
Abstract
Background
Elective eradication of superficial vein incompetence (SVI) is advocated after superficial vein thrombosis (SVT) to prevent venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), and to prevent recurrent SVT. However, this practice currently lacks evidence and not all SVT patients are referred.
Method
Pilot study based on retrospective review of medical records for patients in Örebro county, Sweden; diagnosed with SVT during 2019. Patients in primary care without venous intervention were compared with patients from a vascular service treated with eradication for SVI, regarding prevalence of VTE and recurrent SVT during one-year follow-up.
Results
Out of 236 records reviewed, 97(41%) were included, 44 in the vascular care, and 53 in primary care. Erroneous diagnosis and coding were common causes for exclusion. The groups differed in ultrasound verified SVT 25(47.2%) and 35(79.5%) (p = .001), LMWH treatment 13(24.5%) and 24(54.5%) (p = .002), and history of prior SVT 19(35.8%) and 31(70.5%) (p = .001).
There was no difference in the incidence of VTE during follow-up, 1(1.9%) and 1(2.3%) (p = 1.000), or recurrent SVT, 7(13.2%) and 6(13.6%), respectively (p = .951).
Conclusions
This pilot study cannot confirm if elective eradication of SVI after SVT reduces the risk of VTE and recurrent SVT, however, the incidence of VTE was low in both groups. Limitations of the study are the small sample size and the lack of duplex ultrasound in all cases in both groups at diagnosis and at follow-up. Further prospective studies on homogenous populations are needed.
Keywords
Introduction
Superficial vein thrombosis (SVT) in the lower extremities, often called thrombophlebitis, is a condition of acute inflammation and thrombosis of a superficial vein, most commonly occurring in varicose veins (VV). Superficial vein thrombosis was previously seen as benign and self-limiting, but studies show a correlation with an increased risk of venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE).1–4 According to the European Society for Vascular Surgery (ESVS) guidelines on management of venous thrombosis, duplex ultrasound (DUS) examination is therefore recommended in ambiguous cases, where the SVT is more than 5 cm in length and in situations where DVT cannot be ruled out. 5
Evidence for treatment of SVT is currently inconclusive, especially regarding prevention of VTE. Options for the acute phase include topical anti-inflammatory treatment and anti-inflammatory drugs for distal SVT with extension less than 5 cm, low molecular weight heparins (LMWH) or anticoagulants is recommended if the SVT is more extended, close to junctions with deep veins, affecting the GSV and SSV or if the general risk for thrombosis is increased . 2 In a later stage, ablation or removal of the affected veins is also possible.2,6 Referral to specialized care in vascular surgery for assessment and possible elective eradication of superficial vein incompetence(SVI) is commonly practiced, with the aim to reduce the risk of recurrent SVT and the risk of VTE, however, this practice is currently not evidence based. 2 Due to scarring and thickening of the veins, it may also be more difficult to perform, with increased risk of complications and residual VV afterwards. 7
During assessment of diagnostic codes used for SVT in the county of Örebro, it was discovered that only a minority of all SVT cases were referred from primary care to a vascular service, thus it was possible to compare patients undergoing eradication of superficial vein incompetence (SVI) with patients treated in primary care only.
The aim of this study was to compare patients diagnosed with SVT in primary care, who were not referred to a vascular service, with those referred and treated with eradication of SVI, regarding demographics and the prevalence of VTE and recurrent SVT during one year of follow-up.
Methods
Design and study population
This was a retrospective cohort study based on review of medical records for consecutive patients over 18 years of age diagnosed with SVT in the county of Örebro in Sweden during 2019. The first group was non-referred patients who were identified in primary care, five urban and three rural areas where selected representing a population of approximately 100 000 inhabitants. The second group consisted of patients treated with eradication of SVI in a vascular service due to a recent SVT.
The venous interventions were performed at Karlskoga Vein Centre, where all treatments of SVI are performed in the county of Örebro, and no earlier than three months after SVT. All patients in the vein center were examined with DUS by an experienced vascular surgeon, including deep and superficial veins, and the examination was repeated prior to intervention. As a routine complete ablation of venous incompetence was aimed for, that is, endovenous ablation of saphenous trunks and larger tributaries, and phlebectomies or sclerotherapy of varicose tributaries. Postoperative LMWH treatment was given only if risk factors were present such as old age, obesity, previous DVT, prior SVT, or previous SVT close to deep veins.
Several ICD-10 codes could potentially be used for the SVT diagnosis, and in order not to miss cases as some patients may have erroneously been diagnosed with DVT, a broad search was made including ICD-10 codes I80.0-9 and I83.1-2, and an additional sample of codes specific for primary care. For the same reason, diagnostic codes for DVT for the included patients were searched in medical records from the emergency wards.
Inclusion criteria and patient characteristics
The SVT and SVI diagnosis were evaluated and confirmed from the description in the medical records, either from typical clinical signs described in the text or from documented DUS findings. Typical clinical signs were painful tender lumps or cords with increased heat and redness in areas following saphenous or varicose veins. The study only included SVT in the lower extremities with VV.
Patients were not included in the study if they had a previous intervention for VV the year preceding the SVT diagnosis, as the intervention per se may cause tender lumps or postoperative SVT and DVT.
Gender, age, history of repeated SVT, medical treatment for the SVT, clinical description, DUS findings, and anticoagulant treatment for other reasons than SVT were recorded for the included patients. The following risk factors for DVT and PE were also noted; previous DVT or PE, Covid-19, BMI, estrogen therapy, and active malignancy.
One-year follow-up and outcome
Medical records for both cohorts were reviewed for a one-year period regarding events of VTE, recurrent SVT, and postoperative complications. Medical records for emergency care were also included in order not to miss events unknown to primary care or the vein center. For the primary care cohort, the start of this timespan was the date of described SVT diagnosis as this was the starting point for a treatment strategy without intervention, and for the vascular cohort the date of the eradication of SVI as this was the start of a treatment strategy with intervention.
The main outcomes were the incidence of VTE and recurrent SVT during follow-up, and a secondary outcome was complication rates after venous intervention.
Statistical analysis
IBM SPSS statistics 26 was used for all statistical calculations.
The cohorts were compared for outcomes during follow-up using asymptotic Pearson’s Chi-Square or Fisher exact test, with a significance level at 0.05. The null hypothesis was that there was not a difference in the incidence of VTE and recurrent SVT in patients treated in primary care only versus the surgically managed group at one year.
A power analysis was not performed as the incidence of SVT in primary care was not known.
Ethical considerations
Ethical approval was granted from the Swedish Ethical Review Authority with the following reference number; 2020-06908 and the study was carried out in accordance with European GDPR laws.
Results
Potential patients with SVT and the selection process
Inclusion to the primary care and the vascular service cohort
Hundred possible patients with SVT were identified in primary care of which 53 were included and 136 in the vascular service where 44 were included. The use of possible codes varied substantially between institutions and unspecific coding was common where the code could be used for more than one diagnosis.
Cause for exclusion and ICD-codes for the excluded patients
A total of 47 patients were excluded from the primary care. The most common cause for exclusion was erroneous diagnosis and coding with 27 excluded, in order from most common to least common; ruptured baker cyst diagnosed with ultrasound, erysipelas later treated with antibiotics, hematoma related to trauma, lump described with no pain or sign of inflammation, no clinical signs associated with SVT as basis for diagnosis, sarcoidosis, and lymphoma. The remainder were excluded due to unspecific coding or lack of information in the medical records or DUS to confirm the SVT diagnosis.
Ninety-two patients at the vascular service were excluded, the most common cause, 65 patients, was the use of unspecific ICD-codes, mainly I83.1 (varicose veins of lower extremities with inflammation), which could be interpreted as inflammation of skin or VV. Two patients were excluded due to erroneous diagnosis, two due to lack of information in medical records or DUS, and one due to planned extensive open surgery with another main indication. The remainder were excluded due to postponed or cancelled interventions or no intervention planned, and postoperative inflammation of treated veins coded as SVT.
Diagnosis and ICD-codes used for the included patients
ICD-codes for the included patients.
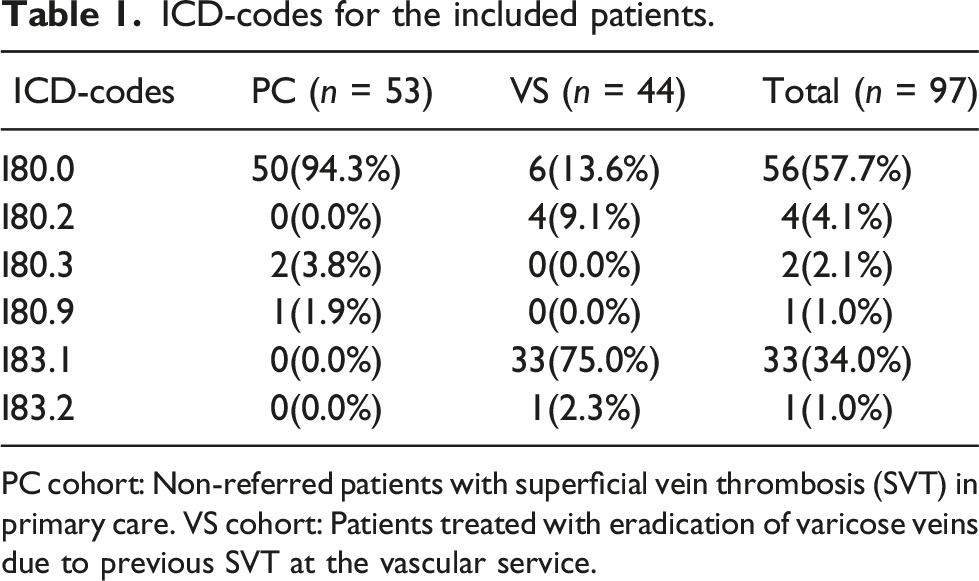
PC cohort: Non-referred patients with superficial vein thrombosis (SVT) in primary care. VS cohort: Patients treated with eradication of varicose veins due to previous SVT at the vascular service.
I80.0 Phlebitis and thrombophlebitis of superficial vessels of lower extremities, I80.2 Phlebitis and thrombophlebitis of other and unspecified deep vessels of lower extremities, I80.3 Phlebitis and thrombophlebitis of lower extremities, unspecified, I80.9 Phlebitis and thrombophlebitis of unspecified site, I83.1 Varicose veins of lower extremities with inflammation, I83.2 Varicose veins of lower extremities with both ulcer and inflammation.
Primary care vs vascular service
Demographics of the cohorts and study population
Patient demographics.

PC cohort: Non-referred patients with superficial vein thrombosis (SVT) in primary care. VS cohort: Patients treated with eradication of varicose veins due to previous SVT at the vascular service.
SVT: Superficial vein thrombosis, LMWH: Low-molecular weight heparins, NOAC: Non-vitamin K oral anticoagulants, DVT: Deep vein thrombosis, PE: Pulmonary embolism. Prior SVT: Previous history of more than one SVT diagnosed at different occasions.
Asymptotic Pearson’s Chi-square and Fisher exact test were appropriate.
It was not possible to determine the extent of the SVT in many cases due to missing information in the clinical description or DUS protocol. Body mass index was only recorded in 26 cases of which 15 were overweight (>25), 9 (17.0%) in primary care and 6 (13.6%) at the vascular service.
In 47.2% of the patients in primary care and in 79.5% at the vascular service, the SVT diagnosis was confirmed by DUS. However, all patients at the vascular service were examined with DUS by routine, but signs of SVT were not always specifically stated in the surgeons’ description of the DUS findings, thus the missing 20.5% are such cases where history of SVT is described as an indication for eradication of SVI without specific description of such DUS findings.
DVT/PE and recurring SVT during follow-up
Outcome during one-year follow-up.

PC cohort: Non-referred patients with superficial vein thrombosis (SVT) in primary care. VS cohort: Patients treated with eradication of varicose veins due to previous SVT at the vascular service.
SVT: Superficial vein thrombosis, VTE: Venous thromboembolism, DVT: Deep vein thrombosis, PE: Pulmonary embolism.
Asymptotic Pearson’s Chi-Square for Recurrent SVT and Fisher exact test for VTE.
Description of the two VTE cases
One patient in the primary care cohort with an SVT located in the small saphenous confirmed with DUS and not treated with anticoagulants was diagnosed with a DVT in the popliteal vein one month later when symptoms changed from localized inflammation to swelling of the lower leg. There was no new SVT during the one-year follow-up. No previous risk factors for VTE were known and no history of previous prior SVT.
In the vascular service, one patient had a PE 11 months after VV intervention, no risk factors were known nor any previous history of prior SVT.
Perioperative complications and incomplete eradication of SVI
Two patients had inflammation along the treated vein during the first month after surgery. In some cases, surgical records described difficulties to pass catheters through scarred veins and also to perform phlebectomies. Eleven patients in the vascular service had incomplete eradication of SVI, nine of these residual VV of which 7 underwent repeated intervention, and two other patients had recanalization of the trunk veins and were treated again. Two of the patients with recurrent SVT had incomplete eradication of SVI.
Discussion
This retrospective study showed that patients with previous SVT who were treated with elective VV removal had equally low prevalence of VTE during one-year follow-up than patients with SVT who were not referred from primary care. Erroneous coding and diagnosis were common, many of the patients diagnosed with SVT in primary care were poorly described in the medical records, not examined with DUS and not treated with anticoagulants, but still the prevalence of VTE was surprisingly low in both groups. This may be interpreted as a true benefit of venous intervention if the right patients were selected for referral, or as no benefit if the groups were comparable. The study cannot answer this as the majority of the patients were not examined with DUS and examining every SVT patient with DUS is not recommended in current guidelines. 2
The role of elective superficial venous intervention after SVT has been scarcely studied, but in spite of low evidence it is commonly recommended, and previous SVT is often seen as a true medical indication for treatment of VV without skin changes that would otherwise not be reimbursed. The rationale is to remove the source and starting point for a thromboembolic process, however, it is not known how important the local pathology is, some SVT occur synchronously with DVT even in the contralateral limb and thus possibly reflects a systemic prothrombotic state. 8
In this study, the incidence of VTE after SVT was low, 2.1%, but the number of included patients was small in comparison with other studies. The incidence differs between studies, including those referred to in the ESVS guidelines, with recurrent SVT between 6.2 and 22.6% and DVT at 1.5–6.2% during the first three months.2,9–12 Some reasons for the differing figures may be selection bias, that is, if patients are examined in primary or specialized care, if patients without VV are included, and also if the SVT diagnosis has been confirmed with DUS. Our study used a follow-up timespan of one year compared to three months in other studies.2,3,13 The risk for VTE has been shown in other studies to be highest during the first 90 days, thus it may not affect the results to a large degree. 14 In a systematic review, including 21 studies and 4358 patients, synchronous DVT at the time of SVT diagnosis was 18.1% and PE 6.9% compared to one synchronous case in this study. 4
This was a retrospective study of clinical practice and thus has its limitations. As presented in Table 2, the vascular service had a higher number of patients treated with LMWH, more patients with a history of prior SVT and a to a larger extent the SVT diagnosis was verified by DUS, thus the vascular patients may have had a higher incidence of VTE and SVT had they not been treated. One of the ambitions of this study was to consider the severity of the SVT in the comparison, but due to lacking description of the size in the medical records, this was not possible. This in turn may reflect the busy life of general practitioners, where a tender lump in the lower leg is not described in detail, and also at the vascular service where duplex findings may be documented in a very concentrated form. There is also the question about the validity of the SVT diagnosis since around half of the cases from primary care were not verified by DUS. However, according to local and international guidelines, this is not recommended, clinical diagnosis is deemed as accurate if the SVT is smaller than 5 cm, located to the lower leg and with no suspicion of DVT. Examining all patients with temporary tender lumps in their lower legs with DUS would require considerable resources.
In spite of these limitations, this study provides data about the common practice of eradication of SVI after SVT, and to the best of our knowledge this has not been studied before. Furthermore, the prevalence of VTE after SVT in the group of non-referred patients in primary care was surprisingly low despite deficiencies in diagnostics and treatment. Current practice of only referring selected patients for VV intervention may thus be adequate and safe in clinical practice, and also the adherence to guidelines such as the ESVS where further investigations with DUS is not considered mandatory if the SVT is limited. However, more studies are needed about this subject including risk stratification in patient selection for referral to vascular service.
When studying the benefit of eradication of SVI, the rate of complications is also important, however, in our study these were few and of minor severity. Some of the patients from the vascular service had repeat intervention, due to residual VV. This can be expected to some extent since venous procedures may be more difficult to perform after SVT. 7
Eradication of SVI is mainly indicated for other reasons than the risk of VTE, that is, relief of symptoms and prevention and healing of venous ulcers, however, the effect on quality of life was not studied here.
Conclusion
This study cannot confirm if elective eradication of SVI after SVT reduces the risk of VTE and recurrent SVT, however, the incidence of VTE was low in both groups. Limitations of the study are the small sample size, which is probably lacking power, and the lack of DUS in both groups at diagnosis and at follow-up. Prospective randomized studies on homogenous populations are needed, including risk stratification in patient selection for referral to vascular service.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Skandinavian Research Foundation for Varicose Veins and other Venous Diseases 2021.
Guarantor
LB
Contributorship
LB conceived the project, HÅ and LB designed the project, collected, analyzed the data and wrote the article.