
Abstract
In the medical field, ultrasound is commonly used for diagnostic imaging due to its ability to provide real-time images. However, High-Intensity Focused Ultrasound (HIFU) is also used for other clinical purposes, such as thermal tissue ablation. In the case of varicose veins, the potential role and benefits of HIFU have been known for a long time despite in-vivo results have mostly been preliminary and experimental, particularly regarding its effect on venous wall. The aim of this brief report is to describe how HIFU acts on venous wall in human incompetent great saphenous veins.
Introduction
High Intensity Focused Ultrasound (HIFU), also known as echotherapy, offers a unique solution that combines therapeutic ultrasound with ultrasound monitoring. This innovative approach involves directing a highly focused beam of high-intensity ultrasound onto a vein, like using a magnifying glass. 1 By delivering controlled thermal energy, the ultrasound causes the vein wall to undergo a thermal damage resulting in shrinkage, collapse or obliteration. This procedure creates a fibrotic seal, leading to the closure of the vessel and/or significant reduction in size. The use of this particular “outer-body” thermal technique can be used to achieve veins occlusion but also has the potential to restore their normal function and provide beneficial hemodynamic effects through shrinkage.
Despite the key effects on vein wall seem to be similar to those seen after other conventional endovenous techniques (e.g., laser, radiofrequency, or sclerotherapy), these findings have been obtained through in vitro or animal studies.2,3 Moreover, there are some clinical and ultrasound findings that change during days/months after treatment, with progressive wall remodelling leading to therapeutical shrinkage. 4 Aim of this report is to describe HIFU effects on incompetent great saphenous vein (GSV) wall at different postoperative follow-up times.
Methods
Four patients (all female, aged 41 ± 11 years, all with varicose vein disease and GSV incompetence [CEAP C2]) and candidate to GSV stripping and phlebectomies, underwent segmental GSV HIFU (Sonovein® HD [Theraclion, Malakoff, France]) for research purpose before the intervention, using the Authors’ group validated protocol. 4 According to preoperative Duplex scan examination performed in orthostatic position, all GSV were incompetent from the terminal valve to varicose veins origin, with a diameter more than 6 mm. A 3-cm GSV segment was explanted at 24-h, 7-days, 1-month, and 4-months follow-up after HIFU, at the same GSV stripping time.
The surgical specimens were fixed in 4% buffered formalin and sent to the histopathology laboratory, according to Barnat et al. 3 ; they were described macroscopically and sampled with a transverse section and a longitudinal sample of the vessel. The specimens thus oriented were processed with the standard technique which includes progressive dehydration in an ascending scale of ethyl alcohol to xylol clarification and the subsequent embedding in paraffin melted at 60°C. Five micrometres’ sections of the paraffin block were obtained and placed on glass slides and stained with Hematoxylin-Eosin. All patients sign an informed consent. The study was carried out according to the declaration of Helsinki. Regional Ethic Committee provided communication of receipt and resolution for case series (n. 39779).
Results
All specimens (5 for each follow-up time) were analysed.
24-h follow up
It’s possible to see the first change as adventitia oedema and haemorrhagic spots inside the media, while the endothelium appears normal (Figure 1(a)). Asterisks indicate vein lumen. (a), (24 h) The venous wall shows adventitial oedema and micro hemorrhagic spots (arrows); (b), (1 week) The venous vessel wall shows evident adventitial oedema, enhanced haemorrhagic reaction, and practically intact intima (Haematoxylin-Eosin); (c), (1 month) hyalinization is more evident and the acellular substance separates the smooth muscle cells of the vascular wall (Haematoxylin-Eosin); (d), (4 months) Complete obliteration of the venous vessel (the lumen is reduced to a thin fissure marked by the overlaid endothelium of the two faces) and complete fibrosis of the vessel wall and perivenous tissue (Haematoxylin-Eosin).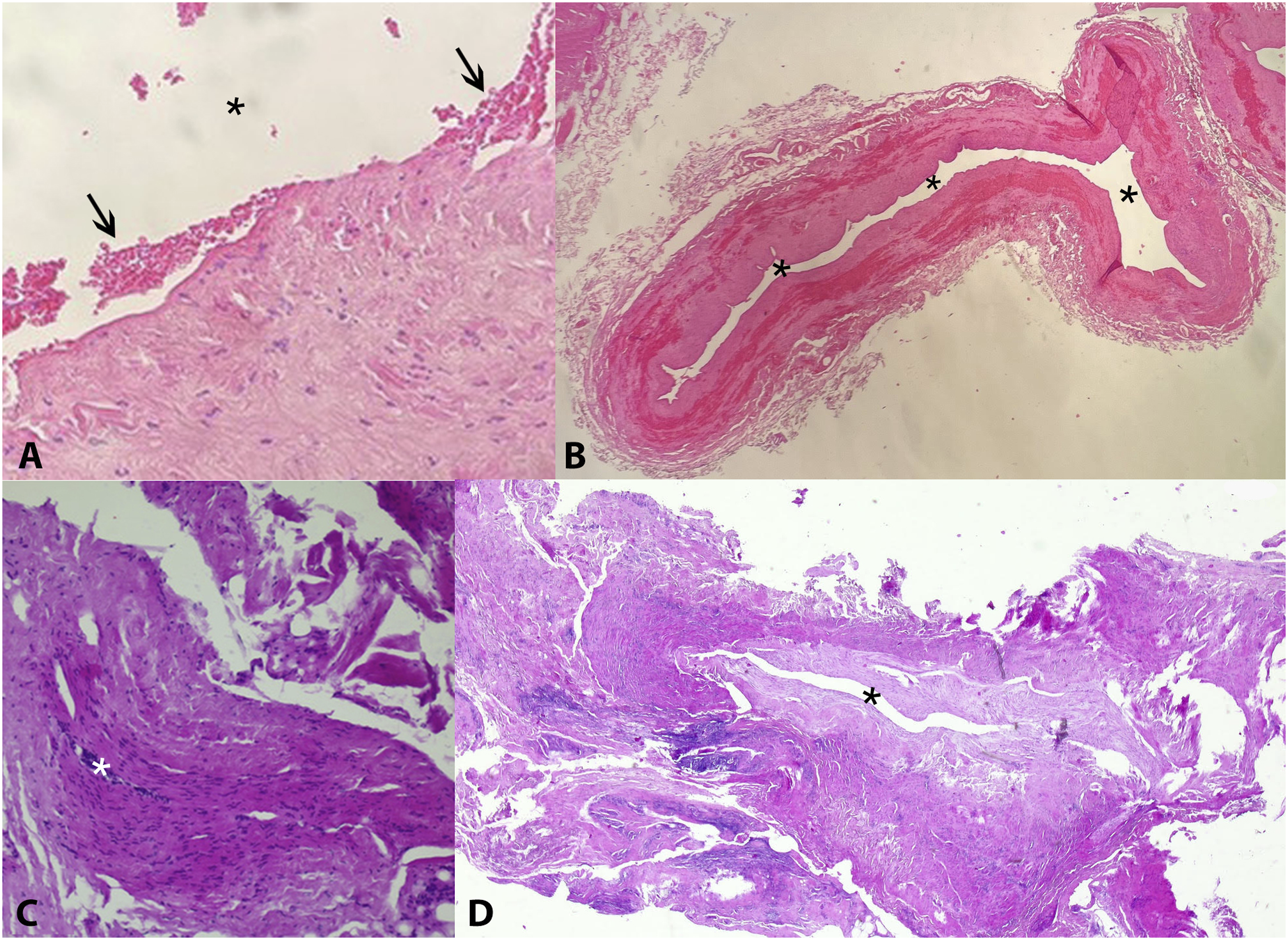
Seven-day follow-up
The haemorrhagic spots in the tunica media are more evident with muscular cells degeneration (partial haemorrhagic necrosis). Adventitia oedema is still present and the intima with few changes (Figure 1(b)).
One-month follow up
This pattern is enhanced with the Hyaline substance that replace in most of the samples the media and the intima, the first step to fibrosis degeneration. Now the lumen is virtual (Figure 1(c)).
Four-month follow-up
Complete hyalinosis of media, intima and total wall remodelling with mild or absent inflammation. Extensive steatophagic changes surrounding the vein with fibroblasts and fibrosis (Figure 1(d)).
Discussion
This concise and pivotal paper presents histological observations regarding alterations in the GSV wall after HIFU treatment and it is the first report describing these microscopical findings in humans.
By subjecting the target vein wall to focused thermal stress, HIFU reaches temperatures as high as 90°C, inducing localized coagulative necrosis. This process subsequently triggers a progressive hyalinosis and hyperplasia within the tunica media, accompanied by myocyte degradation, steatophagic reaction, as well as inflammation of the adventitia and local peri-venous fat tissue, resulting in a progressive and ongoing fibrous healing. Present results confirmed the findings reported by Barnat and collaborators in a sheep model. 2
Despite HIFU provokes similar damage if compared with endothermal techniques (e.g., endovenous laser [EVLA] or radiofrequency ablation [RFA]), some differences remain unusual and worthy of highlighting.
First, endothelium seems to be not significantly damaged in our sample collected 4 months from HIFU. It is well-known that histological examination of GSV wall after endovenous techniques reveals intimal injury and inflammatory cell infiltration, with complete de-endothelialization just after one RFA cycle 5 or within 2 min after foam sclerotherapy injection. 6 Conversely, HIFU could provide a sort of extravenous thermal ablation (ExTA) maintaining partially unharmed the intima layer, showing only a thickening. 4 This effect could minimize the HIFU effect on blood/wall interaction and provide vein “restoration”, instead of vein “ablation”.
Second, local injury was also observed in the perivenous space leading to vacuolization, known as fat-fibronecrosis due to lipid and fibrotic predominance. This is visible on ultrasound as “perivenous haze” during the first week and over time, it progresses to a consolidated sleeve-like fat-fibrosis around the vein, remaining permanent even after 2 years (ongoing not published data).
Conclusion
HIFU could provide specific vein wall damage, maintaining intact the endothelium and contracting the perivenous space. A new technology drives to new effects, sometimes unknown before, and these findings could be disruptive in haemodynamic treatment of GSV incontinence. Further analysis should be done to specify different patterns according to HIFU energy delivered, and the clinical impact of these vein wall modifications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The regional ethics committee approved this study.
Guarantor
PC.
Contributorship
Conception and design of the study: PC, DB, MP, EN, LS. Acquisition of data: PC, MP, EN, LS. Analysis and interpretation of data: PC, DB, MP, EN, LS. Drafting the article: PC, DB, LS. Revising it critically: PC, DB, MP, EN, LS. Final approval of the version to be submitted: PC, DB, MP, EN, LS.