
Abstract
Background:
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have emerged as a potential treatment for antipsychotic-induced weight gain. This meta-analysis aimed to investigate the efficacy of GLP-1RAs on weight, body mass index (BMI), waist circumference, and visceral fat in patients receiving antipsychotics.
Methods:
We searched PubMed, Embase, the Cochrane Central, and APA PsycINFO through April 21, 2026, for randomized controlled trials (RCTs) of GLP-1RAs in patients treated with antipsychotics. Outcomes included weight, BMI, waist circumference, and visceral fat. Between-group mean differences (MDs) and their standard errors were used for meta-analyses. The risk of bias was assessed using the Cochrane Risk of Bias 2.0 tool. This study is registered with PROSPERO (CRD420251118829).
Results:
Nine RCTs including 595 participants were identified, of whom 294 received GLP-1RAs and 301 received placebo. Four studies reported visceral fat outcomes. GLP-1RAs significantly reduced body weight (MD −6.82 kg (95% confidence interval; CI −9.66 to −3.97), p < 0.0001), BMI (−2.23 kg/m2 (95% CI −3.15 to −1.30), p < 0.0001), waist circumference (−4.94 cm (95% CI −6.92 to −2.96), p < 0.0001), and visceral fat (−0.37 kg (95% CI −0.69 to −0.05), p = 0.0255) compared with placebo. The certainty of evidence was rated as moderate across all outcomes.
Conclusion:
This meta-analysis demonstrates the benefit of GLP-1RAs in reducing body weight, BMI, waist circumference, and visceral fat. These findings support the clinical utility of GLP-1RAs as adjunctive treatments in patients with psychiatric disease and underscore the need for further trials with adiposity endpoints.
Keywords
Introduction
Mental disorders represent a major global public health burden. Epidemiological evidence indicates that approximately 60% of individuals with severe mental illness, such as schizophrenia spectrum disorders, major depressive disorder (MDD), and bipolar disorder, are overweight or obese, a prevalence nearly threefold higher than in the general population (Afzal et al., 2021). Specifically, patients with schizophrenia show markedly elevated rates of metabolic syndrome and central obesity, with 53% meeting the criteria for metabolic syndrome and 73% presenting with central obesity (Trott et al., 2025). Psychiatric disorders themselves predispose individuals to excessive weight gain, while excess adiposity in turn impairs symptom control and worsens clinical prognosis (De Hert et al., 2009; Leutner et al., 2023). Compared with patients with MDD or bipolar disorder, individuals with schizophrenia are approximately 2.8–4.4 times more likely to develop obesity (Correll et al., 2015). A recent review further highlighted that clozapine and olanzapine, which exhibit prominent 5-HT2C, H1, and M3 receptor antagonism, confer a greater risk of weight gain than antidepressants (Dayabandara et al., 2017; Solmi et al., 2024). This adverse metabolic effect has substantial clinical implications, as it reduces medication adherence and frequently necessitates discontinuation or switching of therapy, thereby complicating long-term management (Doane et al., 2022; Weiden et al., 2004).
To manage antipsychotic-induced weight gain (AIWG), clinical guidelines recommend a stepwise approach. Lifestyle modification is typically the first-line strategy, followed by dose adjustment or switching to agents with lower metabolic liability. The American Psychiatric Association (APA) guideline recommends considering antipsychotics with reduced weight gain potential (Keepers et al., 2020). The International Guidelines for Algorithmic Treatment (INTEGRATE) for the pharmacological management of schizophrenia also emphasize cardiometabolic monitoring and lifestyle advice (McCutcheon et al., 2025). The guideline recommends treatment adjustment when clinically significant weight gain, defined as an increase of more than 5% within 3 months, is observed. It advises switching to an alternative antipsychotic or initiating adjunctive therapy such as metformin or glucagon-like peptide-1 receptor agonists (GLP-1RAs).
Among adjunctive pharmacologic agents, metformin has been the most extensively studied. Randomized controlled trials (RCTs) have demonstrated significant reductions in body weight from baseline with minimal adverse events (Modabbernia et al., 2014; Wang et al., 2012). Moreover, metformin is inexpensive and easy to administer, further supporting its clinical utility. Consistent with these findings, recent guidelines including the INTEGRATE recommend adjunctive metformin as a potential treatment strategy for managing AIWG (Carolan et al., 2025; McCutcheon et al., 2025). Orlistat has also shown reductions in body mass index (BMI) among overweight or obese patients receiving antipsychotics, particularly in men (Joffe et al., 2008; Xie et al., 2024). Other agents, including betahistine, topiramate, and reboxetine, have shown inconsistent effects (Barak et al., 2016; Narula et al., 2010; Poyurovsky et al., 2003), and their clinical use is limited by neurocognitive adverse events.
GLP-1RAs, originally developed for the treatment of type 2 diabetes, exert metabolic benefits by enhancing insulin secretion and promoting satiety (Friedrichsen et al., 2021; van Can et al., 2014). Given that AIWG is mechanistically linked to insulin resistance and dysregulated appetite control, GLP-1RAs represent a biologically plausible strategy to counteract these metabolic effects (Albaugh et al., 2011; Ebdrup et al., 2012; Teff et al., 2013). Recent RCTs of liraglutide, exenatide, and semaglutide have demonstrated weight loss among patients treated with antipsychotics (Larsen et al., 2017; Siskind et al., 2020, 2025), and previous meta-analyses have supported these findings (Siskind et al., 2019). However, most prior reviews have focused primarily on weight change, without systematically evaluating other anthropometric or adiposity indices such as BMI, waist circumference, and visceral fat that more directly reflect cardiometabolic risk (Bak et al., 2024; Goetz-Kundera et al., 2025). Moreover, several recent RCTs have not yet been incorporated into previous meta-analyses, warranting an updated synthesis (Siskind et al., 2019).
Therefore, the purpose of this study was to systematically evaluate the efficacy of GLP-1RAs not only on body weight but also on BMI, waist circumference, and visceral adiposity in patients receiving antipsychotic treatment. By integrating evidence from the most recent RCTs, this meta-analysis aims to clarify the clinical utility of GLP-1RAs in mitigating antipsychotic-associated metabolic complications.
Methods
Study design and registration
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO, registration number: CRD420251118829) (Page et al., 2021).
Search strategy
We systematically searched PubMed, Embase, the Cochrane Central and APA PsycINFO from inception up to April 21, 2026. Both MeSH terms and free-text keywords were used to enhance search sensitivity and specificity. The main search keywords included “antipsychotic agents” AND “glucagon-like peptide-1 receptor agonist OR GLP-1RA,” along with related search terms and MeSH terms. The detailed search strategy is provided in the Supplemental Table S2. The reference lists of the included studies were reviewed to identify any additional eligible studies. No language restrictions were applied.
Eligible studies met the following criteria: (1) participants were patients with serious mental illness receiving typical and/or atypical antipsychotic agents; (2) GLP-1RAs as interventions; (3) placebo-controlled; (4) outcomes included anthropometric measurements such as body weight, BMI, waist circumference, or visceral fat; and (5) RCTs. Studies that focused exclusively on non-anthropometric outcomes (e.g., cognition, gene expression) were excluded.
Dual selection and data extraction
Two independent reviewers screened titles and abstracts of articles based on prespecified eligibility criteria, with the same two reviewers assessing full-text articles. In cases where conflicts remained despite discussion, a senior researcher was consulted to reach a consensus. Inter-rater agreement during the dual selection process was assessed using Cohen’s κ statistic. For meta-analysis, study characteristics were extracted, including the number of patients, baseline and post-intervention measurements and effect size of treatment.
Risk of bias assessment
The Cochrane Risk of Bias 2 tool was used to assess study quality across five domains: (1) randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported result (Sterne et al., 2019). A study was rated as “low risk” if all domains were judged to be at low risk of bias. If there were any “some concerns” but no “high risk” domains existed, the overall evaluation was “some concerns.” Any study with a “high risk” rating in any domain was deemed “high risk.”
Statistical analysis
All analyses were conducted using a random effects model, which was prespecified to account for anticipated heterogeneity across studies. Heterogeneity was quantified using the I2 statistic. The primary outcomes of interest were body weight, BMI, waist circumference, and visceral fat. Continuous variables were summarized using the between-group mean difference (MD) and its standard error (SE) as the primary effect measure. If a study directly reported the MD and SE, those values were used. If only baseline and post-intervention group means were available, MD and SE were calculated from change scores. Where treatment effect and either 95% confidence intervals (CI) or p-values were reported, the corresponding SEs were derived accordingly. When the standard deviation of within-group differences was not reported, it was imputed using an assumed correlation coefficient (r) of 0.5 between pre- and post-treatment measurements. The correlation coefficient value of 0.5 approximates the empirical median within-group correlation observed in active treatment arms across clinical trials of continuous outcomes (Balk et al., 2012). To evaluate the robustness of the findings, sensitivity analyses were performed by varying the assumed correlation coefficient to 0.7 and 0.9. In addition, a leave-one-out analysis was conducted to assess the influence of individual studies on the pooled effect size.
Forest plots were generated to visually represent the pooled effects for each outcome. Potential publication bias was explored visually using funnel plots. All analyses were performed in R version 4.5.1 (R Core Team, 2025) with the meta package (version 8.2.0; Balduzzi et al., 2019) .
Subgroup analysis
Predefined subgroup analyses were performed according to drug ingredient, treatment duration, and risk-of-bias category to further explore potential sources of heterogeneity. For the drug ingredient subgroup, studies were classified into exenatide, liraglutide, and semaglutide groups. For treatment duration, studies were grouped based on a 24-week cutoff. This threshold was chosen to distinguish shorter trials from those with more prolonged GLP-1RA exposure and approximately corresponded to the distribution of follow-up durations across the included studies. Given the limited number of studies, this categorization was intended as an exploratory assessment of whether the pooled effects differed between shorter and longer treatment exposure. For the risk-of-bias category, studies were classified into “low risk” and “some concerns or high risk” groups.
Certainty of evidence
Certainty of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach in GRADEpro software. Starting from a high-certainty rating, each outcome was evaluated across five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
Included studies and patient characteristics
The systematic search yielded a total of 377 records. After automatic removal of 85 duplicates, 292 records remained. Following title and abstract screening, 18 studies were retrieved for full-text review. Inter-rater agreement between reviewers was substantial (Cohen’s κ = 0.71, 95% CI 0.53–0.89). Ultimately, nine RCTs met the predefined eligibility criteria and were included in the meta-analysis, as illustrated in the PRISMA flow diagram (Supplemental Figure S1).
The key characteristics of included studies are presented in Table 1. Nine RCTs included a total of 595 participants, with 294 allocated to the GLP-1RA arm and 301 to the placebo group. Treatment durations ranged from 9 to 40 weeks. Interventions included exenatide in three trials, liraglutide in three trials, and semaglutide in three trials. Participants across the nine included trials primarily had schizophrenia or schizoaffective disorder, although some studies also enrolled individuals with psychosis, bipolar disorder, or MDD. Glycemic inclusion criteria differed across trials, with four trials including participants with or without type 2 diabetes. The antipsychotic agents used varied across studies, with clozapine and olanzapine being the most common. The mean age of participants ranged from 34 to 45 years, and the mean body weight ranged from 88 to 122 kg. Baseline BMI, waist circumference, and visceral fat are summarized in Tables 1.
Characteristics of included studies.
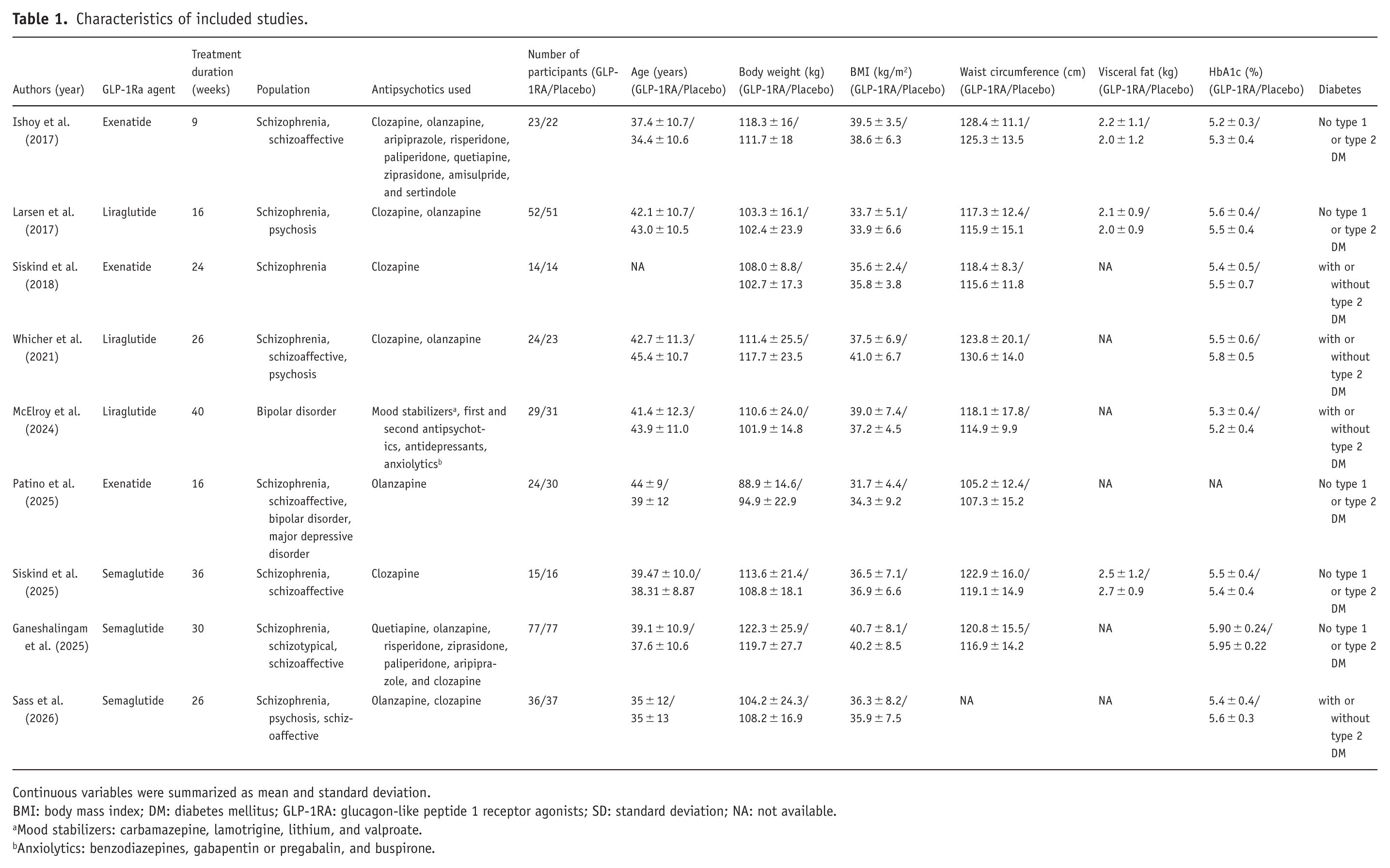
Continuous variables were summarized as mean and standard deviation.
BMI: body mass index; DM: diabetes mellitus; GLP-1RA: glucagon-like peptide 1 receptor agonists; SD: standard deviation; NA: not available.
Mood stabilizers: carbamazepine, lamotrigine, lithium, and valproate.
Anxiolytics: benzodiazepines, gabapentin or pregabalin, and buspirone.
Summary of findings and certainty of evidence for main outcomes using the GRADE approach.
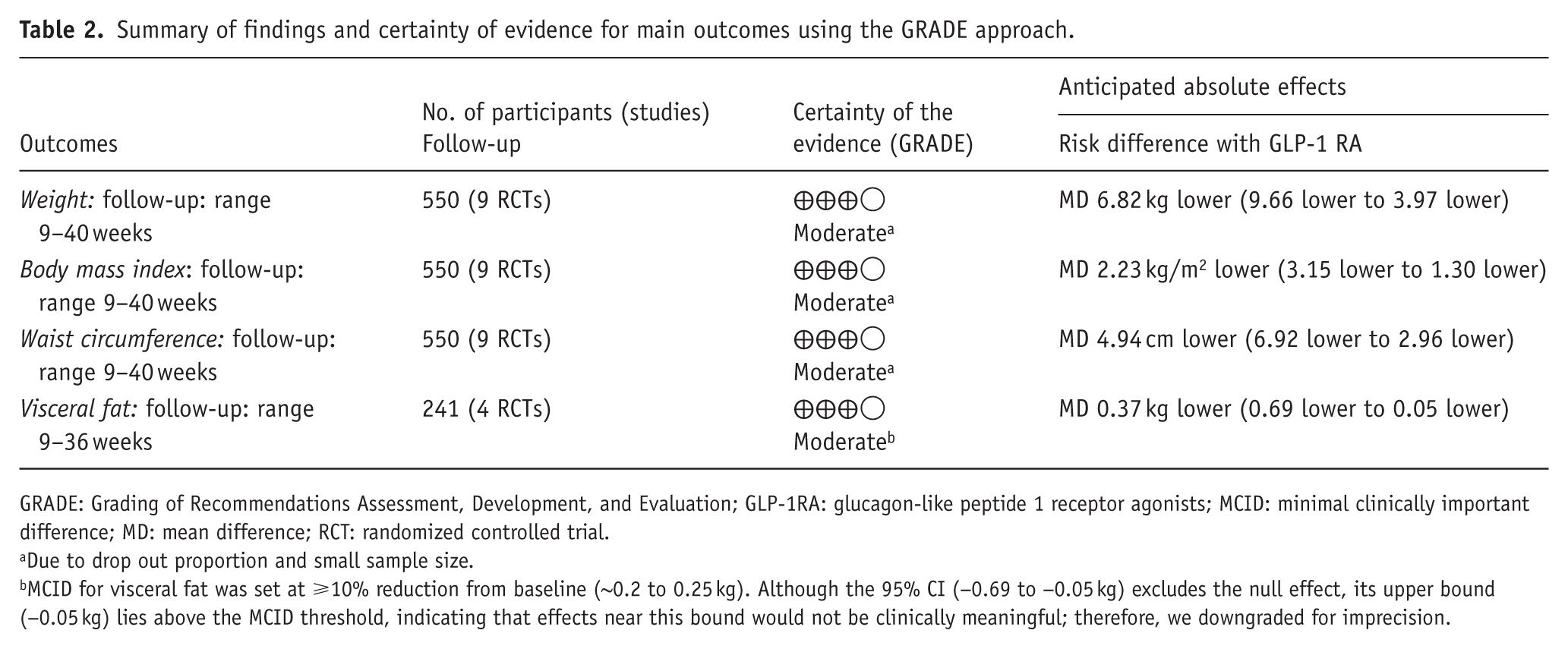
GRADE: Grading of Recommendations Assessment, Development, and Evaluation; GLP-1RA: glucagon-like peptide 1 receptor agonists; MCID: minimal clinically important difference; MD: mean difference; RCT: randomized controlled trial.
Due to drop out proportion and small sample size.
MCID for visceral fat was set at ⩾10% reduction from baseline (~0.2 to 0.25 kg). Although the 95% CI (−0.69 to −0.05 kg) excludes the null effect, its upper bound (−0.05 kg) lies above the MCID threshold, indicating that effects near this bound would not be clinically meaningful; therefore, we downgraded for imprecision.
Risk of bias assessment of included studies
Of the nine included studies, six were judged to be at low risk of bias across all domains. Due to missing outcome data, one study was rated as having some concerns, and the other two studies were judged to be at high risk of bias.
Main results of the meta-analysis
Assuming r = 0.5, the meta-analysis of body weight showed a significant reduction in the intervention group compared with placebo (MD = −6.82 kg (95% CI −9.66 to −3.97), p < 0.0001; Figure 1(a)). BMI also decreased significantly with treatment (MD = −2.23 kg/m2 (95% CI −3.15 to −1.30), p < 0.0001). Waist circumference showed a significant reduction compared with placebo (MD = −4.94 cm (95% CI −6.92 to −2.96), p < 0.0001). Four studies reported visceral fat. Visceral fat mass was measured by dual-energy X-ray absorptiometry in all four studies. The pooled estimate showed a statistically significant reduction with GLP-1RA treatment (MD = −0.37 kg (95% CI −0.69 to −0.05), p = 0.0255).

Forest plots of outcomes: (a) body weight, (b) BMI, (c) waist circumference, and (d) visceral fat.
Subgroup analyses
Figure 2 presents the subgroup analysis of body weight reduction by drug. The semaglutide subgroup showed a markedly greater reduction in body weight (MD = −11.45 kg (95% CI −15.78 to −7.12)), whereas exenatide and liraglutide reduced body weight by −3.67 and −5.16 kg, respectively.
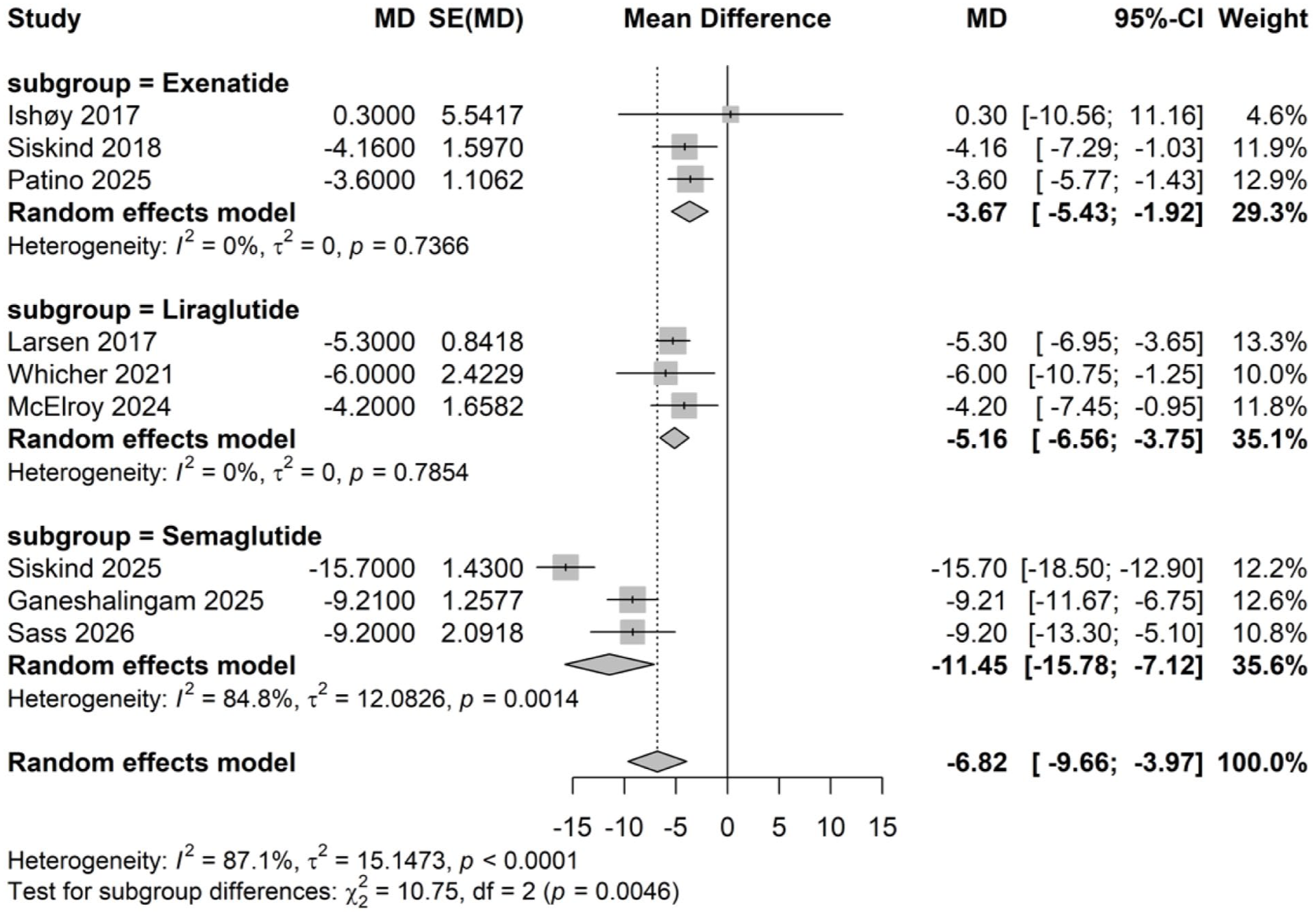
Subgroup analysis of body weight by drug ingredient.
Additional subgroup analyses were performed according to treatment duration and risk of bias categories. The nine included trials were divided into two subgroups, with one subgroup having a duration of ⩽24 weeks and the other >24 weeks. The test for subgroup differences was statistically significant (p = 0.035), indicating that treatment duration modified the effect, with longer durations associated with greater weight loss (Figure 3). Studies with ⩽24 weeks of intervention demonstrated a modest but significant reduction in weight (MD = −4.51 kg (95% CI −5.78 to −3.25)). Although the effect estimate from studies exceeding 24 weeks was larger (MD = −8.99 kg (95% CI −12.96 to −5.03)), the individual trials within this subgroup showed considerable variability in the magnitude of weight loss.

Subgroup analysis of body weight by treatment duration.
Subgroup analysis according to risk-of-bias category showed consistent weight reduction across categories (Figure 4). Studies rated as “low risk” showed the larger reduction (MD = −7.96 kg (95% CI −11.91 to −4.02)). The studies rated as “some concerns” or “high risk” showed reductions of −4.06 kg (95% CI −5.75 to −2.38). The test for subgroup differences was not significant (p = 0.0750), indicating that the overall effect was consistent irrespective of risk-of-bias rating. Subgroup analysis results for BMI and waist circumference are presented in the Supplemental Figures S3–S8.

Subgroup analysis of body weight by risk of bias category.
Sensitivity analysis
Sensitivity analyses were performed by varying the assumed pre-post correlation coefficient to 0.7 and 0.9 (Supplemental Figures S9 and S10). The pooled MDs for body weight, BMI, waist circumference, and visceral fat remained consistent with the main analysis, assuming r = 0.5. For body weight, the MD was −6.82 kg (95% CI (−9.66 to −3.97)) in the main analysis, −6.69 kg (95% CI (−9.56 to −3.83)) when r = 0.7, and −6.45 kg (95% CI (−9.40 to −3.49)) when r = 0.9, indicating robustness of the main findings. Supplemental Figure S11 shows the results of the leave-one-out analysis. The analysis demonstrated that no single study disproportionately influenced the pooled effect estimate. When each trial was sequentially omitted, the MD for body weight remained consistently significant, ranging from −7.28 kg (95% CI (−10.37 to −4.19)) to −5.67 kg (95% CI (−7.39 to −3.94)). The overall pooled estimate was stable at −6.59 kg (95% CI (−7.51 to −5.66)).
Publication bias
The funnel plot did not suggest substantial asymmetry (Supplemental Figure S12).
Certainty assessment
Table 2 presents the GRADE summary of findings and the certainty of evidence for each of the four main outcomes. Of the four outcomes assessed, weight, BMI, and waist circumference were reported in all nine trials, whereas visceral fat was available in four trials. The certainty of evidence was consistently rated as moderate across all outcomes. For visceral fat, the certainty was initially rated as high but was downgraded to moderate because of imprecision, given that the upper bound of the 95% CI lies above the minimal clinically important difference threshold of approximately 0.2–0.25 kg.
Discussion
This analysis was conducted to investigate the effects of GLP-1RAs on body weight and adiposity indices in individuals receiving antipsychotic treatment. The meta-analysis of nine RCTs involving 595 patients showed that GLP-1RAs were associated with significant reductions in body weight, BMI, waist circumference, and visceral fat. In subgroup analyses, semaglutide showed the largest effect, whereas exenatide and liraglutide produced relatively modest reductions.
When the effects of all GLP-1RAs were pooled, clinically meaningful reductions were observed across all anthropometric and adiposity measures evaluated. For body weight, the pooled estimate corresponded to a reduction exceeding 5% of baseline body weight, and semaglutide in particular achieved a reduction exceeding 10%, meeting the more stringent criteria for weight loss (Ryan and Yockey, 2017). The magnitude of BMI reduction was consistent with a comparable percentage reduction in body weight. For waist circumference, a large cohort study reported that each 5 cm increment was associated with a 13%–17% higher mortality risk (Pischon et al., 2008). The pooled reduction of 4.94 cm observed in our meta-analysis approaches this increment, suggesting that waist circumference reduction with GLP-1RAs has the potential to translate into long-term cardiometabolic benefit. For visceral fat, the point estimate of the pooled reduction exceeded 10% of the baseline value.
Previous studies have also reported similar findings supporting the role of GLP-1RAs in counteracting AIWG. With respect to weight reduction, our findings align with a prior individual patient data meta-analysis examining exenatide and liraglutide (Xie et al., 2024). That study reported mean reductions of −3.71 kg in body weight, −1.19 kg/m2 in BMI, −3 cm in waist circumference, and −177.51 g in visceral fat over 12–24 weeks (Xie et al., 2024). Beyond the RCTs included in that review, our meta-analysis also incorporated semaglutide and observed greater reductions across several anthropometric measures (Ganeshalingam et al., 2025; Sass et al., 2026; Siskind et al., 2025). Consistent with our results, a recent network meta-analysis comparing multiple pharmacological strategies including GLP-1RAs, metformin, naltrexone, and bupropion identified liraglutide and metformin as among the most effective options (Goetz-Kundera et al., 2025). When interventions were stratified by treatment duration at 12 weeks, metformin was favored in the short term and liraglutide in the longer term. By incorporating evidence from semaglutide trials, our study updates the comparative landscape and further strengthens the case for GLP-1RA-based management of antipsychotic-associated weight gain.
Antipsychotic drugs such as clozapine and olanzapine are strongly associated with weight gain and metabolic disturbances. Antipsychotics can induce insulin resistance independent of weight change by interfering with insulin signaling pathways (Hahn et al., 2013). They also promote obesity via appetite stimulation mediated by 5-HT₂C and H₁ receptor antagonism and hypothalamic AMP-activated protein kinase (AMPK) activation, with additional contributions from dopaminergic pathways and alterations in neuropeptides. In this context, metformin counteracts metabolic abnormalities by activating AMPK, reducing hepatic gluconeogenesis, improving insulin sensitivity, and indirectly attenuating appetite. By contrast, GLP-1RAs primarily reduce energy intake via central GLP-1 receptor activation and delay gastric emptying while enhancing insulin secretion and suppressing glucagon in a glucose-dependent manner. Taken together, metformin and GLP-1RAs target AIWG by modulating insulin resistance and appetites, whereas GLP-1RAs generally produce greater reductions in body weight, likely due to more potent, centrally mediated appetite suppression.
In this analysis, both waist circumference and visceral fat showed significant reductions, although the estimate for visceral fat was less precise, with its upper 95% CI bound approaching the minimal clinically important difference threshold. Two factors may account for the less precise estimate for visceral fat. First, relatively few trials directly measured visceral fat, limiting statistical power to detect a significant result. Second, waist circumference captures both subcutaneous and visceral fat and is consistently reported across studies, thereby offering greater statistical power. Population characteristics may also contribute, as the included trials primarily enrolled non-diabetic patients with schizophrenia receiving clozapine or olanzapine. Previous studies in obesity populations suggest that visceral fat reduction may be more pronounced in individuals with type 2 diabetes or NAFLD (Liao et al., 2023).
Beyond differences across outcomes, a subgroup analysis by drug revealed that semaglutide showed the greatest mean reduction in body weight. This finding is consistent with previous comparative effectiveness clinical trials in overweight or obese populations and in type 2 diabetes, in which semaglutide produced greater weight loss than liraglutide (Capehorn et al., 2020; Rubino et al., 2022). The longer half-life of semaglutide may contribute to its greater efficacy in weight reduction, and its once-weekly dosing regimen may also enhance adherence compared with once-daily liraglutide or metformin. Across RCTs with durations ranging from 9 to 40 weeks, GLP-1RAs were associated with significant reductions in body weight, BMI, waist circumference, and visceral fat. Some studies, particularly the semaglutide trial, also demonstrated greater magnitudes of visceral fat reduction (Siskind et al., 2025). As ongoing semaglutide trials are expected to show similar improvements in anthropometric outcomes, future research should determine whether these effects translate into sustained cardiometabolic benefits. Evidence from the SELECT trial has already shown that semaglutide significantly reduced major adverse cardiovascular events in patients with obesity (Lincoff et al., 2023). Further studies are warranted to assess whether such long-term cardiometabolic advantages can be generalized to patients receiving antipsychotic treatment.
The overall risk of bias across included trials was acceptable, although one study was judged as having some concerns and the other two as high risk mainly due to participant dropout. Attrition was largely attributable to treatment discontinuation. In the study with a high dropout rate, participants discontinued for reasons such as adverse events, loss to follow-up, and protocol violations (McElroy et al., 2024; Patino et al., 2025). In the remaining trials, dropout rates were not high. Notably, in the CODEX study (Siskind et al., 2018), there were no dropouts in either the intervention or placebo arm, and dropout rates in the semaglutide trials were also lower than in the other studies (Ganeshalingam et al., 2025; Siskind et al., 2025). These findings suggest that the dropout pattern in AIWG trials reflects class-specific tolerability rather than a bias unique to psychiatric cohorts. Nonetheless, treatment discontinuation remains clinically relevant, as it may attenuate real-world effectiveness compared with that observed in trials.
GLP-1RAs were generally well tolerated in patients with AIWG. Across the RCTs included in the meta-analysis, the most commonly reported adverse events were gastrointestinal issues, such as nausea, vomiting, and diarrhea, with some cases leading to treatment discontinuation. Other reasons for discontinuation included mood dysregulation or suicidal ideation, although no significant differences were observed between the intervention and placebo arms in this regard. Given that no clinically meaningful differences in psychiatric adverse events were observed, GLP-1RAs do not appear to have a negative impact on the management of underlying psychiatric disorders.
This study has some key strengths. First, we included the most up-to-date RCTs, incorporating recently published data through 2026. Second, this analysis is the first meta-analysis of AIWG that includes semaglutide, thereby extending the evidence beyond earlier reviews that were limited to exenatide or liraglutide. Third, beyond body weight, we quantitatively synthesized changes in waist circumference and visceral fat, enabling a focused evaluation of abdominal adiposity outcomes.
Several limitations should be acknowledged. First, visceral fat was reported in only four trials. Although the pooled estimate reached statistical significance, the upper bound of the 95% CI approached the minimal clinically important difference threshold. Second, the included trials varied in treatment duration, and the long-term effects on weight and cardiometabolic outcomes remain to be established. Moreover, the included trials almost exclusively involved patients treated with clozapine or olanzapine, thereby restricting generalizability to those receiving other antipsychotics.
Conclusion
To our knowledge, this is the most up-to-date meta-analysis of GLP-1RAs for AIWG, including semaglutide. We found significant reductions in body weight, BMI, waist circumference, and visceral fat. These data support the adjunctive use of GLP-1RAs in patients with psychiatric diseases and AIWG.
Supplemental Material
sj-docx-1-jop-10.1177_02698811261456190 – Supplemental material for Effects of glucagon-like peptide-1 receptor agonists on anthropometric and adiposity measures in patients with antipsychotic-induced weight gain: A systematic review and meta-analysis
Supplemental material, sj-docx-1-jop-10.1177_02698811261456190 for Effects of glucagon-like peptide-1 receptor agonists on anthropometric and adiposity measures in patients with antipsychotic-induced weight gain: A systematic review and meta-analysis by Songmin Lee, Min-Gul Kim, Mike Trott, Dan Siskind and Jae Hyun Kim in Journal of Psychopharmacology
Footnotes
Author contributions
S.L. and J.H.K. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. S.L. and J.H.K. conceived of and designed the study. J.H.K., M.G.K., M.T., and D.S. contributed to data interpretation and critical revision of the manuscript for important intellectual content. S.L. performed the statistical analyses. J.H.K. and M.G.K. obtained funding and supervised the study. All authors had final responsibility for the decision to submit for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of the Korea Machine Learning Ledger Orchestration for Drug Discovery Project (K-MELLODDY), funded by the Ministry of Health & Welfare and Ministry of Science and ICT, Republic of Korea (grant number: RS-2024-00460694).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
No new data were generated or analyzed in this study. All data included in the meta-analysis are from previously published randomized controlled trials. Summary data from the COaST trial were obtained through author correspondence.
Supplemental material
Supplemental material for this article is available online.