
Abstract
Objective
To initiate the development of an agreed core outcome set for post-stroke facial palsy, identifying which outcome domains should be measured in research and may inform clinical practice.
Design
Two online e-Delphi rounds followed by an online consensus meeting.
Setting
International, multi-disciplinary.
Participants
Clinicians and researchers working in post-stroke facial palsy.
Methods
Delphi items were developed from existing literature, qualitative interviews with stroke survivors and patient/public involvement, then aligned with ICF levels. Participants completed two e-Delphi rounds rating outcome domains on a 1 to 9 GRADE scale: 7 to 9 ‘critical’; 1 to 3 ‘least important’. All domains were discussed at the consensus meeting and included in the final list if ≥70% of participants voted ‘yes’ to include the domain in the core outcome set.
Results
In total, 156 Delphi questionnaires (round one, 101 participants from 16 countries; round two, 55 from 12 countries) were completed. Fifteen participants from 6 countries attended the consensus meeting. Three outcome domains were agreed for inclusion in the initial core outcome set: (1) facial movement and sensation, (2) everyday function, and (3) living with facial palsy.
Conclusions
We report the first internationally informed consensus between clinicians and researchers on ‘what’ outcome domains are important to measure for post-stroke facial palsy. We share these findings to encourage their measurement and to guide next steps. Our future work includes a separate consensus study, using a more inclusive methodology, on ‘what’ to measure with lived-experience stakeholders, and a systematic review on ‘how’ to measure these outcomes. COMET Initiative registration (December 2024): https://www.comet-initiative.org/Studies/Details/3295
Introduction
Central facial palsy frequently occurs as a consequence of stroke,1,2 with estimates indicating an incidence of 45% to 60% in acute stroke.3–6 This condition can impact physical appearance, verbal and non-verbal communication, eating, drinking, swallowing and the ability to express emotions,4,7–9 negatively affecting the quality of life and psychological well-being of stroke survivors. 10
Recent systematic reviews of assessment and rehabilitation for post-stroke facial palsy have highlighted considerable variability in the outcome measures used in research.1,11 Studies included in these reviews assess diverse domains, including motor impairment and symmetry, oro-facial muscle strength, neurophysiological pathways, and patient-reported function and quality of life. Although the Sunnybrook Facial Grading System and the House-Brackmann scale are the only tools with psychometric validation specifically for post-stroke facial palsy,12,13 a variety of assessments are applied in clinical practice, including informal oromotor assessments, the Stennert index, 14 the Facial Disability Index 15 and the Facial Clinimetric Evaluation Scale.2,16 This diversity in outcome measurement, across both research and clinical settings, limits comparability between studies, making it difficult to synthesise findings and evaluate treatment efficacy.11,17
While consensus guidelines and evidence-based management strategies exist for peripheral facial palsy (e.g. Bell's palsy), 18 no such framework is currently available for post-stroke facial palsy. Although both conditions affect facial movement, post-stroke facial palsy differs fundamentally in its underlying pathology, clinical presentation, recovery trajectory and the broader context in which it occurs, alongside other stroke-related impairments such as aphasia, dysarthria, dysphagia, cognitive and emotional changes.1,3 These differences mean that outcomes prioritised for peripheral facial palsy cannot be assumed to be relevant or sufficient for post-stroke facial palsy, and a condition-specific core outcome set is therefore needed. Before developing evidence-based management strategies, it is essential to ensure we know ‘what’ to measure and ‘how’ we do this with a core outcome set. A core outcome set is an agreed minimum set of outcomes that should be measured and reported in all studies for a specific condition, to improve comparability, reduce selective reporting, and support both research and clinical practice. 19
Our ultimate aim is to develop a consensus-based core outcome set for post-stroke facial palsy with agreed measures. The aim of the present study is to agree on ‘what’ outcome domains should be measured for post-stroke facial palsy from the perspective of clinicians and researchers, as a first step in development. The third key stakeholder group of critical importance in the development of a core outcome set is the views of people with lived experience, and this work is being carried out separately using a methodology that is inclusive of people with communication, cognitive and fatigue related needs commonly experienced after stroke.
Methods
Research ethics approval was obtained from the University of Manchester (2024-21316-38685) and a protocol published. 20 The study was registered with the COMET Initiative (December 2024): https://www.comet-initiative.org/Studies/Details/3295. Methods were developed in accordance with the Core Outcome Set standards for development (COS-STAD) recommendations 21 and the Core Outcome Set standardised protocol (COS-STAP) checklist. 22 We used a modified e-Delphi rounds and a consensus meeting, and five steps were followed (Figure 1).
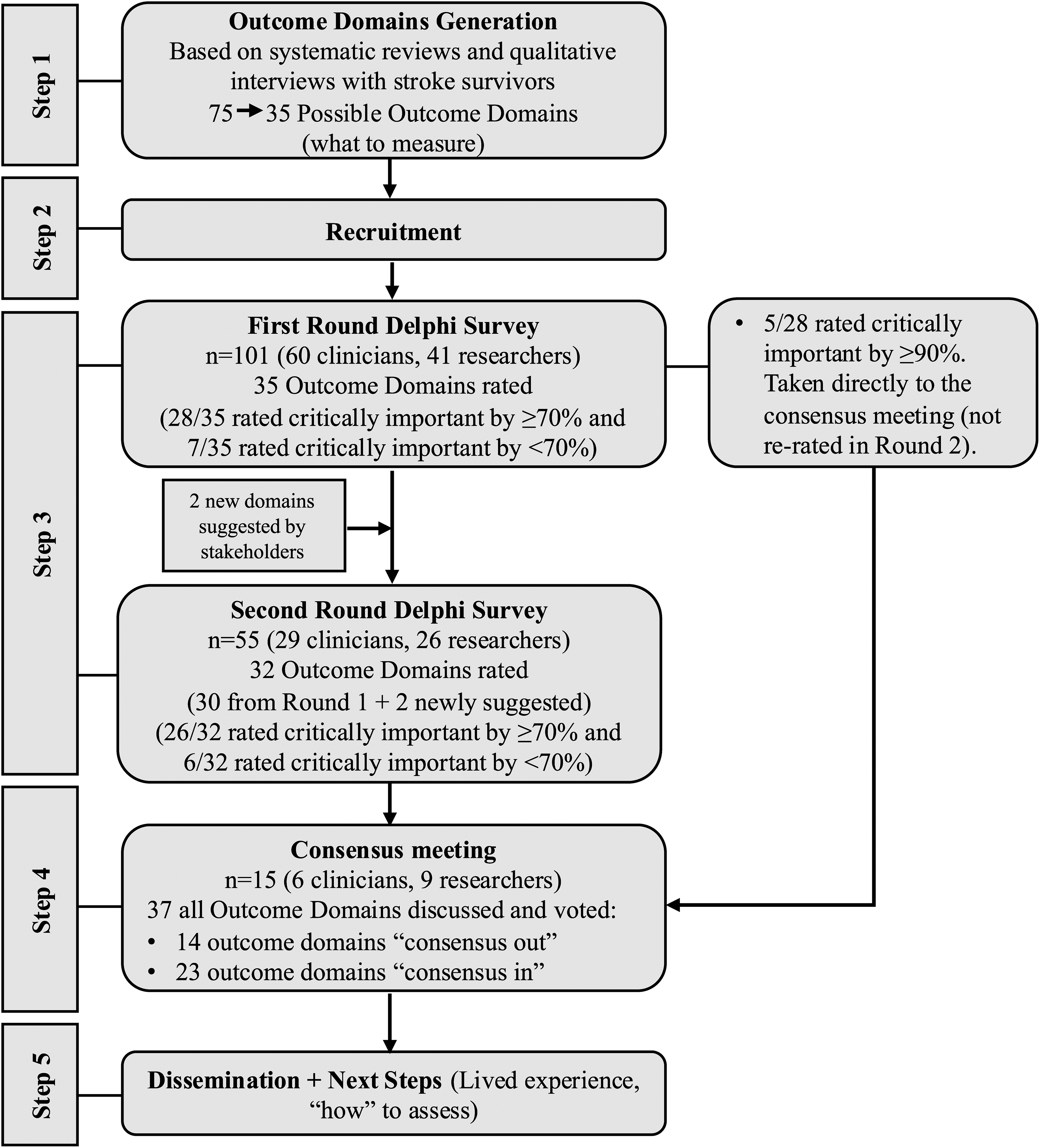
Flow diagram showing the initial stages in the development of the core outcome set for post-stroke facial palsy.
Step-1 (Outcome domains generation): A comprehensive long list of potential outcome domains was generated using existing systematic reviews of post-stroke facial palsy,1,11 supplemented by an updated systematic search of all major databases conducted by the research team (manuscript in preparation) and findings from qualitative interviews with people living with stroke. 23 Before launching the Delphi rounds, the study management group (HSE, AB, MC and CM) screened the preliminary long list to refine it into a feasible set of distinct outcome domains for Delphi rating. Each item was reviewed against the following pre-specified criteria, informed by COMET guidance and the COS-STAD recommendations21,24: (1) duplication, items conveying the same construct using different wording were merged under a single, clearly worded domain; (2) conceptual validity as an outcome domain, items were retained only if they represented a measurable outcome, and removed if they instead described an intervention, a process of care, a clinical sign used for diagnosis, a risk factor, or a measurement tool rather than an outcome; (3) specificity to post-stroke facial palsy, items reflecting generic stroke outcomes without a clear link to facial palsy were excluded; and (4) granularity, overly narrow items were subsumed under broader parent domains to avoid redundancy and reduce participant burden. Decisions were made by consensus within the study management group, with disagreements resolved through discussion. The co-researchers with lived experience then reviewed the refined list to confirm clarity, meaningfulness and that no important concepts had been lost. The consolidated outcome domain list was then systematically grouped by the research study team (HSE, AB, MC and CM) according to the International Classification of Functioning, Disability and Health (ICF) framework, 25 organising outcome domains into distinct domains: body structures and functions, activity, participation, and well-being/quality of life and released as an e-Delphi.
Step-2 (Recruitment): Two stakeholder groups were targeted for this international study: researchers involved in stroke or facial palsy research, and any healthcare professionals with experience treating patients with post-stroke facial palsy. Recruitment was conducted through various international clinical networks of healthcare professionals working in facial palsy and stroke (such as the World Stroke Organisation, Facial Therapy Specialist International and World Federation for NeuroRehab), social media platforms (X, Bluesky and LinkedIn), and by contacting researchers identified in relevant systematic reviews and published studies.1,11,26–28 All participants gave informed consent to participate after reviewing the participant information sheets.
Step-3 (e-Delphi rounds): The Delphi process comprised two rounds, during which participants rated the importance of each outcome domains on a 1 to 9 scale, where 1 to 3 indicated ‘least important’, 7 to 9 indicated ‘most important’ and 4 to 6 important but not critical which aligns with the Grading of Recommendations Assessment, Development and Evaluations (GRADE) system. 29 Two rounds were used rather than three, as the consensus meeting served as a third and final stage of deliberation, allowing participants to discuss, debate and vote on all outcome domains in real time. This approach is consistent with COMET guidance, 24 which recommends a minimum of two Delphi rounds and recognises that a consensus meeting can fulfil the role of a final round.
Participants were invited to suggest any additional outcome domains they thought were important to consider after round one. All participant-suggested outcome domains were reviewed by the study management group (HSE, AB, MC and CM) using the same pre-specified criteria applied during the initial long-list refinement (see Step-1): duplication, conceptual validity as an outcome domain, specificity to post-stroke facial palsy, and granularity. Decisions were made by consensus within the study management group, with disagreements resolved through discussion.
Outcome domains rated as critically important (7–9) by 90% or more of both stakeholder groups, or as of limited importance (1–3) by 90% or more of both groups in round one of voting, were not re-rated in the second round, and were carried forward to the consensus meeting for discussion. This 90% threshold was used only as a stability rule to reduce participant burden by avoiding re-rating of items with already overwhelming early agreement; it was not the threshold for consensus. In round 2, participants received anonymised, aggregated feedback on both stakeholder groups’ scores from round 1 alongside their own previous ratings, and were explicitly asked to take this group-level feedback into consideration when re-rating each outcome domain. This iterative feedback process is a defining feature of the Delphi method, enabling participants to reflect on where their views aligned with or diverged from the wider group before providing their round 2 ratings. They were asked to rate the importance of each outcome domain on a 1 to 9 scale again.
In the second round, participants were also asked to select the three most important outcome domains at each ICF level, prioritising all outcomes including those removed from re-rating in the second round.
Step-4 (Consensus Meeting): Following the two e-Delphi rounds, an online consensus meeting was held to review the Delphi results. Participants who had completed both e-Delphi rounds were invited, with the aim of including at least five participants from each group (researchers and clinicians). All participants provided written consent and verified their professional credentials prior to the meeting, which was conducted via a secure video conferencing platform (Microsoft Teams) and facilitated by an independent moderator with expertise in post-stroke aphasia research, from a different institution and with no prior involvement in post-stroke facial palsy research, ensuring independence from the specific topic under consensus.
In preparation for the meeting, e-Delphi results were analysed and presented separately for each stakeholder group (researchers and clinicians) and outcome domains were organised into tables according to ICF levels. A 70% threshold (with <15% rating an outcome as of limited importance) was used to categorise outcomes after the second round and as the final inclusion criterion at the consensus meeting, in line with COMET guidance and commonly applied cut-offs in core outcome set development. 24 Outcome domains from the second round were categorised into three groups: (1)‘Consensus in’ (where 70% or more of participants in each stakeholder groups rated the domains as critically important [7–9], and fewer than 15% in each group rated it as of limited importance [1–3]); (2) ‘Consensus unclear’ (where 70% or more rated the outcome as critically important in only one group, and fewer than 15% in each group rated it as of limited importance) and (3) ‘Consensus out’ (where none of the groups rated the outcome as important, with 50% or fewer participants in each group scoring it 7–9). This threshold was deliberately set at a more inclusive level than the Williamson et al. recommendation of 70% scoring 1 to 3, 24 in order to avoid prematurely excluding outcome domains before the consensus meeting. Given the breadth of the initial outcome domain list, applying a conservative ‘Consensus out’ criterion reduced the risk of dropping outcomes that participants might have rated more highly following iterative feedback in subsequent rounds, consistent with COMET guidance on managing participant burden across rounds. 24 All domains, regardless of their categorisation, were brought forward for open discussion and electronic voting at the consensus meeting, which served as the definitive and final inclusion criterion.
In addition, outcome domains that were rated as critically important (7–9) by 90% or more of participants in both stakeholder groups in the first Delphi round, and therefore not re-rated in the second round, were also included in the ‘Consensus in’ group. During the meeting, all initially created outcome domains and suggested ones, regardless of their existing consensus status, were discussed and voted for electronically, anonymously. Each domain was presented in turn according to the ICF levels of participation, activity, impairment and well-being, with more time allocated for debate on those with ‘consensus unclear’ status, allowing participants to argue for or against their inclusion. To be included in the final core outcome set, an outcome required at least 70% of participants to vote ‘yes, this is a critically important outcome’.
Following the consensus meeting, the research team reviewed the agreed outcome domains to consider how best to present them for use in research and clinical practice. Where consensus outcomes spanned more than one ICF category or did not fit neatly within a single domain, they were regrouped into a smaller number of overarching domains that more intuitively reflected the priorities of people with post-stroke facial palsy. This regrouping was undertaken by consensus within the research team and is reported in the Results.
Step-5 (Dissemination): Findings from this initial phase of developing a core outcome set for post-stroke facial palsy were disseminated through several channels, including feedback to the patient and public involvement group and presentations at local, national, and international stroke and rehabilitation research meetings and conferences. Reporting is done following the COS-STAR (Core Outcome Set-STAndards for Reporting) guidelines. 30
Results
The initial long list generated 75 potential outcome domains. The Delphi questionnaire was created from this long list, following the removal of 40 outcome domains, which were either duplicates or not considered by the study management group to be a valid outcome domain following the screening process described in step 1 in Methods. The final long list of 35 was grouped into 4 ICF levels: participation level, activity level, impairment level and well-being level outcomes (Supplemental material 1).
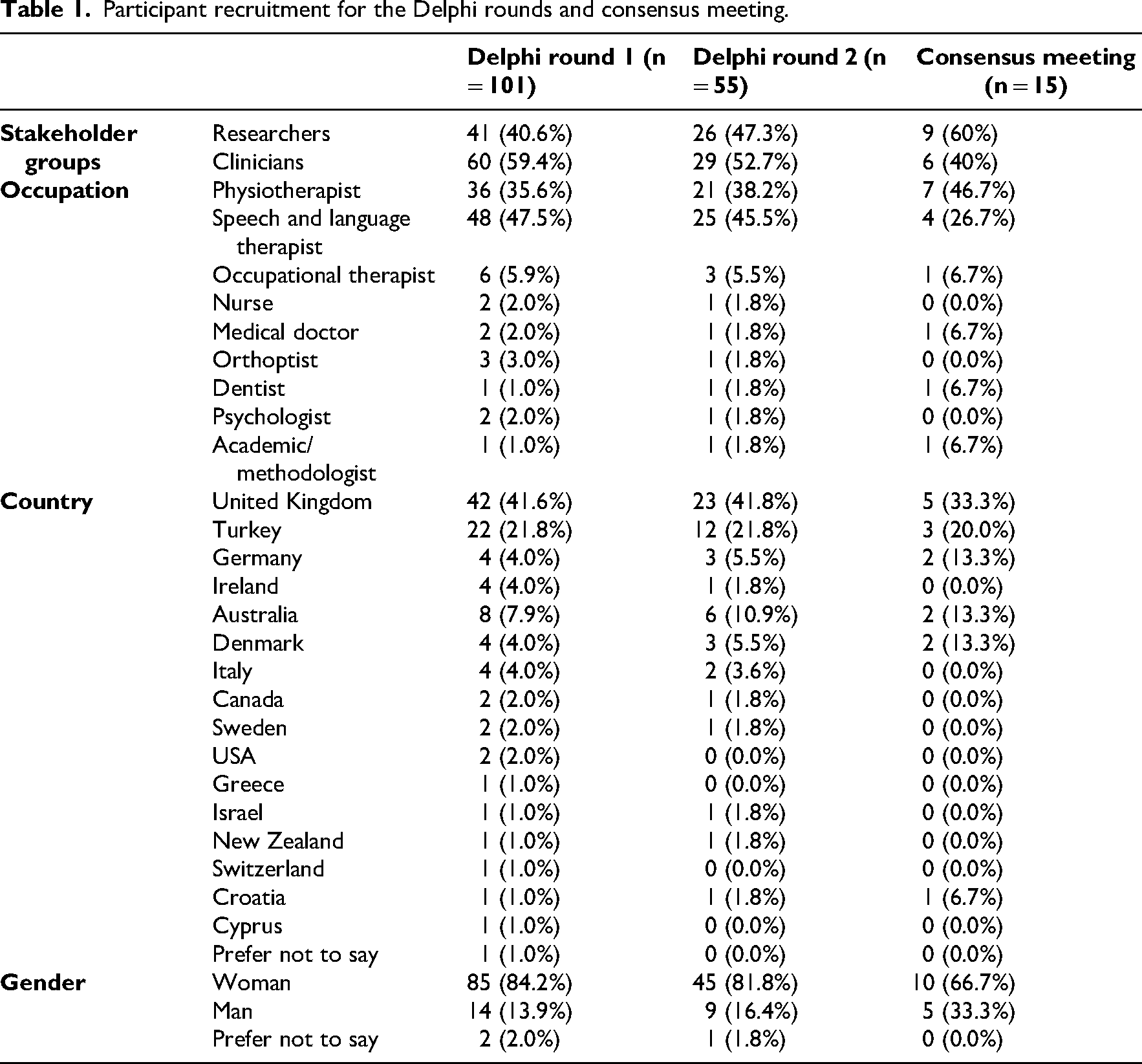
Participant characteristics for the Delphi rounds and consensus meeting in developing a core outcome set for post-stroke facial palsy are shown in Table 1. In the first Delphi round, clinicians outnumbered researchers (60 vs 41); in the second round, numbers were more balanced (29 vs 26), while in the consensus meeting, researchers were more prevalent (9 vs 6). The most common occupations among participants completing both Delphi rounds, and in the consensus meeting, were physiotherapists and speech and language therapists (35.6% vs 47.5% in round 1, 38.2% vs 45.5% in round 2 and 46.7% vs 26.7% in the meeting). Most participants were from the United Kingdom and Turkey (see Table 1). The first Delphi round included participants from 16 countries, the second round from 12 countries, and the consensus meeting from six countries. Women represented the majority of participants throughout the process; over 80% of Delphi respondents in both rounds and 66.7% of those at the consensus meeting. Participants attending the consensus meeting were from six different occupations, and six countries.
Participant recruitment for the Delphi rounds and consensus meeting.
In the first round of the Delphi, 28 out of 35 outcome domains met the inclusion threshold, with over 70% of both stakeholder groups rating them as highly important (scores of 7–9) (Figure 1). These spanned all ICF domains. Five outcome domains reached 90% stability (≥90% agreement in both groups) and were therefore not re-rated in round 2, but carried forward to the consensus meeting. These were: (1) ability to have a conversation, (2) facial expressions to communicate emotions, (3) ability to close/open mouth, (4) ability to move lips/cheek and (5) impact on emotional well-being (Figure 2). Detailed analysis of first round voting is shown in Supplemental material 1.
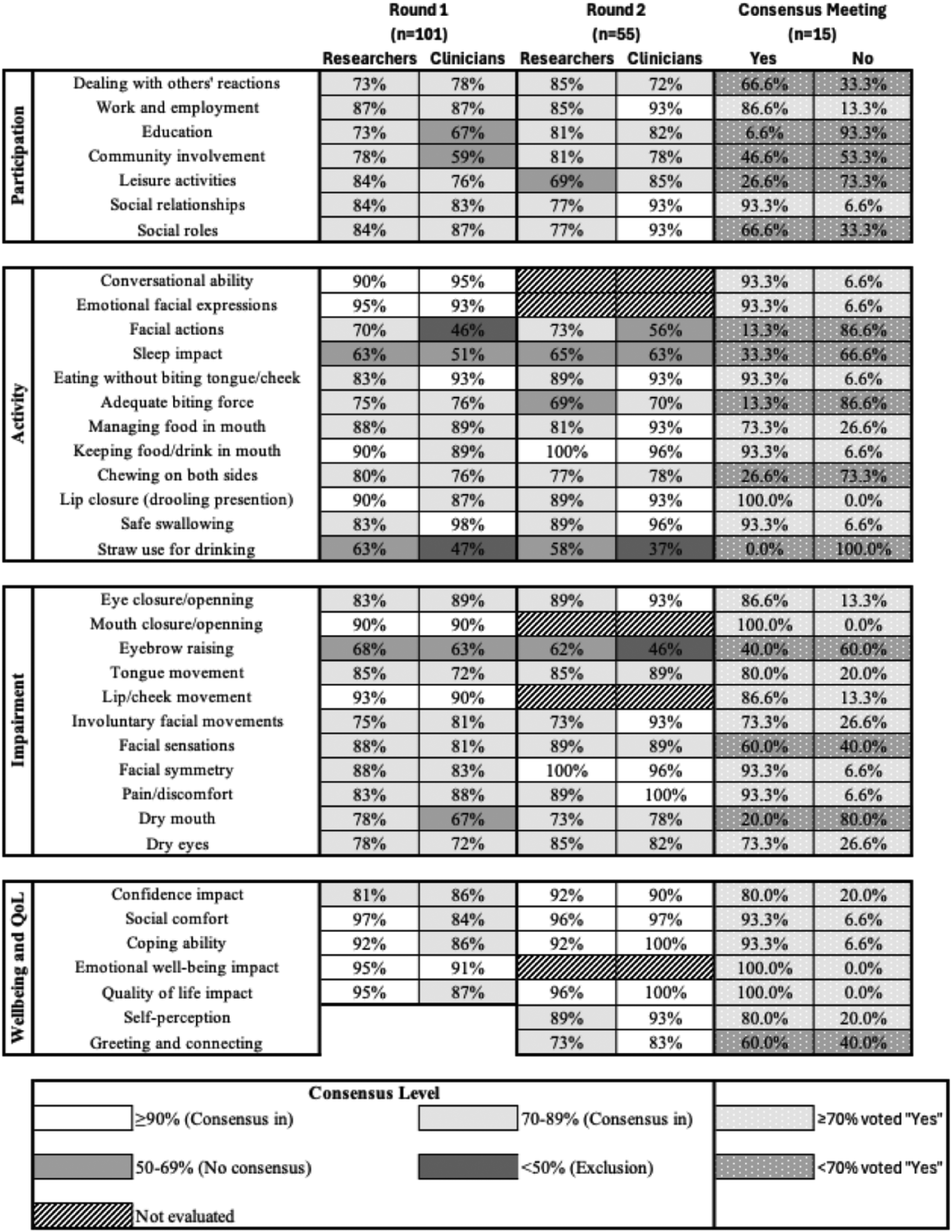
Delphi rounds and consensus meeting – consensus heat map.
Notably, no outcome domains were voted out in the first round as none reached consensus from both groups as being ‘not important’. Some outcome domains in the first round showed differences between stakeholder perspectives, particularly ‘facial actions like whistling/blowing’, where researchers rated them as more important than clinicians did. (Figure 2; Supplemental material 1).
Eight additional outcome domains were suggested by participants. Two new questions were included: impact on self-perception (e.g. body image and identity) and impact on greeting and connecting with family, friends or partners (e.g. by kissing). Of the remaining suggestions, two were incorporated into existing questions, three were already covered within the Delphi questionnaire, and one was excluded as it represented a clinical detail rather than an outcome.
After removing five outcomes that reached high consensus and adding two suggested wellbeing-level outcomes, 32 outcome domains were included in the second round, where 26 met the inclusion threshold (Figure 1). Six of the 26 outcome domains achieved ≥90% consensus from both groups and the remaining 6 of 32 outcome domains were below the 70% inclusion threshold in both groups as shown in Figure 2. Detailed analysis of the second-round voting, including prioritisation by participants, is shown in Supplemental materials 2 and 3.
The consensus meeting was run in June 2025 by an external facilitator. All 37 outcome domains from the Delphi rounds (32 + 5) (Figure 2) were discussed in detail at the meeting. After discussions, 23 out of 37 outcome domains met the criteria (≥70% of participants to vote yes) for inclusion in the core outcome set for post-stroke facial palsy, while 14 were excluded from the core outcome set (<70% of participants to vote yes) (Figure 2).
Following the consensus meeting, the research team reflected on how best to present and organise these 23 outcome domains to maximise their clarity and practical utility for future research and clinical practice. While the ICF framework had been invaluable for the initial development and prioritisation process, we found that the final set of consensus outcomes often spanned multiple ICF categories or did not fit neatly within a single domain. To address this, we undertook a process of regrouping the 23 consensus outcome domains into three overarching domains that more intuitively captured the lived experience and priorities of people with post-stroke facial palsy: facial movement and sensation, everyday function (with subdomains of communication, eating, drinking, and swallowing), and living with facial palsy (including psychosocial well-being and participation in daily life). This regrouping process is illustrated in Figure 3. Clear definitions for each of the three outcome domains are provided in Supplemental material 4.

Core outcomes for post-stroke facial palsy.
Discussion
Through rigorous consensus work with two stakeholder groups, we have agreed on ‘what domains should be measured’ for post-stroke facial palsy, completing the first step of the development of a core outcome set. Having this agreed set of domains for use in research and clinical practice should help to improve outcome reporting for post-stroke facial palsy and enable researchers to compare and combine findings more easily, thereby supporting better evaluation of treatments. 31 Among clinicians and researchers, we reached consensus that the core outcome set for post-stroke facial palsy should include three domains: (1) facial movement and sensation, (2) everyday function (communication, and eating, drinking and swallowing) and (3) living with facial palsy.
The ‘facial movement and sensation’ domain captures impairment-level constructs within the ICF body structures and functions, specifically related to which facial muscle movements (voluntary, involuntary and asymmetry) and sensory changes occur after stroke.4,10,25 Traditionally, research in this area has focused on measuring these impairment-level outcomes, often using clinician-rated scales and objective assessments.1,11,16,32 Although there is growing recognition that people with lived experience may place greater value on activity and participation-level outcomes, our findings suggest that researchers and clinicians continue to regard specific muscle movements as important outcomes for people after stroke.33,34 The next phase of our work will explore how people with lived experience and their family members or significant others prioritise these outcomes.
The ‘everyday function’ domain encompasses activity-level outcomes that capture how facial palsy affects core daily tasks, notably communication and eating, drinking, and swallowing, aligning with the ICF focus on real-world performance and participation. Stakeholders prioritised outcomes such as the ability to have a conversation, use facial expressions to communicate emotions, and maintain eating, drinking and swallowing functions. These priorities are supported by evidence that stroke-related oro-facial impairment reduces chewing efficiency, tongue force, oral sensitivity and lip restraining forces, is associated with dysphagia and poorer oral health-related quality of life, with limited spontaneous recovery in the absence of targeted rehabilitation. 10 The importance of facial expression for communication is further highlighted by research that found facial impairment is visible in everyday interactions and may explain why clinicians and researchers considered this to be important. 35
The ‘living with facial palsy’ domain addresses participation and well-being constructs within the ICF framework, capturing the psychosocial and role-related consequences of post-stroke facial palsy beyond impairment and activity. Stakeholders prioritised outcomes like confidence, social comfort, coping, emotional well-being, quality of life, social relationships and work impact. These priorities are consistent with evidence that facial palsy after stroke affects emotion, social signalling, and can lead to stigma, withdrawal, and mood disturbance, impacting social participation and health-related quality of life.4,7,8,10,28 Importantly, cohort data indicate that central facial palsy can negatively affect quality of life and depressive symptoms more than dysarthria among functionally independent stroke survivors, underscoring the importance of facial appearance and expressivity for social participation and mental health. 36
This study followed established guidance for core outcome set development, using a transparent multi-stage process that combined a two-round Delphi process with an independently facilitated consensus meeting.21,22,30 The ICF was used as an a priori framework24,25 to support the systematic generation and prioritisation of outcome domains. Following the consensus meeting, we made a deliberate decision to regroup the agreed outcomes into three overarching domains, as several spanned more than one ICF category. To develop a core outcome set, the voice of lived experience is crucial to the process.37,38 In our study, people with lived experience of stroke were involved as co-researchers in creating the Delphi rounds, but were not included as a stakeholder group for this phase. Instead, qualitative interviews with stroke survivor participants involved in a co-occurring study were used to inform this study on what was important to people with lived experience. A parallel study for this core outcome set will include this stakeholder group as participants using the nominal group technique, instead of online surveys. This approach will be more supportive and accessible to stroke survivors living with cognitive and communication challenges. 39 Despite its strengths, this study has several limitations. First, participation, while international (16 countries), was concentrated in the United Kingdom and Turkey, which may introduce geographical and health-system bias and limit applicability in underrepresented regions. Cultural differences in how visible physical disabilities such as facial palsy are perceived and responded to may also shape which outcomes are prioritised, and these perspectives may not be fully represented in our sample. Second, the stakeholder balance also varied: clinicians outnumbered researchers in the Delphi rounds, whereas researchers were more prevalent at the consensus meeting, potentially influencing voting dynamics. In addition, as in all Delphi studies, attrition across rounds may have introduced selection bias.
In conclusion, this study provides an internationally informed first step towards a core outcome set for post-stroke facial palsy that specifies what should be measured in research, addressing longstanding heterogeneity in outcome reporting. The professional stakeholders prioritised three domains to be measured: facial movement and sensation, everyday function (with two subdomains: communication and eating, drinking, swallowing), and living with facial palsy, providing a coherent biopsychosocial framework that links impairment, activity, and participation. Adoption of our final core outcome set will support consistency, reduce reporting bias, and enhance comparability and evidence synthesis across studies. Future work will focus on inclusion of the patient perspective and work to explore ‘how’ to measure these domains.
Post-stroke facial palsy requires a comprehensive biopsychosocial approach that extends beyond measuring facial muscle function to include meaningful impacts on daily activities and quality of life. Until the core outcome set is finalised, clinicians should use these outcome domains to guide clinical assessment, goal setting and treatment planning for post-stroke facial palsy across facial movement, everyday function and psychosocial well-being. The three consensus domains reflect a coherent biopsychosocial framework, spanning impairment (facial movement and sensation), activity (everyday function, including communication and eating, drinking and swallowing), and participation and well-being (living with facial palsy), highlighting that meaningful care must address all three levels rather than impairment alone.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155261458311 - Supplemental material for Towards a core outcome set for post-stroke facial palsy: Results from an international e-Delphi study and online consensus meeting with professionals
Supplemental material, sj-docx-1-cre-10.1177_02692155261458311 for Towards a core outcome set for post-stroke facial palsy: Results from an international e-Delphi study and online consensus meeting with professionals by Havva Sumeyye Eroglu, Audrey Bowen, Matthew Checketts and Claire Mitchell in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155261458311 - Supplemental material for Towards a core outcome set for post-stroke facial palsy: Results from an international e-Delphi study and online consensus meeting with professionals
Supplemental material, sj-docx-2-cre-10.1177_02692155261458311 for Towards a core outcome set for post-stroke facial palsy: Results from an international e-Delphi study and online consensus meeting with professionals by Havva Sumeyye Eroglu, Audrey Bowen, Matthew Checketts and Claire Mitchell in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155261458311 - Supplemental material for Towards a core outcome set for post-stroke facial palsy: Results from an international e-Delphi study and online consensus meeting with professionals
Supplemental material, sj-docx-3-cre-10.1177_02692155261458311 for Towards a core outcome set for post-stroke facial palsy: Results from an international e-Delphi study and online consensus meeting with professionals by Havva Sumeyye Eroglu, Audrey Bowen, Matthew Checketts and Claire Mitchell in Clinical Rehabilitation
Supplemental Material
sj-docx-4-cre-10.1177_02692155261458311 - Supplemental material for Towards a core outcome set for post-stroke facial palsy: Results from an international e-Delphi study and online consensus meeting with professionals
Supplemental material, sj-docx-4-cre-10.1177_02692155261458311 for Towards a core outcome set for post-stroke facial palsy: Results from an international e-Delphi study and online consensus meeting with professionals by Havva Sumeyye Eroglu, Audrey Bowen, Matthew Checketts and Claire Mitchell in Clinical Rehabilitation
Footnotes
Acknowledgements
Many thanks to Dr Paul Conroy, University of Dublin, who facilitated the consensus group meeting with patience and expertise. Thanks to the time and effort given by all the participants who completed the online Delphi surveys. Thanks to the time and effort given by all the participants attending the consensus meeting. The names of those who provided consent for their names to be published are listed below:
Dr Anna-Maria Kuttenreich
Dr Aslı Demirtaş
Dr Brooke-Mai Whelan
Mrs Clare Carling (specialist physiotherapist)
Ms Daniela Jakobsen
Mrs Gillian Capriotti
Ms Helen Saunders
Assist. Prof. Hrvoje Budincevic, MD, PhD
Prof Dr Ilke Keser
Associate Professor, Jesper Fabricius
Ms Martina Parisi
Dr Mohit Kothari
PT. PhD. Prof Nilufer CETISLI-KORKMAZ
Prof Dr Orlando Guntinas-Lichius
Associate Professor Praveen Kumar
Ethical consideration
Ethics approval was granted by University of Manchester (2024-21316-38685).
Consent to participate
Informed consent was obtained from all participants; digital consent was used for the e-Delphi questionnaires, and written consent for the consensus meeting.
Author contributions
HSE wrote the first draft. All authors read and commented on the paper and approved the final manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. HSE's PhD programme is funded by the Republic of Turkey Ministry of National Education for providing financial support. CM is funded by a personal postdoctoral fellowship from the Stroke Association (![]() ) SA_PDF_21\100017.
) SA_PDF_21\100017.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data produced in the present study are available upon reasonable request to the authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.