
Abstract
Objectives
Chronic refractory lower-extremity edema often remains undiagnosed despite standard evaluations that focus primarily on excluding deep vein thrombosis. We aimed to elucidate the underlying etiologies and assess the utility of a comprehensive, structured diagnostic protocol.
Methods
We retrospectively analyzed a prospectively enrolled, referral-based cohort of 58 patients with chronic refractory lower- extremity edema who underwent a structured multimodal diagnostic protocol after failure of standard noninvasive evaluation. Etiologies were classified as non-thrombotic iliac vein lesions, pulmonary hypertension, superficial venous insufficiency, or multifactorial.
Results
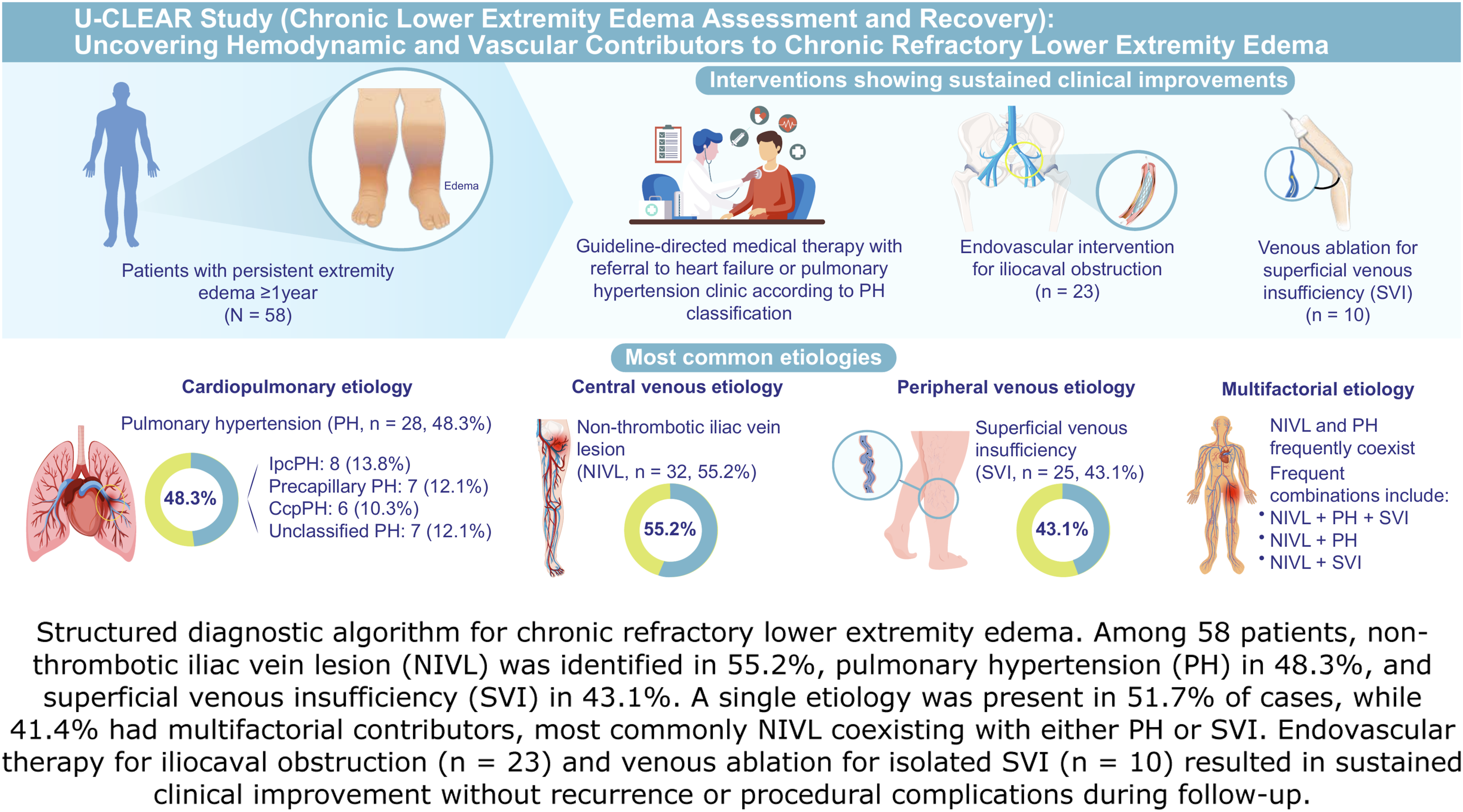
Non-thrombotic iliac vein lesions, pulmonary hypertension, and superficial venous insufficiency were identified in 55.2%, 48.3%, and 43.1% of patients, respectively. Single etiologies accounted for 51.7% of cases, 41.4% were multifactorial, and 6.9% remained unclassified. Among pulmonary hypertension cases, isolated postcapillary pulmonary hypertension associated with heart failure with preserved ejection fraction was the most common (13.8%). Superficial venous insufficiency was the sole cause in 12.1% of cases, while in others, it coexisted with non-thrombotic iliac vein lesions or pulmonary hypertension. Interventions included iliocaval endovascular therapy (n = 23) and saphenous vein ablation (n = 10), with the remainder receiving conservative therapy. Over a median follow-up of 2.98 years, 86.2% of patients achieved objective clinical improvement.
Conclusions
This protocol reduced the number of repeated low-yield ultrasound examinations and facilitated targeted treatment. A structured diagnostic protocol integrating duplex ultrasonography, invasive hemodynamic testing, and intravascular imaging enables accurate etiologic classification of chronic refractory lower extremity edema. This approach identifies treatable contributors, supports tailored interventions, and may improve outcomes while reducing unnecessary testing.
Keywords
Introduction
Chronic lower-extremity edema is a common clinical presentation. Despite conservative treatment, some patients experience persistent edema that progressively worsens, leading to complications such as cutaneous fibrosis, stasis dermatitis, venous ulcers, and cellulitis, all of which substantially impair quality of life.1–7 Peripheral edema occurs in up to 20–30% of older adults, with a subset of these individuals experiencing persistent, treatment-refractory symptoms. 1
Chronic refractory lower extremity edema, defined as persistent swelling that is unresponsive to standard treatments, poses ongoing diagnostic and therapeutic challenges. Patients with chronic refractory lower extremity edema frequently undergo repeated duplex ultrasonography, are prescribed nonspecific medications that may cause adverse effects, and often present to emergency departments with recurrent symptoms, such as painful erythematous swelling, prompting evaluation for deep vein thrombosis (DVT) or cellulitis. Despite these efforts, the underlying etiology often remains undetermined.8–10
Venous hypertension due to structural and functional abnormalities is a major contributor to chronic lower-extremity edema. Structural contributors include valvular reflux, venous outflow obstruction, and post-thrombotic changes. In contrast, functional factors include elevated central venous pressure, impaired calf muscle pump function, and lymphatic insufficiency.3–7,11 The mechanisms facilitating venous return from the lower extremities—including the cardiopulmonary pump, venous valves, and calf muscle pump—play central roles in maintaining venous pressure, and impairment of these mechanisms leads to chronic venous hypertension.3–7 Sustained venous hypertension induces endothelial dysfunction, increased vascular permeability, and chronic inflammation at the microvascular level, resulting in tissue injury and clinical manifestations such as varicosities, stasis dermatitis, lipodermatosclerosis, and venous ulcers.6,7,12,13 In contrast to the traditional Starling model, net interstitial fluid clearance occurs predominantly via the lymphatic system rather than capillary reabsorption. Therefore, persistent edema reflects an imbalance between increased capillary filtration and insufficient lymphatic drainage.14,15 The initial diagnostic evaluation for lower-extremity edema often relies on venous duplex ultrasonography to exclude DVT. Traditional vascular evaluations often do not include reflux testing or assessment of iliocaval obstruction.5–10,16–18 As a result, underlying venous insufficiency and central venous lesions often remain undetected.8–13,19 Recognizing diagnostic blind spots in conventional assessments, we established the Chronic Lower Extremity Edema Program at our institution in 2018. This initiative introduced a structured diagnostic algorithm incorporating both invasive and noninvasive assessments to systematically evaluate chronic refractory edema. The protocol incorporated both reflux testing and dedicated iliocaval duplex ultrasonography performed by an experienced vascular sonographer.
Accordingly, this study focused on a highly selected referral population with chronic refractory disease, in whom conventional diagnostic pathways have failed to identify a clear etiology. This structured protocol was developed specifically for such patients and is not intended to replace the standard first-line diagnostic evaluation. The present study, the UConn Health Chronic Lower Extremity Edema Assessment and Recovery (U-CLEAR), aimed to identify hemodynamic and vascular contributors to chronic refractory lower-extremity edema in patients evaluated through this comprehensive program.
Methods
Patient selection
Patients referred to our interventional cardiology and vascular medicine clinic between May 2018 and February 2023 were screened for enrollment. Eligible patients presented with persistent or recurrent lower extremity edema and associated chronic skin changes despite conservative measures, such as compression stocking therapy (≥20 mmHg), diuretic therapy, exercise, and rehabilitation.
All patients were previously evaluated by physicians to exclude systemic causes of edema. Patients with known internal medicine-related etiologies, including chronic liver disease, chronic kidney disease, and hypothyroidism, were excluded. Patients with clinically diagnosed congestive heart failure or structural heart disease confirmed using echocardiography were also excluded. Venous duplex ultrasonography was performed in all patients to exclude acute DVT.
The duration of edema before referral varied widely, ranging from several months to multiple years. Because many patients were referred after prolonged evaluation elsewhere, precise onset timing was not consistently documented; however, all patients met the criteria for chronic, persistent, treatment-refractory edema. Therefore, this cohort represents a highly selected referral population rather than a general screening sample.
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and approved by the Institutional Review Board of UConn Health (approval number: 20X-253-1). All patients provided written informed consent after being fully informed of the diagnostic and therapeutic procedures involved in the study.
Initial evaluation and patient registration
Edema severity was assessed using a conventional bedside 5-point pitting edema grading scale based on indentation depth and rebound time after standardized digital pressure: Grade 0, no edema; 1+, slight pitting with rapid rebound; 2+, moderate pitting with rebound within ∼15 s; 3+, deep pitting with prolonged rebound; and 4+, very deep pitting with gross swelling and delayed rebound. This semiquantitative scale lacks reliability and reproducibility and was therefore used for baseline characterization only.20,21 Chronic venous disease was classified according to the updated CEAP 2020 classification system: C1 (telangiectasias or reticular veins), C2 (varicose veins), C3 (edema), C4a (pigmentation or eczema), C4b (lipodermatosclerosis or atrophie blanche), C4c (corona phlebectatica), C5 (healed venous ulcer), and C6 (active venous ulcer). 22 For analysis, all C4 subclasses (C4a–C4c) were grouped as C4 to represent chronic skin changes.
Prior medical records, including medication history, laboratory data, echocardiograms, and vascular duplex studies, were reviewed to rule out any previously established etiology. All patients subsequently underwent a structured diagnostic protocol (Figure 1). Structured diagnostic workflow for refractory lower extremity edema. Structured diagnostic workflow for refractory lower extremity edema. The evaluation begins with an outpatient visit and basic laboratory testing, followed by duplex ultrasonography to assess venous reflux and iliofemoral venous anatomy. Comprehensive invasive evaluation, including right heart catheterization, iliocaval venography, and intravascular ultrasound, was then performed via femoral vein access to identify central venous obstruction and cardiopulmonary contributors. IVC = inferior vena cava; IVUS = intravascular ultrasound; RHC = right heart catheterization.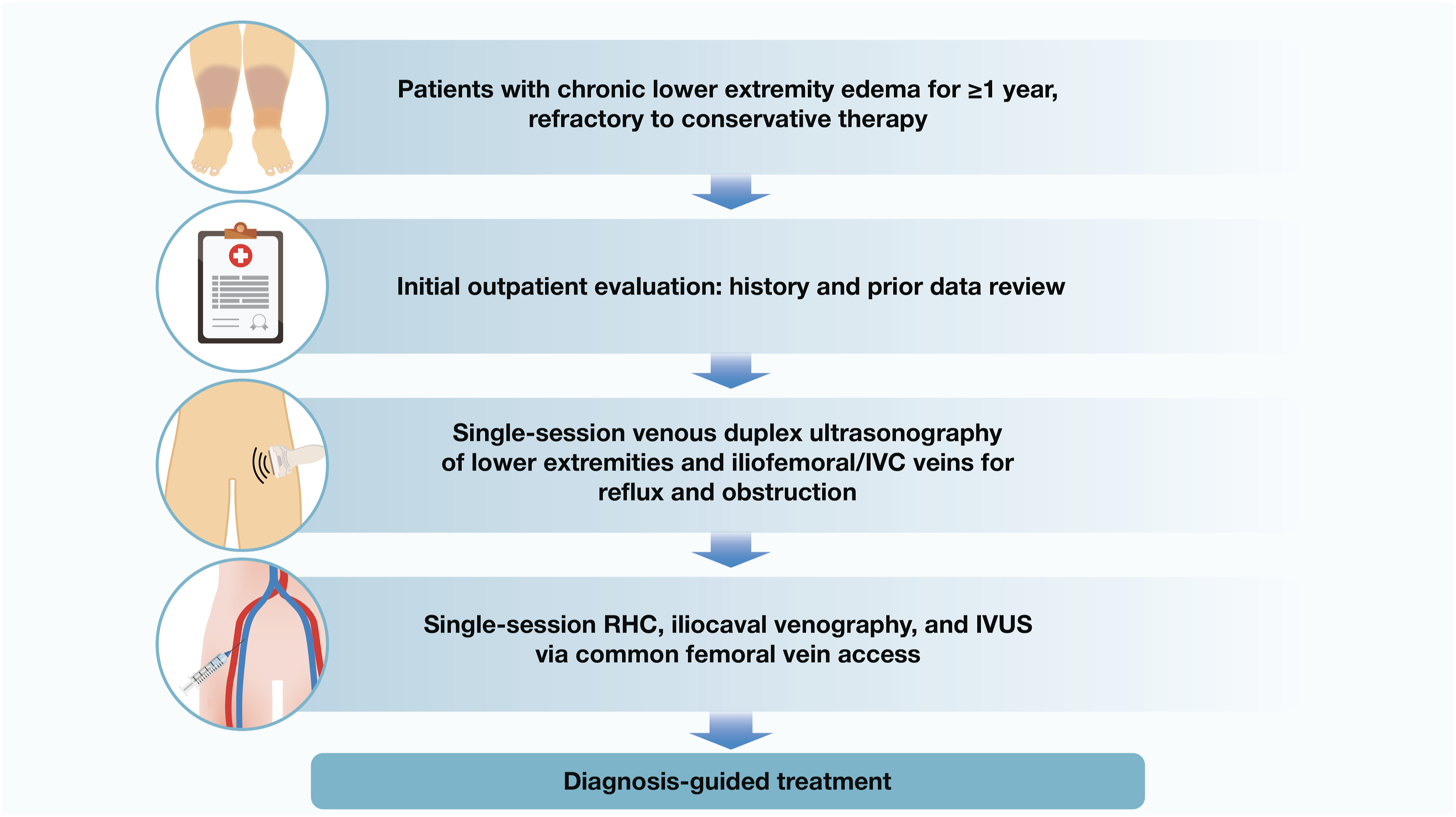
Outpatient noninvasive imaging
All patients underwent lower extremity venous duplex ultrasonography to assess for venous insufficiency and dedicated ultrasonographic evaluation of the iliac veins and inferior vena cava to detect anatomical compression or abnormal Doppler patterns suggestive of central venous obstruction. Standardized protocols were used to evaluate the femoral, popliteal, and saphenous veins.
Venous insufficiency was defined as reflux ≥0.5 s in superficial veins and ≥1.0 s in deep veins. 23 Reflux was assessed with the ultrasound probe positioned over the target vein and provoked by either the Valsalva maneuver or distal limb compression-release techniques, with compression applied distal to the probe.
All studies were conducted by a certified vascular sonographer and reviewed by a cardiologist with expertise in venous imaging.
Invasive hemodynamic and venous assessment
All patients underwent invasive hemodynamic and venous assessments by an experienced interventional team during a single outpatient visit. Right heart catheterization (RHC) via femoral venous access was performed to evaluate the cardiopulmonary causes of venous hypertension. The hemodynamic parameters included mean pulmonary artery pressure (mPAP), pulmonary artery wedge pressure (PAWP), and pulmonary vascular resistance (PVR). Pulmonary hypertension (PH) was defined as mPAP >20 mmHg, according to the 2022 European Society of Cardiology and the European Respiratory Society guidelines.24,25
Based on the hemodynamic abnormality pattern, the patients were categorized into the following groups: (1) isolated postcapillary PH, defined by elevated mPAP and PAWP with normal PVR, suggesting left-sided cardiac involvement; (2) precapillary PH, defined by elevated mPAP and PVR with normal PAWP, typically reflecting pulmonary vascular pathology; (3) combined pre- and postcapillary PH, defined by elevated PAWP and PVR; and (4) unclassified PH, defined by elevated mPAP (>20 mmHg) with low PVR (≤2 Wood units) and PAWP (≤15 mmHg).
Subsequently, iliac vein venography using contrast was performed to assess stenosis, congestion, reflux, or collateral vein formation, followed by intravascular ultrasound (IVUS) to evaluate central venous structures from the common femoral vein to the inferior vena cava. IVUS was performed over a 0.035-inch guidewire using a peripheral IVUS catheter (Philips Volcano, San Diego, CA, USA, or Boston Scientific, Marlborough, MA, USA), which enabled the identification of structural abnormalities consistent with non-thrombotic iliac vein lesions (NIVL), defined as anatomically significant venous outflow obstruction in the absence of prior DVT, including compression stenosis (e.g., May–Thurner syndrome), diffuse narrowing, intraluminal webs, membranous obstructions, and fibrotic changes.26,27 These procedures were conducted safely, with no major complications.
Etiologic classification and treatment strategy
The underlying causes of chronic lower extremity edema were classified into four categories: (1) cardiopulmonary (e.g., PH); (2) central venous obstruction, defined according to the CEAP etiologic classification as secondary causes, including both intravenous (Esi; e.g., post-thrombotic changes) and extravenous (Ese; e.g., nonthrombotic iliac vein lesions [NIVL]) mechanisms; (3) peripheral venous reflux (e.g., superficial venous insufficiency [SVI]); and (4) multifactorial (i.e., a combination of two or more of the above categories).
In the present study, patients with a history of deep vein thrombosis or post-thrombotic changes were excluded; therefore, central venous obstruction predominantly reflected extravenous (Ese) mechanisms, particularly NIVL.
Therapies were tailored to the predominant etiology. Treatment for PH was guided by RHC findings, and patients were referred to specialty clinics for guideline-directed medical therapy.24,25
In cases with multifactorial causes, a stepwise, pathophysiology-guided treatment approach was used. Systemic cardiopulmonary conditions were addressed first, followed by iliocaval venous obstructions and peripheral venous insufficiency, respectively. However, when both cardiopulmonary and central venous abnormalities were detected simultaneously, treatment prioritization was based on which contributor more plausibly explained the patient’s lower extremity edema. In cases where iliocaval obstruction was deemed the predominant driver of symptoms, endovascular intervention was promptly pursued. Conversely, if PH was judged to be the primary etiology, patients were referred to a PH specialty clinic for guideline-directed medical therapy, with iliocaval intervention considered only if edema persisted despite guideline-directed medical therapy.
Treatment decisions for NIVL and SVI are guided by specific anatomical and clinical criteria. For NIVL, intervention was considered when IVUS demonstrated ≥60% venous compression or stenosis, particularly in patients with CEAP class ≥3 (i.e., moderate-to-severe edema, lipodermatosclerosis, or recurrent cellulitis). Procedures were performed only when the treating physician determined that the anatomic lesion was clinically significant and likely contributed to lower extremity symptoms. Treatment involved balloon angioplasty and placement of self-expanding venous stents to restore flow and reduce venous hypertension.11,23
In patients with isolated or predominant SVI, venous ablation was performed using an endovenous radiofrequency technique based on duplex ultrasonographic evidence of substantial saphenous vein reflux (diameter ≥4 mm, reflux duration ≥0.5 s). Ablation was initiated approximately 2 cm distal to the saphenofemoral junction and extended distally, as clinically indicated (Figure 2). Integrated diagnostic and therapeutic framework for refractory lower extremity edema based on pathophysiological mechanisms. Integrated diagnostic and therapeutic framework for refractory lower extremity edema based on pathophysiologic mechanisms. Patients were classified into three major etiologic categories: cardiopulmonary, central venous, and peripheral venous. Cardiopulmonary causes were identified through right heart catheterization (RHC), with patients managed using guideline-directed medical therapy (GDMT) and referred to heart failure (HF) or pulmonary hypertension (PH) clinics as appropriate. Central venous etiologies were assessed using iliocaval venography and intravascular ultrasound (IVUS), with endovascular intervention considered for ≥60% stenosis and supportive clinical findings. Peripheral venous disease was defined by duplex-confirmed superficial venous reflux, with treatment by saphenous vein ablation. Multifactorial contributors were addressed through etiology-directed, multimodal strategies.
Follow-up and clinical assessment
All patients were monitored longitudinally during routine outpatient visits and vascular imaging follow-ups. Symptom improvement was assessed using serial CEAP clinical class documentation. Clinical improvement was defined as a decrease in the CEAP class or regression of edema-related signs (e.g., skin changes, lipodermatosclerosis, or ulceration). In contrast, clinical events were defined as recurrence or persistence of CEAP class ≥C3 after initial improvement, progression to CEAP C4–C6, symptom recurrence confirmed by clinical evaluation, or new reflux on follow-up duplex ultrasonography. Event-free survival was calculated from the date of the initial intervention to the first occurrence of any such event.
In cases of suspected symptom recurrence or clinical deterioration after iliocaval intervention, repeat duplex ultrasonography or contrast venography was performed to assess restenosis or recurrent obstruction.
Patients who underwent venous ablation received short-term outpatient assessment approximately one week after the procedure to evaluate local complications, such as DVT or endothermal heat-induced thrombosis. Follow-up duplex scanning was repeated at 1 month to assess symptom recurrence or residual reflux, and patients were subsequently monitored annually for long-term outcomes.
Results
Baseline characteristics and comorbidities in patients with refractory lower extremity edema.
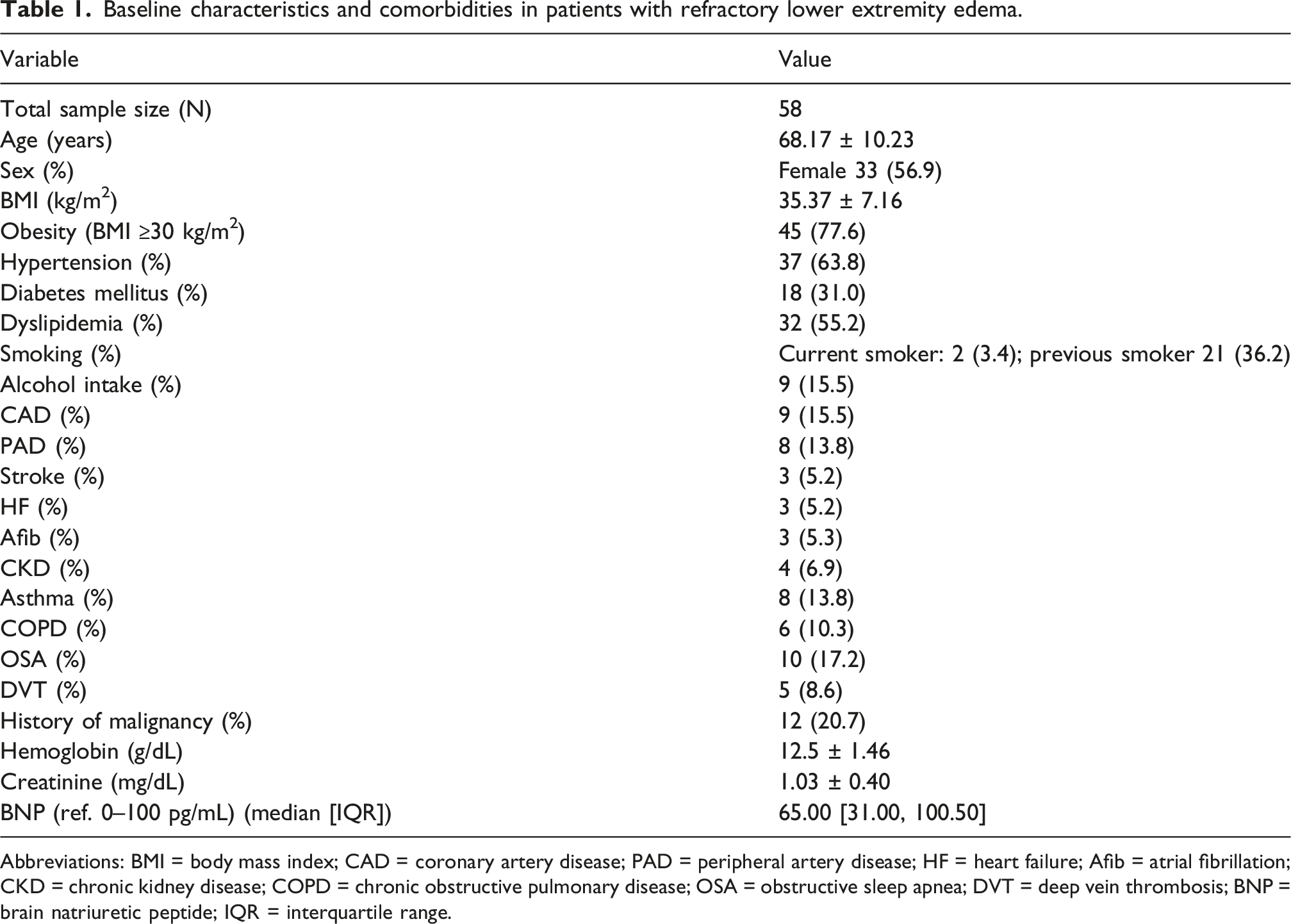
Abbreviations: BMI = body mass index; CAD = coronary artery disease; PAD = peripheral artery disease; HF = heart failure; Afib = atrial fibrillation; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; OSA = obstructive sleep apnea; DVT = deep vein thrombosis; BNP = brain natriuretic peptide; IQR = interquartile range.
Etiologic distribution and classification
Overall, NIVL was the most frequently identified contributor (n = 32, 55.2%), followed by PH (n = 28, 48.3%) and SVI (n = 25, 43.1%) (Figure 3). In this cohort, central venous obstruction predominantly reflected extravenous (Ese) mechanisms, and patients with post-thrombotic (Esi) disease were excluded. Among those with PH (n = 28), subclassification based on invasive hemodynamic assessment revealed isolated postcapillary PH in eight patients (13.8%), precapillary PH in seven (12.1%), combined pre- and postcapillary PH in six (10.3%), and unclassified PH in seven (12.1%). As many patients had overlapping conditions, these proportions reflected both isolated and coexisting etiologies. (a) Proportional contribution of major etiologies and PH classification. (b) Classification of chronic refractory lower extremity edema by combined etiologies of NIVL, PH and SVI. Etiologic distribution and combined contributors to chronic refractory lower extremity edema. (A) Proportional distribution of major etiologies and pulmonary hypertension (PH) subtypes. Among 58 patients with chronic refractory lower extremity edema, the most common etiologies were non-thrombotic iliac vein lesion (NIVL, 55.2%), PH (48.3%), and superficial venous insufficiency (SVI, 43.1%). PH was further classified by hemodynamic phenotype according to the 2022 European Society of Cardiology/European Respiratory Society guidelines: isolated postcapillary PH (IpcPH, 13.8%), precapillary PH (12.1%), combined post- and precapillary PH (CpcPH, 10.3%), and unclassified PH (12.1%). (B) Combined etiology classification of chronic refractory lower extremity edema. Etiologic assessment revealed that 51.7% of patients had a single identifiable cause, while 41.4% had multifactorial contributors. The most frequent overlapping etiologies were NIVL+PH+SVI (12.1%), NIVL+PH (10.3%), NIVL+SVI (10.3%), and SVI+PH (8.6%). Isolated contributions included NIVL (22.4%), PH (17.2%), and SVI (12.1%). Unknown etiology was observed in 6.9%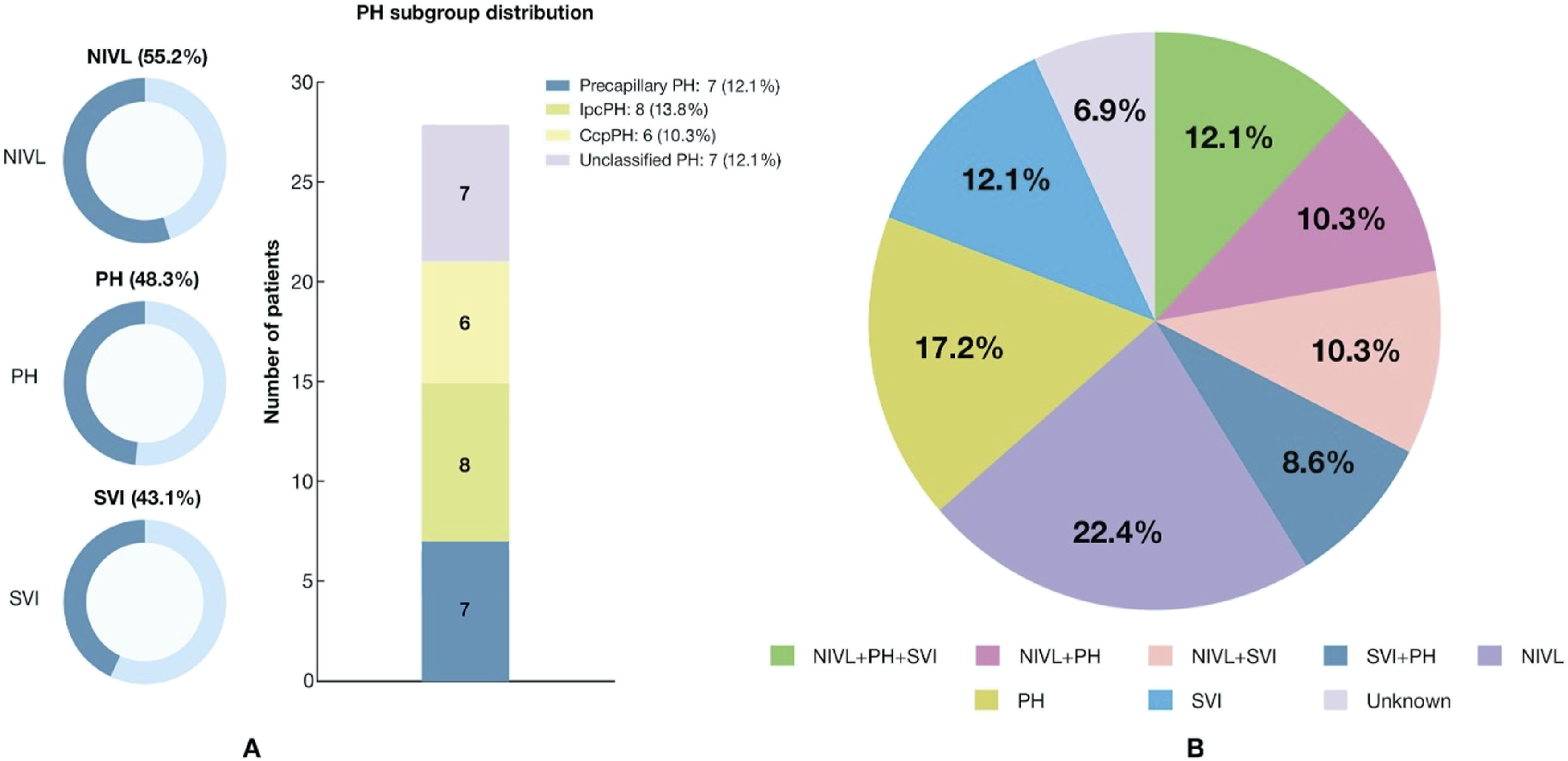
The laterality of edema varied across the cohort, with unilateral edema observed in 19 patients (32.8%) and bilateral edema in 39 patients (67.2%). Unilateral edema was more commonly associated with central venous obstruction, whereas bilateral edema was more frequently observed in cardiopulmonary or multifactorial etiologies.
Diagnostic findings and follow-up outcomes in patients with refractory lower extremity edema.
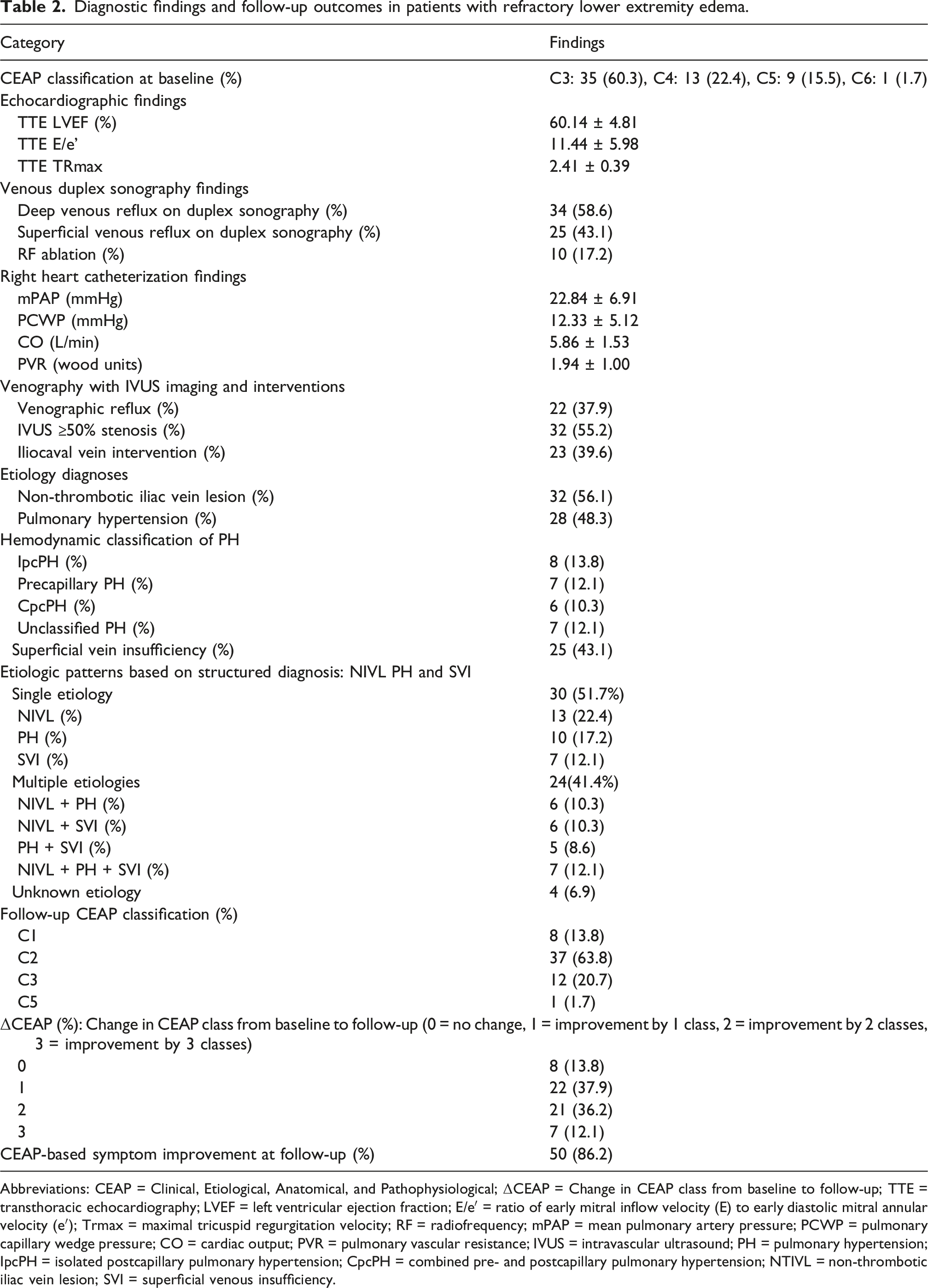
Abbreviations: CEAP = Clinical, Etiological, Anatomical, and Pathophysiological; ΔCEAP = Change in CEAP class from baseline to follow-up; TTE = transthoracic echocardiography; LVEF = left ventricular ejection fraction; E/e′ = ratio of early mitral inflow velocity (E) to early diastolic mitral annular velocity (e′); Trmax = maximal tricuspid regurgitation velocity; RF = radiofrequency; mPAP = mean pulmonary artery pressure; PCWP = pulmonary capillary wedge pressure; CO = cardiac output; PVR = pulmonary vascular resistance; IVUS = intravascular ultrasound; PH = pulmonary hypertension; IpcPH = isolated postcapillary pulmonary hypertension; CpcPH = combined pre- and postcapillary pulmonary hypertension; NTIVL = non-thrombotic iliac vein lesion; SVI = superficial venous insufficiency.
Clinical outcomes stratified by treatment
Based on the predominant pathophysiology, 23 patients underwent iliocaval intervention, 10 underwent venous ablation, and 28 were managed conservatively in the relevant specialty clinics (e.g., PH, heart failure, and cardiovascular medicine). In three patients with coexisting NIVL and SVI, iliocaval intervention was followed by venous ablation due to persistent superficial reflux; these patients were included in both groups for outcome analysis. In the conservative treatment group (n = 28), 23 patients (82.1%) demonstrated objective improvement (ΔCEAP ≥1) accompanied by symptomatic relief, whereas the remaining five patients (17.9%) showed only minimal change without clinically meaningful improvement.
Among the 23 patients who underwent iliocaval intervention, 21 (91.3%) showed sustained improvement in edema and CEAP class. Two patients experienced restenosis requiring reintervention at 12 and 36 months, yielding event-free survival rates of 95.7% at 1 year and 91.3% at 3 years.
Comparative summary of diagnostic etiologies, CEAP progression, and treatment outcomes by management strategy.
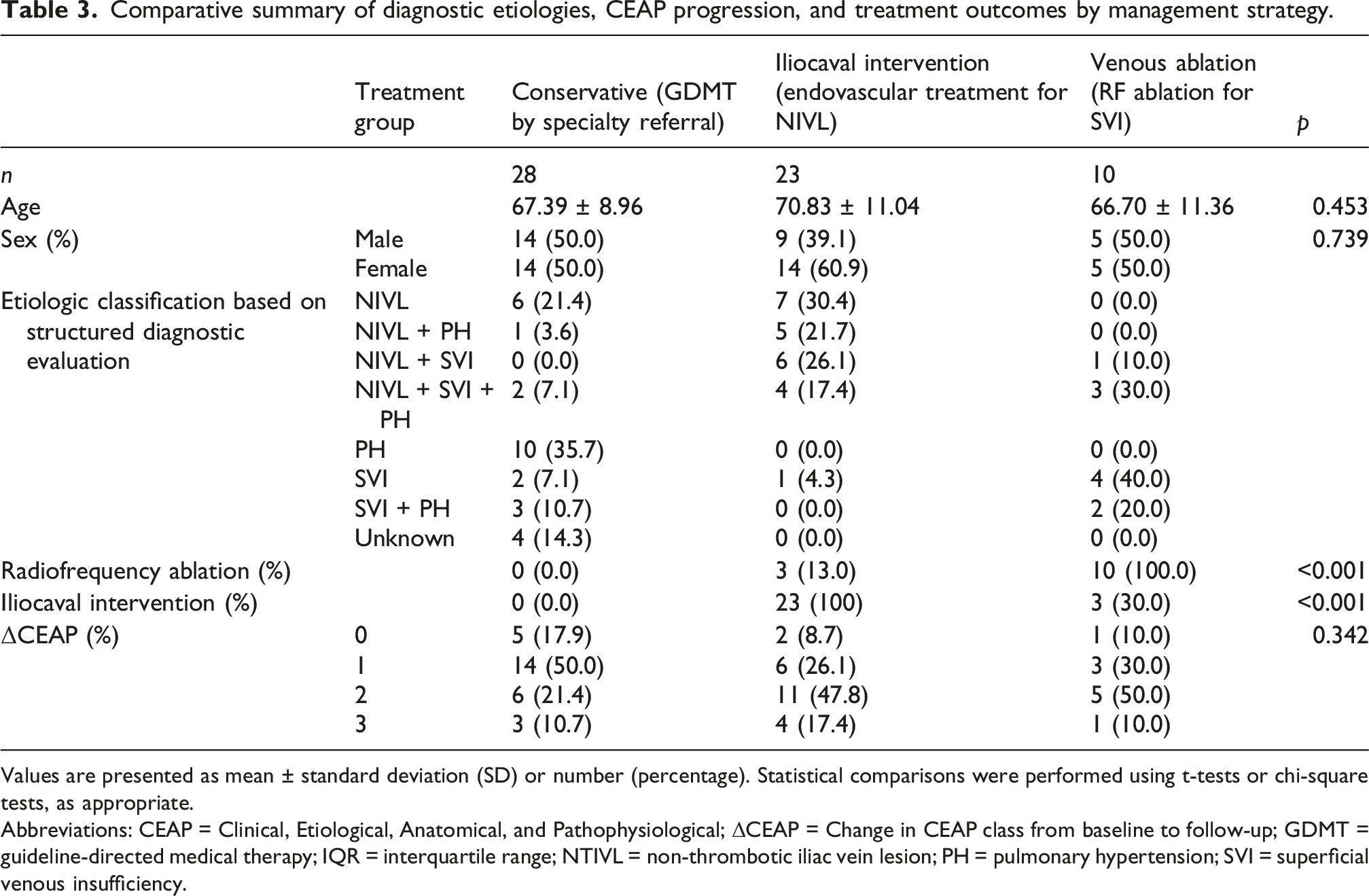
Values are presented as mean ± standard deviation (SD) or number (percentage). Statistical comparisons were performed using t-tests or chi-square tests, as appropriate.
Abbreviations: CEAP = Clinical, Etiological, Anatomical, and Pathophysiological; ΔCEAP = Change in CEAP class from baseline to follow-up; GDMT = guideline-directed medical therapy; IQR = interquartile range; NTIVL = non-thrombotic iliac vein lesion; PH = pulmonary hypertension; SVI = superficial venous insufficiency.
Outcomes of the iliocaval intervention subgroup
Among the 32 patients with ≥50% iliac vein stenosis on IVUS, 23 underwent endovascular treatment based on the presence of ≥60% luminal narrowing and significant clinical symptoms, such as grade ≥3 edema, lipodermatosclerosis, or recurrent cellulitis.
Most patients had extrinsic iliac vein compression, with a mean stenosis severity of 67.6%, with left-sided lesions in 10 patients, right-sided lesions in nine, and bilateral lesions in two. Eleven cases met the criteria for classic May–Thurner syndrome, whereas eight showed atypical compression patterns, including right iliac vein compression or nonvascular external compression. Notably, three cases were associated with unusual extrinsic causes, such as a lumbar vertebral bony spur, a pelvic mass (endometrial cancer), or a transplanted kidney.
One patient with a membranous web in the infrahepatic inferior vena cava was treated with balloon angioplasty without stenting. Overall, the iliocaval intervention group demonstrated durable improvement, with low rates of restenosis and no major complications.
Outcomes of the venous ablation subgroup
In total, 10 patients with isolated SVI underwent endovenous radiofrequency ablation of incompetent veins in an outpatient setting. Follow-up included duplex ultrasonography at 1 month to confirm ablation success and annual clinical and imaging evaluations thereafter. Although one patient experienced limited symptomatic improvement, no recurrent venous reflux or procedural site complications were observed in any patient, indicating durable anatomical and technical success. Event-free survival was 100% at both 1 and 3 years.
Discussion
This study demonstrates the clinical utility of a comprehensive pathophysiology-guided diagnostic protocol for chronic refractory lower-extremity edema. By integrating duplex ultrasonography with reflux testing, right heart catheterization, and iliocaval imaging using IVUS, the protocol reduced unnecessary repeat diagnostic studies and, more importantly, enabled etiology-specific treatment, resulting in meaningful and sustained clinical improvement in this challenging patient population.
From a pathophysiological perspective, a contemporary understanding of microvascular fluid exchange indicates that interstitial fluid clearance occurs predominantly via the lymphatic system rather than capillary reabsorption. Accordingly, chronic edema reflects an imbalance between increased capillary filtration and insufficient lymphatic drainage capacity. In this context, the hemodynamic abnormalities identified in our cohort, such as venous hypertension and cardiopulmonary dysfunction, are likely to contribute primarily by increasing capillary filtration rather than altering fluid resorption.
Importantly, this diagnostic framework is intended for selected patients with chronic refractory edema after standard noninvasive evaluation has failed, rather than for routine assessment of all patients presenting with lower extremity swelling.
NIVL was the most frequent finding (55.2%), underscoring that central venous obstruction is often under-recognized in patients with refractory lower extremity edema. Importantly, the presence of NIVL did not mandate intervention. Iliocaval stenting was not performed routinely based on imaging findings alone. Intervention was reserved for patients with ≥60% stenosis and compatible clinical features, acknowledging that narrowing observed on IVUS may reflect physiological or positional changes rather than true obstruction.13,23,28 Accordingly, these criteria were intentionally conservative to avoid overtreatment. Among the treated patients, procedural surveillance over 3 years showed a persistently high event-free rate, supporting the long-term safety and efficacy of iliocaval intervention in appropriately selected cases.
PH was identified in nearly half of the cohort and was most commonly isolated postcapillary PH related to HFpEF (13.8%). Right heart catheterization enables precise hemodynamic classification, revealing diverse cardiopulmonary disorders that are often not clinically apparent. Given the systemic nature of these conditions, management required a multidisciplinary approach involving cardiology, pulmonology, and vascular medicine, ensuring accurate diagnosis and classification-specific, guideline-directed therapy, with sustained symptom control in refractory edema.29,30
SVI occurred in 43.1% of the patients and was the sole or dominant cause in 12.1%. Incorporating targeted reflux testing and extending duplex ultrasonography to evaluate iliocaval lesions overcomes the limitations of conventional studies that focus solely on excluding DVT. This broader diagnostic approach facilitated the detection of SVI even in multifactorial diseases. When SVI was the only or predominant cause, venous ablation achieved long-term symptom relief.
Unclassified cases (6.9%) may reflect mechanisms not assessed, such as lymphatic dysfunction, muscle pump impairment, or microvascular leakage.14,15
The absence of dedicated lymphatic imaging is an important limitation that may have contributed to residual unexplained edema in a subset of patients. Nevertheless, the relatively low proportion of unclassified cases compared with prior reports suggests that the structured, multimodality evaluation improved the diagnostic yield and reduced the number of patients labeled as having idiopathic edema.
Limitations
This study had several limitations that merit consideration. First, this was a retrospective, single-center study involving a referral-based population, introducing inherent selection bias and limiting the estimation of disease prevalence. The total number of patients with lower extremity edema evaluated in general practice during the study period was not systematically captured.
Second, the duration of edema before referral was heterogeneous and not uniformly documented. Nevertheless, all included patients shared the defining feature of persistent treatment-refractory edema, which was the primary determinant for advanced diagnostic evaluation.
Third, this study was not powered to evaluate differential treatment responses based on edema duration, baseline severity, or comorbidity burden. Accordingly, treatment outcomes were assessed using objective clinical improvement rather than stratified predictors of response, and these findings should be considered hypothesis-generating. Future prospective studies are required to identify predictors of response and refine the patient selection criteria.
Fourth, the etiologic classification was based on a structured diagnostic framework aligned with the CEAP classification; however, patients with prior deep vein thrombosis or post-thrombotic changes (Esi) were excluded by design. Therefore, central venous obstruction in this study predominantly reflected extravenous (Ese) mechanisms, particularly nonthrombotic iliac vein lesions, which may limit the generalizability to broader populations with secondary venous disease. In addition, lymphatic function was not directly assessed despite its central role in interstitial fluid clearance in chronic edema. Finally, edema severity was evaluated using a semiquantitative bedside grading scale, which is subject to inter-observer variability and limited reproducibility, and was therefore used primarily for baseline characterization rather than as a primary outcome measure.
Footnotes
Ethical considerations
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and was approved by the Institutional Review Board of UConn Health (approval number: 20X-253-1).
Consent to participate
All patients provided written informed consent after being fully informed about the diagnostic and therapeutic procedures involved in the study.
Author contributions
The study concept and patient cohort originated under the care of Juyong Lee, who served as the guarantor and corresponding author. Kyutae Park performed retrospective data analysis and manuscript drafting and served as first author. Srinivas Nadadur contributed to the initial study concept, and Sungmin Lim subsequently expanded data collection and organization. Debapria Das, Khagendra Dahal, Agnes S. Kim, Patrick Corcoran, Michael A. Azrin reviewed and revised the manuscript for intellectual content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
Please kindly note that an abstract based on this study has been submitted to the American Heart Association (AHA) 2025 Scientific Sessions (Control ID: 4341605).
In addition,preliminary findings from this work were presented as
Lee J, Nadadur S, Srinivas. Chronic Refractory Leg Edema Requires Multimodality Investigation Due to Undiagnosed Etiologies. American Venous Forum (AVF) 2022 Annual Meeting, February 23–26, 2022, Florida, USA. This manuscript has not been previously published and is not under consideration elsewhere.
Guarantor
Juyong Lee, MD, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.