
Abstract
Objectives
To investigate the prevalence, clinical characteristics and risk factors of hospital acquired venous thromboembolism (HA-VTE) in a Chinese Hospital.
Methods
Retrospective analysis of patients diagnosed as HA-VTE in a single institution from January 2016 to December 2022 was performed. Patients with VTE prior to admission or within 48 h after admission were excluded. Demographic data of patients was retrieved from the electronic medical database, and parameters affecting the occurrence of HA-VTE were analyzed.
Results
4,022 patients from 321,997 episodes of medical admissions were diagnosed as VTE. Among these, 952 (23.7%) fulfilled the criteria of HA-VTE, corresponding to an incidence of 0.296%. 76% of patients presented with HA-deep vein thrombosis (DVT) alone, 13% presented with isolated HA-pulmonary embolism (PE), and 11% presented with concomitant HA- DVT and PE. Risk factor analyses showed statistically higher incidence in patients with elder age (67.5 ± 15.5 vs 48.3 ± 17.2 years, p < .001), male gender (0.346% vs 0.262%, p < .001), malignancy (0.513% vs 0.252%, p < .001), trauma (0.659% vs 0.28%, p < .001), emergency admission (0.664% vs 0.186%, p < .001), ICU stay (2.981% vs 0.226%, p < .001), and patients undergoing major surgery (0.702% vs 0.176%, p < .001). Patients with HA-VTE had longer hospital stay (22.5 ± 26.6 vs 7.21 ± 9.23 days, p < .001) and higher mortality rate (8.51% vs 1.01%, p < .001). The crude incidence rate of HA-VTE increased annually from 0.75 per 1,000 patients in 2016 to 5.89 per 1,000 patients in 2022. The subspecialties with the highest incidence rate of HA-VTE were cardiovascular surgery (1.40%), neurosurgery (1.10%), and respiratory medicine (0.72%).
Conclusion
This is one of the few large scale studies to show that HA-VTE, accounting for nearly one quarter of all VTE events, occurs in 0.296% of adult hospitalizations. Patients with elder age, malignancy, ICU stay, and undergoing major surgery require more intensive HA-VTE surveillance and prevention.
Introduction
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), is a preventable cause of hospital death, 1 affecting millions globally per annum as a leading contributor to global disease burden. 2 VTE is the third major cause of cardiovascular mortality after heart attack and stroke.3,4 Hospital acquired VTE (HA-VTE), defined as an event occurring during or within 90 days post-hospitalization, plays a significant role in morbidity, mortality and disablement. It has been reported three quarters of all VTE related deaths are from HA-VTE.2,5–8 Preventing HA-VTE as a complication of medical care has become an international imperative. HA-VTE can be circumvented through risk evaluation and implementation of efficient thromboprophylaxis. Published studies revealed a high incidence of thrombosis in hospitalized high-risk patients, and considerable risk reduction could be achieved by VTE pharmacological prophylaxis.9,10
The prevalence of VTE varies among different ethnic/racial groups. 11 According to our previous published data, the most common cause of VTE in Chinese population were immobilization, malignancy and trauma or surgery. 12 The incidence of DVT and PE after major operation were 0.2% and 0.12%, respectively. 13 Detailed comprehension of VTE incidence, mortality, and attributes within healthcare systems is integral for VTE care planning and resource allocation. The incidence of HA-VTE was reported to be approximately 100 per 100,000 person-years in Western countries,14,15 but data on the incidence of HA-VTE in Asian population is scarce. The aim of this study was to investigate the prevalence, clinical characteristics and risk factors of HA-VTE in a cohort of Chinese patients.
Methods
This is a retrospective analysis of patients diagnosed as HA-VTE at our institution from January 2016 to December 2022. This study was approved by the hospital’s institutional review board (IRB No. 2024025). The demographic data of patients was retrieved from the electronic medical database (iMedical HIS, iMEDWAY Technology Co. Ltd, Beijing, China), and parameters affecting the occurrence of HA-VTE were analyzed. This study was conducted according to STROBE guidelines. 16
Definition of HA-VTE and collection of data
HA-VTE was defined as DVT or PE occurring at least 48 h after clinical admission or within 90 days of hospital discharge following an inpatient stay of at least 2 days1 17 VTE documented on admission or occurred within 48 h after hospitalization was defined as community-acquired VTE (CA-VTE). Distal DVT, also named as calf DVT, was defined as thrombus below the popliteal vein. 18 Proximal DVT was defined as DVT in the popliteal, femoral or iliac veins. 19 All patients diagnosed as VTE using the International Classification of Disease, Tenth Edition (ICD-10) at our center between January 1, 2016, and December 31, 2022 were identified from our hospital electronic database. Patient demographics and past medical history were reviewed and retrieved manually, and tabulated.
Inclusion and exclusion criteria
Inclusion criteria were: (1) patients ≥18 years old; (2) VTE was confirmed with duplex ultrasound or computerized tomography angiography (CTA) or digital subtraction angiography (DSA); (3) VTE occurred at least 2 days after admission.
Exclusion criteria were: (1) patients diagnosed as VTE on admission or previously documented VTE, or within 48 h after hospitalization; (2) patients with previous VTE after review of medical record; (3) patients younger than 18 years old.
Statistical analysis
This was a descriptive analysis to determine the incidence of VTE and describe the demographic and clinical characteristics of this population. We calculated means and standard deviations (SD) for continuous variables and proportions for binary variables (including VTE incidence). Comparisons between patients with and without HA-VTE were performed using either 2-tailed t tests or χ2 analysis. The annual variation of HA-VTE risk was analyzed by calculating odds ratio (OR) and fitting a nonlinear regression curve of incidence rate. Statistical significance was set at p < .05. All statistical analyses were performed using SPSS 26.0 software (IBM Corp, Armonk, NY).
Results
A total of 4,022 VTE patients were identified from 321,997 adult inpatients, including 3,070 diagnosed with acute VTE on admission or within 2 days after hospitalization. A total of 952 patients with HA-VTE were included in this study, accounting for 23.6% of all VTE events. The flow chart of screen for patients with HA-VTE was shown in Figure 1. The incidence of HA-VTE was below 1%. Approximately three quarters of patients with HA-VTE presented with DVT alone (Figure 2). Nearly half of DVT occurred during hospitalization (56.4%, 468/830) were proximal DVT. Flow chart for screening of patients diagnosed as hospital acquired venous thromboembolism. Percentage of deep vein thrombosis (DVT) and pulmonary embolism (PE) in the 952 patients with hospital acquired venous thromboembolism.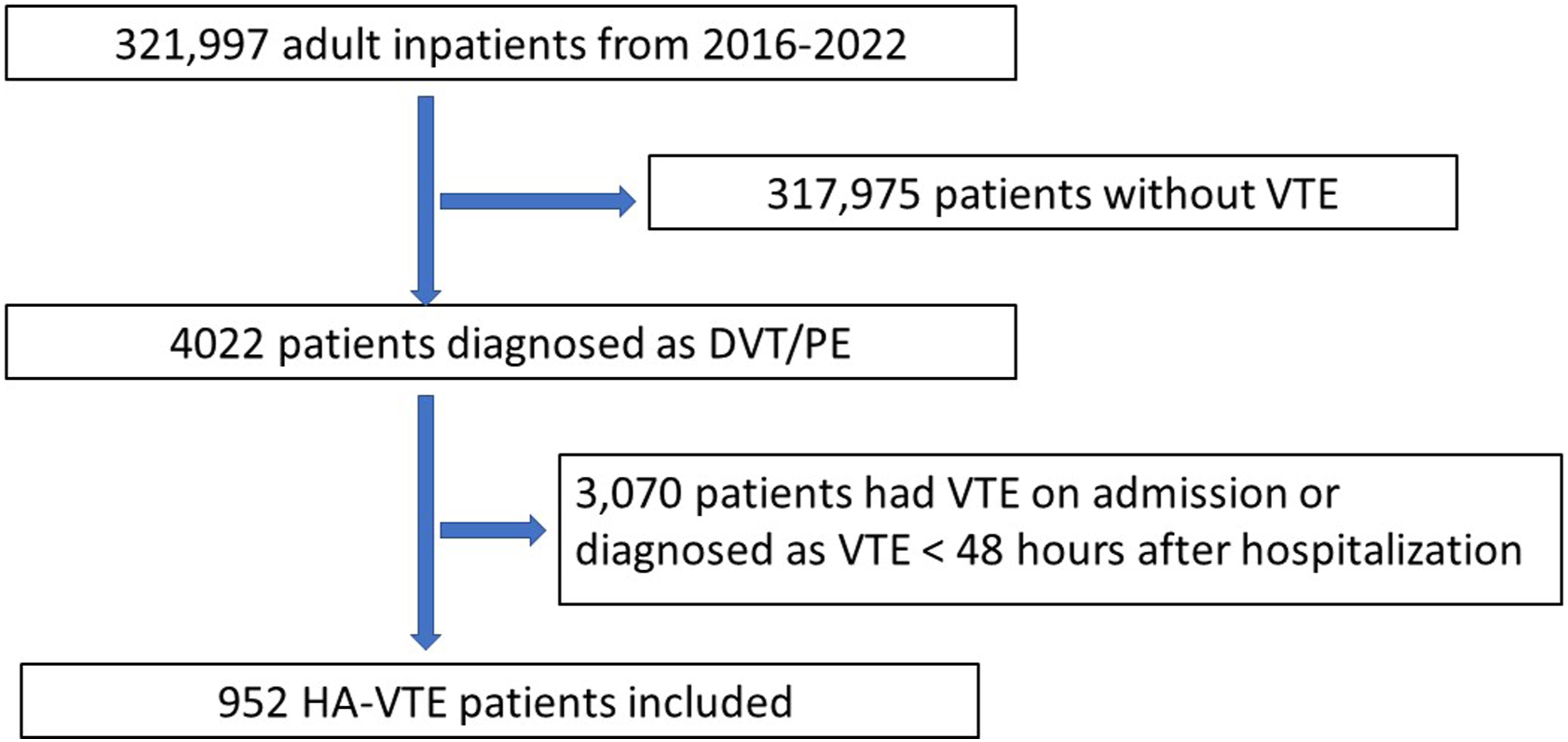

Comparison between patients with hospital acquired venous thromboembolism (HA-VTE) and without VTE.

Comparison between hospital acquired and community acquired venous thromboembolism.

HA-VTE: hospital acquired venous thromboembolism; CA-VTE: community acquired venous thromboembolism; PE: pulmonary embolism; ICU: intensive care unit; VTE: venous thromboembolism.
Univariate analysis of risk factors associated with the occurrence of hospital acquired venous thromboembolism.

Incidence of hospital acquired venous thromboembolism across age groups.

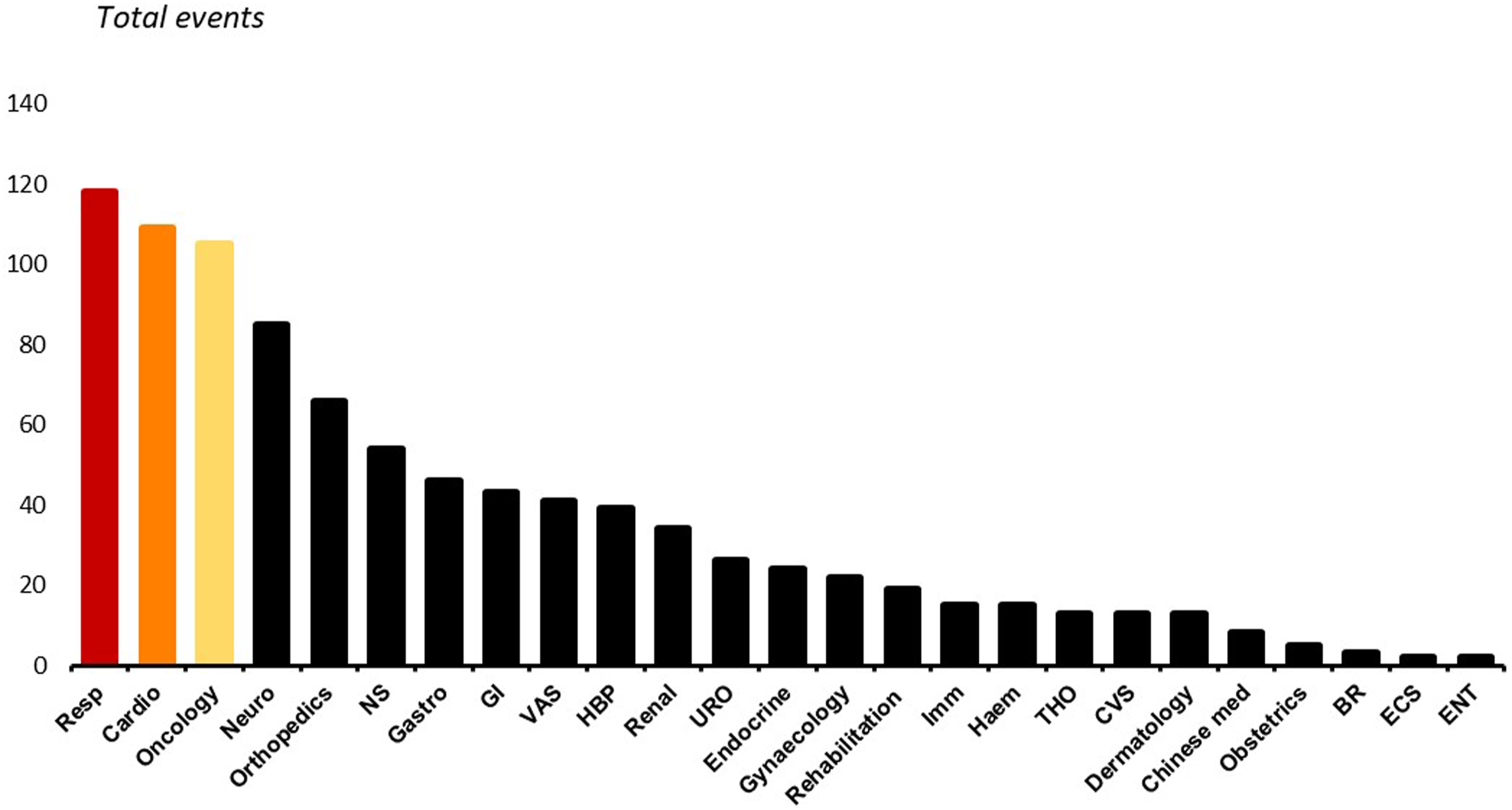
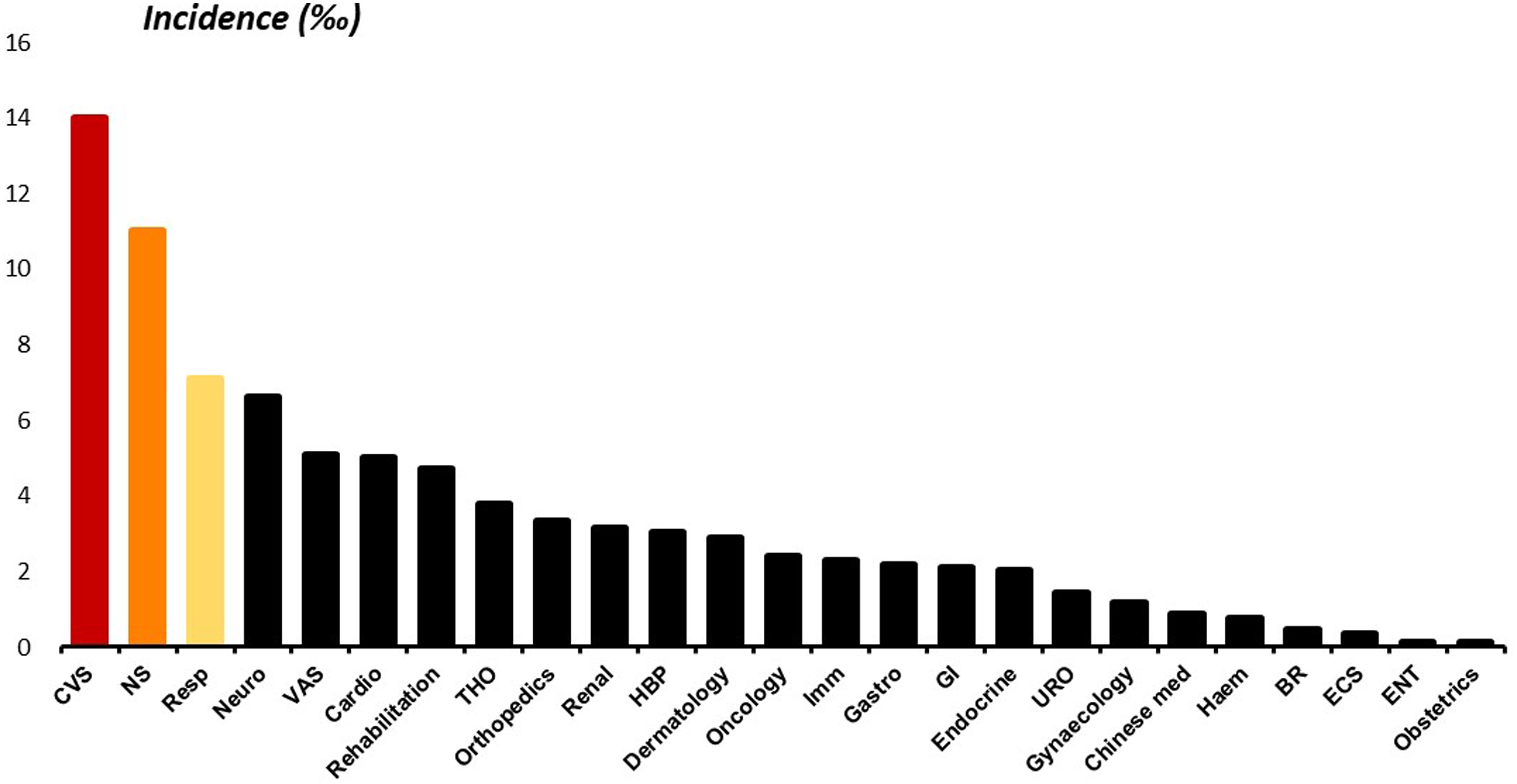
During the study period, the crude incidence rate (CIR) of HA-VTE increased annually from 0.75 per 1,000 patients in 2016 to 5.89 per 1,000 patients in 2022 (Figure 3). In patients with HA-VTE, the most frequently concomitant morbidity leading to the initial hospitalization were respiratory disease (12.39%), cardiovascular disease (11.45%), cancer (11.03%), neurological disease (8.93%), and orthopedic disease (6.93%) (Figure 4). The subspecialties with the highest incidence rate of HA-VTE were cardiovascular surgery (1.40%), neurosurgery (1.10%) and respiratory medicine (0.71%) (Figure 5). Crude incidence rate of hospital acquired venous thromboembolism from 2016 to 2022. HA-VTE: Hospital Acquired Venous Thromboembolism; CIR: Crude Incidence Rate. Distribution of events of hospital acquired venous thromboembolism according to subspecialties (Resp, respiratory medicine; Cardio, cardiology; Neuro, neurology; NS, neurosurgery; Gastro, gastroenterology; GI, gastrointestinal surgery; VAS, vascular surgery; HBP, Hepato-Biliary-Pancreatic Surgery; URO, urology surgery; Imm, immunology; Haem, haematology; THO, thoracic surgery; CVS, cardiovascular surgery; BR, breast surgery; ECS, endocrine surgery; ENT, ear-nose-throat surgery). Incidence of hospital acquired venous thromboembolism according to subspecialties (Resp, respiratory medicine; Cardio, cardiology; Neuro, neurology; NS, neurosurgery; Gastro, gastroenterology; GI, gastrointestinal surgery; VAS, vascular surgery; HBP, Hepato-Biliary-Pancreatic Surgery; URO, urology surgery; Imm, immunology; Haem, haematology; THO, thoracic surgery; CVS, cardiovascular surgery; BR, breast surgery; ECS, endocrine surgery; ENT, ear-nose-throat surgery).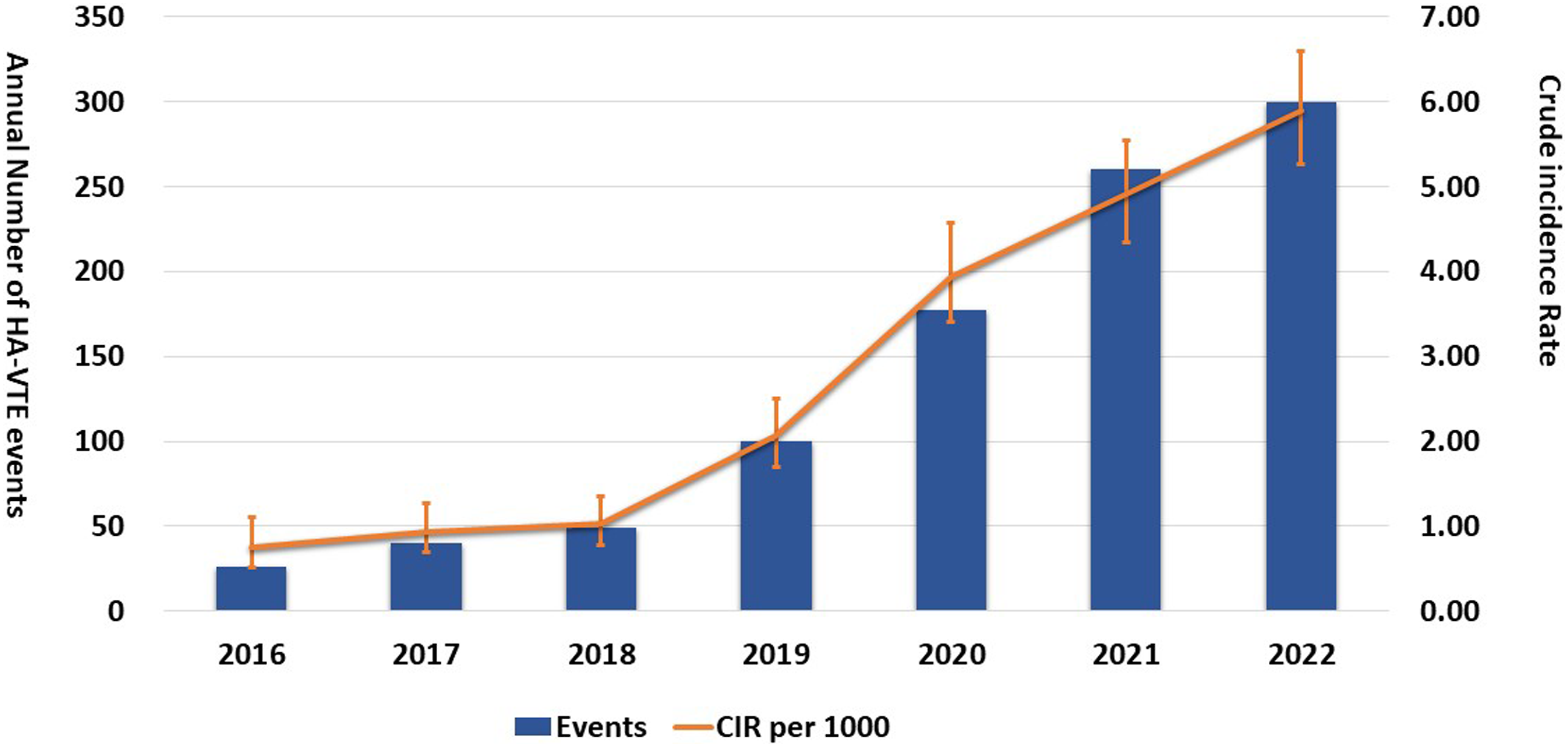
Discussion
This is one of the first studies to report the incidence of HA-VTE in Chinese patients, and showed that the incidence was 0.296% over a 7-year period, and addressed a real knowledge gap in the incidence of HA-VTE in patients of Chinese ethnicity. Previous study only reported that the incidence of HA-VTE was 0.57% in Chinese patients with cardiovascular disease. 20 Similar data from Caucasian population is also sparse. Kevane et al. reported the rate of HA-VTE was 0.14% within the Ireland East Hospital Group. 21 A multi-institutional study conducted in the United States revealed an incidence of approximately 0.25%, 22 while the incidence of HA-VTE in England was reported to be 0.17%. 23 The epidemiological characteristics of HA-VTE and CA-VTE were similar, including mean age, sex composition, and mortality. However, HA-VTE patients had prolonged hospital stays and higher rates of intensive care, indicating the presence of more severe and complex conditions in these individuals. Furthermore, HA-VTE patients demonstrated a lower incidence rate of concomitant PE, potentially attributable to earlier diagnosis and treatment during hospitalization.
A recent published study revealed that patients presented to emergency department with VTE had a higher risk of mortality at a mean follow up of 2.1 years. 24 It has been reported 40% of HA- VTEs were preventable. 25 There is increasing evidence in the past decades that risk stratification and prophylactic methods are useful in preventing HA-VTE.26,27 The American Heart Association has a policy statement to reduce HA-VTE by 20% by the years 2030. 28 Randomized controlled trials have demonstrated that pharmacologic thromboprophylaxis can substantially decrease the incidence of PE and DVT among medical and surgical individuals.29,30 However, the implementation of universal thromboprophylaxis is not advocated owing to potential bleeding complications. According to 2012 ACCP guidelines, mechanical or pharmacological prophylaxis is recommended for patients at moderate or high risk of VTE. 19 It is imperative to evaluate the risk of hospitalized patients to pinpoint those with augmented VTE risk and a diminished bleeding risk, and subsequently administer tailored appropriate thromboprophylaxis.19,31 In a decision analysis modelling study in NHS hospitals in England, offering pharmacological prophylaxis of VTE for all eligible medical inpatients was considered as the most cost effective strategy. 32 We found that patients with advanced age, male gender, emergency admission, cancer, ICU stay, trauma and extensive surgery, notably those with cardiopulmonary or neurological conditions are more likely to developed HA-VTE. The incidence of HA-VTE increased significantly with elder age, more than half of the HA-VTE events occurred in patients over 65 years old.
The common risk factors associated VTE in hospitalized patients include older age, obesity, infection, acute stroke, inflammatory bowel disease, malignancy and surgical procedures.33–35 The incidence of DVT and PE following stroke in eastern China were reported to be 4.49% and 0.80 respectively. 36 During the study period, the incidence of HA-VTE increased annually, potentially due to more frequent VTE screen in hospitalized patients. In addition, more and more patients with complex disease, advance age, malignancy and undergoing major surgery were admitted over the years, this may lead to an increasing incidence of HA-VTE. Moreover, patients with coronavirus disease 2019 (COVID-19) were more likely to developed VTE during hospitalization as COVID-19 was associated with inflammation and thrombosis.37,38
To improve the outcome of VTE prevention, numerous measures have been used worldwide. In US, John Hopkins multi-disciplinary VTE prevention collaborative developed a mandatory tool for VTE risk stratification and prophylaxis in 2005. 39 The US Joint Commission and the National Quality Forum also implemented a standardized project to prevent VTE in 2005. 40 In UK, VTE prevention was identified as one of the two national goals by National Health Service Operation Board. 41 In 2018, National Institute for Health and Care Excellence published the guideline to reduce the risk of hospital-acquired DVT or PE in hospitalized patients aged more than 16 years old. 42 The Asian guidelines on prevention of VTE was first published in 2012, 43 and it was updated in 2017. 44 In China, recommendations on prevention and management of HA-VTE was first published in 2012. 45 Standardized prevention of VTE has been one of the national medical quality and safety improvement targets advocated by China Health Commission since 2021. 46 In our center, the multidisciplinary program on VTE prophylaxis was implemented in 2020. Lau et al perfectly summarized the ideal VTE prevention process: standardized assessment of VTE risk, prescription of optimal and appropriate prophylaxis, and provision of prescribed VTE prophylaxis. 47
This study had several limitations. Firstly, we were unable to identify those HA-VTE occurred within 90 days after discharge. Therefore, the precise incidence of HA-VTE may be underestimated. Secondly, most of the ultrasound scan were performed for DVT screening, it was unable to conclude how many patients with HA-VTE were symptomatic. Lastly, mechanical or pharmacal prophylaxis of VTE were not taken into consideration. Hence, the consequence of thromboprophylaxis in high-risk patients remained unknown. Further study is warranted to assess the effect of targeted risk stratifications and mechanical or pharmacal prophylaxis in prevention of HA-VTE.
Conclusion
Our study suggested that HA-VTE, accounting for at 23.7% of all VTE events, occurred in 0.296% of adult Chinese patients. Patients with elder age, malignancy, admitted to ICU, and those undergoing major surgery, particularly those with cardiopulmonary and neurological conditions, required more intensive HA-VTE surveillance and prevention. Our findings provided compelling evidence for prioritizing strategies to reduce the risk of VTE among hospitalized patients.
Footnotes
Author’s note
Presentation Information, This study was presented in the International Poster Competition session at the 2024 Vascular Annual Meeting of the Society for Vascular Surgery, Chicago, Illinois, June 19-22, 2024.
Author contributions
Study design: Li HL, Zhang H, Chan YC
Data collection: Li HL, Zhang H
Data analysis: Li HL, Zhang H, Cheng SW
Manuscript preparation: Li HL, Zhang H, Chan YC
Critical review and revision: Li HL, Chan YC, Cheng SW
Final approval of the article: Li HL, Zhang H, Chan YC, Cheng SW.
Declarations conflicting interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grants from Guangdong Medical Research Foundation, China (No. B2023117).
Ethical statement
Guarantor
Yiu-Che CHAN, MB BS BSc MD FRCS FRCS (General Surgery) FCSHK, Associate Professor, Division of Vascular Surgery, Department of Surgery, The University of Hong Kong, Queen Mary Hospital, South Wing, 14th Floor, K Block, 102 Pokfulam Road, Hong Kong SAR, China. Email: