
Abstract
Objectives
The aim of this study was to assess the prevalence of sublingual varicosity and lower limb varicosity in pregnant women, and to analyze the relationship between these variables.
Methods
This was a descriptive, analytical cross-sectional study conducted through clinical examinations of the oral cavity and lower limbs of pregnant women. The sample consisted of 193 pregnant women receiving care through a prenatal program. Sublingual varicosity was categorized using a dichotomous scale: grade 0 and grade 1. Lower limb varicosities were classified based on the CEAP clinical classification system.
Results
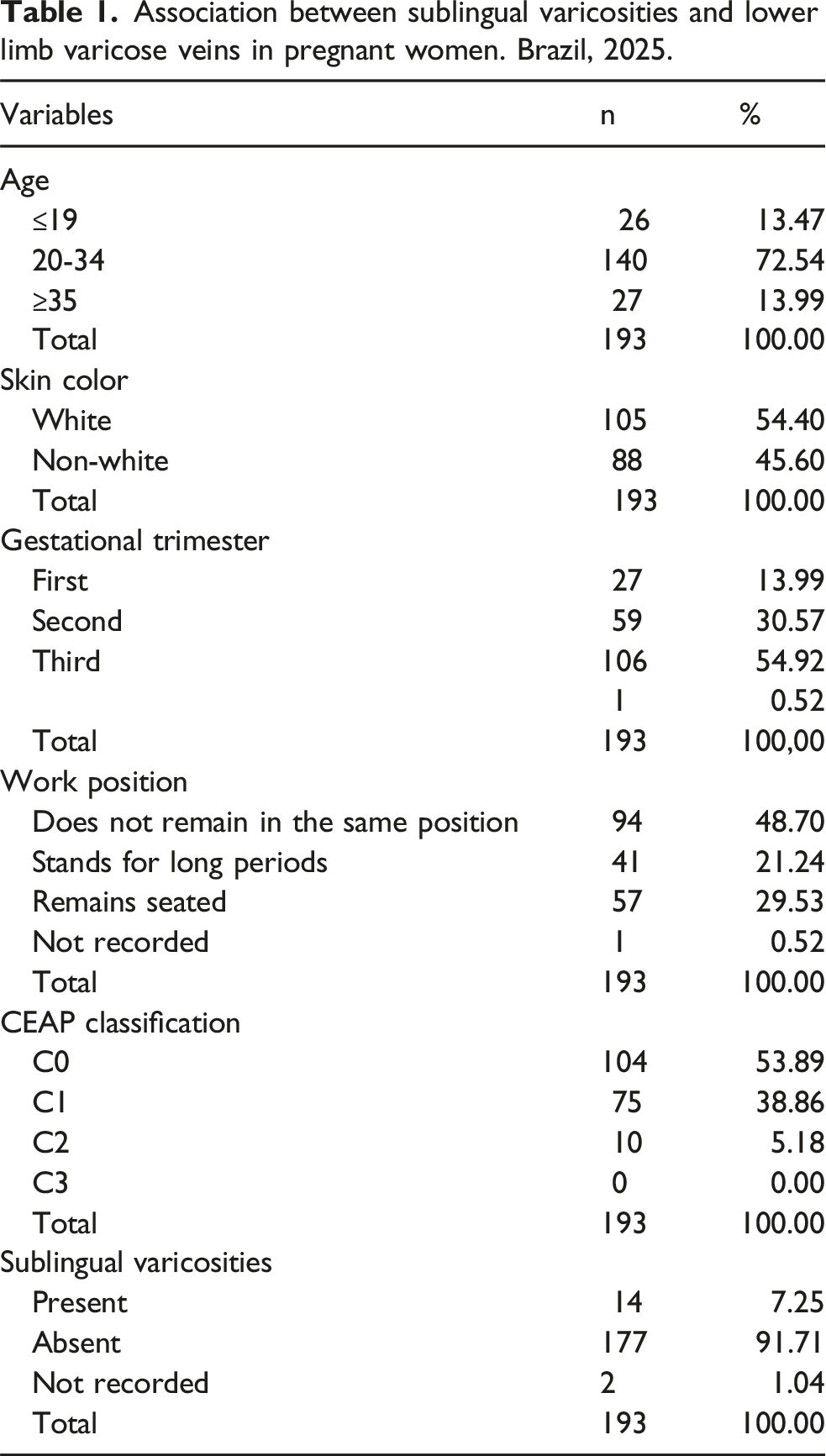
The prevalence of lower limb varicosities among the pregnant women was 85 out of 193 (44.04%), while sublingual varicosities were observed in 14 out of 193 participants (7.25%). A significant association was found between sublingual varicosities and lower limb varicosities (p = .0095).
Conclusion
The prevalence of sublingual varicosity was lower compared to lower limb varicosity, and an association between the two conditions was observed in pregnant women.
Introduction
Varicose veins are dilated, tortuous superficial veins that have lost their primary function of returning venous blood from the lower extremities to the heart. According to their diameter, they are classified into three categories: varicose veins (>3 mm), which are visibly protruding and typically involve the trunks of the great or small saphenous veins and their tributaries; reticular veins (1–3 mm), located within the dermis and not directly connected to the main axial veins; and telangiectasias (<1 mm), representing intradermal venous dilations. 1
Varicose veins are an occupational disease affecting a significant portion of the global population. 2 Prevalence varies by region, with higher rates in Western countries and lower rates in Papua New Guinea3,4. Major risk factors include sex, family history, obesity, combined hormonal contraceptives, prolonged standing, number of pregnancies, and occupational activity. 5
Evidence suggests that primiparous women (who have given birth once) exhibit a higher incidence of varicose veins compared to nulliparous women (who have never given birth), while multiparous women (who have given birth two or more times) are at the greatest risk.6,7 In 70% to 80% of women who develop varicose vein-related symptoms during pregnancy, these symptoms manifest in the first trimester, typically within two to 3 weeks after the onset of pregnancy. 8 Various outcomes have been investigated in studies on venous changes during pregnancy, including vein diameters, venous reflux, and stasis, all of which tend to worsen by the end of the gestational period.9,10
Sublingual varicosities usually present as multiple bluish or purplish elevations on the ventral tongue surface. 11 Their development is associated with connective tissue alterations and venous wall weakening from age-related elastic fiber degeneration. 12 Prevalence varies with systemic conditions, age, and behavior, reaching 70% in patients with cardiovascular disease versus 27% in individuals over 40 without it. 13 Associations have also been reported with smoking,14–16 hypertension,14–18 cardiovascular disease,19–21 and denture use. 20 However, evidence linking sublingual and lower limb varicosities remains scarce. As pregnancy is a known risk factor for leg varicosities, further research should investigate the prevalence of sublingual varicosities and their possible association with lower limb varicosities.
The objective of this study was to investigate the prevalence of lingual varicosities and lower limb varicosities in pregnant women, as well as the association between these variables.
Methods
This was a descriptive, analytical cross-sectional study conducted through clinical examinations of the oral cavity and lower limbs of pregnant women.
The sample consisted of pregnant women who sought care at public healthcare units of the Brazilian Unified Health System (SUS) and at the Specialty Medical Outpatient Clinic. Pregnant women were included in the study, and those who presented any of the following conditions were excluded: lesions on the lower limbs; any known ongoing degenerative disease; pregnant women classified as CEAP 4, 5, or 6; history of varicose vein surgery; inability to open the mouth; and those diagnosed with cancer in the head and neck region.
Pregnant women classified as CEAP stages 4, 5, or 6 were excluded from the study due to the presence of advanced clinical manifestations of chronic venous disease, including significant trophic changes. The inclusion of such cases could introduce bias in the analysis of the association between lingual varicosities and lower limb varicosities, as the pathophysiology in these stages is more complex and may involve multiple additional factors, such as chronic inflammation, lymphatic impairment, and a history of ulcers. Considering that sublingual varicosities may serve as an indicator of lower limb varicose veins, it is ideal that diagnosis occurs during the early stages of the disease.
The sample size calculation was based on data from a pilot study involving pregnant women who were not included in the final sample. The determination considered the prevalence of lower limb and lingual varicosities as primary outcomes, adopting the variable requiring the largest minimum sample size. Based on a population of 583 pregnant women registered in the municipality’s public health system, with a 95% confidence level, a 5% margin of error, and an expected prevalence of lower limb varicosities of 80%, the minimum required sample size was calculated to be 174 participants. Lists of pregnant women enrolled in the public prenatal care program were obtained, and eligible individuals were contacted and invited to participate in the study.
Intraoral and extraoral examinations were conducted in a single appointment by a calibrated examiner using a dental mirror and wooden spatula to assess the ventral surface of the tongue, floor of the mouth, lower lip mucosa, and lower limbs. Sublingual varicosities were classified dichotomously: grade 0 (few or no varicosities) and grade 1 (evident varicosities). 19 Lower limb varicosities were classified using the CEAP clinical system: C0 (no visible varicose veins), C1 (telangiectasias or reticular veins ≤4 mm), C2 (truncal varicose veins), C3 (varicose-related edema), C4 (skin changes such as hyperpigmentation, venous eczema, lipodermatosclerosis, atrophie blanche, or corona phlebectatica), C5 (healed venous ulcer), and C6 (active venous ulcer). 22
Data were analyzed using descriptive statistical techniques and the results were presented in tables. Data processing and statistical analysis were conducted using BioEstat software version 5.3, 23 and the G-test of association was applied at a 5% significance level.
This study was approved by the Human Research Ethics Committee, in accordance with the Declaration of Helsinki. 24 It was classified as minimal risk research, following the applicable national resolutions regarding research involving human subjects.
Results
Association between sublingual varicosities and lower limb varicose veins in pregnant women. Brazil, 2025.
Association between sublingual varicosities and lower limb varicose veins in pregnant women. Brazil, 2025.
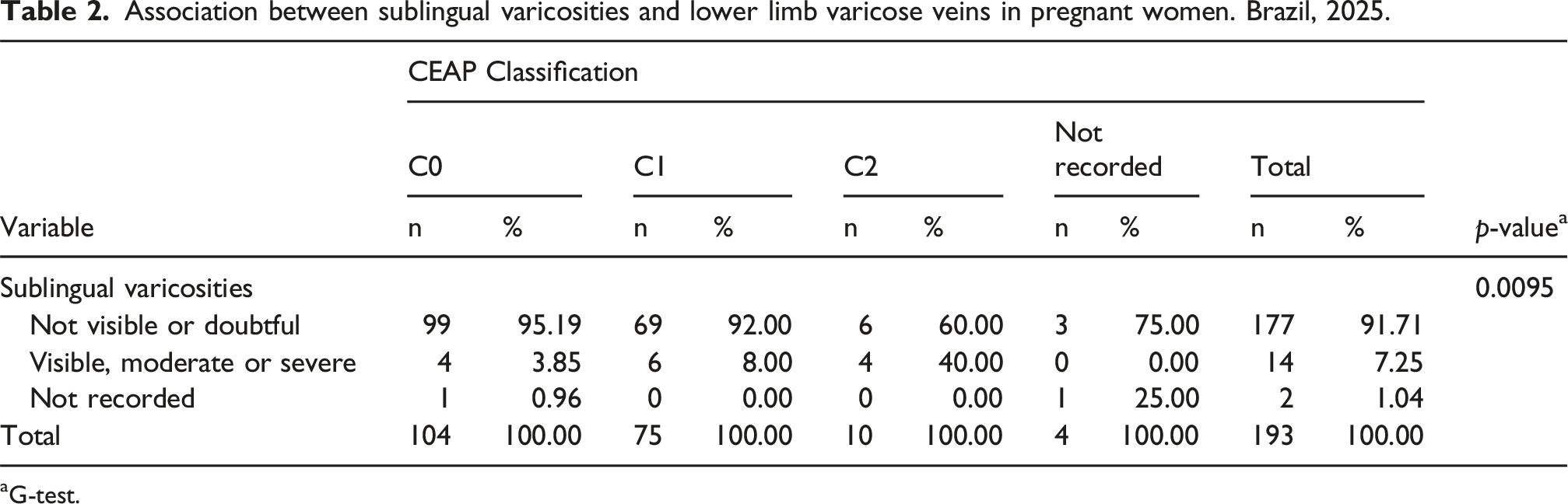
aG-test.
Discussion
This study on the prevalence of sublingual and leg varicosities found an association between lingual varicosities and lower limb varicose veins. Few studies have explored this relationship; however, these findings support a previous investigation in an Iranian nursing home for elderly individuals, which reported a statistically significant association (p < .0001) between sublingual varicosities and lower limb varicosities. 25
Superficial venous reflux is currently considered the most frequent cause of morpho functional alterations. 26 Venous blood from the lower limbs returns to the right atrium against gravity through the superficial and deep venous systems. 27 Therefore, the veins of the legs face the challenge of transporting blood back to the heart against gravitational forces, which may explain the higher prevalence of lower limb varicosities (44.04%) compared to sublingual varicosities (7.25%).
The prevalence of lower limb varicose veins during pregnancy ranges from 20% to 50%, rising to 70% when including other varices such as telangiectasias. 28 This condition is linked to increased blood volume and hormonal and mechanical factors. Elevated estrogen and progesterone levels increase venous capacitance and weaken vascular walls, respectively.29–32 Fetal growth and maternal weight gain raise intra-abdominal pressure, potentially compressing the inferior vena cava and reducing central venous return. This venous pressure increase can cause valvular insufficiency and varicosities.8,33 Additionally, relaxin, a vasodilatory hormone from the corpus luteum, further elevates pressure on lower limb venous valves during pregnancy.29,34–36
Pregnancy induces profound hormonal and hemodynamic changes due to increased progesterone levels, smooth muscle relaxation, expanded plasma volume, and venous compression caused by the gravitational effect of the enlarging uterus. 29 These factors contribute to the onset or worsening of varicose veins. 33 The detection of subtle or atypical manifestations, such as lingual varicosities, may represent an early clinical sign of systemic venous overload and serve as a simple, rapid, and low-cost indicator, as it can be easily assessed during an oral clinical examination. In primary care or prenatal settings, this may function as a risk marker for the development of lower limb varicosities, thereby enabling the implementation of preventive measures.
Pregnancy increases the risk of developing varicose veins in women. 37 Similar varicose vein prevalence in nulliparous women and men 38 highlights pregnancy as a significant risk factor. Pregnant women should adopt preventive measures such as weight control, smoking cessation, regular physical activity, behavioral and postural strategies to avoid prolonged standing or sitting, and the use of compression stockings.39,40 These measures address not only aesthetic concerns but also symptoms like pain, heaviness, itching, and edema in the lower limbs, 41 which impair quality of life. Advanced cases may lead to varicose eczema, hyperpigmentation, and venous ulcers, requiring multidisciplinary treatment. 42
Hormonal changes in pregnancy reduce peripheral vascular resistance, 36 causing hemodynamic shifts that promote varicosities, including in the oral mucosa. Gestational hypertension raises capillary hydrostatic pressure, dilating veins in areas like the sublingual region, and induces endothelial dysfunction and inflammation, worsening vascular function and increasing edema and varicosities. Sublingual varicosities are suggested markers of arterial hypertension, 43 which affects 5%–10% of pregnant women and causes major maternal-fetal morbidity and mortality, including preeclampsia, eclampsia, placental insufficiency, and fetal death. 44 Though little studied in pregnancy, they may be an early visible sign of systemic vascular dysfunction useful for screening gestational hypertension during dental visits.
The presence of lingual varicosities and their potential association with peripheral venous disease remains underexplored in the literature, particularly among pregnant women. The recognition of subtle or atypical signs, such as sublingual varicosities, may have relevant clinical implications, allowing for the early adoption of prophylactic strategies, appropriate physical interventions, or timely referral for specialized vascular follow-up. In this way, the present research may pave the way for the development of new clinical parameters aimed at the early assessment and management of chronic venous disease in the pregnant population.
It is important to highlight that sublingual varicosities occur more frequently in older individuals. However, since the study population in this research consisted exclusively of pregnant women, no participants were of advanced age, which may be considered a limitation in the analysis of this condition. Additionally, the fact that the sample size was calculated for a prevalence study also represents a limitation in terms of investigating the association between sublingual varicosities and lower limb varicosities. Nevertheless, these factors do not invalidate the results.
Based on the findings of this study, it can be concluded that there is an association between lingual varicosities and lower limb varicosities. When identifying such alterations, dental surgeons can contribute to the multidisciplinary team by ensuring timely referral and follow-up of pregnant patients. This integrated approach is essential for the early detection of potential systemic complications and plays a significant role in reducing obstetric risks. The clinical recognition of manifestations such as sublingual varicosities reinforces the need for interdisciplinary protocols that consider oral findings as potential markers of relevant systemic conditions, such as gestational hypertension.
Footnotes
Ethical considerations
The Ethics Review Committee approved our interviews on February 14, 2020. Respondents gave written consent for review and signature before starting interviews.
Consent to participate
All participants provided written informed consent prior to participation.
Consent for publication
Written informed consent for publication was obtained from all participants (or from a legally authorized representative) and identifying details have been omitted to preserve confidentiality.
Author contributions
O.A.S.J. conceptualization, methodology, validation, supervision, project administration. M.B.R.C. formal analysis, investigation, data Curation, writing – original draft, visualization. A.F.J.A. investigation. C.M. investigation. G.T.G. investigation. S.A.S.M. conceptualization, methodology, validation, writing – original draft, writing – review and editing, supervision, project administration. All authors reviewed and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
We agree with the publication of research data in appropriate repositories, respecting all ethical and legal considerations, to ensure transparency, reproducibility, and the advancement of scientific knowledge.
Guarantor
S.A.S.M. is the guarantor for this article.