
Abstract
Objective
To systematically evaluate the extent and quality of patient and public involvement (PPI) reporting in prehabilitation programmes and research.
Data Sources
Keyword searches were conducted in MEDLINE, EMBASE, CINAHL, PsycINFO and the Cochrane Central Register of Controlled Trials from 1 January 1994 to 22 October 2025.
Review methods
Using an a priori protocol registered with PROSPERO, a systematic review was conducted in accordance with PRISMA guidelines. A narrative synthesis approach was used to interpret findings across heterogeneous studies. Methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT). A patient representative contributed to the study design and co-authored the review.
Results
From 14,078 records, 16 studies reporting PPI were included from the UK, Australia, Canada, USA and Spain. Most studies involved patients at multiple stages, using varied approaches including experience-based co-design. Reporting quality was suboptimal; only three studies met all items of the GRiPP2-SF checklist criteria, and none used a formal PPI reporting checklist tool.
Conclusion
Few prehabilitation programmes are designed with patient and public involvement; highlighting the need for collaborative approaches to improve acceptability and adherence. Although evidence of PPI is limited, several studies demonstrated sustained and meaningful involvement. Reporting remains inconsistent, underscoring the need for clearer reporting to strengthen the evidence base and support wider adoption. The findings highlight substantial opportunities for collaboration in future programmes, and further research should examine how PPI influences adherence, patient experience and the overall effectiveness of prehabilitation interventions.
Introduction
Prehabilitation programmes have emerged as an innovative approach to optimise patients’ physiological and psychological preparedness before undergoing surgical or non-surgical interventions, such as surgery, chemotherapy or radiotherapy. 1 Prehabilitation prior to elective surgery may have beneficial effects, including fewer postoperative complications, enhanced functional capacity, reduced length of stay and improved quality of life,1–6 although outcomes vary based on population and the certainty of evidence remains generally low, with the exception of exercise and nutritional prehabilitation. 7 The certainty of evidence is limited by low-quality research, risk of bias, small sample size and studies pooling heterogeneous interventions. 6 Whilst there is no universally accepted definition for prehabilitation, a recent definition of surgical prehabilitation has been proposed as the ‘process from diagnosis to surgery, consisting of one or more preoperative interventions of exercise, nutrition, psychological strategies and respiratory training, that aims to enhance functional capacity and physiological reserve to allow patients to withstand surgical stressors, improve postoperative outcomes, and facilitate recovery’. 8 Prehabilitation programmes initially focused on single-component (unimodal) interventions to increase physical function and capacity, and later evolved to include multimodal aspects of care, including medical optimisation (i.e., management of preoperative anaemia, blood glucose optimisation), nutritional support, perioperative education and/or psychological support. 9 However, patient adherence to these programmes, particularly those involving multiple components, has been identified as a challenge. 10 Recent studies recommend stratified approaches to prehabilitation, including more patient-centred or personalised programmes to improve adherence.11,12 Previous studies have also reported that patient adherence is enhanced by patient involvement and participation, 13 although no reviews have examined the use and reporting of patient and public involvement (PPI) in prehabilitation research and design.
PPI in health services design and redesign has increased significantly over the past two decades and has been described as the ‘new Zeitgeist’ in healthcare. 14 PPI is becoming widely recognised as a key factor in the design and improvement of safe, high-quality healthcare services 15 and characterised by active engagement of patients and members of the public working with researchers and healthcare professionals to serve as ‘innovators, informants and distributors of health information’. 16 Often conceptualised as partnerships or collaborations in the healthcare context, there is increasing recognition of the benefits of healthcare professionals, researchers and patients working together in healthcare research and improvement projects, and the importance of the ‘unique and precious’ knowledge and insights of patients which can be utilised to improve patient experiences, services and outcomes. 17
Despite growing evidence of PPI benefits across related health fields such as cancer care, surgery and cardiac research,18–21 no reviews have specifically examined PPI use and reporting within prehabilitation. This is notable given that prehabilitation relies on sustained and meaningful patient engagement and involves challenges such as time-sensitive delivery and multimodal design. Consequently, a focused review of PPI is warranted to determine whether current prehabilitation programmes and research are informed by patient and public perspectives and priorities. As Glasziou et al. 22 have highlighted, failing to involve patients and the public in research design contributes to research waste and risks misalignment with the needs of those the research is intended to benefit. Embedding PPI is therefore essential, not only to ensure that researchers can optimally design future interventions and trials informed by patient insights, but also to promote responsible use of public research funds and align with best practice research guidance. 23
Thus, this review aimed to describe the extent of PPI in prehabilitation programme design, implementation and research, and the quality of reporting. Four key questions guided this review: (1) How and when are patients involved in the research and design of prehabilitation programmes? (2) What activities and approaches are used to involve patients and the public in researching and designing prehabilitation programmes? (3) What are the impacts and outcomes of PPI? (4) What is the quality of reporting on PPI in prehabilitation?
Methods
Study design
This systematic review of qualitative, quantitative, and mixed methods studies was conducted and reported to adhere to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA and PRISMA-P) criteria. 24 The systematic review protocol was developed prior to the literature search and published online via PROSPERO (CRD42020221684).
Defining PPI and codesign
For the purpose of this review, we use the term ‘patient’ to collectively include patients, potential patients, patient representatives, carers, service-users, consumers and members of the public actively involved in the development and design of prehabilitation projects, including the planning and/or conduct of prehabilitation research. PPI specifically refers to research which is carried out ‘with’ or ‘by’ patients and members of the public, rather than ‘to’, ‘about’ or ‘for’ them.25,26 One form of involvement, codesign, refers to active collaboration between patients, healthcare professionals, and/or researchers in designing solutions for a specific problem (i.e., a service or product improvement or innovation). 27 Both PPI and codesign have been included in this review to capture the active involvement of patients in both research and service design/ improvement activities across a wide spectrum of prehabilitation programmes. It is important to note that involvement often occurs along a continuum, ranging from consultation to shared leadership. 28
Definition of prehabilitation
To capture all potentially relevant projects and research related to prehabilitation, we included two different categories of prehabilitation: (1) interventions that aim to medically optimise functional capacity or nutritional status of patients before surgery or medical treatment, with the goal of improving or shortening recovery time, reducing perioperative complications and/or enhancing outcomes; and (2) interventions or practices to support the psychological preparedness of patients before surgery or medical treatment, such as cognitive coping strategies, facilitated peer support, or the use of educational resources.
Study eligibility
Inclusion criteria are outlined in Table 1. All relevant qualitative, quantitative or mixed methods studies that reported PPI or codesign in prehabilitation projects and research, including but not limited to medical optimisation (i.e., management of preoperative anaemia, blood glucose optimisation), physical exercise, nutritional support and/ or psychological support components prior to surgery or medical treatment, were included. To be eligible, articles had to be full-text studies and published in English between 1 January 1994 and 22 October 2025. The year 1994 was selected as this was when the earliest trial 29 was identified in one of the first systematic reviews on prehabilitation. 30 We excluded studies where involvement was limited to patient or the public being a research participant or ‘subject’ (i.e., individuals recruited as research participants for a clinical trial/data collection purpose or being an interview or focus group participant). Where interviews or focus groups were described as being part of a co-design or collaborative process shaping the prehabilitation programme or research, these studies were retained. Studies exclusively related to postoperative rehabilitation (e.g., enhanced recovery after surgery (ERAS), ICU mobilisation) or post-discharge settings (community rehabilitation) were also excluded, as were editorials, opinion pieces, abstracts, conference proceedings, dissertations and protocols.
Inclusion and exclusion criteria.
Non-English full-texts were excluded due to resource and time constraints.
Search strategy
Five online databases were searched (OVID MEDLINE, Elsevier EMBASE, EBSCO CINAHL, PsycINFO, Cochrane Central Register of Controlled trials). The search strategy was developed with an expert health librarian and reviewed by a patient representative (JC). Search terms covered: (1) public, patient, consumer, or service-user involvement; (2) involvement and codesign and (3) prehabilitation. This included international terminology variations, such as ‘consumer’ in Australia, and ‘PPI’ in the UK. Search terms were applied to titles, abstracts, key words and full texts. Reference lists of included studies were manually screened to identify additional articles. A pilot search in MEDLINE was conducted to refine the search strategy before the full search was undertaken (see Supplemental File 1).
Eligibility screening
Search results were imported into Rayyan QCRI systematic review web application, 31 and duplicates removed. Two reviewers (RM, MR) independently screened title and abstract and full texts against inclusion and exclusion criteria (Table 1). If eligibility could not be determined through title and abstract screening, studies underwent full-text screening. Uncertainties were resolved through discussions with a third reviewer (FL).
Data extraction
A data extraction form was developed to capture key aspects of each study and was piloted and refined. Extracted data included study characteristics: year, design, country, methods, sample, setting, prehabilitation type and measurement. Involvement and codesign were classified using an adaptation of the International Association of Public Participation (IAP2) spectrum which included six levels of engagement (learn/inform, participate, consult, involve, collaborate, lead/support). 32 Reporting quality was assessed using the Guidance for Reporting Involvement of Patients and the Public (GRiPP2) short form reporting checklist. 33 One reviewer (MR) extracted data, and a second reviewer (RM) checked 100% for accuracy. Discrepancies were resolved through consensus.
Data synthesis
Given heterogeneity in study design, setting, populations and incomplete reporting, findings were synthesised narratively to identify patterns, similarities and differences. 34
Quality appraisal
Methodological quality of each study was assessed using the Mixed Methods Appraisal Tool (MMAT), 35 suitable for qualitative, quantitative and mixed methods designs. Two reviewers (PAZ and MR) appraised each study, with disagreements resolved by a third reviewer (RM). No studies were excluded on the basis of quality; appraisal informed interpretation of the evidence.
Patient and public involvement
PPI was an integral component of this review to ensure it reflected both patient and healthcare professional perspectives. A member of the Consumer Advisory Group (JC) joined the review team as a patient representative, contributing valuable insights and building on an existing partnership. 36 Their involvement included helping establish review parameters, providing feedback on extraction tables, contributing to data analysis, reviewing the manuscript and co-authoring the paper. Full details, including aims, methods and reflections, on involvement are reported in accordance with the GRiPP2 short form checklist 33 (Supplemental File 2).
Results
Study inclusion
The search strategy yielded 14,078 articles, of which 79 were identified for full-text review.
We excluded 63 articles; the reasons for exclusion are outlined in the PRISMA flow diagram (Figure 1). Following full-text review, 16 articles met the eligibility criteria and were included in the review.
PRISMA flow chart: identification of studies for the systematic review. 24
Study characteristics
Study characteristics of included studies are outlined in Table 2.37–52 Study designs varied, four used Experience Based Co-Design (EBCD),38,39,45,50 three were qualitative studies,37,42,43 two were action research47,48 and two were feasibility studies.40,41 Additional designs included an exploratory randomised controlled trial, 51 a feasibility clinical trial, 44 a participatory codesign/observational cohort study, 46 a cross-sectional study 40 and a Modified Delphi study. 52 Most studies were published after 2017 (n = 14) with the earliest identified study in 2013. The majority of studies were conducted in the United Kingdom (n = 9),37,39,41,42,44,47,48,51,52 and Australia (n = 4),45,46,49,50 the remaining studies were conducted in the United States (n = 1), 39 Canada (n = 1) 43 and Spain (n = 1). 38 Three studies involved a mixed population of patients and their carers,48,50,51 with one study testing an intervention to indirectly support patients through their carers. 51 Eleven studies focused on cancer prehabilitation (pre-operative and non-surgical).38–42,45,48–52 Five studies focused on the development of web-based, app-based or digitally enabled prehabilitation programmes.37,38,40,48,49 Four studies focused on developing non-surgical prehabilitation programmes (e.g., chemotherapy, fibromyalgia).39,44,50,51 Two studies focused on pre-operative orthopaedic surgery (total knee replacement),37,47 and one study focused on developing of criteria for evaluating and designing equitable prehabilitation before cancer surgery. 52
Study characteristics and quality assessment.
EBCD: experience based co-design; TKR: total knee replacement; QI: quality improvement.
*Mixed Methods Appraisal Tool (MMAT) [ 21 ]; Y = Yes, N = No, CT = Can’t Tell.
Section 1 of the MMAT for qualitative studies. b Section 4 of the MMAT for quantitative descriptive studies. c Section 5 of the MMAT for mixed methods studies. d Section 2 of the MMAT for quantitative randomised controlled trials. e Section 3 of the MMAT for quantitative non-randomised trials; Unimodal*: this study focused on pre-operative patient education as one component of an ERAS multimodal approach; CT* Can’t tell, this paper focused on reporting PPI and did not include complete methodological reporting, CT** Can’t tell, this study included limited reporting on the feasibility trial, and included qualitative methods: Ya Ya Ya Ya CTa.
Characteristics of the prehabilitation interventions
Of the 16 studies, six employed multimodal interventions37,38,41,43,44,49,52 that included psychological support, exercise, nutrition support and smoking cessation in varying combinations across studies. Five used unimodal approaches focusing specifically on preoperative or pre-treatment psychological preparation.40,42,45,48,51 One unimodal study focused on preoperative speech and language therapy alongside prophylactic swallowing exercises, 39 while another unimodal study focused on preoperative psychological support for patients and carers. 48 Two studies adopted bimodal designs that combined psychological preparation with exercise.47,50 Several studies included a focus on the development of educational support and resources to improve psychological preparedness. Of these, three studies provided in-person education sessions with multidisciplinary health care professionals,44,47,50 three provided facilitated group sessions,38,50,51 five produced web-based, app-based or digital information,37,38,40,46,49 two produced education resources in the form of a video or DVD45,51 and one developed a patient information booklet. 47 Two of the studies included a focus on improving nutritional status and weight optimisation of patients prior to surgery.38,46
Level of patient and public involvement
The majority of studies reported clearly on both the characteristics and number of those involved in the research process. A total of 192 individuals were involved across the 16 studies, with the majority identified as patients (n = 101). The remaining individuals were variously described as consumers (n = 38), carers (n = 15), experts by experience (n = 17), patient representatives or advocates (n = 8), public contributors (n = 7), service users (n = 5) and PPI member (n = 1). The terminology used to describe individuals varied considerably across studies, with some terms clearly defined and others used with limited or no explanation of what the term meant or how the role was conceptualised. Three studies involved a single patient,43,44,48 while four studies involved between two and 10 patients and carers,38,39,47,48,50 and five studies engaged larger, mixed groups ranging from 14 to 38 individuals, involving patients, carers/ caregivers, consumer representatives, advocates and experts by experience.42,45,46,49,52 Two studies reported the involvement of ‘patients’ and ‘carers from a cancer service’ but did not provide specific numbers.40,51 Five studies reported on aspects of diversity in relation to PPI,41,42,45,46,52 and only one study incorporated an explicit equity focus. 52 None of the included studies acknowledged intersectionality or overlapping identities such as gender, socioeconomic status, disability or Indigenous identity.
Fourteen of the 16 studies reported involving patients at multiple time-points,37–41,43–50,52 while two did not specify the stages at which patient involvement occurred.42,51 The level of involvement varied from consulting to collaborating. Consulting typically involved seeking patient feedback on discrete aspects such as intervention feasibility, study procedures and materials.40,42,46,49,51 Collaboration entailed a more active and sustained partnership, where patients were members of the research team and contributed to decision-making throughout, including the design, development, implementation and dissemination of prehabilitation programmes and research.41,47,48,50 More detail on the level of PPI in the included studies is described in Table 3.
Overview of PPI.

*Limited reporting of PPI in this study, the description suggests consultation with elements of involvement rather than sustained involvement.
Activities and approaches to involve patients
Seven studies reported sustained and active involvement of patients across multiple phases of the research process,37,41,43,47,48,50,52 including participation as co-applicants on grants and publications, 41 contributions to study design, implementation and dissemination,37,48 involvement in substantive activities such as the delivery of interventions in group sessions, 47 and membership on expert and project advisory panels.37,41,46,52 In four studies, patients shared their own experiences and identified key ‘touchpoints’ and areas for improvement as part of the experience-based co-design (EBCD) process.38,39,45,50 In two studies, a prehabilitation intervention was co-designed with carers 51 and patients, 46 and in two studies, patients collaborated in the design of a new prehabilitation model.41,50 Most studies reported adequate detail on patient involvement in discrete activities within the research process, such as advising on the content and delivery of patient facing information such as plain English summaries, videos and booklets,37–39,44,45,47,49,52 contributing to interview analysis,39,41,43,45 advising on prehabilitation programme or model development,41,43,50,51 and informing study protocol and procedures, including intervention feasibility and acceptability.40,42,44 Several studies combined approaches,41,46,49,50,52 using involvement through advisory or steering groups to provide ongoing guidance, while also consulting additional patients for discrete, task focused activities such as usability testing and identifying barriers and facilitators to recruitment and engagement. This blended model allowed research teams to benefit from sustained partnership with a core group of patient advisors, alongside broader input from additional patients when specific perspectives or wider feedback was needed. The approaches used to involve patients are described in Table 3.
Outcomes and impact of patient involvement
There was variation across studies in how the impact of patient involvement and prehabilitation were reported (Table 4). Four EBCD studies reported the impact of patient involvement in the research process, noting that the co-design process generated rich insights and enabled clear identification of patient priorities, key topics, and ‘touchpoints’ which were important to patients in the development and delivery of prehabilitation services.38,39,45,50 One EBCD study reached consensus on the development of a model of prehabilitation for patients with prostate cancer, 50 and one action research study reported the process facilitated identification of educational content and delivery preferences which were relevant for patients and linked to enhanced recovery. 48 One feasibility study reported the involving PPIE representatives led to significant and beneficial changes to the initial design of a prehabilitation programme, helping to maximising acceptance, recruitment and retention. 41 A Delphi study similarly noted that patient involvement improved the clarity of statements and language, resulting in simpler, easy-read versions of Delphi statements and key materials. 52 Only one study explicitly outlined predetermined patient outcomes measures, indicating statistically significant improvements in understanding symptoms, managing side effects and meeting patient information needs through the ‘Take Care’ intervention. 51 Provider outcomes, assessed through surveys, focused on perceived implementation efficiency and burden. 40 Process outcomes were reported in eight studies, encompassing the acceptability of the prehabilitation intervention (n = 2),40,51 the acceptability of the co-design process (n = 3),39,45,50 methods and content of information sharing (n = 2)40,48 and the change process (n = 1). 47 These examples illustrate the tangible impact that meaningful involvement can have on the quality and acceptability of prehabilitation interventions and programmes.
Summary of prehabilitation programmes and outcomes.
* Key outcome measures/ measurement tools not applicable due to the study focus on co-design/action research process, and intervention development.
Focus areas included: Smoking, diabetes management, anaemia/low iron, emotional wellbeing, frailty, pain management, alcohol and drugs medication management, activity and exercise, and nutrition and weight optimisation; MDT: Multidisciplinary Team; TKR: Total knee replacement.
Quality of reporting for patient and public involvement
The quality of reporting on PPI in relation to GRiPP2 criteria varied (Table 5). All but three studies40,44,47 clearly described the aim of involvement, and all 16 studies described patient involvement methods. Thirteen of the 16 studies, except for Corriveau et al., 43 Courel-Ibáñez et al., 44 and Tsianakas et al., 51 described patient involvement in the results. The majority of studies also included patient involvement in the discussion and conclusion.38,39,41,43–45,47–50,52 Demonstration of the final criterion was less evident, with only three studies,38,41,50 providing a detailed reflection and critical perspective on patient involvement, four studies providing a partial reflection,39,40,45,51 and nine studies providing no critical reflection/ perspectives.37,42–44,46–49,51 Table 5 provides a summary of reporting in relation to the GRiPP2 criteria.
Summary of reporting adherence with the GRiPP2 checklist.
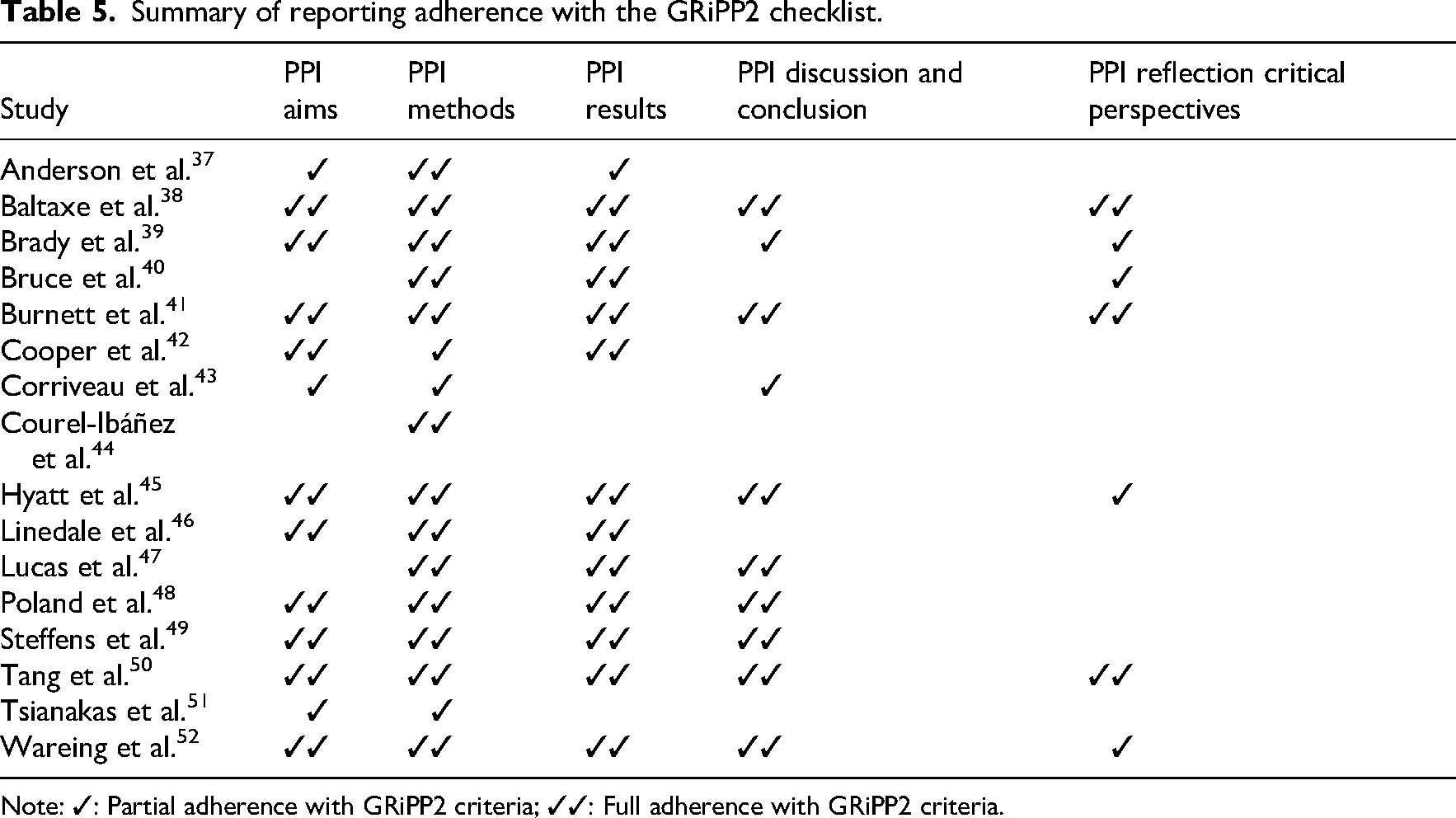
Note: ✓: Partial adherence with GRiPP2 criteria; ✓✓: Full adherence with GRiPP2 criteria.
Quality appraisal of included studies
Study quality varied, and half of the of the sixteen studies met all quality criteria.37,42,43,47,48,50–52 While six of the qualitative studies met all quality criteria, two studies did not have evidence that the interpretation of the results was substantiated by the data (Criteria 1.4), and there was a lack of coherence between qualitative data sources, collection, analysis and interpretation (Criteria 1.5). Two of the three mixed methods studies did not include an adequate rationale for using a mixed methods design (Criteria 5.1), and one of the studies did not address divergencies and inconsistencies between quantitative and qualitative results (Criteria 5.4). A summary of the quality appraisal is presented in Table 2.
Discussion
A growing interest in PPI within prehabilitation is evident, yet the limited number of studies reporting PPI suggests that this momentum has not fully translated into consistent practice within the field. The findings of this systematic review align with evidence from previous research, indicating that PPI is recognised as valuable but remains underutilised.53,54
This suggests substantial scope and opportunity for future development and implementation within prehabilitation settings. It remains unclear, however, whether the limited use and reporting of PPI, particularly in areas such as prehabilitation, reflects a lack of awareness about its relevance and application, unfamiliarity with EQUATOR reporting guidance, 33 or broader barriers such as limited resources, time and skills. A recent systematic review identified multiple barriers to PPI in healthcare, including limited knowledge and institutional support, negative attitudes towards patient contributions, resistance to involvement, organisational constraints and inadequate training and accessibility. 55 Additionally, a recent BMJ study suggested that underreporting may not be solely due to a misunderstanding of reporting standards or structural barriers, but also from a lack of actual PPI activity and a reluctance to report unsuccessful or tokenistic PPI. 56 This suggests that a complex mix of contextual, attitudinal, and structural factors may contribute to the underutilisation and underreporting of PPI in prehabilitation. Greater use of established frameworks such as EBCD, and tools such as GRiPP2 can provide guidance and improve reporting of PPI. Journals also have a key role to play; some journals such as BMJ, now require PPI reporting at submission, a practice that could be more widely adopted. 57
In examining the characteristics of PPI reported within the included studies, further limitations are evident. Three studies involved a single patient,43,44,48 four studies involved between two and 10 patients and carers,38,39,47,48,50 and five studies engaged larger mixed groups of 14–38 individuals, involving patients, carers/ caregivers, consumer representatives, advocates and experts by experience.42,45,46,49,52 While most studies demonstrated a clear commitment to involving patients and people with lived experience, reporting on the characteristics of those involved was limited. Five studies reported on aspects of diversity in relation to PPI,41,42,45,46,52 highlighting gaps in transparency and representation. Only one study included an explicit equity focus, 52 and none acknowledged intersectionality or overlapping identities such as gender, socioeconomic status, disability or Indigenous identity.
The absence of diversity reporting is notable given the recency of the studies and longstanding concerns about the lack of diversity in PPI. Critics have observed that PPI often involves ‘well-behaved’ or ‘acquiescent’ people 58 with greater economic, social or cultural capital, 59 which can exclude marginalised groups, frequently described as ‘hard to reach’, ‘vulnerable’ or ‘high risk’.60,61 The lack of intersectional perspectives further limits understanding of whether involvement reflects the experiences of people who may face additional barriers to accessing or engaging with prehabilitation. Ensuring that PPI captures a broad range of identities and experiences is essential for advancing equity,52,62 and future studies should report more clearly on those involved so that diversity and representation can be assessed and strengthened.
Despite growing recognition of the value of PPI in health research, it is still rarely evaluated. Where evaluation does occur, the impact often remains unclear.63,64 Most studies described involvement rather than assessing its effects on outcomes or service delivery, and none examined PPI impact on specific outcomes such as prehabilitation adherence. Few studies offered critical reflections on PPI processes, limiting insights into its unique contributions and challenges in the context of prehabilitation. Greater transparency and evaluation are needed, particularly regarding involvement processes, support structures, remuneration and power dynamics, to strengthen interpretation of PPI outcomes and advance learning in this emerging field.
Our findings reveal limited geographical representation in prehabilitation research, with most studies from the United Kingdom and Australia, and a limited number from Spain, Canada, and the United States, largely published after 2017. This pattern reflects broader developments in patient involvement, 65 likely driven by strong policy and funding incentives from organisations such as the National Health and Medical Research Council (NHMRC, Australia), 66 National Institute for Health and Care Research (NIHR, United Kingdom) 67 and Patient-Centered Outcomes Research Institute (PCORI, United States). 68 Cancer-focused prehabilitation was particularly prominent, likely reflecting funding priorities and public interest in oncology. 18
To our knowledge, this is the first systematic review to specifically focus on PPI in prehabilitation. The findings highlight the need for improved reporting, particularly in relation to diversity, impact, challenges and critical perspectives. As expectations around PPI continue to grow, greater patient involvement is likely in future studies. Existing frameworks and guidance33,69 can support authentic partnerships and promote greater transparency, but researchers and funders must use these resources critically and reflexively. 70
This review was informed by patient collaborators and established frameworks, including GRiPP2 33 and Manafo. 32 A strength of the review is the inclusion of all prehabilitation studies from the first prehabilitation study in 1994–2025. However, several limitations should be acknowledged; inclusion was restricted to English-language articles, potentially excluding relevant non-English studies; PPI may have been under-reported in some studies or omitted from abstracts, limiting our ability to identify studies which may have included PPI; terminology differences across disciplines or regions may have led to missed studies.
Overall, we found limited but emerging use of PPI in prehabilitation, alongside clear examples of meaningful, sustained involvement. Reporting remains inconsistent, and strengthening the clarity and rigour of PPI reporting is essential to build the evidence base and support wider adoption. Addressing the challenges identified offers an opportunity to ensure prehabilitation programmes better reflect patient priorities and experiences. Future research should examine the outcomes of PPI, including its impact on adherence, patient-experience and the effectiveness of prehabilitation interventions.
Prehabilitation before elective surgery can reduce complications, improve functional recovery and shorten length of hospital stays. Patient-centred, personalised prehabilitation programmes improve adherence and engagement. Greater integration of patient and public involvement in research and practice is needed to optimise patient outcomes.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155261450157 - Supplemental material for Patient and Public Involvement in Prehabilitation: A Systematic Review
Supplemental material, sj-docx-1-cre-10.1177_02692155261450157 for Patient and Public Involvement in Prehabilitation: A Systematic Review by Rachel Muir, Megan Rattray, Peta-Anne Zimmerman, Joan Carlini and Frances Fengzhi Lin in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank Griffith University Health Librarian, Bonnie Dixon and Queensland Health Librarian, Sarah Thorning, for support with development of the search strategy and searches. We would also like to thank Lauren Murray for helpful comments on an initial draft of this paper.
Contributions
Rachel Muir: funding acquisition, conceptualisation, methodology, formal analysis, writing – original draft and writing – review and editing. Megan Rattray: methodology, formal analysis, writing – original draft and writing – review and editing. Peta-Anne Zimmerman: conceptualisation, methodology, formal analysis and writing – review and editing. Joan Carlini: methodology, formal analysis and writing – review and editing. Frances Fengzhi Lin: conceptualisation, methodology, formal analysis and writing – review and editing.
Funding
A seed grant was provided by Griffith University School of Nursing and Midwifery for research assistant support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.