
Abstract
Objectives
The aim of this meta-analysis was to compare compression with no-compression, after radiofrequency endothermal ablation of a truncal varicose vein.
Methods
Databases, such as PubMed, Embase, Cochran Library, and Web of Science, were independently searched by two researchers for relevant literature, preliminary screening was performed, and the full text was read to select studies that met the inclusion criteria. The quality of the included literature was evaluated using the Cochrane Risk of Bias tool, and meta-analysis was performed using Review Manager 5.4.
Results
A total of four randomized controlled trials were included and a total of 552 patients were involved. Among them, 273 patients were in the compression group and 279 in the no-compression group. Meta-analysis results showed that the pain using the 100 mm Visual Analogue Scale was lower in the compression group than the pain in the no-compression group (MD = −4.22, 95% CI = −7.95 − −0.49, p = 0.03). No significant differences in terms of occlusion rate (RR = 0.99, 95% CI = 0.96–1.02, p = 0.55), Aberdeen Varicose Vein Questionnaire (MD = 0.46, 95% CI = −0.80–1.73, p = 0.47), and complications (OR = 1.33, 95% CI = 0.61–2.94, p = 0.47) were observed between groups.
Conclusions
This meta-analysis suggests that compression therapy reduced post-operative pain compared to the no-compression group. However, no additional advantages were observed in terms of occlusion rates, quality of life scores and complications.
Introduction
Varicose veins of the lower extremities are a common manifestation of chronic venous disease with a prevalence of 10–20% in adults. 1 Although rarely life-threatening, they can lead to psychological distress and reduced quality of life. 2 Radiofrequency ablation (RFA) therapy, has revolutionized the modern treatment paradigm for varicose veins and is a common method of endovenous treatment. 3 European and American guidelines recommend RFA as the treatment of choice.4-5 After endovenous RFA treatment, limb compression is commonly applied to reduce the side effects associated with the procedure. The aim of compression therapy is to promote and enhance target vein closure, while reducing petechiae, phlebitis, and possible deep vein thrombosis.6-9 However, recent studies have reported that the use of compression after RFA does not improve success rates, quality of life scores, or patient satisfaction, nor does it improve post-operative complications, or provide additional clinical benefit to patients.10,11 Currently, there is little evidence on the impact of compression on venous ablation outcomes, and the application effect of post-operative compression remains highly uncertain. Given the current uncertainty regarding compression compared with no-compression after RFA, the National Institute for Health and Care Excellence (NICE) guideline development group has advocated further research to assess the clinical and cost effectiveness of this post-operative approach. 4 The aim of this meta-analysis was to compare the efficacy of compression versus no-compression after endovenous radiofrequency ablation and to assess whether compression could provide a benefit to clinical outcomes after endovenous radiofrequency ablation.
Methods
Literature search
The present meta-analysis was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement. 12 Full-text articles published between January 2000 and July 2021 were procured from PubMed, Embase, Cochran Library, and Web of Science. The search terms included: “varicose veins,” “vein varicose,” “veins varicose,” “varix,” “varices,” “radiofrequency ablation,” “ablation radiofrequency,” “ablation radio frequency,” “radio-frequency ablation,” “ablation therapy,” “ablation radio-frequency,” “compression,” “Compression Stocking,” “Stocking Compression,” “Compression Stockings.” No limitations in terms of language of publication were applied. Gray literature was also searched and additional literature was identified from the references cited in selected studies with manual search. Study selection was independently performed by two authors, based on the eligibility criteria. Any disagreements between the two researchers were resolved through discussion.
Eligibility criteria
Inclusion criteria as follows: (1) studies comparing compression and no-compression after RFA, with no restriction on age, gender, race, and nationality of patients; (2) raw data were available for extraction; (3) contained at least one study-relevant outcome indicator. Exclusion criteria as follows: (1) studies with no data available for retrieval; (2) non-raw data; (3) case reports, no full text, small sample studies (n<10), reviews, conference abstracts, animal studies, protocols, and other unrelated studies. No restrictions on publication status, time of publication, and language were imposed.
Outcomes of interest
Primary outcome
Post-operative pain was assessed using the 100 mm Visual Analogue Scale (VAS). 13
Secondary outcome
Secondary outcomes.
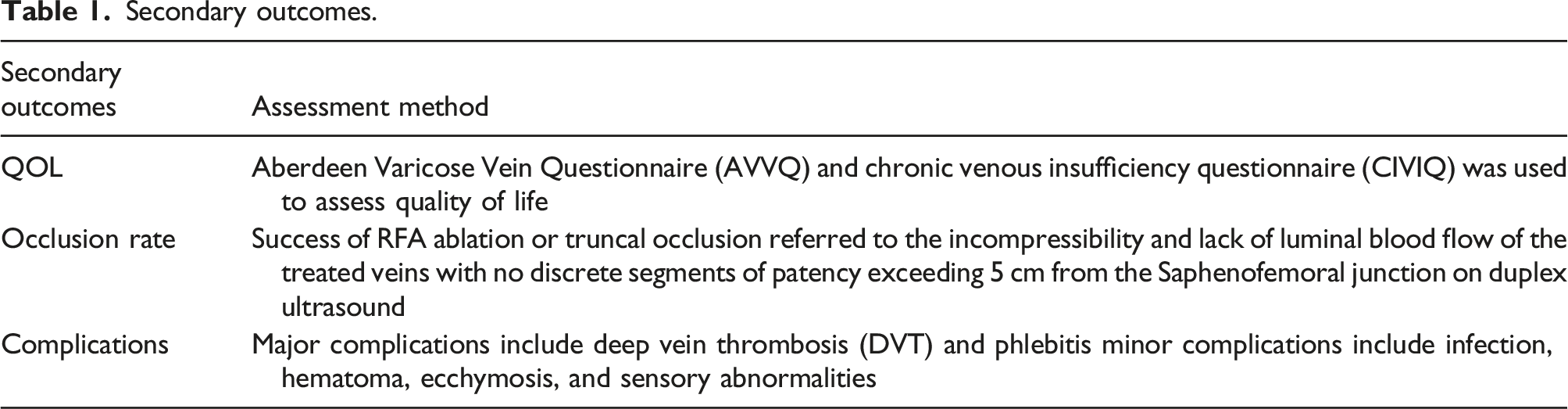
Data extraction and quality assessment
Two researchers performed literature screening data extraction and cross-checking independently by reading the title, abstract, and full text of each study. Included studies were extracted for general information: authors, year of publication, country, study duration, study type, sample size, and follow-up date. The included studies were assessed the included using the Cochrane Risk of Bias tool. 17
Data synthesis
RevMan 5.3 was used to process the data for analysis. The mean difference, relative risk, and 95% confidence interval were used to analyze the statistics for the measurement data and the count data, respectively. The significance cut-off level was set to 0.05 (p < 0.05). Heterogeneity analysis was performed by χ2 test and I2. When I2 < 50%, the fixed-effects model was used to combine effect values; conversely, if I2 > 50%, a random-effects model was used for meta-analysis, and sensitivity analysis was performed to analyze the source of heterogeneity.
Results
Search results
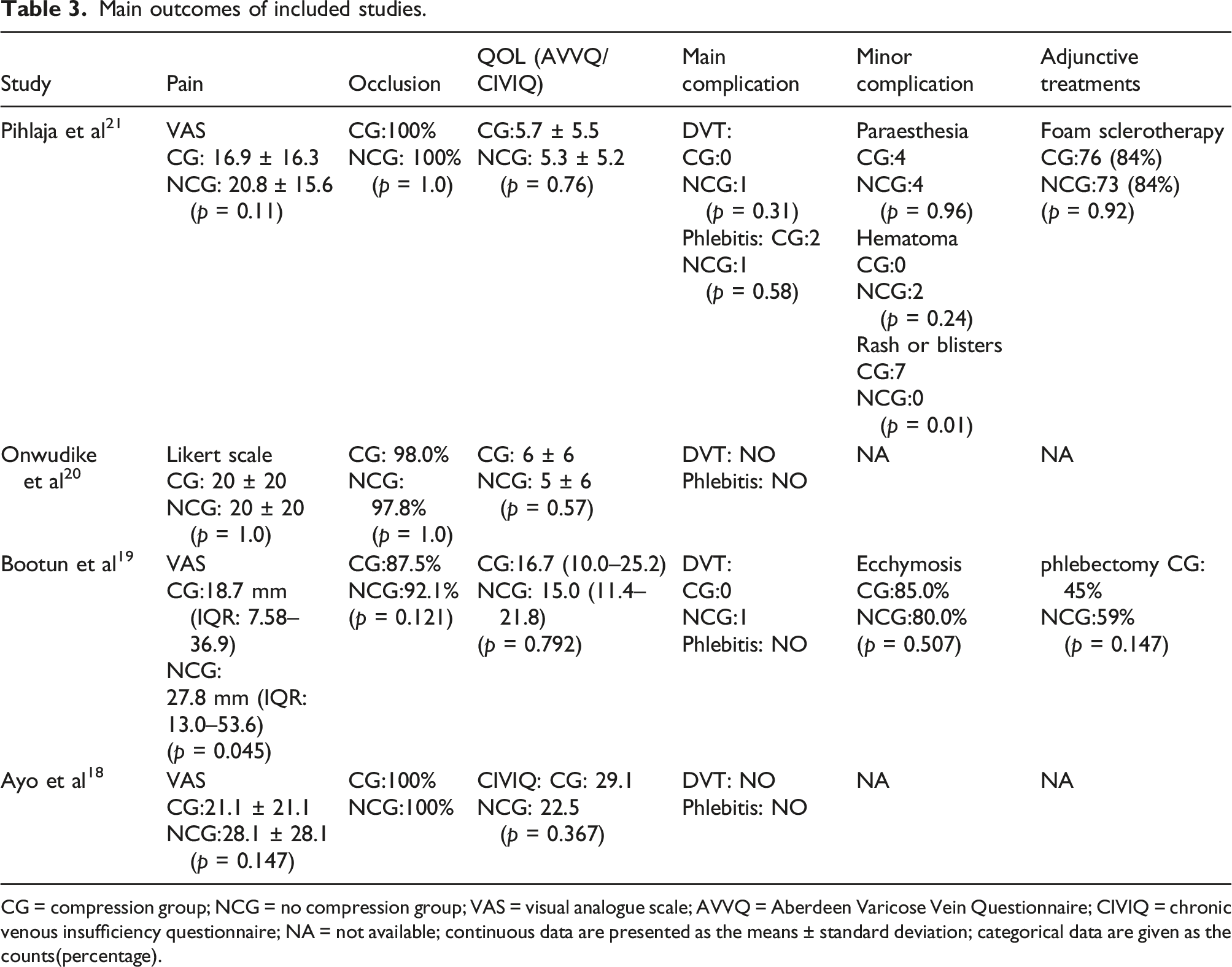
Out of the 581 documents searched, 452 remained after removing duplicates and 432 were excluded by reading the titles and abstracts. By reading the full text, finally four randomized controlled trials (RCTs) were included in this study18,19,20,21(Figure 1). A total of 552 patients were included, 273 in the compression group and 279 in the no-compression group. The basic characteristics and main outcomes of the included literature are shown in Table 2 and 3. Study flow diagram. Characteristics of included studies. CG = compression group; NCG = no compression group; CEAP = Clinical Etiology Anatomy Pathophysiology classification; NA = not available. Main outcomes of included studies. CG = compression group; NCG = no compression group; VAS = visual analogue scale; AVVQ = Aberdeen Varicose Vein Questionnaire; CIVIQ = chronic venous insufficiency questionnaire; NA = not available; continuous data are presented as the means ± standard deviation; categorical data are given as the counts(percentage).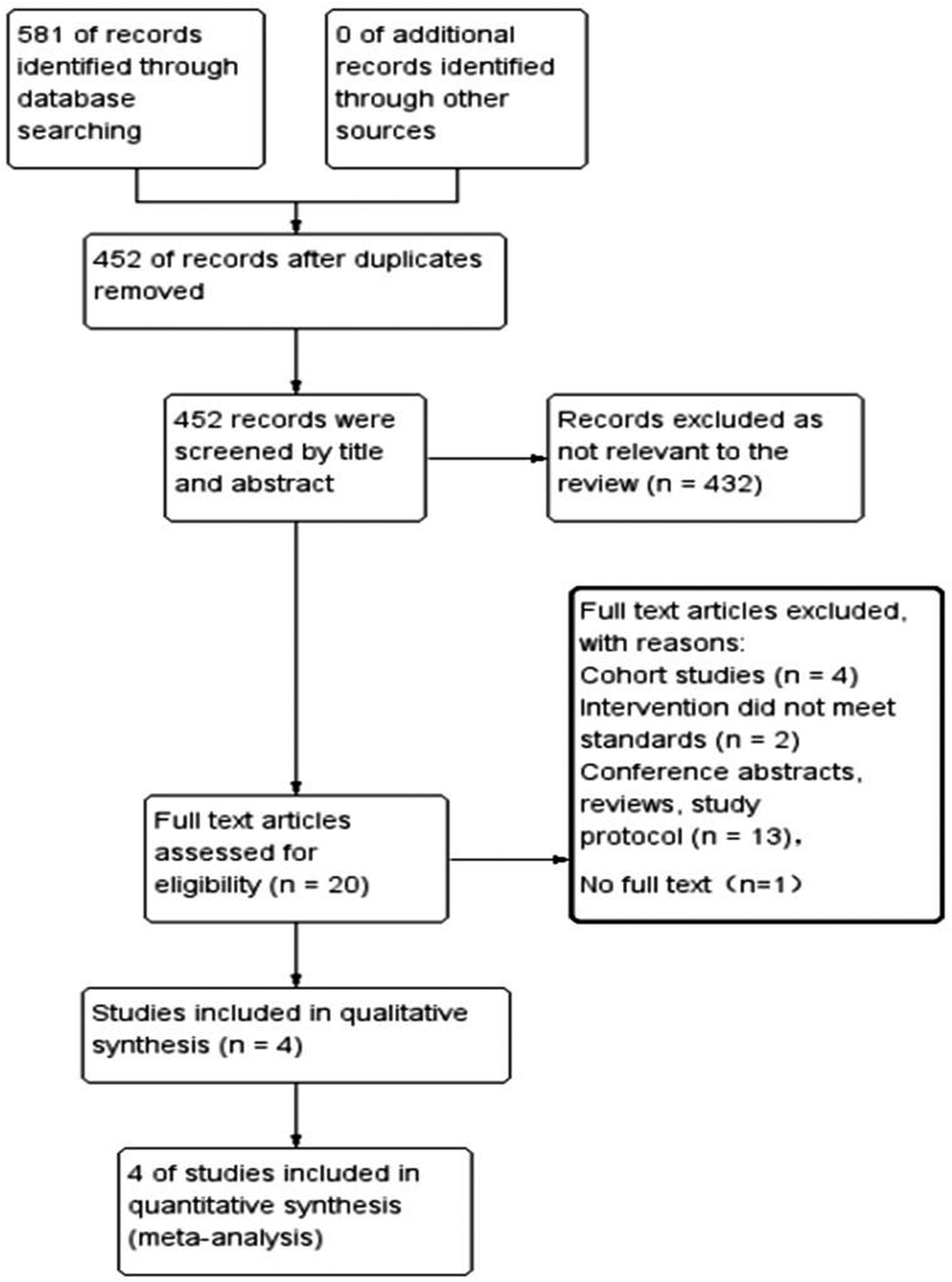

Risk of bias
The results of the Cochrane Risk of Bias Analysis showed that four RCTs ensured a low risk of selection bias. The study by Bootun et al.
19
was considered to be at risk of follow-up bias because some patients were missed during follow-up, resulting in incomplete outcome data. Pihlaja et al.
21
did not report blinding of assessment. Ayo et al.
18
and Bootun et al.
19
did not record analgesic usage after procedure. Onwudike et al.
20
did not prescribe analgesics and patients were advised to take paracetamol as required, but the usage was not recorded (Figure 2). The quality of these four trials. The risk of bias graph and summary.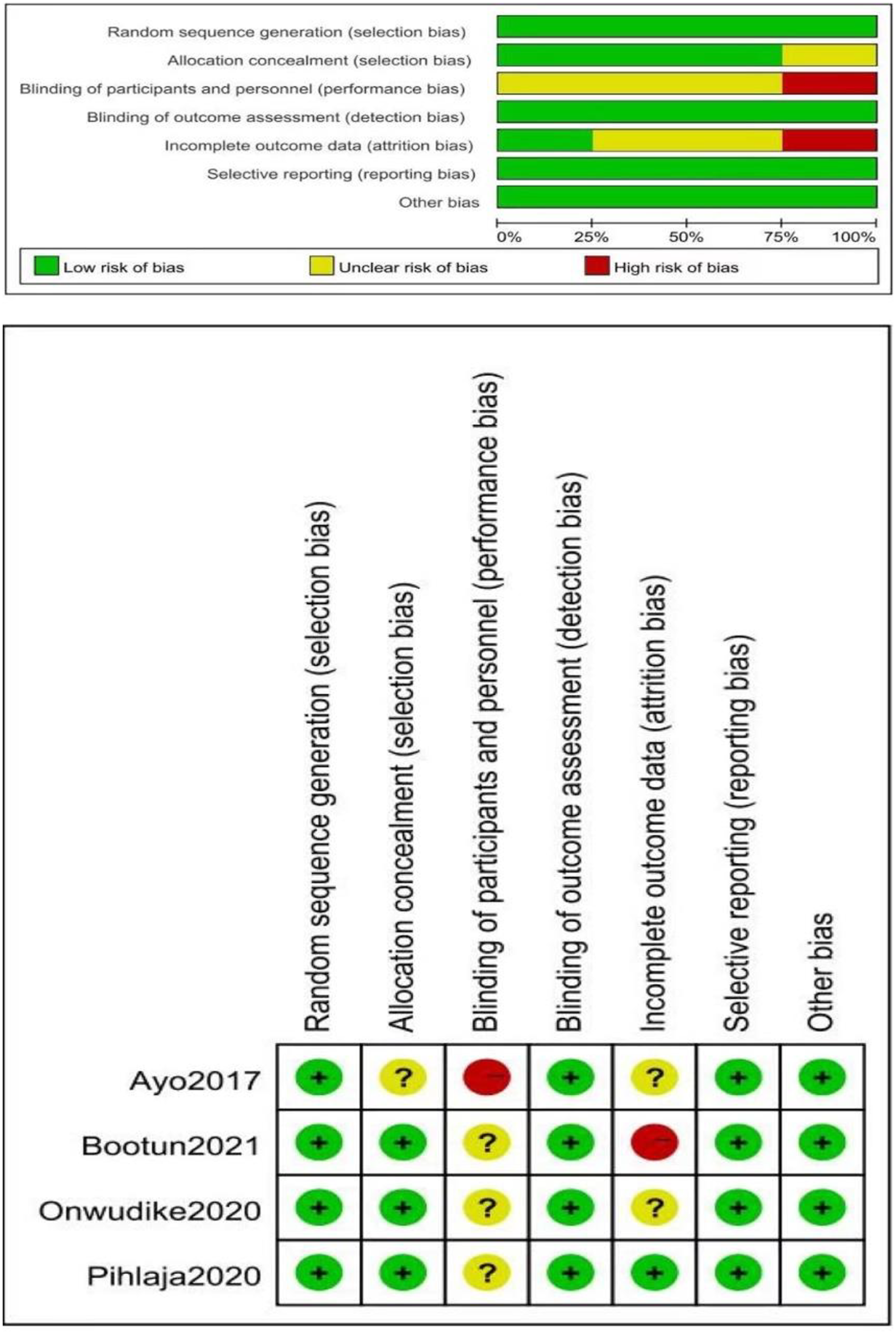
Analysis of study results
Four studies including 560 patients reported on post-operative pain in patients. One RCT could not be pooled because pain was measured by the Likert scale. Using a fixed-effects model, the results showed that compression was associated with lower pain scores than no compression [MD = −4.22, 95% CI (−7.95, −0.49), p = 0.03] (Figure 3). Forrest plot of meta-analysis: the standard mean difference of postoperative pain in studies on patients treated with radiofrequency ablation for varicose veins with or without use of compression after treatment, measured by the visual analogue scale. IV = inverse variance; CI = confidence interval; SD = standard deviation.
The occlusion rate was reported in all four studies and was 96.77% (210/217) and 97.74% (216/221) in the compression and no-compression groups, respectively. Using a fixed-effects model, the combined results of the meta-analysis showed no significant difference in occlusion rates between the compression and no-compression groups [RR = 0.99, 95% CI (0.96, 1.02), p = 0.55] (Figure 4(a)). Forrest plot of meta-analysis: (A) occlusion rate of target vein, (B) Aberdeen varicose veins questionnaire (AVVQ), (C) complications of compression versus no compression. IV = inverse variance; CI = confidence interval; SD = standard deviation; M-H = Mantel-Haenszel.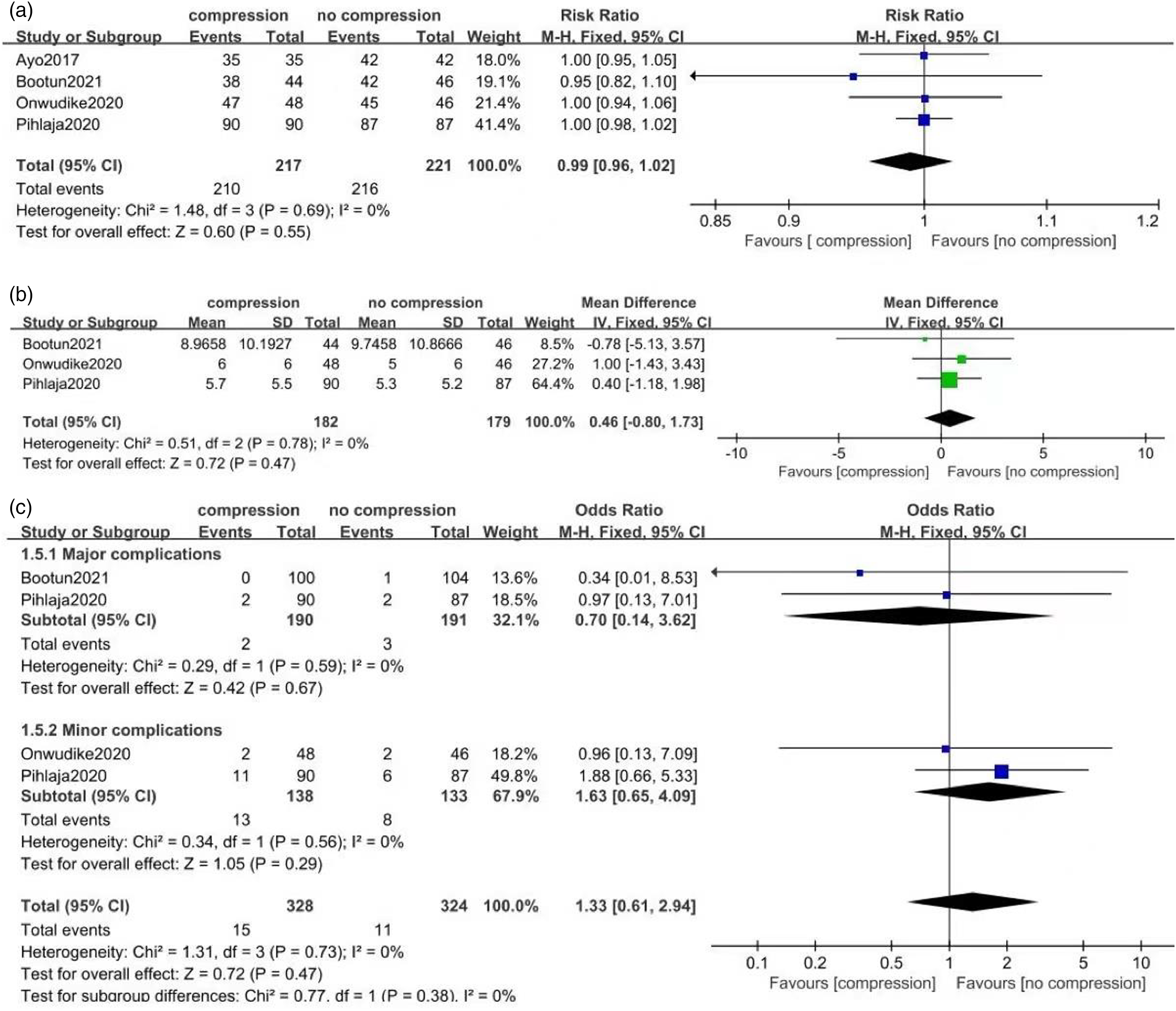
Three studies including 361 patients reported Aberdeen Varicose Vein Questionnaire results. Using a fixed-effects model, the pooled analysis showed no significant difference in Aberdeen Varicose Vein Questionnaire results between the compression and no-compression groups [MD = 0.46, 95% CI (−0.80, 1.73), p = 0.47] (Figure 4(b)).
Major and minor complications were included. The study reported the occurrence of major complications in patients, which were 1.05% (2/190) in the compression group and 1.57% (3/191) in the no-compression group. No significant difference was observed in the incidence of major complications between the compression and no-compression groups [OR = 0.70, 95%CI (0.14, 3.62), p = 0.67]. The incidence rates of minor complications in the compression and no compression were 9.42% (13/138) and 6.01% (8/133), respectively. Additionally, no significant difference was observed in minor complications between the compression and no-compression groups [OR = 1.63, 95%CI (0.65, 4.09), p = 0.29]. This meta-analysis showed that the rate of complications was not significant between the compression and no-compression groups [(OR = 1.33; 95%CI (0.61, 2.94), p = 0.47)] (Figure 4(c)).
Results of sensitivity analysis
Sensitivity analysis was performed by excluding the Bootun et al.
19
study, and the results were similar to the main pooled analysis [MD = −4.42, 95% CI (−8.71, −0.13), p = 0.04] (Figure 5). The difference in pain scores between the compression and no-compression groups was not altered by eliminating the above-mentioned study. Forrest plot of meta-analysis: Sensitivity analysis. IV = inverse variance; CI = confidence interval; SD = standard deviation.
Adjunctive therapy
Other treatments, including foam sclerotherapy and phlebectomy, were also assessed. Although the number of adjunctive therapies reported in the two studies varied, there was no difference between the compression and no-compression groups. The study by Bootun et al. 19 included patients with combined phlebectomies in 45% of the compression group and 59% of the no-compression group. The compression group had considerably reduced median pain levels during the first 7 days. However, overall quality of life was identical across the two groups at 6 months, according to the analysis. Furthermore, the trial by Pihlaja et al. 21 had the highest proportion of patients treated with concurrent foam sclerotherapy, with 84% in each group, but there was no extensive subgroup analysis of these individuals. After excluding the Pihlaja et al. 21 trial, the results of sensitivity analysis for all results remained constant.
Discussion
Radiofrequency techniques have been shown to be effective and safe for the treatment of varicose veins in the lower extremities. 22 Radiofrequency ablation has been demonstrated in previous meta-analyses to be comparable to conventional surgery in terms of efficacy with the added benefit of fewer complications. 23 Compression therapy has been the standard of care based on practice after vein stripping, however, it has never been investigated in the case of RFA. 24 The present meta-analysis based on a comprehensive analysis of included RCTs revealed that compression therapy reduced post-operative pain compared to the no-compression group, but there was no additional advantage in terms of occlusion rates, quality of life scores, and complications.
Pain scores are an important measure that was evaluated in the included studies. The results showed that the pain scores were lower in the compression group than in the no-compression group. Although compression stockings were effective in relieving post-operative pain, the difference between the compression and no-compression groups was relatively small in the VAS and did not appear to be clinically significant. Bootun et al. 19 reported a median pain score of 18.7 mm in the compression group and 27.8 mm in the no-compression group during the first 5 days post-operatively, with a statistically significant difference between the two groups. Concluding that the use of compression during the first 5 days after RFA significantly improved pain scores. However, all patients in this study underwent phlebectomy, and it is possible that this affected their outcomes. Nevertheless, this study suggests that the use of compression may reduce post-operative pain during the first 5 days after varicose vein treatment, regardless of whether phlebectomy was performed. However, this study may lack the power to confirm this conclusion. In addition, six patients in Bootun et al. 19 underwent laser ablation, but the article was included because there was no effect on the results in the sensitivity analysis of the results. Previous reports have shown a reduction in pain in patients who received longer compression after laser ablation.25,26 However, the high temperature generated by laser ablation compared with RFA may also be an important factor affecting the outcome. Krasznai et al. 27 also found no significant difference in pain at 4 h and 72 h post-operatively compared with pain with compression stockings. These findings suggest that compression therapy does not promote better pain control. In addition, the use of paracetamol by patients was reported only in the study by Onwudike et al. 20 in the literature included in the meta-analysis, and the use of analgesics was not clearly documented in the other studies. Therefore, the pain scores reported by patients may not accurately reflect their true pain intensity. In addition, the included studies used the VAS to assess pain, which is a subjective scale that can lead to a risk of bias due to manipulation. Based on the results of this study, we conclude that there was a small advantage in pain in the compression group compared to the no-compression group. However, this result needs to be continuously argued with high-quality evidence.
No statistical difference between the compression and no-compression groups in terms of occlusion rate was detected between the two groups. Chou et al. 28 reported similar results. Onwudike et al. 20 showed that patient age, comorbidities, vein diameter, procedure time, and number of radiofrequency cycles did not affect occlusion. The studies by Elbadawy et al. 29 and Jin et al. 30 reported that factors affecting occlusion may be due to technical issues, such as optimal position of the catheter, effectiveness of anesthetic swelling solution application and limb position. Therefore, the combined analysis of the results of this study showed that the absence of compression did not reduce the rate of occlusion in the target vein.
Three studies reported AVVQ scores and the results of meta-analysis showed no difference in AVVQ scores between the compression and no-compression groups. We conclude that compression did not provide additional benefit in improving AVVQ scores compared to the no-compression group. The studies by El-Sheikh et al. 8 and Chou et al. 28 reported similar results. Based on previous studies, it is commonly believed that compression therapy reduces the occurrence of post-operative complications such as venous thrombosis, extensive petechiae, hematoma, edema, inflammation, or phlebitis.31,32 The results of the three included studies showed no statistically significant differences in major and minor complications between the two groups. In the study by Krasznai et al., 26 there was no significant difference in any single complication between the two study groups at 4 h and 72 h. This is similar to the results. Meta-analysis by Chou et al. 28 also demonstrated similar results. Previous studies have concluded that the associated impact of complications on quality of life or survival is low and that the presence of complications is generally resolved with symptomatic management.33,34 Combined with the results analyzed in this study, it is postulated that compression after RFA may be an unnecessary additional treatment, but there was no large sample or multi-center data comparing the significant differences between the two groups. Therefore, close and rigorous follow-up is needed in the clinic for patients without compression.
This study also has limitations. First, there are few randomized controlled trials on compression or no-compression after RFA, and therefore fewer studies were included. Second, among the included studies, varying degrees of bias were present, no high-quality evidence was found and publication bias could not be performed due to the low number of included literature studies. Third, there were differences in follow-up time between studies, which may impact the results. Furthermore, differences in additional treatment measures, and although studies reported the results of subgroup analyses with concurrent additional treatment measures, fewer studies combined analyses of different additional treatment measures. Finally, adherence to compression was not measured in papers included in the meta-analysis.
Conclusion
This study showed that the compression group reduced post-operative pain compared to the no-compression group, but no additional advantage was observed in terms of occlusion rates, quality of life scores, and complications. Further high-quality randomized controlled trials are still required for the validation of these results.
Supplemental Material
Supplemental Material - Compression versus no compression after endovenous radiofrequency ablation: A meta-analysis of randomized controlled trials
Supplemental Material for Compression versus no compression after endovenous radiofrequency ablation: A meta-analysis of randomized controlled trials by Dengxiao Zhang, Chaohai Shi, Yuan Zhang, Qi Cui, Shaobo Zhai, Yalong Huang, Cong Zhou and Quan Chen in Phlebology: The Journal of Venous Disease
Footnotes
Acknowledgements
We would like to thank all the researchers and study participants for their contributions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was financially supported by Open Fund of Gansu Provincial Key Laboratory of Molecular Diagnosis and Precision Therapy of Surgical Tumors (18JR2RA033).
Ethical approval
This manuscript is not reported studies involving human participants, human data, or human tissue. So, the “ethics approval” is not appropriate for our manuscript.
Guarantor
CQ.
Contributorship
CQ conceived and designed this study. ZD and ZY were responsible for the collection, extraction, and analysis of the data. ZD was responsible for writing the paper. ZC, ZS, and CQ performed the quality evaluation and completed data analysis. SC and HY polished the English language. All authors and participants reviewed the paper and reached an agreement to approve the final manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.