
Abstract
Background
To evaluate kinesiophobia and its relationship with disease-related characteristics and quality of life in lipedema patients.
Methods
In this descriptive case-control study, 40 lipedema patients and 40 participants in the control group were included. All participants were evaluated in terms of body mass index (BMI), pain numeric rating scale (NRS) and pain threshold (PT) scores, kinesiophobia (Tampa Scale for Kinesiophobia - TSK), lower extremity functional scores (Lower Extremity Functional Scale - LEFS), and health-related quality of life (Nottingham Health Profile - NHP) scores. Additionally, the lipedema patients were evaluated in terms of extremity volumes, and total and mean lower extremity fat mass by dual-energy X-ray absorptiometry.
Results
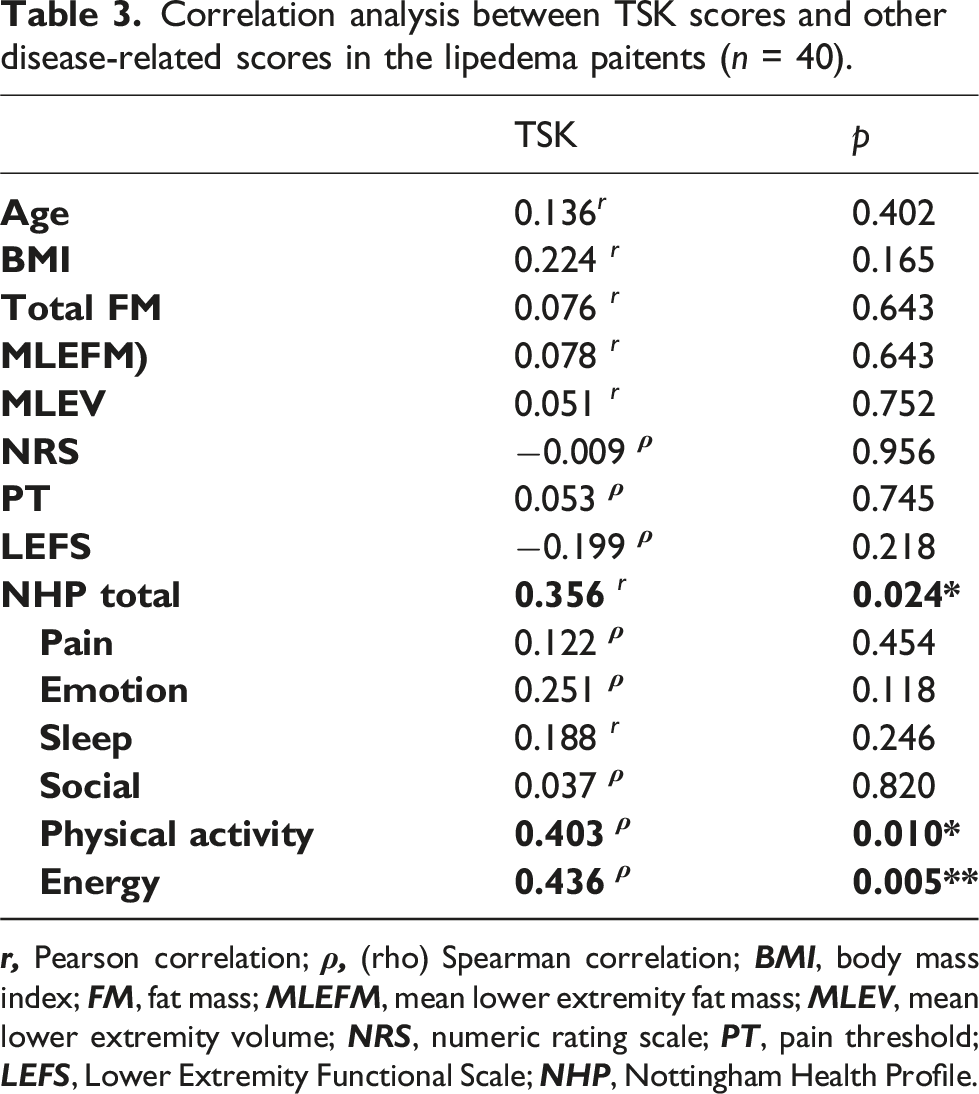
High kinesiophobia was detected in 78% of the lipedema patients and 55% of the control group (p = .033). TSK (p = .048), NRS (p = .001), and NHP total scores (p = .041) were higher and PT scores (p = .007) were lower in lipedema patients compared to the control group. No difference was found between lipedema patients with high and low kinesiophobia in terms of fat mass or extremity volumes. A positive correlation was found between TSK score, NHP total score (r = 0.356, p = .024), NHP physical activity (ρ = 0.403, p = .010) and NHP energy (ρ = 0.436, p = .005) subscale scores
Conclusion
Kinesiophobia is highly prevalent in lipedema patients, regardless of disease-related data and affecting the quality of life of the patients, negatively.
Introduction
Lipedema is a persistent and frequently progressive disorder that is characterized by symmetrical enlargement, pain, and easy bruising in the lower and/or upper limbs. The body type is disease-specific and resistant to excessive exercise and diet. Although there are several hypotheses, including genetic, hormonal, vascular, and lymphatic factors, the pathophysiology of the disease and the mechanism of the pain are still unclear.1,2 Since lipedema is frequently unrecognized, failing to lose weight and feeling chronic pain lead to poor quality of life and psychological problems, such as depression, anxiety, and bulimia nervosa.3,4 Limited limb mobility and pain are the factors that can contribute to health-related quality of life deficiencies. 5
Kinesiophobia is defined as an excessive and irrational fear of physical movement to avoid harm or re-injury. It can also be defined as an excessive irrational fear of physical movement and activity resulting from a feeling of vulnerability due to pain. It appears as a type of fear avoidance behavior.6,7 It has been shown that kinesiophobia is more common in diseases affecting the lower extremities such as obesity, 8 knee osteoarthritis, 9 and lymphedema.10,11 Since lipedema is a chronic disorder characterized by pain in lower extremities, it was hypothesized that kinesiophobia could be seen more frequently in lipedema patients than in the healthy population. Therefore, it was aimed to examine lipedema patients in terms of kinesiophobia, compare them to the control group, compare the lipedema patients with low and high kinesiophobia in terms of disease-related data and to evaluate the correlation between lipedema disease-related data and kinesiophobia.
Material and method
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee. Written informed consent was obtained from all participants.
This descriptive case–control study was conducted in a tertiary hospital. Individuals who applied to the Physical Medicine and Rehabilitation clinic and met the terms of inclusion and exclusion criteria were included between January 2024 and June 2024.
Women with lipedema, aged 18 and over were included in the study. The patients in the lipedema group had no history of liposuction surgery, musculoskeletal/vestibular disease, heart failure, hypothyroidism, no active infection, peripheral vascular disease or cancer. The participants in the control group had no history of systemic, neuromusculoskeletal or vestibular disease. Furthermore, the control group was matched to the lipedema group in terms of age and body mass index (BMI) to ensure comparability between groups. The control group was not selected from hospital patients. Instead, it primarily comprised healthcare professionals and family members accompanying patients without lipedema. This approach was adopted to ensure ease of recruitment.
In this study, lipedema diagnosis was confirmed based on clinical criteria proposed by Wold et al. 12 According to these criteria, the expansion starting from the hips and lower extremities progresses symmetrically bilaterally. Feet generally maintain their normal size and structure. There is moderate to severe sensitivity to digital pressure. Subcutaneous fat tissue is soft and flexible. Usually, the upper body parts are normal in size. There are 5 types and 4 stages of lipedema. 13 Fat accumulation is around the hips and buttocks in type 1, extends from the hips to the knee in type 2, extends from the hips to the ankle in type 3, and if the arms are also involved, it is defined as type 4. In type 5, fat accumulation occurs predominantly only in the calf area. In stage 1, the skin is smooth and soft, but the underlying hypodermis is thickened on palpation. In stage 2, there is a nodular appearance on the skin that resembles orange peel skin. In stage 3, there are large folds and pits on the deformed fat masses. If lymphedema accompanies lipedema, it is considered stage 4. In the present study, participants were eligible if they were diagnosed with lipedema of type 2 or type 3 and classified as stage 1, 2, or 3.
Patients with a diagnosis of lipedema were evaluated by a physical medicine and rehabilitation physician who recorded sociodemographic data, BMI, pain numeric rating scale (NRS) and pain threshold (PT) scores, extremity volumes, total and mean lower extremity fat mass, kinesiophobia (Tampa Scale for Kinesiophobia - TSK), lower extremity functional scores (Lower Extremity Functional Scale - LEFS) and health related quality of life (Nottingham Health Profile - NHP) scores. In the control group, BMI, NRS, PT, TSK, LEFS, and NHP scores were recorded.
Patients with lipedema were compared with the control group in terms of age, BMI, pain and pain threshold, TSK, LEFS, NHP scores. Then the lipedema group was divided into two groups, those with low and high kinesiophobia, and these two subgroups were compared in terms of age, BMI, extremity volumes, total and mean lower extremity fat mass, pain and pain threshold, TSK, LEFS, NHP scores. Additionally, correlation analyses were conducted within lipedema group to examine associations between TSK scores and each of the following variables: age, BMI, extremity volumes, total and mean lower extremity fat mass, pain and pain threshold, LEFS, and NHP scores.
Outcome measures
• • Algometric measurements were performed to determine • For the • Dual-energy X-Ray Absorptiometry (DXA) measurements were performed with the patient in the supine position at head-heel distance with a radiation dose of 5.08 μSv, voltage of 83.00 Kv, and current of 0.2 mA (Primus, X-ray densitometer, Osteosys Co. Ltd., Guro-gu, Seoul, Korea). • • •
Sample size
G*Power (V3.1) software (Informer Technologies, Inc., Los Angeles, USA) was used to calculate the required sample size. Using data from a previous study, the effect size in our sample size calculation was found to be 0.64. Based on a power of 80% and a 5% level of significance, the total sample size required was calculated as 80. 23
Statistical analysis
Statistical analyses were conducted using SPSS version 23.0 software (IBM Corporation, Armonk, NY, USA). Continuous data were presented as mean ± standard deviation (SD) and median (interquartile range), while categorical variables were expressed as numbers and percentages. The normality of the data distribution was evaluated with the Kolmogorov-Smirnov test. Depending on the normality of the variables, comparisons between groups were performed using either the independent samples t-test or the Mann-Whitney U test. Categorical variables were analyzed using Pearson’s chi-square test. Correlations among quantitative variables were assessed using Pearson or Spearman correlation coefficients. A p-value of less than 0.05 was considered statistically significant.
Results
A total of 80 participants were included in the study, 40 lipedema patients and 40 controls matched for age and BMI. High kinesiophobia was detected in 78% of the lipedema patients (n = 31) and 55% of the control group (n = 22), and this difference was statistically significant (p = .033, Figure 1). High and low kinesiophobia percentages of the groups (p = .033).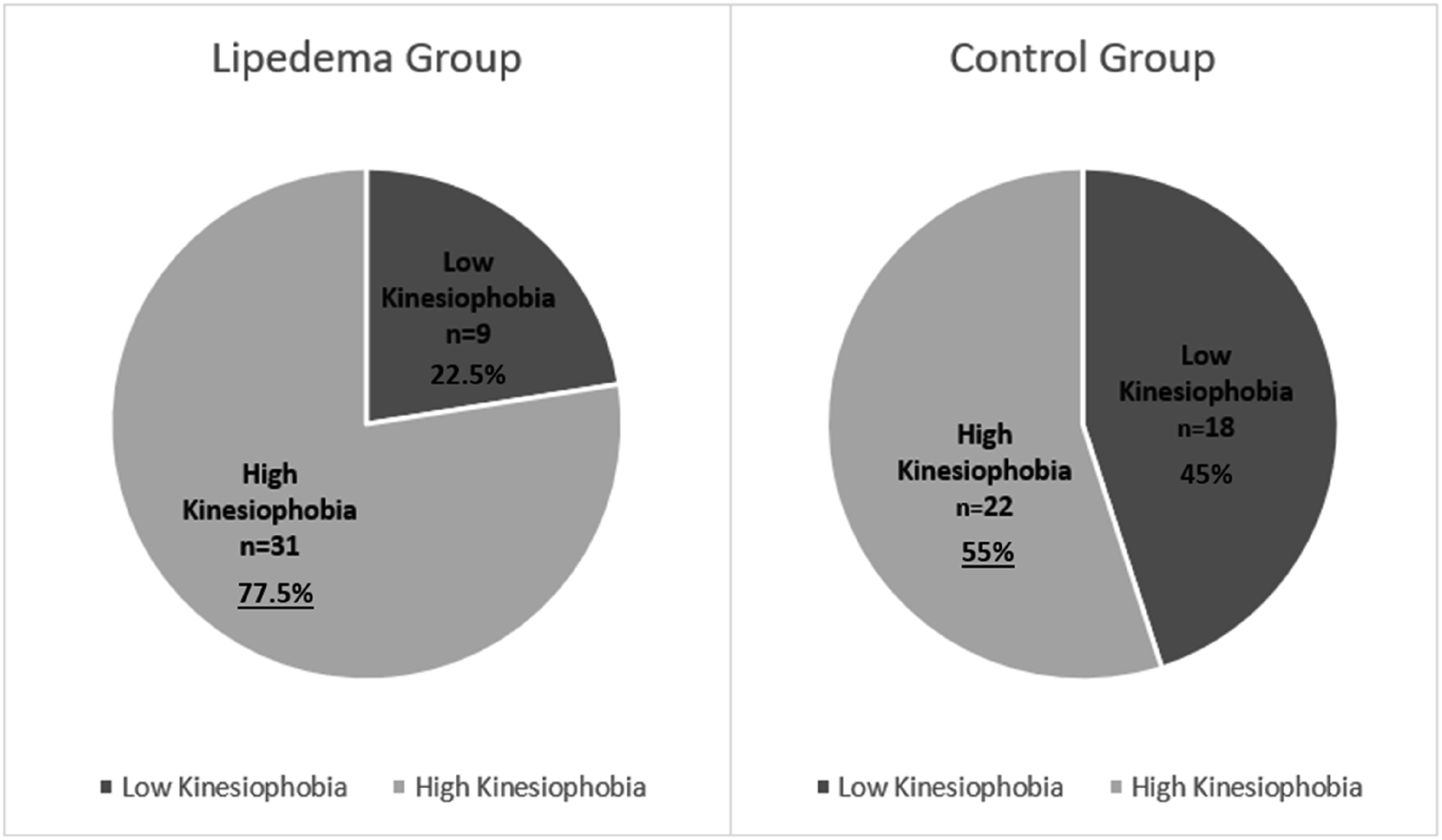
Comparisons between lipedema and group.

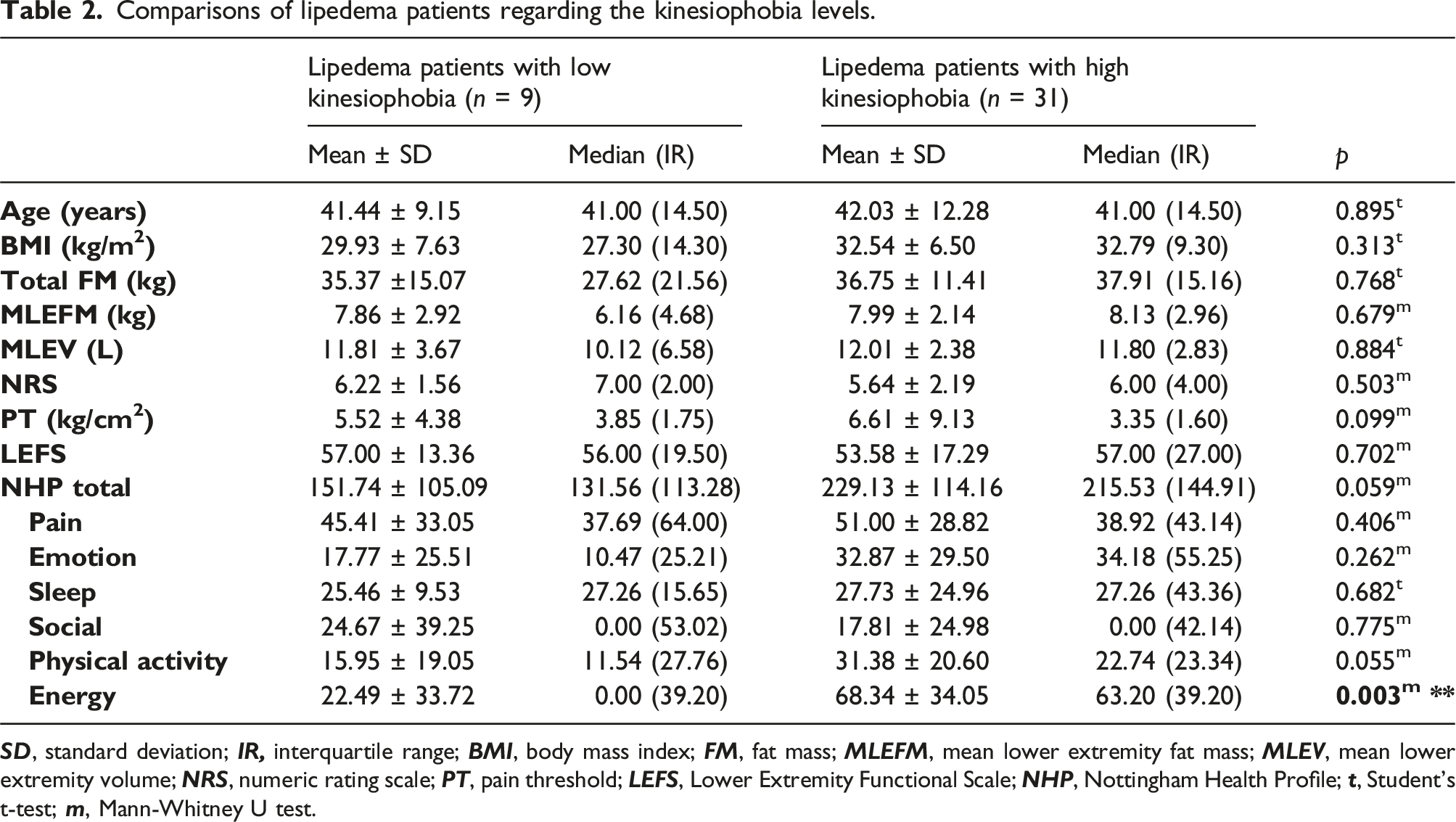
Comparisons of lipedema patients regarding the kinesiophobia levels.
Correlation analysis between TSK scores and other disease-related scores in the lipedema paitents (n = 40).
Discussion
To the best of our knowledge, this is the first study evaluating kinesiophobia in patients with lipedema. The hypothesis of the study was that kinesiophobia would be higher in the lipedema patients than in the control group, and that kinesiophobia would be related to high fat mass and extremity volumes. The results of the study partially supported this hypothesis. The TSK scores of patients in the lipedema group were higher than those in the control group and the number of patients with high kinesiophobia was statistically significantly higher in the lipedema group. In addition, pain scores were higher, pain threshold and pain-related quality of life were lower in the lipedema patients than in the control group.
It is known that pain is the primary complaint in lipedema. 24 In addition to the painful nature of lipedema fat, the negative effects of the disease-specific body structure on the lower extremity joints and spine also contribute to pain. 25 In the present study, high pain levels and low pain thresholds were to be probably the most important causes of kinesiophobia. Furthermore, lipedema is characterized by the failure of extreme diets and physical activity to reduce fat accumulation. 26 Unsuccessful exercise experiences throughout life may also contribute to the development of kinesiophobia.
Previous studies have stated that obesity is a risk factor for kinesiophobia.8,27,28 However, since the BMIs of the lipedema and control groups were similar, the findings of this study suggest that kinesiophobia in lipedema patients cannot be solely attributed to a high BMI. Although the rate of kinesiophobia was relatively high in the control group- possibly due to obesity- it was significantly more common in the lipedema group (77.5%) compared to the control group (55.0%). Moreover, the absence of a correlation between TSK scores and BMI in the lipedema group further supports this finding. On the other hand, the high prevalence of kinesiophobia observed in the control group was also unexpected. Since the study was conducted in a tertiary hospital setting, a substantial proportion of the control participants were healthcare professionals and family members accompanying patients. It is therefore plausible that exposure to a high-stress clinical environment and emotional concerns related to caregiving may have contributed to elevated levels of anxiety and stress, thereby influencing their kinesiophobia scores. This recruitment strategy was adopted to facilitate accessibility; however, the unique background of the control participants may have influenced certain psychosocial variables, such as work-related stress, emotional burden from caregiving, or heightened sensitivity to health-related symptoms, potentially limiting the generalizability of the findings.
From another perspective, the humiliation and shame that lipedema patients experience may contribute to increased kinesiophobia levels. As shown in the study conducted by Melander et al, these women are humiliated because they are perceived as “fat” and seen as “characterless” by others since they cannot control their bodies. 29 Over the years, they may internalize these humiliations, and the resulting distortion of self-perception may cause them to become ashamed of their bodies. This social experience may lead them to avoid movement in order not to be noticed and thus avoid being judged and humiliated by others. For this reason, it can be considered that these psychosocial factors may be among the reasons for the increased kinesiophobia observed in patients with lipedema.
When patients with high and low kinesiophobia were compared within the lipedema group, there was no significant differences were in disease-related measurements (pain threshold, total and lower extremity fat mass, and extremity volumes). This suggests that kinesiophobia emerges regardless of the severity of lipedema. DXA was used for fat measurement in the study. DXA is a preferred and useful method in the diagnosis and follow-up of lipedema.30,31 However, its major disadvantage is its inability to differentiate between fat and water. 32 Therefore, further studies using methods that allow high-quality evaluation of soft tissue, such as MRI, may provide more definitive results.
In the evaluation of the lipedema group, no correlation was found between TSK scores and BMI, pain, lower extremity function, fat mass, or lower extremity volumes. Unfortunately, these results didn’t support the hypothesis of the present study. It was slightly surprising that TSK scores did nor correlate with disease-related variables, since considering that the main pathology in lipedema is hypertrophic, fibrotic and inflamed adipose tissue.33,34 Although the sample size was determined through a power analysis based on a previous study, it is believed that this relationship could be evaluated more thoroughly in larger future studies.
Another important finding of this study was the significant correlation between kinesiophobia scores and NHP scores, suggesting that kinesiophobia is associated with a worse overall quality of life. In particular, the life domains of energy and physical activity were negatively affected. Similarly, in a previous study it is reported that pain and low physical activity levels negatively affect overall health. 35 In order to improve the quality of life of lipedema patients, beyond the commonly suggested interventions such as physical exercise, 36 diet-induced weight loss, 37 decongestive therapies,38,39 treatment for fibromyalgia symptoms,40,41 and even surgery, 42 it is important to provide medical support specifically targeting kinesiophobia.
Lipo-lymphedema (stage 4 lipedema) patients were not included in this study. However, it is known that even in early stages, interstitial fluid accumulation increases in lipedema patients. 43 Potential contributing factors promoting fluid accumulation in lipedema include increased limb capillary pressure, tissue structural alterations, impaired vascular permeability, increased lymphatic area, and insufficient lymphatic outflow. 44 As in lymphedema,10,11 where interstitial fluid increases due to lymphatic drainage disorders, kinesiophobia was found to be high in lipedema patients in this study.
In conclusion, kinesiophobia is highly prevalent in lipedema, regardless of disease-related factors. Considering that achieving a normal BMI, and engaging in exercise are recommended as the first-line treatments for lipedema, avoidance of movement due to kinesiophobia could negatively impact treatment success. If kinesiophobia is not addressed, patients may find themselves in a vicious circle: they avoid movement due to kinesiophobia, treatment is hindered due to lack of movement, and worsening symptoms further reinforce the fear of movement. To break this cycle, kinesiophobia must be recognized and managed. Given its high prevalence and detrimental impact on quality of life, kinesiophobia should be routinely assessed in individuals with lipedema and effectively addressed through targeted interventions to enhance treatment outcomes and overall well-being.
Footnotes
Authors’ note
The author (Mihrinur Dilvin Türköz) has moved to ‘Giresun Physical Therapy and Rehabilitation Centre, Giresun, Turkey’ since completing the research.
Author contributions
Conceptualization: ZK, MDT, BK, NÇY. Data curation: ZK, MDT, BK. Analysis: ZK, BK. Investigation: ZK. Methodology: ZK, MDT. Software: ZK, MDT. Visualization: ZK, NÇY. Writing - original draft: ZK. Writing - review & editing: ZK, MDT, BK, NÇY.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee of Giresun Education and Research Hospital (approval no: 18.12.2023/11). Also, the study was performed according to the Helsinki Guidelines.
Informed consent
A written informed consent was obtained from each patient.
Guarantor
ZK
Data Availability Statement
The datasets analysed during the current study are not publicly available due to the privacy of subjects but are available from the corresponding author on reasonable request.