
Abstract
Objective
Participation plays a pivotal role in rehabilitation for people with multiple sclerosis. In clinical practice, the International Classification of Functioning, Disability and Health serves as a basis for characterizing participation. However, this framework lacks the subjective perception of participation. This study examines the perceived participation of people with multiple sclerosis and gait impairment through a sense of connection, efficacy, and meaning.
Design
Qualitative research design with focus group and individual interviews.
Setting
Participants were interviewed using an online conference tool.
Participants
Transcripts from four online focus group interviews with people with multiple sclerosis and gait impairment (4–6 participants each, totaling N = 19, aged 33 to 76, with 12 females) and from 12 individual interviews with participants from these focus groups were analyzed.
Intervention
None.
Main measures
Two researchers coded transcripts using qualitative content analysis by Kuckartz.
Results
A sense of connection was about common activities, a sense of inclusion, sameness, familiarity, and contributing to a social system. Experiences of exclusion, otherness, and foreignness were reported. A sense of efficacy ranged from a sense of competence, influence, and independence to a sense of dependence, a lack of spontaneity, and helplessness, leading to refraining from activities. Meaningful activities, sensual experience, a sense of purpose, identity, and equality were related to a sense of meaning.
Conclusions
Perceived participation goes beyond the ability of being involved in life situations. Clinicians following a patient-centered approach can incorporate the presented perspective of people with multiple sclerosis and gait impairment on participation into their clinical action.
Introduction
Multiple sclerosis is a degenerative disease of the central nervous system 1 with increasing prevalence. 2 Symptoms impact various physical and mental functions. 3 People with multiple sclerosis and gait impairment are especially vulnerable to participation restrictions. 4 Studies show that mobility impairment negatively impacts the quality of life and activities of daily living of people with multiple sclerosis.5,6 Maintaining and improving participation is thus a central element of rehabilitation processes. 7 Yu and Mathiowetz 8 argue that individualized and participation-oriented interventions are particularly valuable for people with multiple sclerosis. In their paper on reviews focusing on rehabilitation interventions and participation among people with multiple sclerosis, Momsen et al. 9 conclude that, due to the progressive nature of multiple sclerosis, it is essential to incorporate the person's perspective into rehabilitation processes, and future research should focus on related experiences of people with multiple sclerosis.
Following the International Classification of Functioning, Disability and Health (ICF), participation is defined as “involvement in a life situation,” 10 (p.14). A subjective side to that involvement 10 is being acknowledged but not included. Studies bring forth the idea of expanding the ICF by this emotion- and perception-based dimension of participation.11–14 The social identity approach to health and well-being 15 can serve as such a complementary approach. 16 Following this approach, social identities originating from social group memberships can positively impact health through (1) a sense of connection, (2) a sense of meaning, (3) a sense of efficacy, and (4) social support.15,17 While the ICF offers a framework for determining how a person is involved in a life situation, the social identity approach to health and well-being can help answer how respective involvement is perceived. 16 Against this background, the following research question will be investigated: How do people with multiple sclerosis and gait impairment subjectively perceive participation in terms of a sense of connection, efficacy and meaning?
Methods
A qualitative research design encompassing semi-structured online focus group interviews and individual interviews with people with multiple sclerosis and gait impairment was chosen. Focus group and individual interviews can complement each other by not only allowing for the emergence of collective insights but also creating a protected space in the individual interview, where subjective experiences and feelings can be addressed that might not be raised in the group setting. 18 The focus group interviews took place as part of the project Multiple Sclerosis—Patient-oriented care in Lower Saxony (grant number: 01VSF19046). 19 Ethical approval was obtained from the corresponding Research Ethics Committee (Research Ethics Committee of the Hannover Medical School, reference number 9173_BO_K_2020; Faculty of Health Sciences, University of Oldenburg, Germany, reference number 2020-108 and 2021-077). This study was registered with the German Clinical Trials Register (Number: DRKS00025532).
Recruitment and data collection
The purposive sampling strategy consisted of: (1) recruitment for focus group interviews, followed by (2) recruitment for individual interviews among the participants of the focus group interviews. The German Multiple Sclerosis Society Lower Saxony sent out invitations for the focus group interviews to 433 members living with multiple sclerosis. Participant selection was based on pre-defined inclusion criteria encompassing (a) 18 years of age or older, (b) sufficient knowledge of the German language, (c) diagnosed with multiple sclerosis, and (d) owning or being in the immediate process of receiving a walker, manual wheelchair, or electric wheelchair/scooter. If the number of requests outnumbered the size of the focus group, participants were selected based on a balanced composition of demographic and clinical characteristics in the focus groups. Out of 29 people interested, nine people did not fulfil the selection criterion d (n = 6) or the intended group composition (n = 3). One participant could not participate due to technical problems. In sum, 19 people with multiple sclerosis and gait impairment took part in an online focus group interview. Of these 19 participants, 13 were also interviewed individually. Informed consent was obtained for both the focus group interviews and the additional individual online interviews.
Focus group interview questions revolved around the experience of participation. The individual interview guide focused on the participant's most important participation area and associated senses of connection, efficacy, and meaning 15 (Supplemental material A: Interview guides). The interview guide for the focus group interviews was pilot tested with people with multiple sclerosis. The individual interview guide was tested with the first participant and proved suitable. The focus group interviews and individual interviews took place between May and August 2021 using an online conference tool. Pre-meetings with the participants to test the online conference tool and explain the purpose of the study were held. A subsection of each focus group interview lasting between 20 and 32 min was analyzed for the present research question. Individual interviews lasted between 18 and 56 min.
Data analysis
The focus group interviews and individual interviews were transcribed verbatim. Two researchers (EMD and NR) analyzed the data using qualitative content analysis as described by Kuckartz, 20 allowing for structuring the data material stepwise both deductively and inductively. The steps that were carried out are outlined in more detail in the following paragraphs. The data analysis software MAXQDA 2022 21 was used.
Interviews were split into two sets. The first set was coded independently by EMD and NR with the main categories: sense of connection, sense of efficacy, or sense of meaning 15 (Table 1) (step 1: deductive coding). A text passage was coded with one of the three main categories if the sense was experienced in the context of one of the nine activities and participation domains listed in the ICF 10 : (1) Learning and applying knowledge, (2) General tasks and demands, (3) Communication, (4) Mobility, (5) Self-care, (6) Domestic life, (7) Interpersonal interactions and relationships, (8) Major life areas, (9) Community, social and civic life. The coding was compared after each transcript and discussed until a consensus was established. The second set of interviews was then coded with the main categories by EMD. NR checked the coding, and disagreement was discussed until a consensus was found.
Main categories deductively developed based on the social identity approach to health and well-being 15 and subcategories inductively developed during fine-coding.
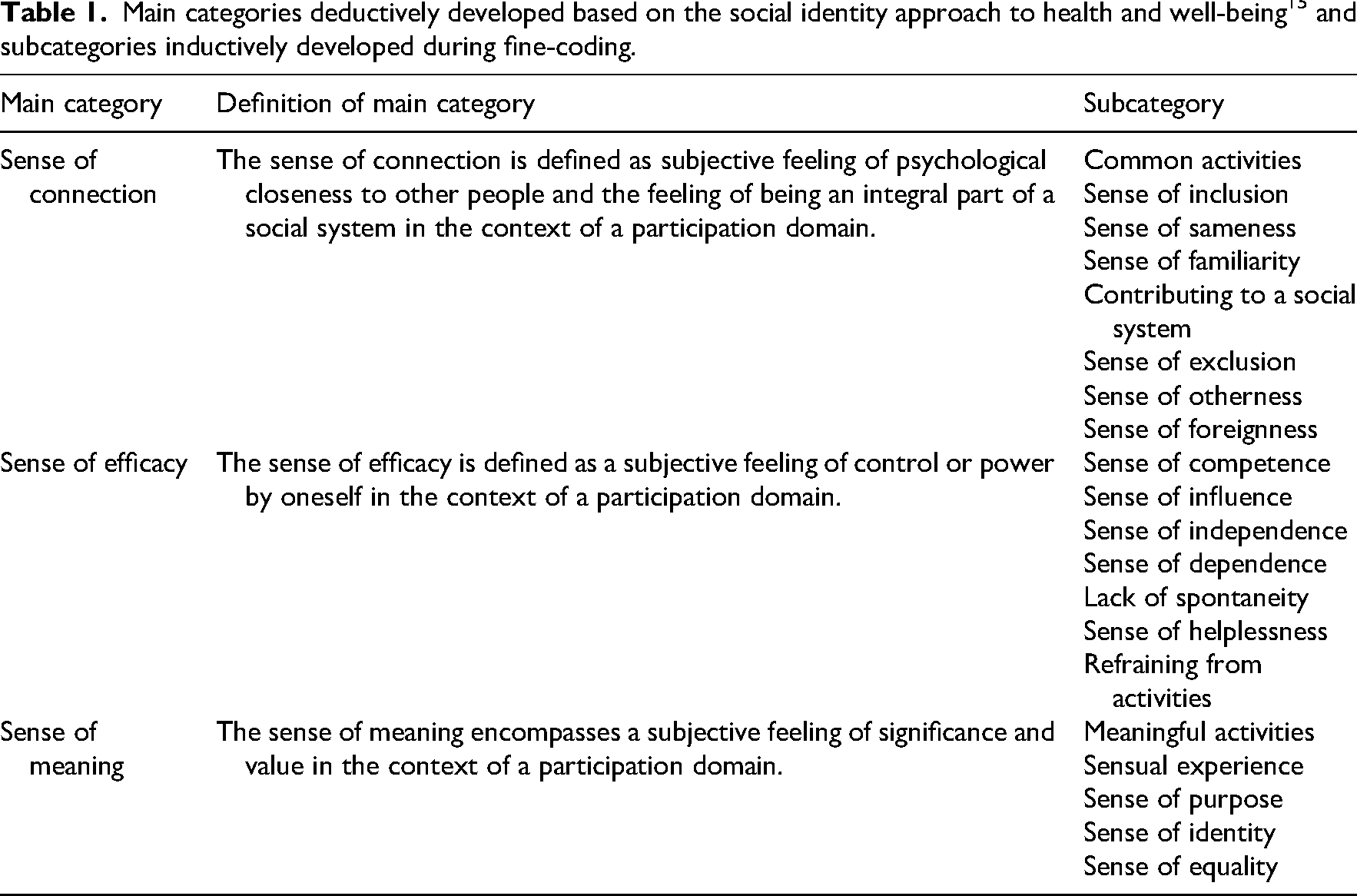
Inductive fine coding (step 2) was then carried out to grasp variations of the three senses. First, possible subcategories were developed by EMD and NR. EMD, NR, and ALB discussed the resulting subcategories until a consensus was found. Then, EMD and NR fine-coded interviews independently, resulting in a Kappa = 0.62. 22 Because the intercoder reliability was identified as good, 20 EMD fine-coded the remaining interviews, and NR checked the coding of each interview.
Two PhD students with a background in psychology (EMD, female) and health sciences (DH, male) moderated the focus group interviews. The individual interviews were conducted by EMD. The transcripts of both the focus group interviews and individual interviews were analyzed by EMD and NR (female, a studied occupational therapist). All researchers were trained in conducting qualitative research. The consolidated criteria for reporting qualitative research (COREQ) checklist 23 served as an orientation for this study.
Results
The final sample encompassed 19 participants who reported being diagnosed with MS diagnosis for between 2 and 33 years. They relied on various mobility assistive devices, such as walkers or wheelchairs. All of them took part in one of the four focus group interviews (4–6 participants each). Thirteen of these 19 participants were also interviewed individually. One individual interview had to be excluded from data analysis due to poor audio quality. The final data set consisted of four transcribed focus group interviews and 12 transcribed individual interviews. Participant characteristics are shown in Table 2.
Sociodemographic and clinical characteristics of participants (n = 19) a .
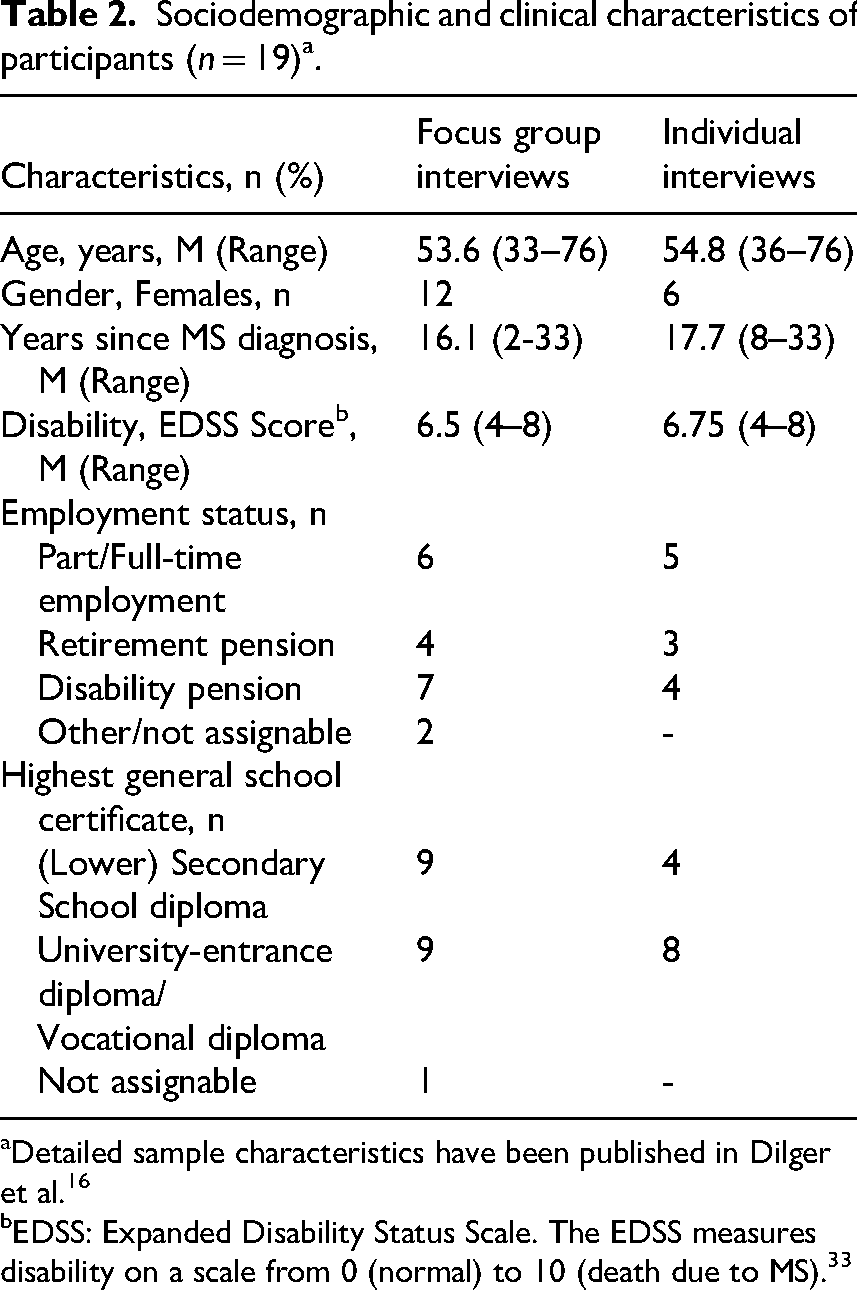
Detailed sample characteristics have been published in Dilger et al. 16
EDSS: Expanded Disability Status Scale. The EDSS measures disability on a scale from 0 (normal) to 10 (death due to MS). 33
The data were analyzed through the lens of the three senses (Table 1, column 1). Subcategories were developed inductively (Table 1, column 3). In sum, 354 text passages were coded (sense of efficacy = 168 codes; sense of connection = 115 codes; sense of meaning = 71 codes).
Sense of efficacy
A sense of efficacy, defined as a subjective feeling of control or power by oneself, 15 in the context of a participation domain, proved to be a major topic in various participation domains.
The interviewees experienced efficacy through a sense of competence, characterized as a feeling of being able to cope well with demands. It draws on the experience of efficiently handling challenges and activities in a participation domain as illustrated by one participant: “(…) at work it [work tasks] simply – it just runs smoothly” (#12, Personal Interview). Mobility and work were mainly addressed by the interviewees when talking about a sense of competence. Experiencing a sense of influence, characterized by the feeling of being able to influence states and decisions, was a distinguishable experience of a sense of efficacy. Both senses occurred individually or collectively, for example, as part of a work team.
A sense of independence from external circumstances or objects in one's own life and action emerged as a distinct part of a sense of efficacy. To have a choice and to act autonomously in the respective participation domain were key experiences associated with this valued sense of independence. However, sometimes, taking part in a participation domain was also accompanied by a sense of dependence on external circumstances or objects, which was, in contrast, perceived as burdensome. In discussing their personal participation experience, the focus group members elaborated on their feelings of dependence and their wish for a higher sense of independence: #8: But, of course, I would rather not [laughs] need a walker. Interviewer #1: #15, did you want to say anything about it? #15: Yes, I also see it that way, that without it [mobility assistive device], you are not really capable anymore, but you want everything to be like it used to be. (Focus Group #2)
The spectrum of experiences of a sense of efficacy also reached a sense of helplessness, in which the participants still attempted to carry out activities but experienced this process as increasingly difficult. The feeling of being unable to cope with the demands was dominating. At some point, the efforts and feelings were too burdensome, so that a person refrained from engaging in an activity after a personal cost-benefit consideration process: Interviewer #2: Could you possibly elaborate a bit further on what kind of emotions that brings up in you? #14: Frustration. [emphasis added] #3: Frustration and you simply stop doing it [participating in life situations with a mobility assistive device]. #9: Exactly. [emphasis added] It is like a mountain that is in front of you and when you are at home and, and, and you realize, or you have gathered information, that there are these difficulties, (…), then you keep hands off it, then you stay at home. (Focus Group #4)
Sense of connection
The sense of connection is defined by a subjective feeling of psychological closeness to other people and the feeling of being an integral part of a social system 15 in the context of a participation domain.
The participants stated that common activities are a relevant part of a sense of connection. The focus was on engaging in activities together with others, resulting in a pleasant feeling. It encompassed activities with friends, family, or colleagues and was mostly about being active together. The nature of the activity was often not the main focus of the interviewees; the process of doing it together is what mattered.
Feeling connected was also perceived through activities where the focus did not lie on the process of carrying out activities together, but on the fact that the activities serve the aim of contributing to a social system: (…) then the colleagues approach you and say: Look, we need this right here, do you have time? So, I also do work that is not only part of my field of work, because I simply belong to the team and for that I also work overhours, if the team needs it. (#12, Personal Interview)
A sense of connection was also about a sense of inclusion. The participants talked about how much they felt included in a social unit, such as a group of people or society in general. Having contact was important and exceeded the mere carrying out of an activity together, as one participant stated when referring to his group of friends as “being right in the middle of it, not just on the sidelines” (#2, Personal Interview). A sense of inclusion also encompassed the feeling of “being accepted” (#11, Personal Interview) and “being taken care of” (#5, Personal Interview). One participant emphasized the importance of this feeling of inclusion for all people with multiple sclerosis and that avoiding loneliness is important.
A sense of exclusion, referring to both a specific group and society as a whole, manifested itself in a loss of social contacts and increasing social isolation.
Comparing oneself to others was an experience leading to a sense of both otherness and sameness. A sense of sameness revolved around situations in which the interviewees felt similar to others and in which distinction due to multiple sclerosis-related symptoms was not in the foreground. One participant described trying to actively elicit this sense of sameness by concealing the symptoms and thus producing social situations in which differences vanish: During a conversation, when I get together with others, I also try to conceal it a bit (…) I am, so to say, a seating height, which means that if I sit, then you don’t really see it (…) so when I sit, I can – if you may say it like that – have a normal conversation (…). (#9, Personal Interview) And there are those difficulties that come up again and again and show me: “Look, you’ve got your MS [multiple sclerosis]” and, well, that way, you realize, that you are not really equal, equally worthy – no worth, that's not the right expression – that you just cannot hear, talk, sit on the same level like others. (#9, Personal Interview)
In various areas of life, especially with friends, family, and work, a sense of connection was perceived through a sense of familiarity, often described as knowing each other “for an eternity.” The interviewees described how they grew into the illness together with others, which led to no major changes in interpersonal contact despite the growing impact of multiple sclerosis on physical functioning. Knowing the people with multiple sclerosis prior to or at the onset of multiple sclerosis was relevant to the development of a sense of familiarity. In contrast, one interviewee described a sense of foreignness when finding oneself in a new situation with people who do not know about the illness.
Sense of meaning
A sense of meaning encompasses a subjective feeling of significance and value 15 in the context of a participation domain.
The participants described meaningful activities as a source of a sense of meaning. Some participants reflected on the degree of sense of meaning experienced when an activity is carried out. The following participant emphasized that the activity should not simply be carried out but should be carried out in a meaningful way: “So that my [partner] and I can spend a whole day somewhere again. Yes, without having to just sit somewhere on a bench or something like that, that we are actually able to look at something” (#19, Focus Group #3).
The perception of sensual experiences—such as hearing or seeing—during activities emerged as a facet of participation, as one participant illustrates: “The beauty, that I can virtually see, sense, feel it with my own eyes and my own ears and to process it by myself instead of hearing it from others” (#2, Personal Interview).
According to the interviews, a sense of meaning was also about a sense of identity formed through participation in relevant life roles. The participants described how participation domains offer space for unfolding and developing one's own identity, independent of multiple sclerosis: (…) when I am on the street, I am the [person] with the wheelchair. But at [workplace], I am the [person] from [workplace location] or I am [name of participant] so there I am [emphasis added] a person and not limited to the MS [multiple sclerosis] or the wheelchair. (#12, Personal Interview)
While a sense of identity focused on the individual's self, a sense of purpose referred to a feeling that one's actions contribute to a higher societal objective that goes beyond oneself.
A sense of meaning was, from the interviewee's perspective, also about a sense of equality that embraced a feeling of equal worth of oneself in relation to other social groups or society in general. Sometimes, the participants pronounced that their feeling of being equal in relation to all of society is impaired in an all-encompassing way: The feeling is – it is often said that everything should be done so that in everyday life, we feel the same as others and so on, but that is all nicely said on the paper (…) but then the feeling, that you are not actually taking part everywhere – nobody can really take it away from you. (#9, Personal Interview)
Discussion
The results suggest that people with multiple sclerosis and gait impairment experience a sense of connection, efficacy, and meaning 15 in various forms: A sense of efficacy ranged from feeling competent, influential, and independent to experiences of dependence and lack of spontaneity. A sense of efficacy could be impaired when one felt helpless, which could lead to a trade-off process resulting in completely refraining from an activity. Similarly, a sense of connection ranged from high psychological closeness in terms of feeling included, experiencing a sense of sameness, or being able to contribute to a social system, which was accompanied by positive feelings through common activities, to low psychological closeness, when a sense of exclusion, otherness, and foreignness occurred. A sense of meaning was experienced through meaningful activities, sensual experience, a sense of purpose and identity, and a sense of equality. The senses partly express themselves in opposing sensual poles (sense of exclusion and inclusion, sense of dependence and independence, sense of sameness and otherness, sense of helplessness and competence).
The different facets of a sense of connection, efficacy, and meaning were frequently accompanied by strong expressions of positive and negative affect. This is in line with assumptions of the social identity approach to health and well-being, which indicate that meaning, connection, and efficacy are resources for enhanced health and well-being, while an impaired feeling is connected to impaired health and well-being. 15 Social groups and common activities, frequently mentioned by participants of this study, were also found to be relevant to adjusting to a changed life with multiple sclerosis. 24 The participants describe how a sense of helplessness precedes the process of refraining from activities. Talking about when a sense of helplessness is experienced could help clinicians and patients to identify options to adapt the activity so that the person does not need to withdraw from it. The results also show that a sense of equality was fostered when the needs of people with multiple sclerosis were considered. Participatory approaches can highlight the perspectives of people with multiple sclerosis and gait impairment and lead to creating inclusive environments that are important for participation, such as workplaces.
The results share common ground with those of other studies that investigated perceptual facets of participation among populations with chronic illness or physical impairment, for example, people with early rheumatoid arthritis, 14 people with spinal cord injury, 25 and people with physical disabilities, 26 in which, for example, a sense of belonging and influence 14 or a sense of control 25 and mastery 26 was reported. The results could be the basis for the development of a checklist for use in clinical practice covering perceptual facets of participation of people with multiple sclerosis.
The study has some limitations that need to be considered. Although only a limited number of people responded to the invitation, a heterogeneous sample was reached with regard to gender, age, and form of multiple sclerosis. Due to the sampling considering assistive devices, our participants report moderate to severe disability, as well as an average of more than 16 years since the onset of multiple sclerosis. The methodologically rigorous process of data analysis by researchers with an interdisciplinary background, including independent coding and regular reflection and discussion sessions, ensures confidence in the presented results. All participants were members of the German Multiple Sclerosis Association Lower Saxony. This might be associated with a higher motivation to share information about the illness experiences and more access to resources, such as information. Also, disability was measured through self-assessment, 27 which might have yielded different values than if it had been assessed objectively. 28
The results indicate that although participation is sometimes objectively possible, it might not be perceived as fulfilling. This is in accordance with a study showing that the frequency of involvement in a participation domain is less strongly associated with physical and mental health measures in people with multiple sclerosis than the level of self-efficacy to participate in that activity. 29 This highlights the need for clinicians to consider both objective and subjective dimensions of participation when designing interventions, because they might differ.
In conclusion, the experience of participation of people with multiple sclerosis and walking difficulties encompasses a subjective perspective. While the ICF had been developed with the aim of increased inclusion of the patient's perspective,
30
this aim has not been implemented consistently. The person's own perspective, personal expertise, and feelings are conceptual elements of person-centredness
31
which is a key characteristic of effective rehabilitation.
32
Based on our study, perceptions mirroring the perspective of people with multiple sclerosis and walking difficulties on participation can be used for research and clinical action. It complements the literature of objective measures with the subjective component. Our study can serve rehabilitation service providers to develop interventions and to have a shared language and understanding of aspects of perceived participation in interdisciplinary teamwork of health professionals.
Clinicians employing a patient-centered approach can gain insights into the subjective perspective on participation of people with multiple sclerosis and gait impairment. Objective participation does not necessarily correspond with the perception of participation. How participation is experienced depends on the context and the feelings that arise. When developing and evaluating interventions for people with multiple sclerosis, clinicians should incorporate the subjective perspective on participation. This includes aspects such as a sense of independence, competence, and inclusion.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155261458318 - Supplemental material for How do people with multiple sclerosis who have walking difficulties perceive participation? A qualitative analysis
Supplemental material, sj-docx-1-cre-10.1177_02692155261458318 for How do people with multiple sclerosis who have walking difficulties perceive participation? A qualitative analysis by Anna Levke Brütt, Elise-Marie Dilger, Nadja Reeck, Dyon Hoekstra and Annett Thiele in Clinical Rehabilitation
Footnotes
Acknowledgements
Our thanks go out to all study participants for sharing their experiences. We would like to specifically thank Anja Grau from the German Multiple Sclerosis Society Lower Saxony for the recruitment of the participants for the focus group interviews. We would like to thank Robin Forstenhäusler for transcribing the individual interviews of this study. We would also like to thank all members of the MS-PoV research group for the discussion and reflection processes within the MS-PoV project.
Author contributions
Conceptionalization: EMD, ALB. Methodology: EMD, ALB. Analysis: EMD, NR, ALB. Investigation: EMD, DH, ALB. Writing—original draft: EMD. Writing—review and editing: EMD, NR, DH, AT, ALB. Supervision: ALB, AT.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Federal Joint Committee's Innovation Fund under Grant 01VSF19046 (funding recipients: Hanover Medical School, Institute for Epidemiology, Social Medicine, and Health Systems Research (Consortium Leader); University of Oldenburg, Junior Research Group for Rehabilitation Science and Research Group for Education and Didactics in chronic and progressive diseases and physical disabilities, German Multiple Sclerosis Society Lower Saxony, Health Services Research Unit, AOK Lower Saxony and MS Research and Project Development gGmbH (all Consortium Partners)) and the German Pension Insurance Oldenburg-Bremen (funding recipient: University of Oldenburg for installing the Junior Research Group for Rehabilitation Science).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
For protecting the identity of the participants, the transcripts of the focus group and individual interviews are not publicly accessible. Further anonymized excerpts for specific categories can be obtained by contacting the first author, upon giving a comprehensible rationale.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.