
Abstract
Background and aims
Vascular in renal transplant recipients, although uncommon, may pose risks to graft function and patient outcomes. This study investigated the prevalence and characteristics of saphenofemoral junction (SFJ) reflux and lower-limb venous parameters in kidney transplant recipients.
Methods
In this cross-sectional study, patients with a history of kidney transplantation referred to Sina Hospital in Tehran, Iran, from January 2022 to 2024 were included. Duplex ultrasound was used to assess the presence of SFJ reflux, SFJ reflux time, and the diameters of the great saphenous vein (GSV), common iliac vein, external iliac vein, and common femoral vein.
Results
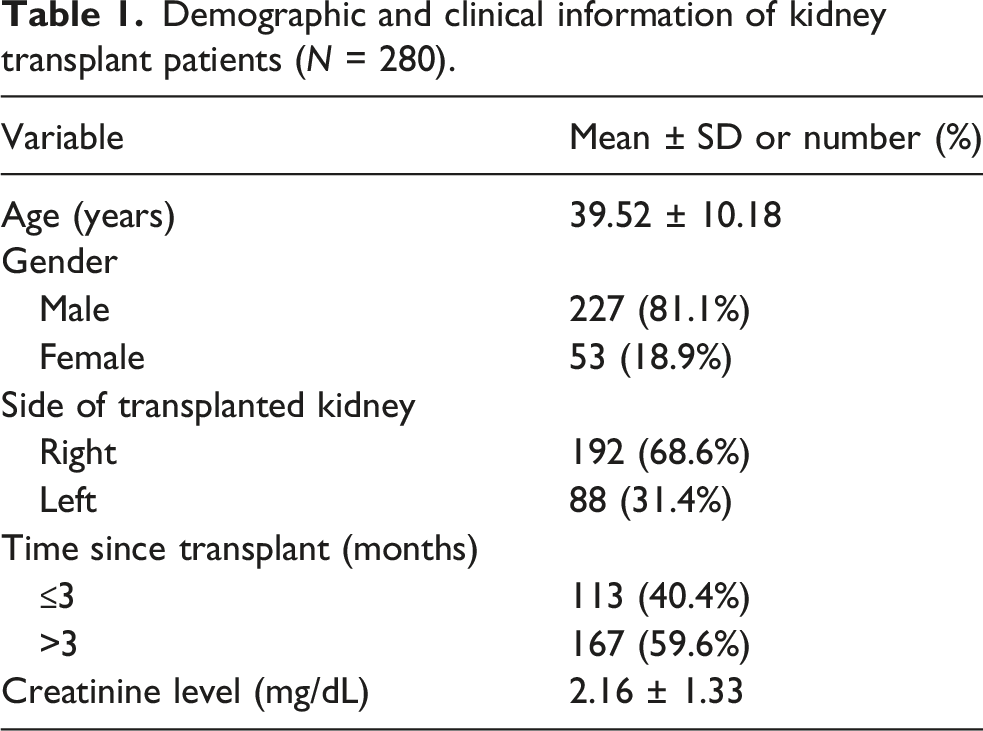
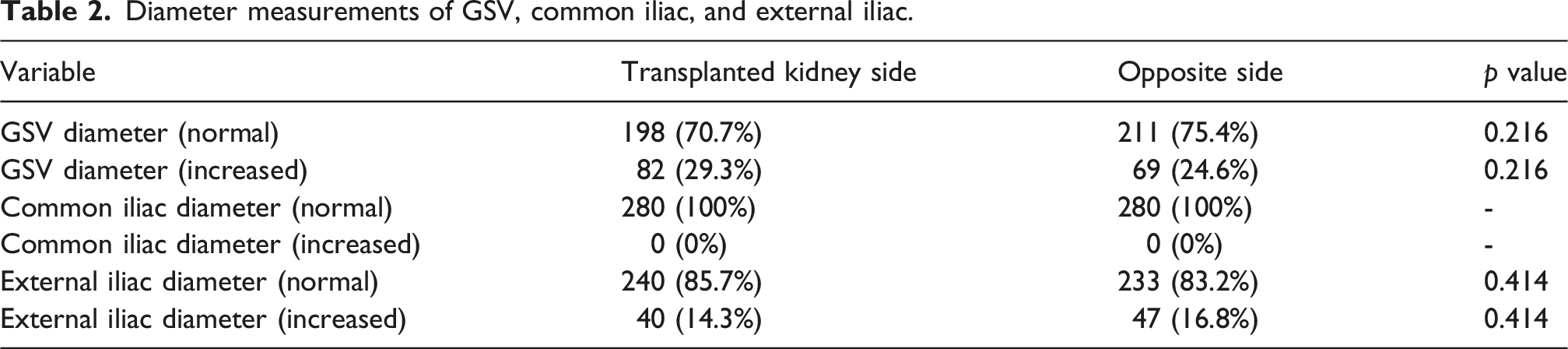
A total of 280 patients were evaluated, with a mean age of 39.52 ± 10.18 years; 227 patients were male (81.1%). The transplanted kidney was located on the right side in 192 patients (68.6%). SFJ reflux was identified in 30 patients (10.7%), of whom 56.7% had bilateral reflux. There was no significant relationship between SFJ reflux and the side of the transplanted kidney (p = 0.273). The GSV diameter was increased in 29.3% of patients on the transplant side and in 24.6% on the contralateral side. The diameters of the common iliac veins were normal in all patients. External iliac vein diameter was increased in 14.3% of patients on the transplant side and in 16.8% on the contralateral side.
Conclusion
SFJ reflux was observed in 10.7% of kidney transplant recipients. No significant association was found between SFJ reflux and the side of the transplanted kidney. Lower-limb venous diameter parameters did not differ significantly between the transplant side and the contralateral side.
Key points
10.7% prevalence of SFJ reflux in kidney transplant patients.
No significant relationship was observed between SFJ reflux and the side of the transplanted kidney.
There were no significant differences in the diameters of the GSV, common iliac, external iliac, and common femoral vein between the lower limbs on the transplanted kidney side and the opposite side.
Introduction
Peripheral vascular disease (PVD) is a significant and often underdiagnosed condition among patients with renal insufficiency and renal transplant recipients. 1 Known cardiovascular risk factors such as diabetes, hypertension, dyslipidemia, and hemodialysis are key risk factors contributing to vascular calcification, which in turn leads to PVD. 2 The presence of PVD is associated with impaired transplant outcomes, particularly due to complications during the anastomosis between the renal artery and the recipient’s iliac artery. 3
In patients undergoing kidney transplantation, the standard procedure involves anastomosing the allograft to the recipient’s iliac vessels. This procedure can be complicated by iliac vessel calcification, which is common in patients with PVD. High-risk patients are typically evaluated preoperatively with imaging of the abdominal iliac artery system to detect potential iliac artery disease. 3 Early vascular complications post-transplantation include renal vein or renal artery thrombotic events, while later complications encompass arterial stenosis, pseudoaneurysms, and arteriovenous fistulas. Duplex ultrasound is the gold standard for diagnosing chronic venous insufficiency and identifying these complications. 4
Vascular disorders are among the most significant post-transplant complications in kidney transplant patients, potentially leading to the loss of the kidney allograft.5–7 Also, acute or chronic renal vein thrombosis can occur, and the latter can cause lower limb varicosis by changing the venous hemodynamics and increased pressure in the lower limb veins following surgery. 8 The manipulation of iliac vessels during transplantation can alter venous return and lead to venous insufficiency, characterized by the dilation of veins and malfunctioning valves. 9
Varicose veins and related symptoms are among the most common chronic vascular disorders of the lower limbs and can significantly affect patients’ quality of life. Treatment of varicose veins has traditionally involved saphenofemoral and saphenopopliteal junction ligation with or without vein stripping, which has been a mainstay of patient care. 10 Patients with varicose veins may be asymptomatic or may present with symptoms such as leg discomfort, heaviness, swelling, and skin changes. Complications may include dermatitis, ankle edema, spontaneous bleeding, superficial thrombophlebitis, lipodermatosclerosis, and ulceration. 11
Saphenofemoral junction (SFJ) reflux is a condition in which the valve at the junction between the great saphenous vein (GSV) and the femoral vein fails, leading to retrograde blood flow and venous insufficiency. The GSV, the longest vein in the body, plays an important role in venous drainage of the lower limb. Its diameter, as well as the diameters of the common iliac, external iliac, and common femoral veins, can be useful indicators of venous status. 12 Changes in the diameters of these vessels, particularly dilation or narrowing, can affect blood flow dynamics and contribute to complications such as varicose veins. 13
Given the high prevalence of kidney transplantation and the potential for postoperative vascular disorders, as well as the burden of venous insufficiency associated with acquired factors such as prolonged standing or sitting, reduced physical activity, obesity, and aging, evaluation of SFJ reflux and varicose veins in kidney transplant patients may be clinically relevant. This study aimed to explore the relationship between SFJ reflux on the side of the transplanted kidney versus the opposite side. We investigated whether manipulation of the iliac vessels in kidney transplant patients was associated with an increased likelihood of SFJ reflux and varicose veins in the lower limb on the side of the transplanted kidney.
Methods and materials
Study design and population
This cross-sectional study was conducted at a tertiary university hospital in Iran, from January 2022 to 2024. The study was approved by the local ethics committee ([blinded for peer review]). Written informed consent was obtained from all participants, ensuring compliance with ethical standards for medical research and the Declaration of Helsinki.
Data were collected from kidney transplant patients who visited the radiology department for routine check-ups during the study period. The study included all adult kidney transplant recipients who consented to participate and met the inclusion criteria. Patients with a history of kidney transplant rejection, lower limb amputation, chronic venous insufficiency, stent placement in the lower limb, femoral arteriovenous fistula, significant vascular damage during surgery, or suspected/confirmed deep venous thrombosis were excluded.
Sample size
A pilot study involving Doppler ultrasound analysis of 21 randomly selected patients revealed a 9.5% prevalence of SFJ reflux. Using a confidence level of 95% and a statistical power of 80%, we determined a required sample size of 280 patients. Participants were selected using an available sampling method.
Data collection
Collected data included demographic information (age, gender), clinical details (time since transplant, side of transplanted kidney, serum creatinine level), and ultrasound findings (resistive index of the transplanted kidney, color Doppler and grayscale ultrasound parameters).
Ultrasound evaluation
A radiologist performed ultrasound evaluations using color Doppler and grayscale imaging. The following parameters were assessed bilaterally: • Presence and duration of SFJ reflux • Proximal diameter of the GSV post-valve • Diameter of the common femoral, common iliac, and external iliac arteries and veins
The diameters of the common iliac and external iliac arteries were categorized as normal or increased (aneurysmal). A common iliac artery diameter >18 mm in men and >15 mm in women, 14 and an external iliac artery diameter >10 mm were classified as aneurysmal. 15 An average GSV diameter of 5 mm was considered normal.
Statistical analysis
Data were analyzed using SPSS version 25. Descriptive statistics summarized using means, standard deviations, counts, and percentages. Comparative analyses of ultrasound findings between the transplanted and contralateral sides were conducted using t-tests, Chi-Square tests, and Fisher’s Exact tests. Statistical significance was set at p < 0.05.
Results
Demographic and clinical information of kidney transplant patients (N = 280).
Diameter measurements of GSV, common iliac, and external iliac.
Saphenous-femoral junction reflux (SFJ) and other measurements.

The mean ± standard deviation of diameters of GSV, common iliac, external iliac, and common femoral veins in the transplant site and the contralateral side.

SFJ reflux was identified in 30 patients (10.7%), with 56.7% showing reflux bilaterally and 43.3% unilaterally (predominantly on the side of the transplanted kidney in 84.6% of unilateral cases). No significant association was found between SFJ reflux and the side of the transplanted kidney (p-value = 0.273) (Table 3). In all cases where SFJ reflux was detected, the reflux time exceeded 500 milliseconds.
There were no statistically significant differences observed in GSV, common iliac vein, external iliac veins, and common femoral veins diameters between the lower limbs on the transplanted kidney side and the opposite side (all p-value >0.05) (Table 4).
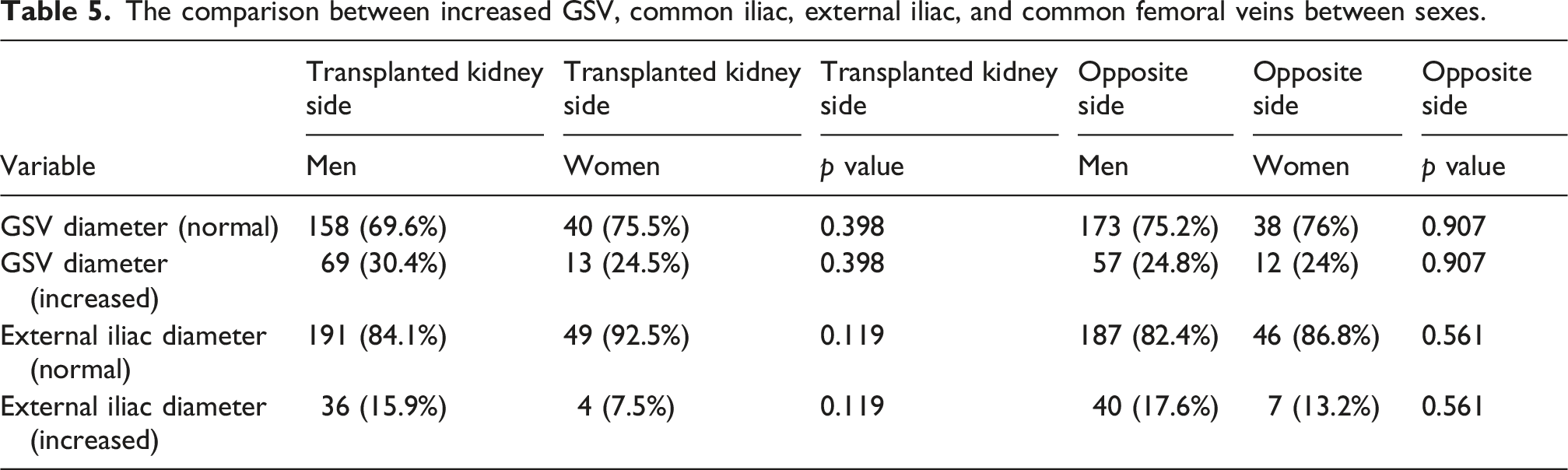
The comparison between increased GSV, common iliac, external iliac, and common femoral veins between sexes.
Age comparison and diameter measurements.

Comparison of diameter measurements with creatinine levels.

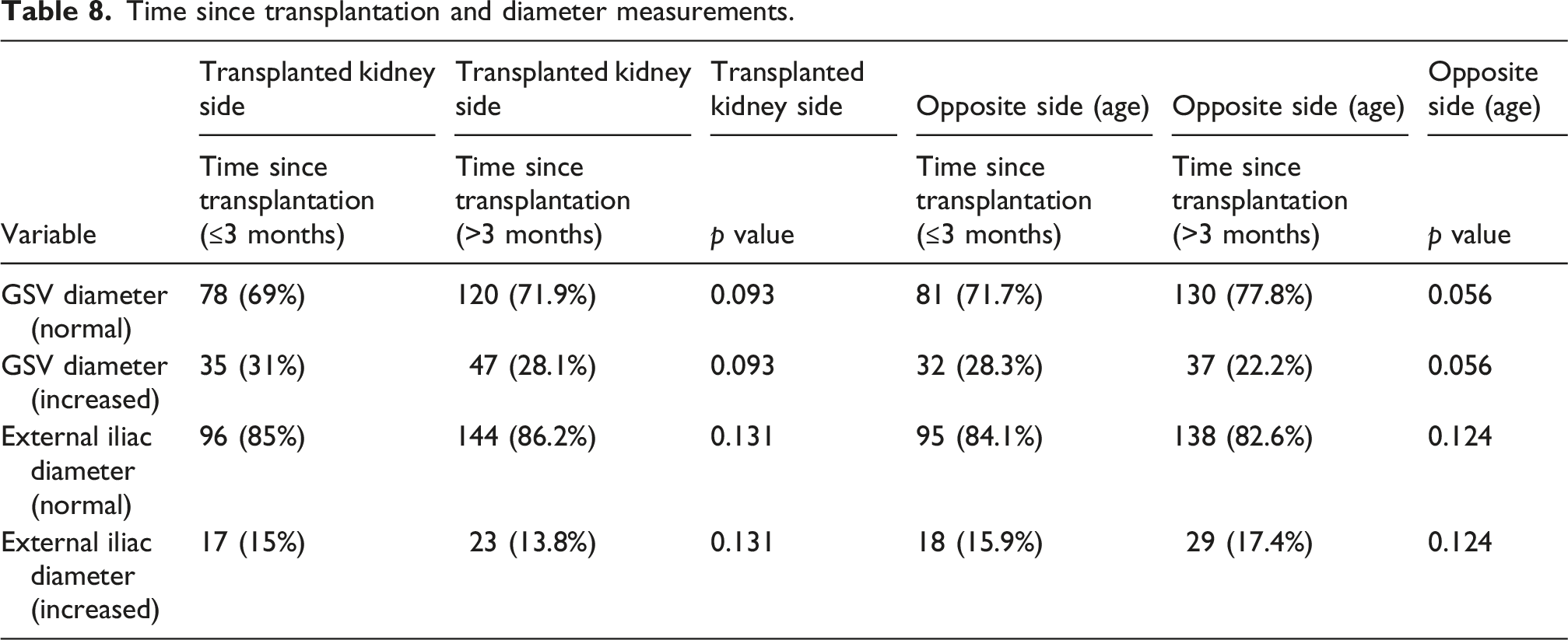
Time since transplantation and diameter measurements.
Diameter comparisons and SFJ reflux presence.

Discussion
This study showed a relatively low prevalence of SFJ reflux, observed in 10.7% of kidney transplant patients. Notably, there was no significant difference in the prevalence of SFJ reflux between the lower limb on the transplanted kidney side and the opposite side. Additionally, we found no significant differences in the diameters of the GSV, common iliac vein, external iliac vein, and common femoral vein between the two sides. These findings suggest that kidney transplantation was not associated with measurable differences in the evaluated lower-limb venous reflux or venous diameter parameters between the transplant side and the contralateral side in this cross-sectional cohort. Because most previous reports have focused on arterial or graft-related vascular complications, data specifically comparing SFJ reflux and lower-limb venous diameters between the transplant side and the contralateral side are limited.
Although the incidence of vascular complications after transplantation is not high, clinically significant arterial or venous complications may adversely affect graft function or patient outcomes. Recognition of clinically significant post-transplant vascular complications remains important, particularly in symptomatic patients. Vascular complications have been reported in 1 to 23% of kidney transplant recipients. 16 In the current era of optimizing postoperative recovery and reducing hospital complications, it is useful to determine the incidence and characteristics of these vascular complications.
To our knowledge, this topic has not been explored in depth. In a 2015 study by Alexander et al., it was reported that changes in perfusion in the limb on the same side as the transplant were not significantly different from changes in the opposite limb. 17 Aktas et al. (2011) documented 47 vascular complications (2.55%) in kidney transplant recipients, with renal artery stenosis, renal allograft artery kinking, renal vein kinking, and renal artery thrombosis being the most common. 18 Another study indicated that SFJ incompetence was observed in fewer than half of the legs with proximal GSV reflux at the SFJ. In more than half of the cases, the cause of the reflux was drainage of the proximal GSV from distal tributaries. 19
Superficial venous drainage from the lower anterior abdominal wall into the proximal GSV is via the superficial epigastric veins, superficial iliac circumflex veins, and superficial external pudendal veins. Multiple veins from the upper thigh also drain into the proximal GSV. In a standing position, the natural direction of flow in these veins is downward. When the GSV is incompetent, it drains into the distal GSV, contributing to reflux. 19
In Cappelli et al.'s study, the recurrence in patients who underwent ligation of the SFJ tributaries was attributed to the pressure overload from the lack of drainage in the GSV at the ligated tributary, which potentially serves as a stimulus for venous inflammation and disease progression. 19
Chronic venous insufficiency patients often exhibit venous hemodynamic disturbances correlated with clinical severity. Our study investigated whether the vein diameter at SFJ in the lower limb on the transplanted kidney side and the opposite side could indicate hemodynamic impairment. We found no significant differences in the diameters of the GSV, common iliac, external iliac, and common femoral vein between the lower limbs on the transplanted kidney side and the opposite side. 20
Mendoza et al. explored the relationship between GSV diameters measured at the SFJ and proximal thigh to assess venous impairment, concluding that measurements in the proximal thigh are more accurate and have higher sensitivity and specificity for predicting reflux and classifying venous disease. They noted that GSV reflux in the groin is challenging to assess due to the shape of the vein being influenced by the confluence of the epigastric, pudendal, tributary veins, and aneurysmal dilation from deep vein reflux, making groin measurements less reliable. 21
Navarro et al. demonstrated that measuring GSV diameter helps identify patients with clinically relevant venous hemodynamic impairment. 22 Choi et al. found a correlation between GSV diameter in venography and reflux in duplex ultrasound in patients with varicose veins, with a cutoff of 5.880 mm being predictive of preoperative reflux. 23 Similarly, other studies have shown that reflux detected in preoperative duplex ultrasound indicates an increased GSV diameter.24–26
This study had several limitations. The precise anatomic location and branching pattern of the SFJ were not evaluated. Given that previous studies have demonstrated variability in SFJ anatomy and the importance of tributary management in surgical outcomes and recurrence, future studies should consider detailed SFJ reflux patterns. Another limitation was the lack of assessment of clinical manifestations in patients with and without SFJ reflux. In addition, the cross-sectional design limits causal interpretation, and longitudinal studies with longer follow-up are needed to examine vascular complications in kidney transplant patients with SFJ reflux.
Finally, pre-transplant lower-limb vascular data were not available. Therefore, a study comparing ultrasound findings before and after transplantation would provide a more accurate assessment of potential transplant-related vascular changes.
Conclusion
Our study demonstrated a 10.7% prevalence of SFJ reflux in kidney transplant patients. No significant relationship was observed between the presence of SFJ reflux and the side of the transplanted kidney. Additionally, there were no significant differences in the diameters of the GSV, common iliac, external iliac, and common femoral vein between the lower limbs on the transplanted kidney side and the opposite side. Overall, these findings suggest that kidney transplantation may not substantially affect the evaluated lower-limb venous parameters on the side of transplantation compared with the contralateral side.
Footnotes
Ethical considerations
Ethical approval was obtained (IR.TUMS.SINAHOSPITAL.REC.1402.105). The study was conducted in accordance with the Declaration of Helsinki.
Author contributions
SM, FZB, FT, HA, GM, HR, ZB, and OT contributed to the conception and design of the study, data acquisition, and analysis and interpretation. SM and FT drafted the manuscript. All authors critically revised the manuscript for important intellectual content, approved the final version, and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Transparency statement
The study was approved by the local ethics committee ([blinded for peer review]). Written informed consent was obtained from all participants, ensuring compliance with ethical standards for medical research and the Declaration of Helsinki.
Guarantor
FT.