
Abstract
Background:
Dignity is a cornerstone of palliative care and represents a complex, multidimensional concept that warrants further conceptual integration.
Aim:
To synthesise evidence regarding patients’ experiences of dignity in palliative care, with a particular emphasis on cultural influenceVs.
Design:
An integrative review was conducted following Whittemore and Knafl’s framework.
Data sources:
Six databases (CINAHL, MEDLINE, ProQuest Sociological Abstracts, PsycINFO, Scopus, and Web of Science) were searched from inception to 28 February 2025. Targeted hand-searches of key journals were performed between March and June 2025.
Results:
A total of 32 articles were included. Patients’ understandings varied but dignity was commonly described as “being treated like a human being.” Three themes were identified: (1) Inner experience, encompassing physical and psychological experiences, self-worth, resilience, and spirituality; (2) Relational and interactional dynamics, including personal autonomy and self-determination, and social relationships and support systems; and (3) Macro-structural determinants, comprising healthcare systems and delivery, as well as economic and socio-political circumstances. Cultural values shaped the perception and preservation of dignity. In collectivist societies, dignity was intricately linked to family, community, religion, and social harmony, whereas in individualist societies, dignity centred on autonomy and control over end-of-life decisions. Immigrants negotiated dignity through interactions between cultural values and healthcare expectations within host countries.
Conclusions:
This review provides an integrated understanding of the factors shaping patients’ perceptions of dignity in palliative care across cultures. The findings could usefully inform patient-centred and culturally sensitive palliative care practices that uphold dignity and promote well-being at the end of life.
In palliative care, the concept of dignity lacks consistent definition.
Patients’ experiences of dignity are influenced by family, social support, and cultural background.
Patients may have varied understandings of dignity in palliative care settings, but the core shared meaning is “being treated like a human being.”
Patients’ experiences of dignity in palliative care are shaped by relational and interactional dynamics, as well as macro-structural determinants.
Cultural background can influence patients’ understandings of dignity, with particular differences between collectivist and individualist societies, as well as immigrant groups.
Healthcare providers need to uphold patient dignity on multiple levels, including individual, interpersonal, and institutional levels.
Culturally sensitive nursing practices help maintain the dignity of different patient groups.
Introduction
Dignity is a complex, multidimensional concept in palliative care, encompassing a person’s sense of self-worth, autonomy, and social recognition in the context of life-threatening illness.1,2 Although dignity is often discussed in ethics as an intrinsic and universal human value, this review focuses on the lived experience of dignity in terms of how it is understood experienced, perceived, and responded to by patients and their families during end-of-life care. Maintaining dignity is closely related to improving patients’ mental health, symptom relief, and quality of life, and can also foster patients’ participation and satisfaction in the care process, ultimately enriching their end-of-life experience. 3 Dignity is also closely associated with patients’ sense of identity, control over their lives, and roles within family and society.4,5 When dignity is compromised, patients are more likely to experience heightened anxiety, depression, and emotional distress, which will further diminish the quality of their end-of-life.4,6
Patients’ lived experiences of dignity are central to effective palliative care. The preservation or loss of dignity is something patients—and their families—experience firsthand. Due to the reality of physical decline and dependence on others, as well as uncertainty about the future, patients in the terminal stage of their illness often experience negative emotions such as anxiety, fear, or helplessness, which are directly related to the maintenance of their sense of dignity.7,8 At this time, family members are often uniquely aware of the patient’s need for dignity. In many cases, they not only offer emotional support, but also advocate for patients in medical decisions and daily care, becoming important supporters of dignity being achieved.9–11 In contrast, the perspectives of healthcare professionals are typically based on clinical observations and assessments, which may not fully capture the patient’s actual experience throughout the course of the illness. 12 As family caregivers provide continuous care and share the experiences of the palliative care process with patients, incorporating both patient and caregiver perspectives is essential for a more comprehensive understanding of the dignity of patients with palliative care needs.
Individual differences and cultural backgrounds profoundly influence patients’ perceptions of dignity.13,14 In addition to common influencing factors such as personal experiences, social relationships, care tenor, patients’ understanding of dignity may also vary due to differences in cultural norms, religious beliefs, and social environment. 15 Dignity therefore is not merely a psychological phenomenon, but is deeply rooted in family interactions, and social relationships. Furthermore, patients’ perceptions of dignity, as well as their accounts of dignity violations, differ markedly across cultural contexts. In some cultures, dignity is grounded in collective family and community roles, 16 while in others it centres on individual autonomy and self-determination. 17 Understanding these culturally shaped perceptions of dignity is therefore essential for interpreting how dignity is perceived and negotiated in end-of-life care. In this context, a systematic and comprehensive analysis of relevant literature and cross-cultural research is essential for a full understanding of the multi-dimensional nature of dignity in end-of-life care.
This integrative review investigates both patients’ understandings of dignity and families’ interpretations of dignity as these evolve over the end-of-life illness trajectory. Consistent with the above focus, this review examines dignity primarily as a lived and perceived experience reported by patients and their family caregivers. By clearly emphasising the experiences of dignity from the perspective of both patients and their families, this review aims to provide some insights that can be referred to in patient-centred and culturally sensitive palliative care practices. Based on this rationale, the present review has three objectives: (1) to define the concept of dignity from the perspective of patients undergoing palliative care; (2) to synthesise literature on patients’ lived experiences of dignity; and (3) to examine the influence of culture on the understanding of dignity in palliative care.
Methods
Design
This integrative review followed Whittemore and Knafl’s 18 five-stage framework, which provides a systematic approach for synthesising evidence from qualitative, quantitative, and mixed-methods studies. The five stages included: (1) identifying research questions that focussed on patients’ experience of dignity in palliative care; (2) conducting a comprehensive literature search across multiple databases; (3) evaluating the relevance and quality of the collected studies; (4) analysing and synthesising findings to identify patterns, themes, and their interrelationships; and (5) organising the results in a clear and coherent structure. The review was reported in accordance with the updated preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines to ensure transparency and replicability. 19 Qualitative and quantitative findings were integrated to provide a comprehensive understanding of dignity in palliative care.
Selection criteria
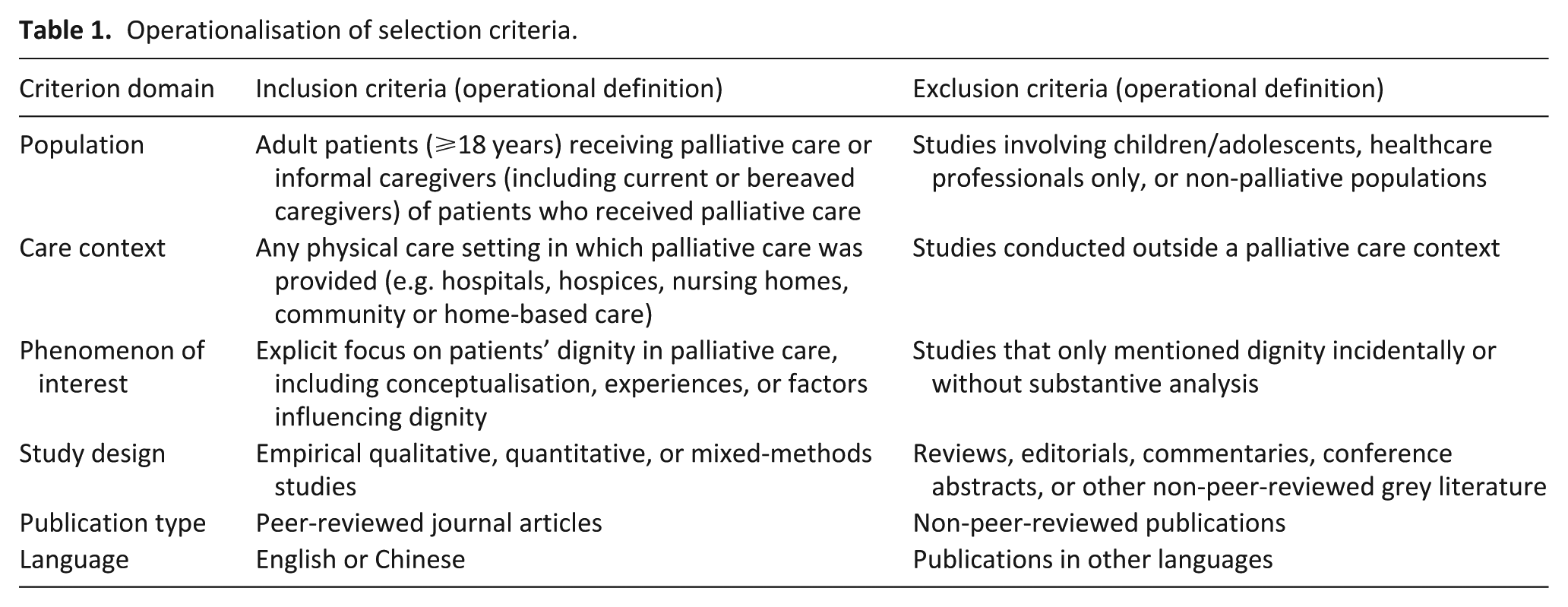
Studies were eligible if they involved adult patients receiving palliative care or family caregivers who currently or previously provided direct care to these patients, regardless of their healthcare settings, and reported experiences related to patients’ dignity in palliative care. Peer-reviewed empirical articles published in either English or Chinese were included. Searches were limited to English when databases did not support Chinese-language filtering. Reviews, editorials, conference abstracts, or non-peer-reviewed grey literature was excluded, as were studies which only briefly mentioned dignity. Further details regarding the inclusion criteria can be found in Table 1.
Operationalisation of selection criteria.
Search concepts
The search terms were organised around two core concepts: dignity and palliative care. For dignity, the truncated word digni* was used to cover related forms, such as dignity and dignified. For palliative care, the search content included palliative care itself as well as related terms, including hospice care, terminal care, terminally ill, life support care, end-of-life care, care of the dying, life-limiting illness, non-curative care, and end-stage care. Boolean operators were used to combine the two concepts.
Search strategies
Six databases (CINAHL, MEDLINE, ProQuest Sociological Abstracts, PsycINFO, Scopus, and Web of Science) were searched from inception to 28 February 2025. The search strategy was adjusted according to the indexing structure of each database. Where feasible, filters were applied to limit results to peer-reviewed empirical studies involving adults and published in English or Chinese. The complete search strings and search process are provided in Supplemental Material 1. The search yielded a total of 6627 records. To identify studies published after the database search cutoff date, targeted hand-searches of key journals were conducted between March and June 2025. No additional eligible studies were identified through the hand-search.
Article selection
After conducting database searches, all retrieved records were imported into EndNote to remove duplicates. After removing duplicates, the remaining records were exported to Microsoft Excel to support structured documentation and tracking of all screening decisions. Title and abstract screening was performed by the primary reviewer (WY) based on the predefined inclusion criteria. Records with uncertain relevance were discussed with the supervisory team (RF, and DR when necessary) to support the inclusion decision. Subsequently, the primary reviewer (WY) assessed the full-text articles using the designed data extraction table to systematically collect key information from studies that met the inclusion criteria. Any uncertainties regarding eligibility were resolved through team discussion (via meetings and email) until consensus was reached. In total, 32 studies were included.
Quality assessment
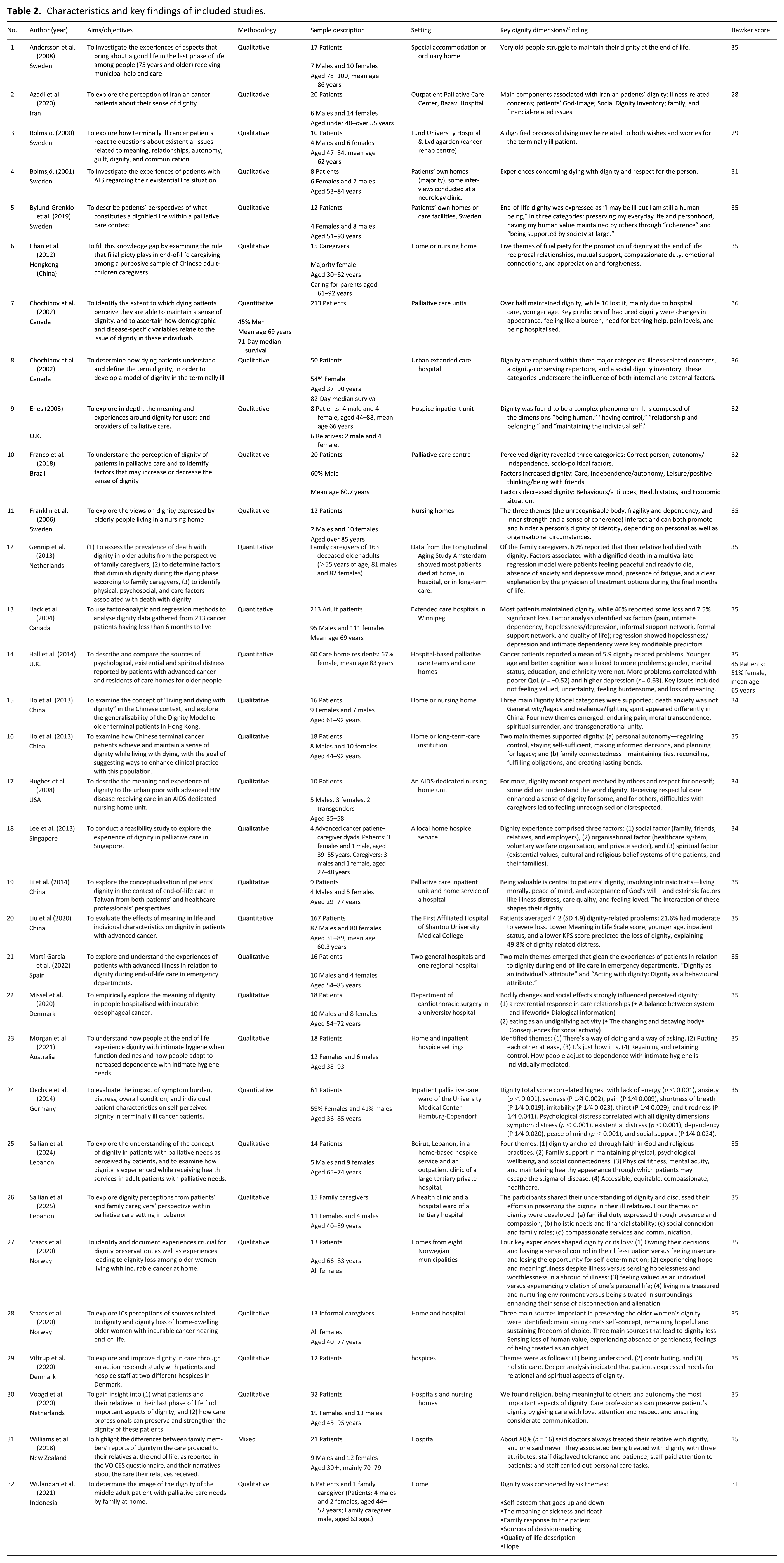
The quality of the included studies was assessed using the appraisal tool developed by Hawker et al. 20 This tool uses a four-point scale to evaluate nine aspects, including abstract and title, introduction and aims, method and data, sampling, data analysis, ethics and bias, findings, transferability, and implications and usefulness. The quality level ranges from very poor to good, with a total score ranging from 9 to 36. Higher scores suggest better methodological rigour. After the primary assessor (WY) completed the initial assessment, two additional reviewers (RF and DR) independently verified the results. The total Hawker scores of these 32 studies ranged from 28 to 36, with majority scoring exceeding 31 (Table 2). All studies were of acceptable quality, and no studies were excluded during this process. These scores were subsequently used to provide a basis for assessing confidence in the conclusions drawn from this review.
Characteristics and key findings of included studies.
Data extraction
The data extraction process was conducted using a structured Excel spreadsheet. A matrix of study characteristics was constructed to systematically collect descriptive and methodological information from each study, including author, title, aims, methodology, sample characteristics, setting, country, and dignity-related findings. In the subsequent stage, all results relevant to the review objectives were extracted. To maintain methodological rigour and facilitate later analysis, qualitative and quantitative results were first extracted separately. Data extraction was performed manually in Excel to ensure the accurate capture of complex and detailed data. Any uncertainties that arose during the extraction process were resolved through discussions with the supervisory team.
Data synthesis
The data synthesis was conducted based on the framework outlined by Whittemore and Knafl 18 and encompassed the following steps: (1) Data reduction: WY refined and focussed the extracted findings to retain data relevant to the review objectives; (2) Data display: WY, RF, and DR collaboratively developed a summary table (Table 2) to present the relevant data, with RF and DR verifying the final content for completeness and accuracy; (3) Theme identification: WY performed independent coding of the qualitative data. Qualitative findings were synthesised through an integrative thematic synthesis, involving iterative reading, coding, and clustering of findings across studies. 21 WY reanalysed and synthesised the findings of all studies to identify recurring patterns and develop a more comprehensive thematic framework concerning dignity in end-of-life care. Cultural context was considered as an additional analytical perspective to explore how culture influences patients’ experiences of dignity. Categories were employed to structure the Results section, thereby enhancing the clarity and coherence of the findings; (4) Data comparison and conclusion verification: WY incorporated quantitative data into the thematic framework to confirm and expand the identified themes, and re-checked all themes against the dataset to ensure credibility. RF, DR, and MG subsequently reviewed the integrated themes and discussed any uncertainties or potential inconsistencies. Any disagreements regarding coding, data integration, or theme development were resolved through discussion until consensus was reached. This process resulted in an integrated conclusion combining insights from both qualitative and quantitative evidence; (5) Documentation: Detailed notes and records of coding, integration, and theme refinement were maintained in Excel files to provide an audit trail.
Results
PRISMA-guided study selection
Following the PRISMA 2020 guidelines, the screening process was conducted in four stages: identification, screening, eligibility, and inclusion. In the identification stage, 6627 records were identified through the database search, of which 1510 duplicate records were excluded. During the screening stage, 5117 titles and 3458 abstracts were assessed, resulting in 220 articles considered to have potential relevance. After full-text review of these 220 articles, 32 studies met the inclusion criteria, comprising 25 qualitative studies,17,22–45 6 quantitative studies,11,46–50 and 1 mixed-methods study. 51 The numbers of articles at each stage of the selection process are shown in the PRISMA flow diagram (Figure 1).

PRISMA-based flow diagram illustrating the results of the study selection process.
Study characteristics
In this review, all research participants were patients with life-limiting illnesses, most commonly cancer.11,17,22–25,27–33,35–44,46–51 Some studies also included individuals with cardiovascular disease,11,31,44,45 neurological conditions,26,39,40 organ failure,39,40 or HIV. 34 Sample sizes varied widely, ranging from small-scale qualitative studies to large-scale quantitative studies involving over 200 patients and family caregivers. All studies focussed on adult patients, with several specifically targeted women,41,42 low-income populations,23,34 or ethnically and religiously diverse groups.39,44 Care settings included home care,11,22,24,27,28,33,35,38,39,41,42,45,48 hospices,30,38,43 inpatient and outpatient palliative care units,11,17,23,25,26,29,31,36,39,40,42,44,46–51 long-term care facilities,11,27,33 nursing homes,22,28,32,34,44 and emergency departments. 37 A substantial number of studies were conducted within groups in collectivist cultural contexts, including individuals from Iran, Lebanon, Indonesia, Singapore, China, Brazil, and Māori communities in New Zealand.22,23,28,31,33,35,36,39,40,45,49,51 Other studies focussed on individualist populations, such as individuals from Netherlands, Sweden, the United States, and European-descendant communities in New Zealand.11,26,27,34,51 In addition, one study specifically examined immigrant groups from collectivist cultural backgrounds living in individualist countries. 44 A summary of these studies is presented in Table 2.
Findings
The results fell into three broad categories: (1) the concept of dignity in palliative care, (2) patients’ experiences of dignity in palliative care, and (3) the role of culture in shaping dignity in palliative care.
Category 1: The concept of dignity in palliative care
Although patients’ understanding of dignity in palliative care varied across the studies reviewed, several recurring terms and expressions highlight how patients themselves perceived dignity. The most common and central definition emphasised “being treated like a human being.”25–27,29,30,34,37,42 Patients generally stressed that even at the end of life, they still wanted to be treated as individuals with complete personality and dignity, rather than just “patients” or less than human. For example, some participants expressed: “I wish to be regarded and treated like a person, not like a patient..” 25 “Give me respect; I give you respect. . .I’m not no animal. I’m a human being..” 34 These expressions highlighted that patients’ dignity involved more than their physical condition and was fundamentally grounded in recognition and respect as a human being. Another recurring definition was “live up to my values,” linking dignity to self-identity and personal worth.31,35,36 Other expressions included “have control,”30,31,42 “be independent,”29,42 “accept death,” 29 “maintain identity and social roles.” 40
Category 2: Patients’ experience of dignity in palliative care
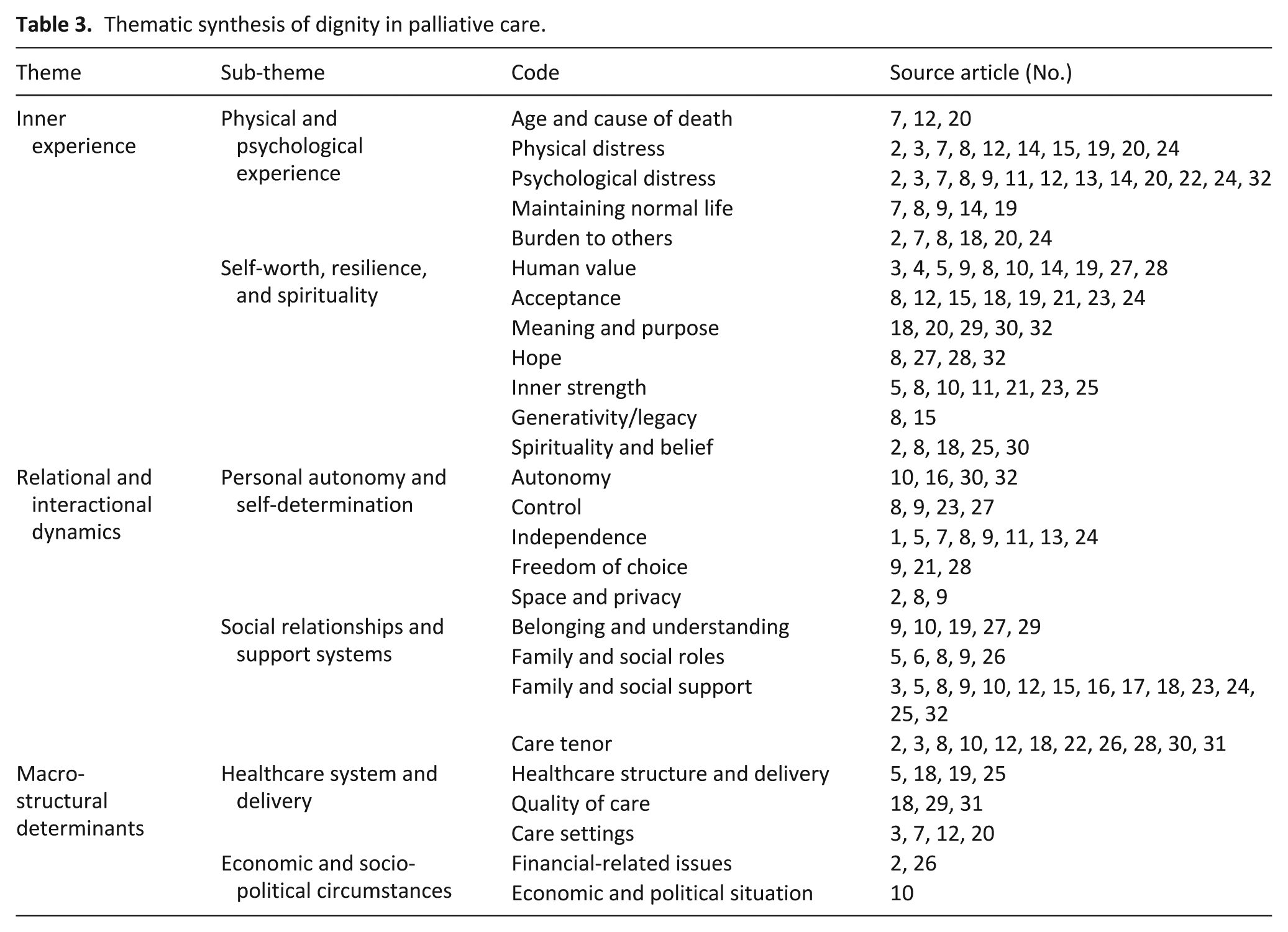
The synthesis of quantitative and qualitative research reveals the multifaceted nature of dignity among people with life limiting illness. Most patients reported that their dignity was intact or only slightly affected, while a smaller proportion expressed moderate concern, and only a few described loss of dignity as a severe or major problem.46,49 Family caregivers also held differing views on patients’ dignity at the end of life, with 69% believing their loved one died with dignity, while nearly one-third held the opposite view. 11 Experiences of medical care also played a crucial role. Most families reported that nurses (90%) and doctors (80%) showed respectful attitudes when treating patients. 51 Under Category 2, three themes were identified, incorporating both qualitative and quantitative insights. The underlying codes and source studies for each sub-theme and theme are also provided are shown in Table 3.
Thematic synthesis of dignity in palliative care.
Theme 1: Inner experience
This theme refers to the patients’ personalised and subjective experiences of dignity, including two sub-themes: physical and psychological experience, and self-worth, resilience, and spirituality.
Physical and psychological experience
The physical and psychological dimensions of patients’ experiences reflect how dignity can be eroded by the challenges imposed by illness. Advanced age and cause of death were associated with dignity.11,46,49 Various forms of physical distress, such as enduring pain and illness-related suffering, were documented across multiple studies.11,22,23,29,36,46,48–50 Psychological concerns were also prominent, including fear of experiencing a poor-quality death, body image disturbance, and illness-related emotional distress.11,17,23,29,30,32,45–50 In addition, both patients and caregivers when discussing patients’ dignity, described a desire to maintain a normal life while simultaneously feeling like a burden.23,29,30,35,36,46,48–50 Despite these challenges, patients actively sought to maintain their dignity through inner resources, leading to the second sub-theme: self-worth, resilience, and spirituality.
Self-worth, resilience, and spirituality
Patients, as well as caregivers when reflecting on patients’ dignity, emphasised the importance of sustaining human value and personal identity, as reflected in notions of being a valuable person, maintaining one’s self-concept, and ensuring continuity of self.26,27,29–31,36,41,42,48 Meaning-making, hope, and spirituality were central to resilience, with patients describing experiences of hope and meaningfulness despite their illness.11,22,29,35–38,41–45,49,50 They also drew on inner strength through positive thinking, optimism, humour, and a fighting spirit, with references to pride, moral transcendence, spiritual healing, and coherence.22,23,27,29,31,32,35,37–39,44 Together, these accounts demonstrate a dynamic internal process in which individuals negotiated dignity in the face of loss and decline.
Theme 2: Relational and interactional dynamics
This theme deals with the ways in which individuals interact with the external world, and how these interactions shape their experience and perceptions of dignity. It consists of two sub-themes: personal autonomy and self-determination, and social relationships and support systems.
Personal autonomy and self-determination
This sub-theme encompasses key concepts that reinforce patients’ sense of self-worth. Autonomy was expressed through personal decision-making and the capacity to retain agency in care.31,33,44,45 Regaining or retaining control over one’s life circumstances was regarded as essential for maintaining dignity and respect and control.29,30,38,41 Similarly, the ability to sustain independence, even in the context of declining physical capacity, was described as central to dignity.24,27,29,30,32,46,47,50 Freedom of choice, including the freedom “to be” and to make decisions in line with one’s values, was closely associated with dignity.30,37,42 In addition, maintaining space and privacy, such as protecting personal boundaries, was consistently emphasised as a condition necessary for preserving dignity.23,29,30
Social relationships and support systems
The second sub-theme underscores the role of interpersonal and systemic support in fostering dignity. To this end, both patients and caregivers valued experiences of belonging and understanding, including feeling understood, loved, and appreciated.30,31,36,41,43 The fulfillment of family and social roles, such as sustaining identity and values, preserving roles within the family, and adhering to cultural expectations such as filial piety, further supported a sense of dignity.27–30,40 Family and social support, including being connected with loved ones, maintaining intergenerational unity, and drawing strength from familiar places and spaces, provided important sources of comfort and continuity.11,22,27,29–31,33–35,38,39,45,50 Equally, caring attitudes expressed through love, respect, and attention were described as crucial in reinforcing dignity.11,17,23,29,31,35,40,42,44,51 Conversely, when patients experienced neglect, objectification, or restrictions on autonomy, their inner sense of dignity was profoundly undermined.
Theme 3: Macro-structural determinants
This theme reflects the wider systemic and socio-political factors that influence patients’ dignity during palliative care. This theme includes two sub-themes: healthcare system and delivery, and economic and socio-political circumstances.
Healthcare system and delivery
Within the healthcare system and its delivery, institutional infrastructure, timely and reliable healthcare provision, and the availability of accessible, equitable, and compassionate services were reported across multiple studies as factors that could help maintain dignity at the end of life.27,35,36,39 Holistic approaches to care, staff engagement in personal care tasks, and overall perceptions of care quality also supported patients’ dignity.35,43,51 Moreover, the care setting provided an important context, with some studies suggesting that care delivered in familiar environments, such as home or residential settings, may better support dignity, whereas hospital-based settings were sometimes associated with greater dignity-related distress.11,46,49
Economic and socio-political circumstances
This sub-theme also shaped dignity experiences, as participants reported financial challenges relating to holistic needs and overall stability, 40 expressed concerns about direct financial burdens, 23 and highlighted the impact of broader socio-political instability, including salary insecurity and crime. 31
Category 3: The role of culture in shaping dignity in palliative care
The comprehensive analysis employed cultural background as a lens to investigate the potential impact of cultural factors on patients’ understandings dignity, rather than to conduct direct cross-cultural comparisons. In studies that explicitly reported cultural background, collectivist, individualist, and migration-related characteristics were found to shape patients’ dignity in palliative care. It should be noted that cultural identity is not a fixed essence but is continuously shaped and transformed through overlapping cultural influences. 52 For analytical clarity, the findings were organised by population type, with 11 studies identified as representing collectivist populations,22,23,28,31,33,35,36,39,40,45,49 four as representing individualist populations,11,26,27,34 and one as representing immigrant populations. 44 One New Zealand study included both collectivist (Māori) and individualist (European-descendant) participants and was therefore represented across both these populations in the analysis. 51
Collectivist populations
In the included studies from collectivist societies, patients’ dignity in palliative care appeared to relate to family bonds, communal identity, religious beliefs, and the desire to preserve social harmony.22,23,28,31,33,35,36,39,40,45,49,51 Studies conducted in Iran and Lebanon, suggested that patients’ dignity was shaped by strong religious faith, respect for medical authority, and collective family involvement, with patients deriving meaning from both spiritual frameworks and the emotional support of loved ones.23,39,40 Similarly, research from China and Singapore highlighted how Confucian values emphasised filial responsibility, emotional restraint, and the importance of not burdening others. Enduring pain silently and avoiding direct discussions about death were described as dignified ways of maintaining harmony within the family.22,28,33,35,36 In a study from Brazil, patients’ dignity was influenced by Catholic traditions, the central role of the extended family, and social inequality. A dignified death often involved the presence of family members, emotional connexion, and religious rituals. 31 In research conducted with Māori communities in New Zealand, involvement of whānau (extended family groups) is fundamental to patients’ sense of dignity. 51 In these contexts, patients’ dignity was not primarily associated with autonomy or personal control, but rather with close interpersonal relationships, spiritual meaning, and sense of fulfilling social and familial roles.
Individualist populations
In the included studies from individualist societies, patients’ dignity in palliative care appeared to be linked to autonomy, personal agency, and the ability to maintain control over end-of-life decisions.11,26,27,34,51 In Swedish studies, findings suggested that patients valued independence, privacy, and self-expression, preferring to stay in familiar home environments where they could independently control their daily lives and medical decisions. Open and transparent communication was a cultural norm, and each person was regarded as an independent and autonomous individual throughout the dying process.26,27 In a study from the Netherlands, results indicated that patient-centred care practices that respected patients’ wishes and involving them in end-of-life arrangements may maintain patients’ dignity in palliative care. 11 In research on European-descendant communities in New Zealand, patients’ dignity focussed on the patient and core family, emphasising autonomy, informed consent, and quality of interactions with healthcare professionals. 51 One study from the United States further emphasised dignity as an individualised and self-referential construct, closely tied to personal self-worth and being recognised as a valued individual. 34 Across all of these contexts, findings suggest that patients’ dignity may be shaped by preserving individual identity, enabling self-determination, and supporting patients in finding meaning at the end of life on their own terms.
Immigrant populations
Findings from the included studies with immigrant populations – including Turkish, Moroccan, and Surinamese patients in the Netherlands – suggested that patients from collectivist cultures appear to experience dignity through interactions between their traditional values and Western healthcare expectations. 44 In these studies, experiences of dignity encompassed surrender to God’s or Allah’s will and being meaningful to others within social roles by maintaining connections with family, friends, or the community, rather than emphasising independence. Religious beliefs and practices, including rituals, prayer, or Quran recitation, appeared to support experiences of dignity and help people cope with dependency. Respectful and attentive care from healthcare professionals, protection of physical integrity and hygiene, opportunities for self-direction, and indirect communication about diagnoses and prognoses were also reported as contributing factors. 44
Discussion
This review aimed to identify and integrate the evidence on patients’ experiences of dignity in palliative care, with particular emphasis upon the influence of culture on these experiences. We identified that, across both qualitative and quantitative studies, patients’ perceptions of dignity are multifaceted. However, patients consistently defined dignity as “being treated like a human being.” Across studies, patients’ experiences of dignity were influenced by multiple factors. At the individual level, they were shaped by physical and psychological challenges as well as internal resources. At the relational level, their experiences were influenced by interactions with family members, healthcare providers, and peers. At the structural level, accessibility, fairness, and institutional support all impacted dignity experiences. Finally, at the cultural level, collectivist populations emphasised family relationships and social harmony, individualist groups prioritised autonomy and personal initiative, while immigrant groups described negotiating a balance between traditional values and the expectations of the healthcare system in their host country.
At an individual level, patients’ experiences of dignity are often threatened by persistent physical symptoms and psychological distress. Yet patients actively preserve their sense of dignity by demonstrating strong resilience and mobilising their internal resources. Existing research shows that meaning-making and spiritual practices help patients interpret their suffering within broader values and transcendence, such as through prayer, meditation, and humour, reducing feelings of worthlessness and supporting the continuity of self-identity.41,42,44 Positive psychological processes further contribute by reshaping maladaptive beliefs through cognitive restructuring, enhancing adaptive coping through emotional regulation, and strengthening perceived control through resilience training. These mechanisms not only help relieve suffering but also foster a positive self-image and reinforce one’s sense of competence, which are central to upholding patients’ dignity.53,54 Another form of narrative-based dignity intervention provides patients with structured opportunities to share their life experiences and helps them construct a sense of identity grounded in enduring meaning that persists beyond illness and even death, thereby further enhancing this mechanism. 53 Increasing evidence indicates that this approach can effectively alleviate psychological suffering in patients receiving palliative care and enhance their self-esteem.55,56 The review findings therefore add further evidence that healthcare professionals can support patients by fostering their inner resources and affirming their values and experiences to preserve their sense of dignity, even in the context of severe illness and suffering.
Within the realm of relational dynamics, we found that patients’ dignity is determined by the quality of interpersonal relationships and the nature of caring interactions. Research on families caring for patients with advanced dementia or motor neurone disease shows that advocating for patients’ non-medical personal wishes, engaging in compassionate communication, and preserving narratives of personal experience can help maintain their dignity as their condition deteriorates.57,58 Structured family interventions provides further evidence for this mechanism. For instance, family dignity interventions combined with standard palliative care have been shown to enhance family cohesion and alleviate anticipatory grief, thereby preserving the dignity experiences of patients and their families. 59 In healthcare settings, a review on dignity protection in Sweden found that nursing interventions proposed within dignity models, such as listening, communication, information provision, symptom control, assistance with activities of daily living, and involving patients in decision-making, are effective measures for protecting patients’ dignity. 60 Involving patients in the development of their medical care plans helps respect their autonomy and enhances their sense of self-worth. Similarly, involving them in decisions related to home-based elder care can increase their satisfaction and perceived control. 61 Collectively, these findings indicate that patients’ dignity is fostered through recognition, participation, and advocacy. Integrating these principles into clinical practice can help patients and their families maintain dignity during serious illnesses.
At the structural level, the review findings indicate that patients’ dignity is influenced by the broader healthcare environment, including access to services, fairness in resource allocation, and the organisation of palliative care. There is evidence that integrating principles of equity into healthcare design can enhance patients’ sense of dignity. For example, a study in the Northwest of England found that a model of end-of-life care in socially deprived areas reduced disparities in service access among different socioeconomic groups and ensured patients’ dignity across populations. 62 Conversely, long waiting times, chronic staff shortages, and fragmented care processes are systemic issues that can make patients feel neglected, helpless, and out of control, thereby intensifying their suffering.63,64 Physical and organisational care environments also mechanistically influences patients’ experiences of dignity. A London-based study revealed that patients dying at home tended to be more at peace during their last week, underscoring how the care setting can support emotional well-being and positive relational experiences. 65 Therefore, promoting patients’ dignity at the systemic level in clinical practice requires a strategy that combines system improvements with personalised care, including multidisciplinary collaboration, equity-oriented service design, and respect for the choice of place of death.
At the cultural level, patients’ dignity appears to be shaped by family structures, societal values, religious beliefs, and cross-cultural adaptation. In the studies included in this review from countries with populations often described as collectivist, such as China, Singapore, Lebanon, and Iran, patients sometimes appeared to entrust clinical decision-making to family members and maintain their dignity by enduring suffering or adhering to religious rituals. In these studies, patients generally endorsed collective values while not fully relinquishing their autonomy.22,23,28,33,35 We also identified that significant cultural differences also exist among different collectivist countries. For example, studies conducted in China and Singapore tended to highlight the importance of family support and social roles,22,28,33,35 while studies conducted in Iran and Lebanon more frequently emphasised religious faith as a source of strength.23,39,40 To preserve patients’ dignity in such settings, additional studies suggest that healthcare providers may consider engaging family members as key decision-makers in accordance with the cultural characteristics of each country, integrating spiritual care that respects religious rituals, and ensuring that patient care aligns with the communal values of the family.66,67
Studies conducted in countries commonly described as individualist contexts, such as the Netherlands, Sweden, and the United States, often reported that patients framed their dignity around autonomy and self-actualisation, with independence upheld through informed consent, ethical and legal safeguards, and advance care planning.11,26,27,34 For patients from these cultural contexts, research indicates that care strategies may prioritise clear and open communication, ensure that autonomy is respected through informed choices, and provide access to information and support that facilitate patient engagement in healthcare decisions.11,26,27,34 For immigrant populations in the study included in this review, individuals appeared to balance heritage and host-country norms, maintaining their dignity through a combination of family support, social networks, and personal faith. 44 Other evidence showed that immigrant women in Norway preserved their dignity experiences via family, healthcare staff, peers, and religious beliefs, 68 and Chinese-Canadian immigrants adapted values blending Chinese tradition with new cultural norms. 69 To support dignity in immigrant populations, insights from the wider literature suggests that interventions should emphasise the importance of cultural competence, encourage healthcare providers to be aware of specific cultural practices, and promote collaborative decision-making that respects both family dynamics and individual preferences.70,71 It is worth noting that these patterns reflect the findings reported in the studies included in this review, rather than fixed cultural differences, and the original studies were not designed to conduct direct cross-cultural comparisons. Therefore, these findings should be understood as context-specific insights rather than broad cultural generalisations. However, these insights provide an important starting point for future research.
Although not guided by an established dignity framework, this review’s findings align with Chochinov’s dignity model, strengthening its theoretical underpinnings. Specifically, the themes derived in this review have significant overlaps with the dignity concept model. The sub-theme of physical and psychological experience from the theme of inner experience aligns with illness-related concerns in the dignity model. The sub-theme of self-worth, resilience, and spirituality overlaps with dignity-conserving repertoires, and relational and interactional dynamics aligns with the social dignity inventory. This indicates that these domains coexist in different empirical contexts. Moreover, this review extends existing dignity framework by highlighting two key contributions not explicitly addressed in the original model. First, the theme of macro-structural determinants reflects the wider systemic and socio-political factors that shape patients’ dignity during palliative care, including healthcare system and delivery, as well as economic and socio-political circumstances. Second, cultural context was identified as an important influence on how patients understand and preserve dignity in palliative care. The additional insights from this review broaden the thematic scope beyond existing models and offer a more comprehensive view. Therefore, this study provides a more extensive and comprehensive foundation for understanding patients’ lived experiences of dignity in palliative care.
Strengths and limitations
There are several notable strengths in this integrative review. It integrates both qualitative and quantitative evidence, providing a more comprehensive understanding of patients’ dignity in palliative care from the perspectives of both patients and caregivers. By synthesising findings from studies across diverse cultural and clinical contexts, this review highlights the dynamic, multi-dimensional nature of patients’ dignity experiences. Evidence from immigrant communities further offers valuable insights into how cultural values, family roles, and social relationships shape the end-of-life experience.
Nevertheless, as in all research, some limitations should also be noted. This review focussed on studies most relevant to patients’ dignity in palliative care and excluded studies that only briefly mentioned or offered limited detail on the topic, which may have led to loss of nuanced experiences. Although findings were organised by collectivist, individualist, and immigrant contexts, most studies were not designed for cross-cultural comparison, and study numbers were uneven. Therefore, the patterns described should be interpreted cautiously and cannot be taken as definitive evidence of cultural differences. The included studies were primarily from high-income Western countries, particularly Canada and several European countries (such as Sweden, Netherlands, Denmark, Germany, Norway, and the United Kingdom), with some findings from Asia, the Middle East, and Oceania. However, the proportion of research from low- and middle-income countries (such as Africa, South Asia, and Latin America) is small, limiting the applicability of the findings in these regions. Differences in study design and reporting standards, as well as the lack of data on structurally disadvantaged populations, further limit our conclusions. These limitations highlight the need for future research on patients’ experiences of dignity in end-of-life care within underserved geographical and cultural contexts.
Conclusion
Across varied care settings, a core aspect of dignity in palliative care is being recognised and treated as a human being. Patients’ experiences of dignity are shaped by psychological states, social relationships, and systemic factors. Cultural context influences how patients perceive dignity: collectivist populations focus on family and community, individualist groups emphasise autonomy, and immigrants balance traditional values with the expectations of the host healthcare system. The findings indicate that person-centred and culturally responsive palliative care plays a crucial role in supporting patients’ dignity and promoting their well-being during the end-of-life period.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163261441427 – Supplemental material for Patients’ dignity in palliative care: An integrative review of lived experiences and family perspectives across cultures
Supplemental material, sj-docx-1-pmj-10.1177_02692163261441427 for Patients’ dignity in palliative care: An integrative review of lived experiences and family perspectives across cultures by Wenjing Yan, Rosemary Frey, Deborah Raphael and Merryn Gott in Palliative Medicine
Footnotes
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Author contributions
Wenjing Yan: Conceptualization, data collection, screening and processing, data analysis, and drafting the manuscript. Rosemary Frey: Conceptualization, methodology, data analysis, studies quality assessment and manuscript editing. Deborah Raphael: Conceptualization, methodology, data analysis, studies quality assessment and manuscript editing. Merryn Gott: Conceptualization, methodology, data analysis, manuscript editing, finalizing the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by China Scholarship Council under Grant 202408320104.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data included in this review were obtained from publicly available sources.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.