
Abstract
Objective
This study aimed to implement and evaluate a structured, team-based approach to integrating sexual health into stroke rehabilitation using the Permission-Limited Information-Specific Suggestions-Intensive Therapy model, operationalized through the Stroke Sexual Health Practice Profile.
Design
Quality Improvement Initiative.
Setting
Ontario, Canada.
Participants
Patients attending inpatient or outpatient stroke rehabilitation.
Intervention
The Stroke Sexual Health Practice Profile was developed collaboratively by an interprofessional team and implemented within a stroke rehabilitation program. It outlined standardized practices across the Permission-Limited Information-Specific Suggestions-Intensive Therapy framework, including scripts, educational materials, and documentation protocols.
Main measures
Outcomes included staff knowledge, comfort, and approaches to addressing sexual health, participation in educational activities, patient awareness and comfort discussing sexual health, and documentation of sexual health practices in clinical charts.
Results
Preimplementation surveys identified gaps in patients’ awareness of poststroke sexual health and providers’ confidence in addressing it. Among eligible staff, 86.3% completed online modules and 62.1% attended workshops, which were associated with significant improvements in knowledge and comfort. These gains were partially sustained at 6 months. Postimplementation patient surveys demonstrated improved awareness and comfort discussing sexual health. Chart audits showed increased documentation of sexual health discussions over time.
Conclusions
The Stroke Sexual Health Practice Profile supported integration of sexual health into stroke rehabilitation by improving clinician knowledge and confidence and increasing documentation of care. Sustained improvements may require ongoing reinforcement and system-level supports.
Introduction
Sexual health is a fundamental component of overall health and well-being, encompassing physical, emotional, and relational dimensions.1,2 For individuals who have experienced a stroke, impairments such as hemiparesis, aphasia, fatigue, and changes in body image or mood changes can significantly affect sexual function, intimacy, and identity. Despite these challenges, sexuality remains an important aspect of quality of life across the lifespan.3,4
International clinical guidelines emphasize that stroke survivors should receive education and counseling regarding the impact of stroke on relationships, intimacy, and sexual functioning.5,6 These recommendations are reflected in the Canadian Stroke Best Practice Recommendations, which advocate for structured opportunities to discuss sexual health throughout the continuum of care, beginning in inpatient rehabilitation and extending into community reintegration. 7 Discussions should address physical, psychological, and relational factors, and be tailored to individual needs, including cognitive or communication impairments. 7 These recommendations emphasize that discussions of sexuality should be initiated early, revisited throughout recovery, and tailored to the individual's preferences, abilities, and relational context, highlighting the need for consistent, team-based approaches.
Despite these clear recommendations, implementation remains inconsistent in practice.8–11 Sexual dysfunction and dissatisfaction are common after stroke, yet many patients report receiving little or no information or support. 12 Barriers to integrating sexual health into rehabilitation include limited provider training, discomfort initiating discussions, unclear team roles, and lack of resources.4,13,14 System-level factors including absence of formal policies, time constraints, and implicit assumptions about sexuality in older or disabled adults further contribute to this gap.13,14 Recent studies continue to report practice gaps, suggesting limited progress in translating guideline recommendations into routine care.4,10 Although addressing sexual health has been associated with improved quality of life and relational outcomes,4,15 it is not routinely embedded within stroke rehabilitation care.
To address these challenges, a quality improvement initiative was undertaken at a tertiary rehabilitation hospital in Ontario, Canada to integrate sexual health into routine stroke rehabilitation practice. This initiative built on prior work within a spinal cord injury program, where a structured, team-based approach improved provider confidence and normalized sexual health discussions. 16 The stroke rehabilitation program was selected for adaptation due to the substantial unmet need among stroke survivors and alignment with best practice guidelines. 7
The intervention involved developing and implementing the Stroke Sexual Health Practice Profile, a structured, interdisciplinary approach designed to operationalize sexual health care across the rehabilitation continuum. The Practice Profile was informed by the PLISSIT model (Permission, Limited Information, Specific Suggestions, Intensive Therapy), 17 which provides a tiered framework for addressing sexual health within clinical practice, and was adapted to support role clarity, timing of interventions, and integration into routine workflows. It has been widely applied across diverse clinical populations, including oncology, chronic disease, and rehabilitation settings, to support clinician confidence and communication.16,18–20
The aim of this study was to implement and evaluate this structured, team-based approach to sexual health in stroke rehabilitation. Specifically, the initiative sought to: (1) improve provider knowledge, comfort, and approaches to addressing sexual health; (2) increase consistency of sexual health practices across the interdisciplinary team; and (3) enhance patient access to sexual health education and support throughout rehabilitation.
Methods
Design and setting
This quality improvement initiative was conducted at a tertiary rehabilitation center in Ontario, Canada, and included inpatient, outpatient, and community stroke rehabilitation services. The inpatient program includes 26 beds and serves approximately 250 patients annually, with an additional 250 outpatient and 450 community referrals per year. Care is delivered by an interdisciplinary team including physicians, nurses, occupational therapists, physiotherapists, social workers, speech-language pathologists, and other allied health professionals. Ethics approval was obtained from the Western University Health Research Ethics Board (Project ID 124798).
Implementation framework
The initiative was guided by the Active Implementation Frameworks developed by the National Implementation Research Network, which emphasize staged implementation, use of implementation teams, and iterative improvement cycles. 21 The intervention was informed by the PLISSIT model 17 and the Sexual Rehabilitation Framework, 22 which together support a structured, biopsychosocial, and team-based approach to addressing sexual health in rehabilitation.
Intervention: Stroke sexual health practice profile
The intervention consisted of the development and implementation of the Stroke Sexual Health Practice Profile, a structured interdisciplinary approach designed to integrate sexual health into routine care. The profile operationalized the PLISSIT model across the rehabilitation continuum by defining when and how sexual health should be addressed, and by whom.
It included standardized scripts to support clinicians in initiating conversations, stroke-specific patient education materials (including aphasia-friendly resources), and documentation processes embedded within the electronic medical record. The profile outlined key practice components, including early permission-giving, provision of tailored information, identification of patient-specific goals, and integration of sexual health into discharge planning and referrals.
Implementation process
Implementation followed six stages: exploration, team formation, assessment of current practice, development of the practice profile, action planning, and initial implementation.
Needs were identified through informal feedback from patients and staff, who reported limited opportunities to discuss sexual health and uncertainty regarding roles. An environmental scan of rehabilitation programs across Ontario and Canada revealed substantial variability in practice, with common gaps including lack of structured approaches, limited staff training, and absence of standardized resources.
An interdisciplinary implementation team was established, including clinicians, leadership, individuals with lived experience, and implementation science support personnel.
Preimplementation surveys were conducted with staff and patients to assess baseline knowledge, comfort, perceived roles, and access to sexual health information. These surveys included items on clinician confidence in addressing sexual health domains and patient awareness of available resources.
Using practice profile mapping,21,23 the team defined a structured approach to sexual health across care phases. Stroke-specific adaptations included communication strategies for individuals with aphasia, integration of sexual health into self-care and participation goals, and alignment with interdisciplinary documentation and discharge planning processes. Roles were defined across disciplines to support consistent delivery. Detailed components of the Stroke Sexual Health Practice Profile are provided in Supplement A.
Priority drivers were identified through team consensus informed by baseline data, focusing on staff competency, organizational supports, and workflow integration. A multi-component education strategy was implemented, including introductory sessions, interactive workshops, and e-learning modules. Content addressed stroke-specific considerations such as cognitive and communication impairments, fatigue, medication effects, and safety considerations in resuming sexual activity.
The practice was launched in April 2022 and refined through Plan-Do-Study-Act cycles over 6 months. Feedback from patients and staff informed iterative adjustments, including modifications to timing, documentation processes, and approaches to sensitive discussions.
Evaluation
Implementation and associated outcomes were evaluated using a multimethod approach including staff surveys, patient surveys, and chart audits. Staff surveys were administered at preworkshop, postworkshop, and 6-month follow-up timepoints, and included the Knowledge, Comfort, Approaches, and Attitudes towards Sexuality Scale (KCAASS) 11 alongside additional items assessing perceived roles, knowledge of resources, and comfort discussing sexual health. Patient surveys assessed comfort discussing sexual health, perceived opportunities to engage in these discussions, and awareness of available resources during rehabilitation. Chart audits were conducted to evaluate documentation of key components of the practice profile, including permission-giving, sexual health goal-setting, and discharge planning. Qualitative data were also collected through open-ended survey responses and voluntary focus groups conducted following implementation. These data were analyzed using descriptive thematic analysis to identify common patterns in staff experiences and perceptions. Changes in KCAASS scores across timepoints were analyzed using Kruskal-Wallis tests, with post hoc Dunn's tests and Bonferroni correction applied as appropriate. Documentation rates were summarized descriptively.
Results
Implementation overview
The Stroke Sexual Health Practice Profile was implemented across inpatient, outpatient, and community stroke rehabilitation programs using a structured, interdisciplinary approach. The intervention operationalized the PLISSIT model across the patient care trajectory.
Preimplementation surveys
Prior to implementation, 44 patients completed a survey assessing perceptions of sexual health in rehabilitation. The cohort included 21 females and 23 males, with a mean age of 65.0 years (SD = 16.8). Over half of participants (54.5%) reported that sexual aspects of life were “important” or “very important.” However, only 54.5% indicated awareness of how their neurological condition could affect sexual health, and 31.8% were unaware that individuals with neurological conditions can lead satisfying sex lives. While most patients (81.8%) reported comfort discussing sexual health with a partner, fewer (63.6%) felt comfortable discussing these issues with the healthcare team. Notably, 72.7% indicated insufficient opportunities to discuss sexual health during their care, and 54.5% were unaware of available support resources.
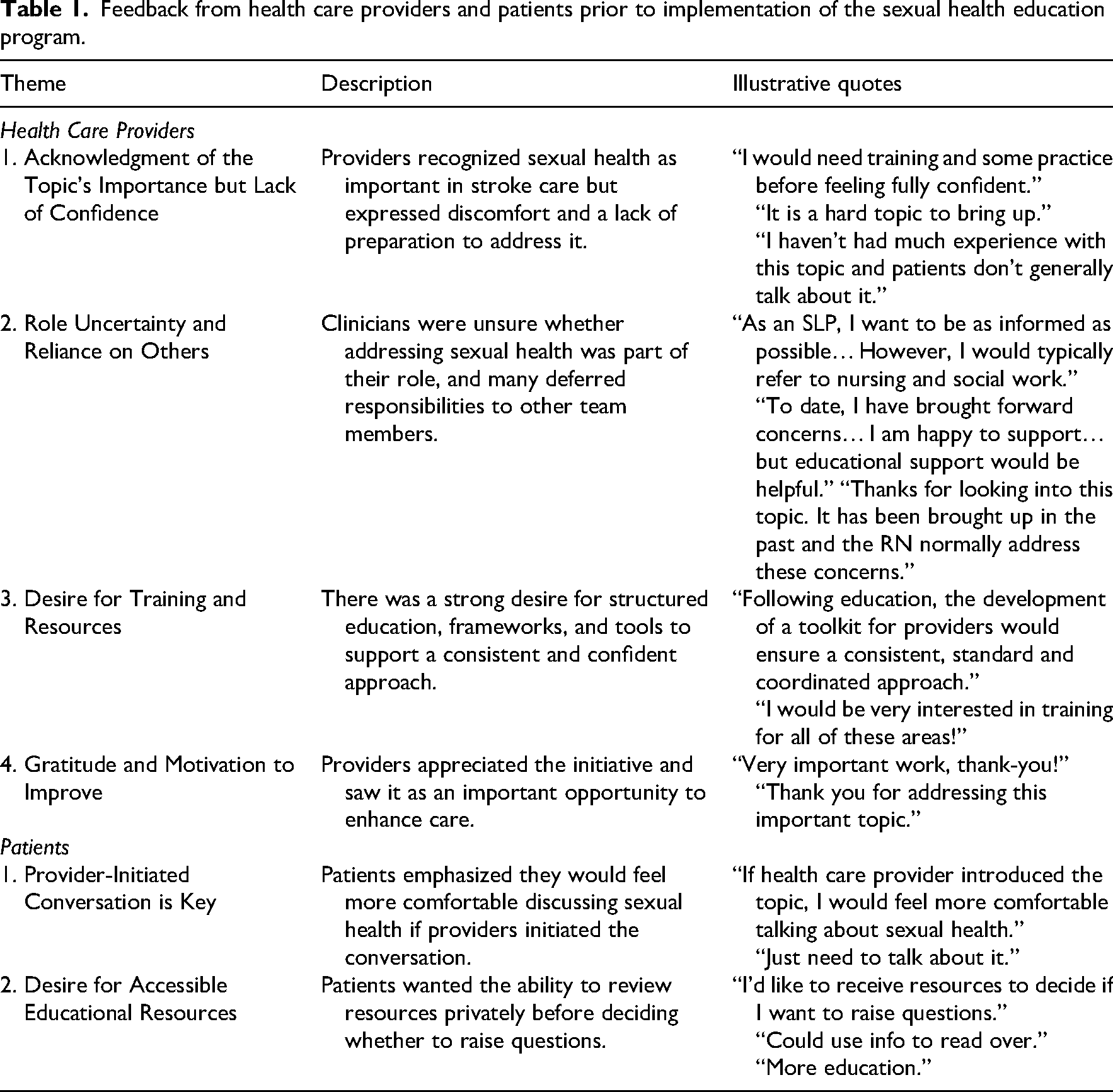
Fifty-two healthcare providers completed the preimplementation survey, representing a range of disciplines and experience levels. Although 32.7% of providers reported that addressing sexual health was part of their role, only 28.8% felt comfortable engaging in such discussions, indicating a gap between perceived responsibility and confidence in practice. Across domains of sexual health, a substantial proportion of providers reported low confidence or uncertainty (Figure 1). Additional qualitative feedback from patients and providers is summarized in Table 1.
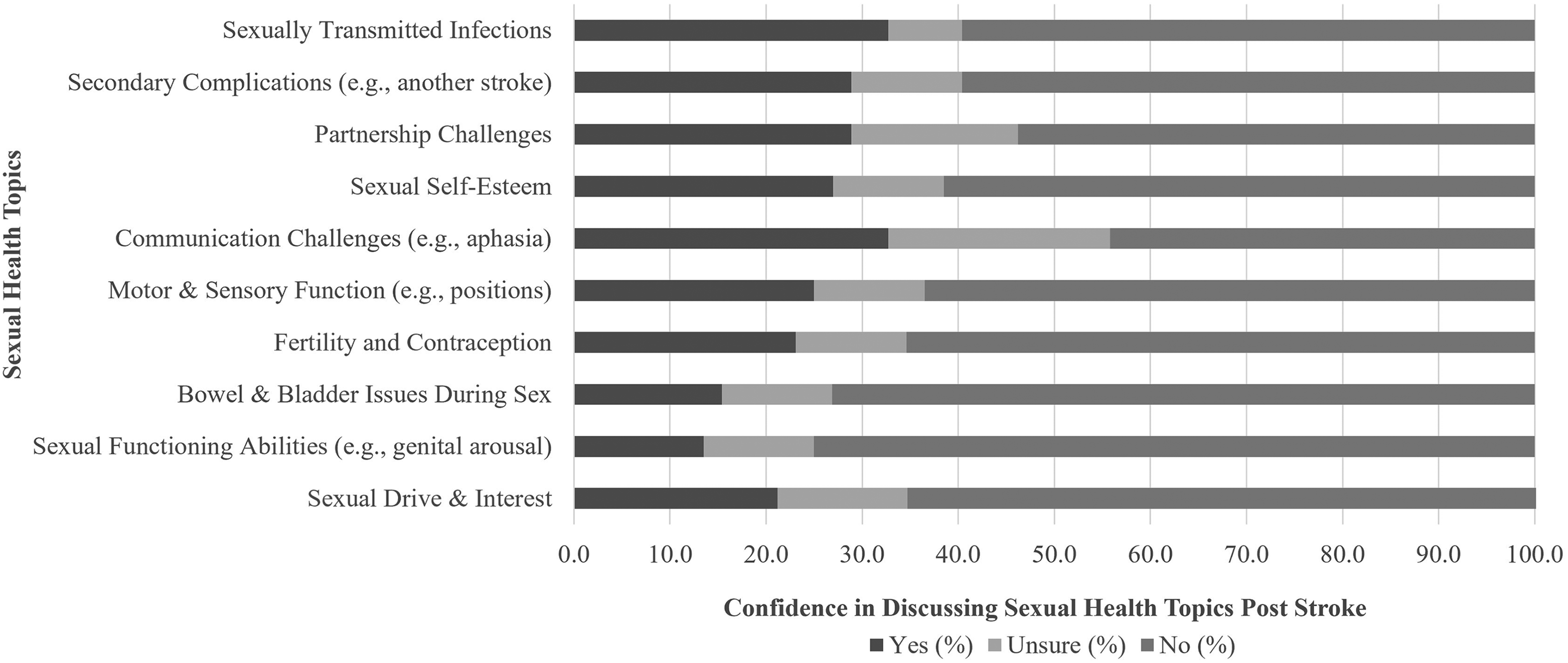
Health care providers’ confidence discussing aspects of poststroke sexual health prior to implementing the sexual health program (N = 52).
Feedback from health care providers and patients prior to implementation of the sexual health education program.
Postimplementation patient survey
Following implementation, 21 patients completed a survey at discharge from inpatient or outpatient rehabilitation. The cohort had a mean age of 67.0 years and included 11 women and 10 men. Compared to preimplementation findings, a greater proportion of patients reported awareness of how their condition could affect sexual health (71.4% aware or very aware) and that individuals with neurological conditions can lead satisfying sex lives (71.4% aware or very aware). Most patients (76.2%) reported comfort discussing sexual health with a partner, and over half (52.4%) reported comfort discussing these concerns with the healthcare team. Opportunities to discuss sexual health remained variable, with 33.3% reporting sufficient opportunities and 52.4% reporting insufficient opportunities. Awareness of available resources improved modestly, with 33.3% reporting awareness and 14.3% reporting being “very aware.” Among those who accessed resources, the majority found them beneficial.
Implementation evaluation
Of 95 eligible staff, 82 (86.3%) completed the online sexual health learning modules. Qualitative feedback from open-ended survey responses and focus groups was analyzed using descriptive thematic analysis. Participants reported increased awareness, confidence, and comfort in addressing sexual health as part of stroke rehabilitation. Key themes included the normalization of sexual health within care, acquisition of practical language for initiating conversations, and appreciation for applied learning through patient scenarios and discipline-specific content. Participants also identified areas for improvement, including the need for more concise and interactive modules, simplified physiological explanations, and additional guidance on managing complex situations such as inappropriate behavior or communication barriers. Expanded thematic findings and illustrative quotes are provided in Supplement B.
A total of 80 healthcare providers completed the preworkshop survey, 73 attended the workshop and completed the postworkshop survey, and 22 completed the 6-month follow-up survey. Responses were collected at each timepoint, with varying participation across surveys.
Kruskal–Wallis H tests revealed significant differences across timepoints in Knowledge, Comfort, and Approach subscale scores, but not Attitude scores (Table 2). The largest effect was observed for Knowledge, with significant improvements from pre- to postworkshop and sustained gains at 6-month follow-up. Comfort and Approach scores also increased significantly following the workshop; however, these gains were not maintained at follow-up. Attitude scores remained stable across all timepoints.
Kruskal–Wallis H test and Dunn's post hoc comparisons for KCASS subscale scores across three timepoints (preworkshop, postworkshop, and 6 months follow-up).
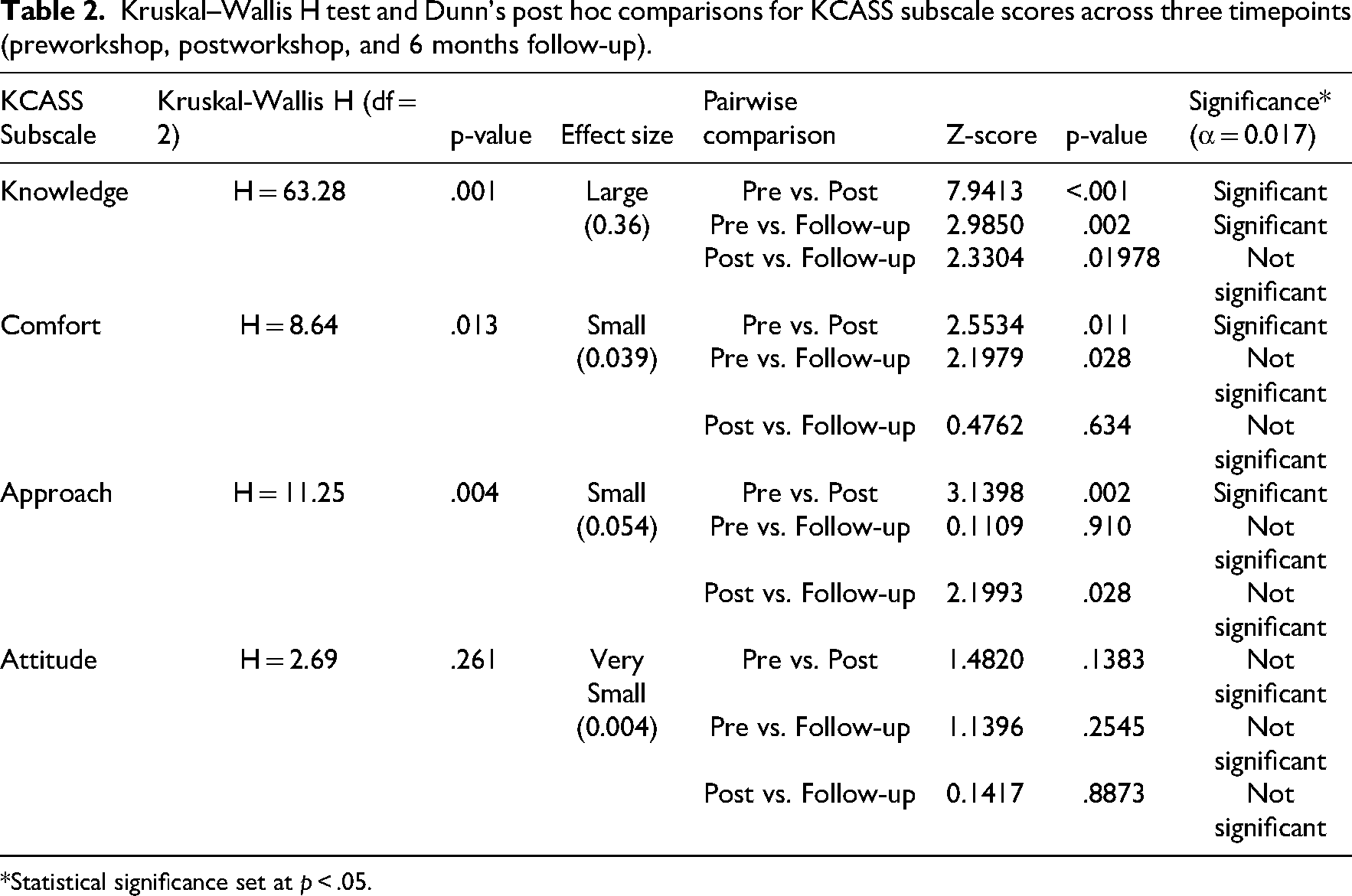
*Statistical significance set at p < .05.
Visual inspection of score distributions (Figure 2) supported these findings, demonstrating increases in Knowledge, Comfort, and Approach following the workshop, with partial attenuation at follow-up.
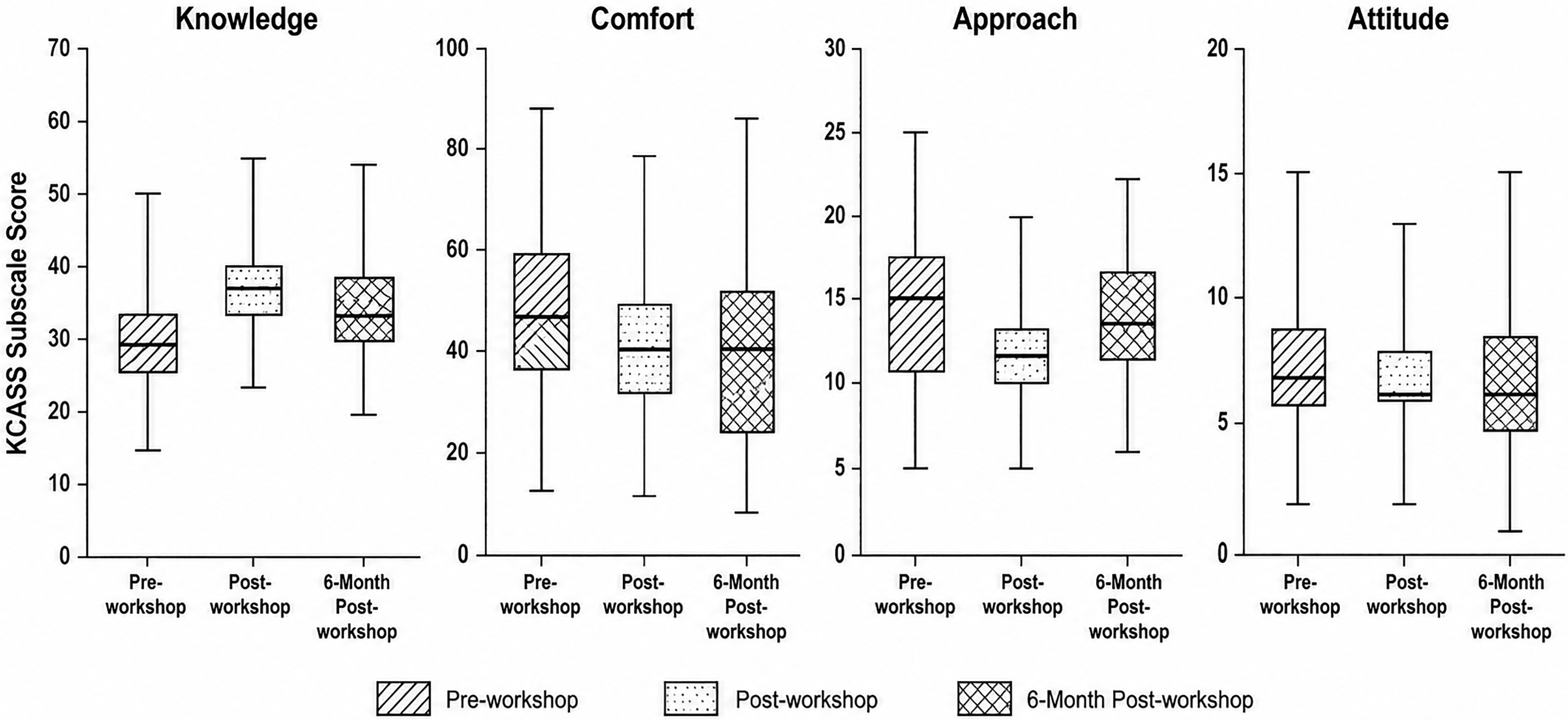
Box plots illustrating distributions of KCASS subscale scores (knowledge, comfort, approach, and attitude) across three timepoints: preworkshop, postworkshop, and 6-month postworkshop. Each box represents the interquartile range (IQR) with the horizontal line indicating the median. Whiskers extend to the most extreme data points within 1.5 × IQR; individual points beyond this range are plotted as outliers. The plots visually reflect the observed trends: a marked increase in Knowledge, Comfort, and Approach scores following the workshop, with partial retention at follow-up, and relatively stable Attitude scores over time.
Chart audits were conducted over two consecutive 3-month periods following implementation. In the first period, 64 of 95 charts (67.4%) included documentation of permission-giving. In the second period, 77 of 98 charts (78.6%) included documentation in the second period. Overall, 73.1% of charts included documentation of permission-giving across both periods. Documentation of sexual health in discharge summaries was higher in the second period, increasing from 45.8% (38/83) in the first period to 66.3% (53/80) in the second period. Overall, 55.8% of charts included discharge documentation related to sexual health.
Discussion
This quality improvement initiative aimed to integrate sexual health education into stroke rehabilitation by enhancing clinicians’ knowledge, confidence, and engagement with the topic. Of 95 eligible staff, 62.1% attended an in-person workshop and 86.3% completed online modules. Participants demonstrated significant short-term gains in knowledge, comfort, and approach to sexual health, with knowledge improvements largely sustained at 6 months. However, comfort and engagement declined over time, approaching baseline levels. While attitudes showed minimal change over time, these were generally positive from the outset. Overall, the intervention was effective in generating immediate improvements; some gains diminished without ongoing reinforcement.
The results of this initiative resonate with those of Low et al., 11 the only other known study to use KCASS in stroke rehabilitation, who conducted a large international survey of stroke rehabilitation professionals. Both studies found that knowledge, comfort, and approach-related confidence are uneven across professional roles, while attitudes toward sexuality are more stable and less amenable to change. Low et al. 11 highlight the complexity of the relationship between education and clinician behavior. Implementation science literature suggests that clinicians develop knowledge and confidence through responding to patient needs in practice, and that training is most effective when embedded within real-world clinical contexts and supported by opportunities for reflection and feedback. 24
Of note, the current study adds to the literature in two novel ways. First, it demonstrated not only short-term gains but also partial retention of knowledge and approach at 6 months postintervention. Second, it examined real-world changes in practice through chart audits, documenting increased permission-giving and improved discharge documentation over time. These objective indicators support the notion that training interventions may support changes in clinical practice, 25 not just shifts in attitudes or self-reported intentions. In contrast to retrospective self-report, our design incorporated both patient perspectives and assessments across multiple timepoints. Baseline patient data revealed a clear demand for opportunities to discuss sexual health, especially among those who felt uninformed about the impacts of stroke on intimacy and function. This is consistent with previous findings in stroke and other neurological populations, reinforcing the need for proactive, structured approaches to clinician education and for integrating sexual health conversations as part of routine care.3,12 These findings are also consistent with a broader pattern observed across chronic disease contexts. A systematic review by McGrath et al. 4 found that health professionals rarely initiate discussions about sexuality, largely due to persistent gaps in confidence, competence, and comfort, further underscoring the need for sexual health training.
The lack of change in attitudes likely reflects a ceiling effect, as baseline attitudes toward addressing sexual health were already positive among participants. In contrast, the observed decline in comfort and approach scores at follow-up highlights the challenges of sustaining behavioral change over time. These findings are consistent with broader implementation literature, which suggests that knowledge acquisition alone is typically insufficient to produce lasting changes in clinical practice.25,26 Sustained improvements in clinician confidence and behavior typically require ongoing reinforcement, opportunities for experiential learning, and integration into routine workflows.24,27 Without continued practice and feedback, initial gains may diminish as competing clinical demands and discomfort with sensitive topics re-emerge. These findings underscore the importance of embedding sexual health training within longitudinal professional development strategies and organizational supports, rather than relying on one-time educational interventions.
Several insights for advancing sexual health in stroke rehabilitation have emerged from this work. First, the significant increase in knowledge immediately following the workshop highlights the value of structured, interactive training for building foundational understanding. However, the partial decline in knowledge and approach scores over time indicates that, to sustain change, clinicians may benefit from ongoing reinforcement through follow-up sessions, resource refreshers, or opportunities for applied practice. The decline in comfort over time suggests that confidence in addressing sexual health may require more than knowledge alone. Comfort likely requires continued engagement and real-world application. Clinical programs should consider integrating practical tools and opportunities for applied learning into routine professional development, as educational interventions alone are unlikely to produce sustained changes in complex clinical behaviors. 26 Notably, participants’ attitudes toward sexual health were already positive and remained stable, suggesting a receptive baseline culture in which to embed these interventions. Finally, the observed improvements in documentation and clinician feedback point to a meaningful shift in practice readiness. Clinical rehabilitation settings should consider implementing system-level supports (e.g., prompts in clinical documentation or clear referral pathways) to normalize and sustain conversations about sexual health as a routine aspect of holistic care.
This study has several limitations. There was no control group so changes in knowledge, comfort, and documentation cannot be definitively attributed to the intervention. Outcomes were measured only up to 6 months postintervention, so long-term sustainability is unknown. Self-reported measures may be subject to bias and do not guarantee behavior change as noted in prior evaluations of educational interventions. 26 Although chart audits offered objective data, documentation may not fully reflect actual clinical practice. Finally, as this was a single-site initiative, findings may not generalize to other settings with different patient populations, professional cultures, or resources. Future research should address these limitations through multi-site, controlled, and longitudinal designs.
Embedding sexual health education into stroke rehabilitation clinical practice is both feasible and impactful. Targeted training improved clinician knowledge and engagement, and early signs of practice change were observed. Sustained improvements require ongoing evaluation, reinforcement, and organizational support. Integrating sexual health as a routine aspect of care can better meet patient needs and promote more holistic, person-centered rehabilitation.
Patients report unmet needs for sexual health discussion during stroke rehabilitation. Structured, team-based approaches can integrate sexual health into routine stroke rehabilitation. Training improves clinician knowledge and confidence but may be insufficient for sustained behavior change. Ongoing reinforcement and system-level supports are required to maintain practice change.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155261459619 - Supplemental material for Implementation and evaluation of a stroke sexual health practice profile for rehabilitation in Ontario, Canada
Supplemental material, sj-docx-1-cre-10.1177_02692155261459619 for Implementation and evaluation of a stroke sexual health practice profile for rehabilitation in Ontario, Canada by Calogero Giurleo, Amanda McIntyre, Anna Kras-Dupuis, Deena Lala and Dalton Wolfe in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155261459619 - Supplemental material for Implementation and evaluation of a stroke sexual health practice profile for rehabilitation in Ontario, Canada
Supplemental material, sj-docx-2-cre-10.1177_02692155261459619 for Implementation and evaluation of a stroke sexual health practice profile for rehabilitation in Ontario, Canada by Calogero Giurleo, Amanda McIntyre, Anna Kras-Dupuis, Deena Lala and Dalton Wolfe in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155261459619 - Supplemental material for Implementation and evaluation of a stroke sexual health practice profile for rehabilitation in Ontario, Canada
Supplemental material, sj-docx-3-cre-10.1177_02692155261459619 for Implementation and evaluation of a stroke sexual health practice profile for rehabilitation in Ontario, Canada by Calogero Giurleo, Amanda McIntyre, Anna Kras-Dupuis, Deena Lala and Dalton Wolfe in Clinical Rehabilitation
Footnotes
Ethical considerations
This study received ethics approval from the Health Services Research Ethics Board at Western University (Project ID 124798).
Author contributions
CG: study conceptualization, data collection, writing, and reviewing. AM: data analysis, writing, and reviewing. AKD: study conceptualization, data collection, and reviewing. DL: study conceptualization, data collection, and reviewing. DW: study conceptualization, writing, and reviewing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors report no conflicts of interest.
Data availability statement
Deidentified data are available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.