
Abstract
Co-victims – surviving relatives of murder and homicide victims – experience practical, emotional, psychological and legal problems as a result of the murder of their loved ones. Available findings are often based on cross-sectional studies. Longitudinal research is necessary to gain an understanding of the problems co-victims face. A total of 28 co-victims have been monitored for more than five years (63 months on average). The outcome shows that problems generally decrease over the course of time. Emotional and psychological problems may grow worse, however, during criminal proceedings and at the time of sentencing. Long-term care and support for this group is desirable.
Introduction
The number of murder and homicide cases in the Netherlands has been falling for years. In the mid-1990s, there was an average of 250 murders a year, by the turn of the century that number had dropped to 200 and for the past few years it has hovered around the 140 mark. 1 This downward trend has also been observed in other Western countries. A murder does not only affect the victim, it also impacts the wider family and network of relatives – the so called co-victims. We choose, in line with some other studies the term co-victims. Other studies refer to these individuals as survivors, victim–covictims or secondary victims. All these terms refer to anyone who has been impacted by the death of their loved one by homicide. The consequences of homicide may be serious and long-term for these people (Asaro and Clements, 2005; Thompson et al., 1998). The psychological issues co-victims have to contend with are more serious than the problems victims of other kinds of crimes experience (Lamet and Wittebrood, 2009; Rando, 1996; Rheingold et al., 2012; Zinzow et al., 2009). Co-victims who have to deal with the violent death of a child experience more severe psychological problems than the relatives of a child who loses his or her life in another way (Amick-McMullan et al., 1991; Murphy, 1996, 1999a, 1999b; Murphy et al., 2003). Various studies have shown that following the death of a loved one, nearly all co-victims display symptoms of posttraumatic stress disorder (PTSD) (Armour, 2002a; Asaro, 2001; Asaro and Clements, 2005; Freeman et al., 1996; Hertz et al., 2005; Kaltman and Bonanno, 2003; Murphy et al., 2003; Rynaerson, 1984; Zinzow et al., 2009, 2011).
The literature on this subject describes the problems affecting co-victims as a complex mourning process (Armour, 2002a; Armour and Umbreit, 2012; Asaro and Clements, 2005; De Keijser, 2004; Vessier-Batchen and Douglas, 2006; Rheingold and Williams, 2015). Besides the normal mourning process, co-victims having to cope with the loss of a loved one as a result of homicide also run the risk of developing PTSD. This may mean a more problematic mourning process than for those who have lost someone close due to a natural death (Parkes, 1993). Moreover, women experience more intensive grief symptoms than men (Sharpe et al., 2014). Co-victims also run a higher risk of long-term depression (Kaltman and Bonanno, 2003; Rheingold and Williams, 2015). A qualitative study by Scott Kenney found that co-victims metaphorically expressed a profound ‘loss of self’ which includes: a permanent loss of future; violating devastation; being a ‘different person now’; loss of control; and loss of innocence (Kenney, 2002: 219).
In the period following the death of a loved one, co-victims may experience repeated intrusive images, nightmares, overwhelming feelings of anger and rage, feelings of fear, excessive alertness and feelings of guilt (Armour, 2002a). An enormous anger against the world in general and the perpetrator in particular, is an additional emotion (Rock, 1998). Co-victims may also feel socially stigmatized because their loved one has died as a result of a crime. Family and friends may avoid the co-victims or speak ill of the way in which the victim died or lived his or her life. This may cause co-victims to be alienated from their social environment. Physical problems that may occur are sleeping and eating problems, headaches and abdominal and stomach aches (Armour, 2002a).
Organizing practical matters (e.g. a funeral) and media attention for the case may impede the mourning process (Malone, 2007). The formal way the police and legal authorities work may severely disturb the grieving process of the co-victims and emotional problems may worsen (Riches and Dawson, 1998; Rock, 1998). A lack of information in particular concerning the police investigation and the criminal proceedings, as well as the non-empathetic attitude of the police and legal authorities are major sources of frustration and grief for co-victims (Armour and Umbreit, 2012; Malone, 2007; Stretesky et al., 2010). According to Armour (2002a), co-victims feel especially traumatized during the first year as a result of their efforts to cope with the impact the crime has had on their daily lives, as well as the demands of the investigative and prosecution process.
The central question in this article is which long-term emotional/psychological, physical and social, practical and legal problems are experienced by co-victims as a result of homicide and how those problems evolve in the years following the crime.
Methodology
Legal system
The Dutch criminal proceedings system differs from the Anglo-Saxon countries where there is the tradition of common law in place. In the Netherlands and other continental European countries the criminal trial is characterized by its inquisitorial quality (Corstens, 2008). In common law countries the accusatory character of the criminal trial prevails. The main characteristic of an inquisitorial trial is its vertical structure. The Public Prosecutor does not appear for the victim but for the community. The judge’s role is an active and truth-finding one and he/she determines the progress of the trial. In contrast with an accusatory trial, the investigation in an inquisitorial trial is carried out by the police under the supervision of the Public Prosecutor. The judge decides on the guilt of the defendant, not a jury. In an inquisitorial trial the defendant is investigated whereas in an accusatory trial two equal parties (the defendant and the Public Prosecutor) are each other’s opponents before a passive judge. In the Dutch legal system the victim or his/her surviving relatives are not a formal party, but they can exercise all kinds of rights, for example, the right to speak. During the court proceedings they give a personal statement on what impact the crime has had on their lives. A Dutch victim support employee may provide support when drafting such a statement. Dutch victim support employees may also provide assistance as to reporting the crime, when witnesses give evidence and during court sessions. Neither victims nor co-victims are obliged to make use of Dutch victim support. This is strictly on a voluntary basis.
Sample
The study group involved co-victims who had lost a child, partner, parent, brother or sister. Recruiting the co-victims was arranged through the Dutch victim support organization, which supports victims and co-victims in practical, legal and emotional matters.
In 2009 and 2010 co-victims of homicide were approached by Dutch victim support case managers at the request of the independent researchers of the Dutch criminological institute Bureau Beke. The case managers asked the co-victims whether they would be prepared to participate in a scientific study. There was no random selection. The case managers were free to invite the co-victims they wanted to participate. If the case managers thought that a co-victim would be unable to handle things emotionally, they were not invited. It is unknown what the characteristics and backgrounds were of the co-victims who were not invited. A total of 62 co-victims involved in 42 homicide cases were approached. All agreed to participate and gave their informed consent. The case managers provided the researchers with the contact information of the co-victims. Most were approached by the researchers during a relatively short period after the homicide had taken place (at least three weeks, at the most three months) in 2009 and 2010. Following that, they were interviewed two or three times before the end of 2013.
Follow-up
In 2015, a number of co-victims – after informed consent – were requested to participate in a follow-up study in order to be able to identify any developments that had taken place. For the follow-up study, 36 co-victims from the first 28 cases were approached; eight co-victims (involved in three cases) refused on grounds of not being able to cope or being unable to participate for practical reasons (e.g. being abroad at the time of the follow-up). Some 28 co-victims involved in 25 cases were involved in the follow-up study and we were able to paint a picture of their development over a period of more than five years after the homicide took place. The average follow-up period was 63 months (five years and three months).
Instruments
The interviews with the co-victims were conducted with the use of a semi-structured questionnaire. For surviving relatives the murder of a loved one is a traumatic, multi-determined and ongoing experience (Armour, 2002a). Therefore it is necessary to cover as many aspects of the co-victims’ lives as possible. During the interviews, which were held according to a fixed set of questions, the following subjects were discussed:
The current status of the criminal trial Experiences with the case manager Emotional and psychological problems Physical and social problems Practical and financial issues Problems arising from the criminal proceedings
A co-victim’s personal situation was the key for more probing questions per subject. An illustration: the co-victims were asked whether they had incurred any physical complaints as a result of the crime. The co-victims might mention, for example, that they suffer from frequent headaches. The probing questions deal with the seriousness of the headaches and with any other physical complaints. The co-victims themselves were given the opportunity to mention any other complaints.
During the follow-up interviews the co-victims were asked if they were still suffering from headaches and/or any other complaints they had mentioned in previous interviews and whether these complaints had increased or decreased in comparison with the earlier measurement. An example of such a question is: ‘Some years ago you said that you were frequently suffering from headaches. Has anything changed in that respect?’ The co-victims themselves indicated to what extent those complaints were still existent.
Every interview (each lasting between one to three hours) was recorded in writing by the researchers. The records indicate to what degree the co-victims experienced problems during the period in question and to what extent their issues had declined or grown worse. Any new problems were also included.
It is important to stress that the co-victims’ own experiences of the complaints were the basis of the eventual view as to whether the problems had increased or decreased. This method of research touches on the phenomenological approach (Armour, 2002b). This entails that subjective, individual experiences determine the way the co-victim describes and experiences his state of mind. Besides the Brief Symptom Inventory (BSI) (see below), no other standardized instruments were used. Neither was the other side heard. Any complaints with regard to the criminal proceedings, concerning, for example, the police or Public Prosecutor, were not submitted to the authorities in question. This phenomenological approach entails that the interpretation of the experiences is a psychosocial construct in which the researchers play a part as well (Armour, 2002b). For our research this was an advantage rather than a disadvantage. It was not truth finding we were after. Our goal was to gain insight into the problems co-victims were faced with as a result of a crime by means of open communication.
The details of the 28 co-victims in the follow-up meeting were then compared to their answers from the first measurement so that developments over time could be mapped.
Psychological problems were measured by means of a standardized measuring instrument: the Dutch translation of the BSI (De Beurs, 2008; Derogatis, 1975a). The BSI is an abridged version of the Symptom Checklist-90–Revised (SCL-90-R; Derogatis, 1975b) and it can be used for a broad inventory of psychological complaints. The BSI consists of 53 items with which nine dimensions of psychopathology can be measured. These nine dimensions include somatization, obsessive–compulsive disorder, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation and psychoticism.
The BSI provides for each subscale indications for Reliable Change (RC), that is, statistically reliable changes. A distinction is made between illness (pathological) and health. The changes may relate to improvements or changes for the worse. Improvement entails that a co-victim has become ‘less ill’ or ‘healthier’. A change for the worse entails the opposite. Special forms of improvement or any changes for the worse are those forms in which the boundary between ill and healthy is crossed. Improvement entails recovery (from ill to healthy) and a change for the worse entails a relapse (from healthy to ill). The total score provides an indication of general psychological health. The BSI scores of 26 co-victims from the first measurement were available. These 26 co-victims also completed the BSI during the follow-up. When interpreting the scores a distinction was made between men and women. A representative sample survey across the Dutch population and a group of ambulant patients with psychiatric complaints made up the reference groups.
Sample information
The characteristics of the sample survey and the case details from the first measurement and the follow-up are included in the following tables. Table 1 demonstrates that most of the 26 co-victims completing the BSI were female. As to gender, there were no differences between the respondents of the final measurement and the non-respondents (p = 0.40).
Sample characteristics of the 26 co-victims who completed the BSI co-victims.

The first wave included 46 victims who were related to the co-victims (Table 2). A case might involve more than one victim, for example, a father who had killed both his partner and his child. The majority of the victims were adult males. There were no significant gender differences between the respondents and non-respondents in the last wave (p = 0.86).
Case information.
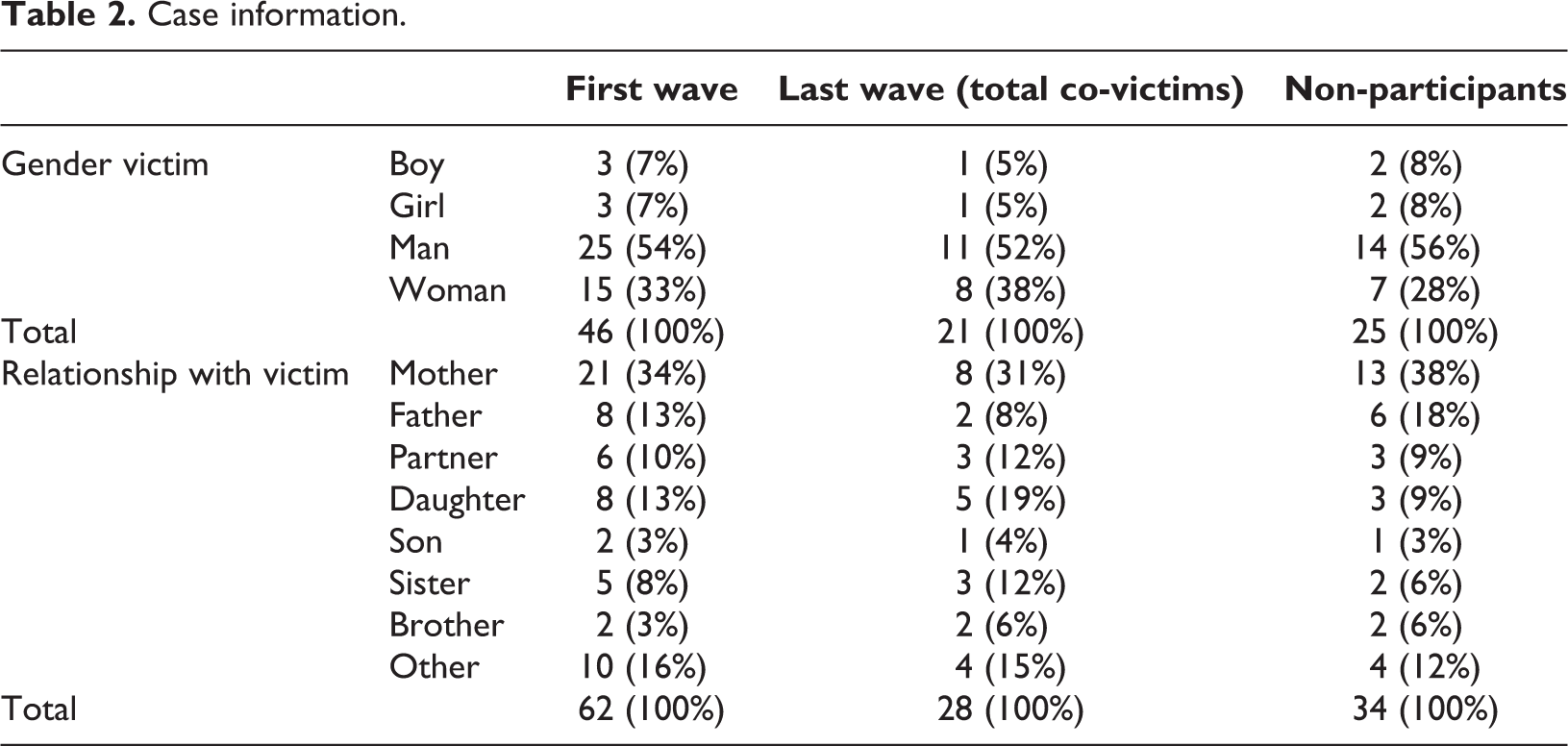
About 50% of the co-victims in the first wave were parents of the victim (47%), mostly mothers (34%). In the last wave, the division with respect to the relationship with the victim was comparable (p = 0.68).
Findings
Emotional and psychological problems
The results from the follow-up clearly demonstrate that the offense has indelible consequences for the co-victims, but that the emotional and psychological problems appear to recede over time. The interviews indicate that co-victims’ feelings of grief, the emotion most frequently mentioned, became less intense over the years, but that they could worsen at certain moments (holidays, birthdays and anniversaries of someone’s death). Respondent indicates that his brother’s death keeps haunting him: ‘It is always on your mind, especially during holidays and on birthdays’. (R20) The mother’s anger has grown in the course of time. There is anger because of the injustice done to them and because the perpetrator gets all the attention and they are not allowed or able to do anything. She thinks it is unfair. The loss has intensified. She misses her son very much. And at certain times she may get very angry with the perpetrator who has done this to them. (R2) The co-victims were very happy and relieved that years after the crime a suspect had been apprehended at last. It meant an end to the uncertainty about who had done it. Just before the arrest they had asked the police about the possibility of a DNA test. When the police called that morning to ask if they could pay a visit, the co-victims thought that they wanted to talk about that test. So they felt immense surprise and joy. At the same time the developments in the case caused feelings to resurface and they were faced with details about the case – how their mother was killed – they had not known before. They find that very hard and difficult to cope with. (R10/11)
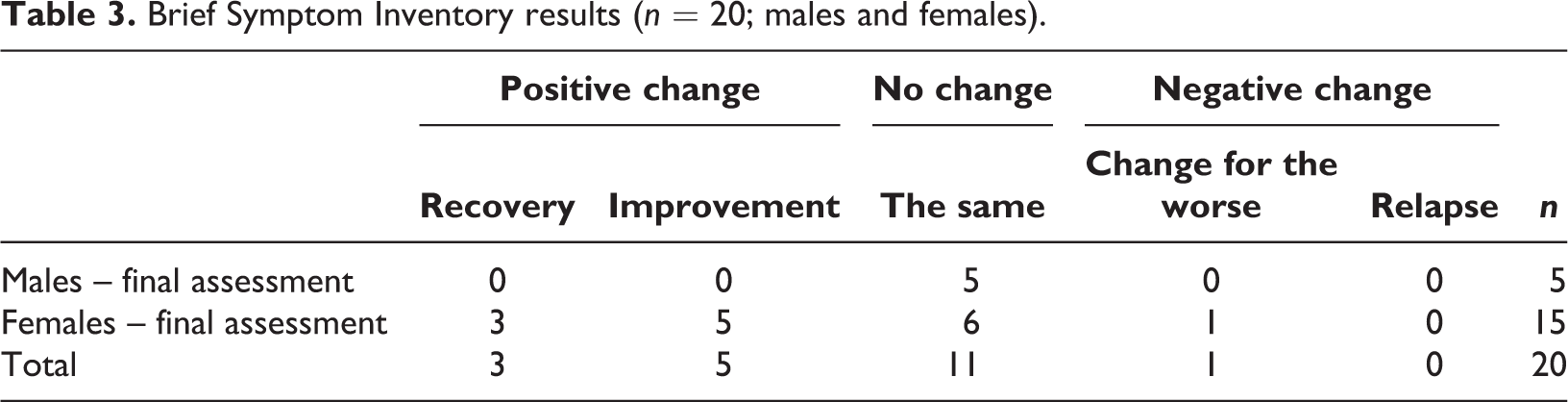
Tables 3 and 4 show the BSI scores from the final assessment compared to the benchmark and they indicate how many co-victims had made progress (positive changes) and how many had regressed (negative changes). It is also possible that there had not been any change in their situation. The BSI results are first of all presented as numbers of co-victims, subdivided into male and female; this analysis comprises 20 co-victims that had a score on all the criteria.
Brief Symptom Inventory results (n = 20; males and females).
Brief Symptom Inventory results (n = 26; males and females).
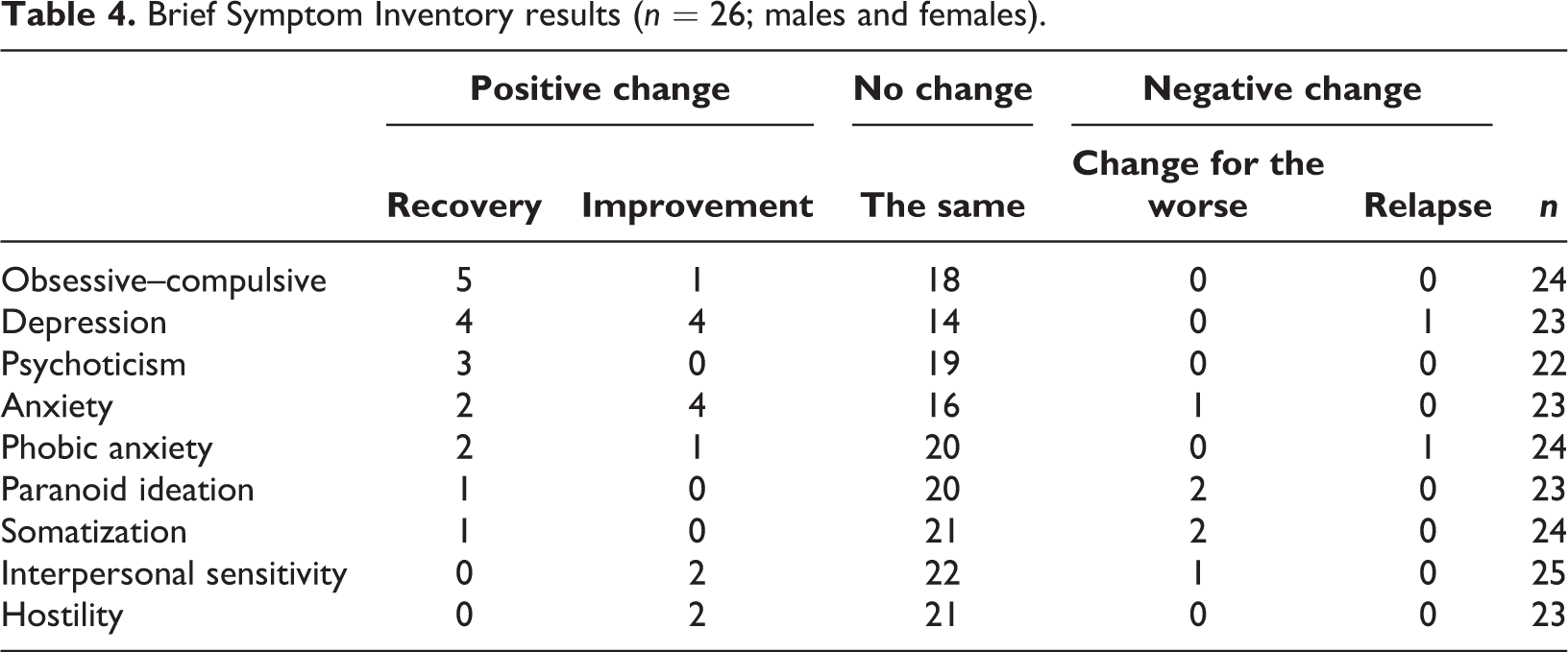
Table 3 clearly shows that about half of the co-victims (who scored on all criteria) display no changes compared with the first wave. This applies to all five men and six women. When compared with the scores of standard groups it is clear that the problems of three of the 11 respondents were very similar to those of the standard group of psychiatric patients. Eight out of 20, on the other hand, made progress, while one regressed. Not a single co-victim relapsed. Table 4 represents the way in which the problems of the co-victims developed with respect to the separate problem areas. 2
As mentioned earlier, the majority of the co-victims did not display any changes in their psychological condition compared to the initial measurement. In other words, their condition remained unchanged when compared to the benchmark. This does not necessarily have to indicate ‘ill’, but can also indicate ‘healthy’. The negative changes include, among other things, somatic complaints and paranoid thoughts. The positive changes mainly refer to feelings of depression, cognitive complaints and anxiety. In the period shortly after the crime she is very depressed; she did not want to live any more. Now she is doing okay. She has learned how to cope with it. She has not worked it through and she says that will never happen. The dog was a great help in keeping her mind off things (walking it and taking care of it). The dog makes her happy. Time is the great healer. The sharp edges gradually disappear. Instead of visiting the grave every day she only goes once a week or every fortnight. (R2)
Physical problems
All 28 co-victims experienced physical complaints after the crime. The most frequently mentioned were headaches, stomach and bowel complaints, sleeping problems and tiredness, cardiac complaints and loss of appetite. The crime exacerbated existing physical complaints. Over the course of time these physical problems gradually diminished and partly disappeared for most co-victims. For some, the physical problems remained or resurfaced at certain, emotional moments such as during the criminal justice process. Many co-victims claimed that they experienced stress all the time because of the crime and that these feelings of stress caused many kinds of physical ailments. I have a lot of complaints. My neck and muscles hurt. I have headaches, I have stomach problems, and I gain weight…all due to stress. My entire body literally aches. (R31)
Social
In the interviews nearly all co-victims indicated that they displayed behaviour in which they avoided other people shortly after the crime, with the exception of close friends and relatives. Some literally locked themselves into their rooms and did not go outside. Others did go out, but avoided places where they might run into people they knew. The co-victims do not feel up to answering other people’s questions about the crime. They could not handle things emotionally. Other people’s well-intentioned questions (e.g. ‘How are you doing?’) met a lot of resistance. These social problems disappeared for most co-victims as the years went by. When questioned they were able to talk about the crime more easily and reminisce about the victim with others. I have built a circle of friends. I can talk to them but I find it hard at the same time. I can also talk well with my neighbour. I felt the need to move on; I could not go on the way I did. I have done it myself…I also walk my neighbour’s dog. (R31)
Practical problems
The co-victims’ answers to the question revealed to what extent they experienced practical problems as a result of the crime. These can be divided into the following categories: financial; administrative; and media.
Almost all co-victims experienced financial consequences due to the crime. They lost their murdered partner’s income, could not pay for their mortgage and were confronted with additional costs due to the funeral and court proceedings. With a few exceptions, these financial problems had been resolved by the time of the final assessment. Co-victims were able to apply for an allowance from the Violent Crimes Compensation Fund, which enabled them to pay off at least a part of the costs. A number of insurance companies paid out benefits. I have not had any real problems, though my loss of income was substantial because my husband’s salary disappeared and I myself lost my job on medical grounds. I had run up debts here and there but of late I have been able to sort things out a bit. I think I should be able to get by on my social security allowance. (R22) ‘The crime is the reason that I have grown to dislike civil servants and bureaucracy immensely. When I have to renew my driving licence or something like that, I ask a friend along because otherwise I will rant at the civil servant in question, who only comes across as stupid and uninterested. It infuriates me again.’ She mentions all kinds of examples in which she has become the ‘victim’ of some civil servant. ‘I feel very frustrated due to all this bureaucracy…and I did not feel that aversion prior to the crime’. (R4)
Legal problems
The legal aspects of the crime run like a thread through all the 28 co-victims’ problems. None of them had had any previous experience with the police, investigative procedures and trials. The legal procedure begins with the identification of their loved one, the police investigation, the criminal proceedings against the suspect and the court verdict. The problems they experienced were varied. They thought that communication from the authorities, especially from the Public Prosecutor’s Office, left a great deal to be desired in certain cases. They were not informed, or were informed too late, when court sessions were postponed, someone was released on probation or when the perpetrator was released. Some also found the way in which they were treated by the police and Public Prosecutor’s Office particularly hard to take. Many co-victims felt that all the attention focused on the perpetrator and that they were not taken seriously. They experienced the trial itself as very emotional. They were completely focused on the trial when they would be confronted with the perpetrator. In general, the sentence the perpetrator received was much lower than they had hoped for. I don’t understand the court verdict at all. The prosecutor’s demand of 15 years for both perpetrators was even reduced by a few years. One of the perpetrators has been released already. The police and the case manager had high hopes of the court imposing a heavier punishment, since the judge was known to be rather strict and he had also reprimanded the perpetrators because of their impertinent behaviour during the trial. The verdict was quite a disappointment for everyone, the more so because no mandatory treatment was imposed. I have contacted the court myself about how on earth that was possible, but they never reacted. They don’t get it at all. I don’t understand the system. (R7) At the time of the trial you must be on your guard all the time. I have experienced a lot of grief and frustration due to the fact that the perpetrator’s lawyer tried to paint a negative picture of the victim in favour of the perpetrator. That is so hurtful. At a police training session I advised them to thoroughly prepare co-victims for how things might play out in a trial. ‘Warn the family about what to expect from the prosecuting lawyer during a trial. It’s an emotional roller-coaster because of insinuations made about the life of the victim and that hurts terribly’. After the final verdict I started to feel a little calmer because at least the perpetrator would spend the next 10 years in prison. Knowing that the perpetrator is in prison now and after that will be extradited is of great importance. If he is not extradited after his detention after all, I can’t guarantee that I won’t take action. I will take steps myself to find out exactly what is going on. (R27)
There had been no arrests in three of the cases. These co-victims were in a state of continual uncertainty about whether ‘their’ case would ever be solved. For them, there was no closure yet.
Conclusion
The murder of a loved one completely changed the lives of the 28 co-victims. They were scarred for life (Armour, 2002a; Kenney, 2002). In their words they had been given a life sentence with all the problems that go with it. The main conclusion is that the co-victims really struggled to cope in the immediate aftermath of the crime, but that their problems generally improved after that. The sharp edges wore off, the grief receded, but the feelings of loss grew. An important finding is that problems may resurface again at the time of the trial, probation and eventually, the release of the perpetrator. Cross-sectional research does not show up the reoccurrence of problems. The longitudinal character of this study shows how important it is not to limit care for the victims and co-victims to the immediate aftermath of the crime, but to provide follow-up care for an extended period and to tailor help and support. This study clearly shows the co-victims’ desire for some form of aftercare, even years after the crime. This is all the more urgent now that court cases in the Netherlands are taking longer. The issues at stake also depend both on the duration and the course of the trial, the mode of sentence, and finally the release of the perpetrator.
The extent to which co-victims were able to mourn was partly determined by the authorities’ attitude concerning their case. Respondents in this study did not always feel their role as co-victim was acknowledged by the authorities; seeing all the attention and resources as focused on the perpetrators. The legal, bureaucratic approach to their case was sometimes at the expense of a ‘humane’ attitude and treatment (Van Wijk et al., 2015). More expertise is needed from the side of legal, law enforcement and health providers (Metzger et al., 2015). Promoting expertise should especially focus on the grieving process and traumatic experiences.
The professional case managers of the Dutch victim support organization played an important role in alleviating these problems, at least according to the co-victims (Van Wijk et al., 2013). Without them they would not have coped. Because of their complex and unique problems, the co-victims believed there should be specialized support (Malone, 2007; Paterson et al., 2006; Ten Boom et al., 2008). The establishment of the position of case manager by the Dutch victim support organization, and their way of working, correspond with recent findings which show that long-term complaints such as PTSD and depression are connected to a lack of specialized support (Rheingold and Williams, 2015). In other words, case managers can prevent problems escalating by advising and assisting the co-victims.
A limitation of this study is that both sides of the argument have not been heard. The starting point has been the co-victims’ experiences and feelings – which by definition are subjective – without taking into account the actual procedures of the authorities that have been criticized. A second limitation is the relatively small size of the survey group. At the same time, this study is unique because it has mapped out the long-term problems of the co-victims. A follow-up study of the co-victims should be longitudinal using a wider variety of standardized measuring instruments. The BSI provides an indication of psychological wellbeing, but is too limited to provide a complete picture of the co-victims’ psychological problems.