlying diseases in the heart, lungs, and other organs.
Due to the variability and complexity of clinical symptoms and signs of PE, clinical diagnosis is still an important issue for clinicians, especially for medical institutions without advanced imaging equipment such as CTPA, or patients with examination risks. Therefore, an effective clinical score for patients suspected of PE is an important basis for PE diagnosis strategy. 19 Currently, the clinical tools commonly used to predict the risk of PE include the Wells score, Revised Geneva score and D-dimer. Although evaluation methods have limitation on diagnosing or excluding PE, the application of these clinical prediction methods can make CTPA examination more targeted.20,21
The Wells score and Revised Geneva score are the most commonly used scoring systems for PE clinical probability, which classifies the probability of PE according to clinical criteria.22–24 Currently, the predictive value of the Wells score and Revised Geneva score systems for inpatient, emergency, or ICU patients is highly controversial.25,26 Research has found that the specificity of the Wells score in predicting PE was lower than the Geneva score, however, the sensitivity was higher.27,28 In this study, ROC curve showed that the Wells score, Revised Geneva score and D-dimer all played certain roles in predicting PE occurrence in patients with DVT, and that the Wells score has a certain advantage.
According to the analysis of the cut off value, when the Wells score was higher than five (5) points, there was a high probability of PE, and the patients should consider further examination (CTPA) to confirm the presence or absence of PE. Therefore, the use of the Wells score system for PE screening in DVT patients can avoid unnecessary advanced imaging techniques to some extent, thereby reducing the economic burden and adverse reactions caused by it. The expected value of D-dimer showed no expected value in this study, which may be related to the lack of age adjustment or because that D-dimer is already increased in patients with DVT.
Limitations and strengths
This was a retrospective and single center study rather than a prospective cohort multicenter study. The study objects were hospital admitted DVT patients due to symptoms of lower limbs, which may have an element of bias. An age adjustment for the predictive value analysis of D-dimer was not carried out. In addition, the treatment status, including anticoagulation, was not analyzed after admission.
Conclusion
A high incidence of PE in DVT patients who have undergone CTPA examination was found. Male patients, patients with coronary heart disease, COPD, right or bilateral DVT, and a previous surgical history are more likely to have PE. In particular, PE occurred in more bilateral PAs than unilateral PA; unilateral PE is more common in the right PA than the left PA. For patients with adverse pulmonary angiography risk, it was valuable to evaluate the possibility of PE in using the Wells score.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the National Natural Science Foundation of China (Grants No. 81071531, No. 81372102) and the Key projects of the Chongqing Municipal Health and Family Planning Commission (Grants No. 2016ZDXM001) for their financial support.
Ethical approval
This is a retrospective and observational study does, not contain any interests and privacy of patients, and for this type of study ethical approval is not required.
Guarantor
DZ.
Contributorship
XiaoYing Chen and Dan Zhang contributed to the concept and design of the research. Xian Liu performed acquisition of patient data. XiaoYing Chen and Xian Liu performed statistical analyses and wrote the manuscript. JingLun Liu and Dan Zhang reviewed the manuscript. XiaoYing Chen and Xian Liu contributed equally to this work and should be considered as co-first authors.