
Abstract
The most common setting for early intervention services for infants and toddlers with disabilities and their families is the home. This article discusses home- and community-based early intervention and how the routines-based interview (RBI) can set the stage for successful home visits. It also addresses what has been learned about home visiting, what important issues face the field with respect to home visiting, and what still needs to be learned. These same issues are discussed for IFSP development.
Home- and Community-Based Early Intervention
According to the 2007 Annual Report to Congress (U.S. Department of Education, 2010; the latest report available), between 1999 and 2004, the percentage of infants and toddlers served under the Individuals With Disabilities Education Improvement Act, Part C, increased from 68.4 to 82.7. What decreased in terms of percentage during that time was infants and toddlers whose primary setting was a program designed for children with developmental delay or disabilities.
Over the past 40 years, two parallel but not necessarily similar versions of home visiting have evolved: those for infants and young children with disabilities and those for young children from disadvantaged backgrounds (Ramey et al., 1992; Sparling, n.d.). The most widespread model of home visitation (note the terminological difference from Part C, where “home visiting” is the customary label) is probably the Olds Nurse Home Visitation Model (Olds, 2009; Olds, Henderson, Kitzman, Eckenrode, & Cole, 1999). Other nationally recognized models of home visitation are Hawaii Healthy Start, which serves families with children at risk of abuse and neglect; Healthy Families America, which serves the same target families; and Parents as Teachers, which focuses on parenting and parents’ determining children’s outcomes.
The difference between programs aimed at at-risk families and those aimed at children with disabilities and their families is highlighted by the different approaches to a curriculum. A well-defined curriculum, which is usually found in programs for at-risk families, suggests that a set series of competencies are taught to all families. In Part C, however, the curriculum is the child’s individualized family service plan (IFSP) outcomes, making it much more individualized than a curricular approach, unless a curriculum-based assessment was used to develop the IFSP. In that case, curricular content is likely to end up on the IFSP.
Organizationally, home visitation, with its large influx of federal support under the Obama administration, has been managed through Maternal and Child Health Services in the U.S. Department of Health and Human Services, whereas federal funds for Part C—with no large influx of funds—are managed through the Office of Special Education Programs, U.S. Department of Education. Part C has largely been excluded from this recent attention on home visitation.
A simplification of the evolution of home visiting in Part C could be as follows. In the 1970s, some early interventionists made regular home visits to teach parents strategies for ameliorating the effects of the infant’s or young child’s disabilities (Phemister, Richardson, & Thomas, 1978). In the 1980s, the pernicious slide toward overspecialization began, with professionals of different disciplines staking out their scope of practice (and source of revenue), leading to a multidisciplinary approach to home visiting (Woodruff & McGonigel, 1988). In the 1990s, as various professional stakeholders drove in their stakes deeper, a medical approach seeped into home visiting. Not surprisingly, the biggest challenge in the 2000s has been funding.
Routines-Based Interview
Home visits should be driven by IFSP outcomes/goals. An early intervention practice for assessing needs and current function, and for eliciting families’ outcomes/goals is the routines-based interview (RBI). Despite almost no data on its effectiveness, the RBI has been incorporated, either by mandate or as an optional activity, into procedures for many states, including Tennessee, Minnesota, Texas, Washington, Kansas, Oklahoma, Utah, Missouri, and Nebraska, as well as the Department of Defense early intervention program.
The five key features of the RBI listed below show how it is an ecologically based (Weisner, 2002) assessment process (not tool), rooted in the emerging engagement theory (McWilliam & Casey, 2008) and family systems theory (Bowen, 1966), aimed at improving family quality of life (Turnbull, Poston, Minnes, & Summers, 2007) and using goal-setting theory (Locke & Latham, 2002).
The structure of the conversation is the family’s routines of the day, defined as everyday activities (Weisner, 2002).
Child functioning within routines is conceptualized as engagement, independence, and social relationships (McWilliam, 2005, 2006); these are the areas about which the interviewer asks the family. How well a child participates (i.e., is engaged) in routines, which includes how independent the child is and the quality of the child’s communication and getting along with others, is consistent with the rising global interest in participation as the fundamental indicator of functioning (Almqvist & Granlund, 2005).
Family-level needs not necessarily tied to routines, such as time for the parent to spend without child care responsibilities, almost invariably arise.
Embedded within the RBI are ratings of satisfaction with individual home routines: At the end of the discussion of each routine, the family is asked to rate their satisfaction on a scale of 1 (terrible time of day) to 5 (great time of day). These ratings are considered an indicator of one dimension of family quality of life—one with which early interventionists can help families (McWilliam, 2010a).
The family chooses outcomes/goals at the end of the interview. Once the family has selected what they want, which is usually 6 to 12 items, they are asked to put those outcomes/goals in their order of priority.
What Have We Learned About Home Visiting?
Early studies of home visiting focused on how professionals spent their time. In a study of 15 home interventionists in Iowa, interactions among the interventionist, the child, and the parent were recorded in terms of (a) the child’s skill development and caretaking, (b) family issues, (c) community services, (d) administration and scheduling, (e) other, and (f) no interaction (McBride & Peterson, 1997). The role of the home interventionist was mostly direct teaching of the child (M = 49.74%, SD = 17.25), with coaching parents a paltry 0.36% (SD = .91). This study raised the alarm that home visits were merely a change in location from a model, in which the child goes into a center for treatment or instruction. In a report of two replications of this study, one with 28 families in early intervention and one with 92 families in Early Head Start, minimal time was focused on facilitating parent–child interactions (Peterson, Luze, Eshbaugh, Jeon, & Kantz, 2007).
Dunst and his colleagues have provided the field with a rich array of data-based approaches to early intervention, not always explicitly about home visiting but almost always applicable to it (Bruder & Dunst, 2005; Dunst, 1985; Dunst, Trivette, & Deal, 1994). Two of the most salient interventions have been helpgiving practices and learning opportunities. Family-centered helpgiving has been described as treating families with dignity and respect, providing family members with the information they need to make informed decisions, involving families actively in obtaining resources and supports, and being responsive and flexible to family requests and desires (Dunst, 2010). In a meta-analysis of 47 studies investigating the impact of family-centered helpgiving practices, the strongest effects of these practices were on satisfaction with the program and self-efficacy beliefs, with smaller effects on child behavior/functioning and parenting capabilities (Dunst, Trivette, & Hamby, 2007). Dunst has concluded that self-efficacy beliefs play an important mediation role in terms of the relationship between helpgiving practices and various outcomes.
In Part C, home visitors visit families not only in the home but also in the community. Dunst, Bruder, and colleagues studied children’s naturally occurring learning opportunities, and families identified 11 home and 11 community categories of learning opportunities (Dunst, Hamby, Trivette, Raab, & Bruder, 2000). The greater the variety of routines (i.e., activity settings) in which children participate, the more positive the consequences in both enhanced learning opportunities and child functioning were (Dunst et al., 2001). When interventionists used everyday activities as sources of learning opportunities, positive benefits accrued, but when practitioners implemented their interventions in everyday activities, negative consequences resulted (Dunst, Bruder, Trivette, & Hamby, 2006). The point is that in home and community activity settings, families, not professionals, should be implementing interventions.
Advances in carrying out home visits in the context of everyday routines have come, in part, from a tradition of embedding interventions within classroom activities (Bricker & Cripe, 1992). In a study of embedding caregiver-implemented teaching strategies in daily routines to promote children’s communication outcomes, intervention was injected into interventionist- or researcher-selected play routines (Woods, Kashinath, & Goldstein, 2004), which would seem to violate the notion that intervention should occur in the contexts where the problem was found (Dunst et al., 2006; Shelden & Rush, 2010). Nevertheless, Woods et al. (2004) were targeting communication objectives, which perhaps can be generalized across routines; they found that all four children demonstrated gains in communication objectives and that test scores across numerous domains improved. Woods’s work has promoted the use of naturally occurring routines for intervention.
Rush and Shelden (2011) have popularized the concept of coaching for a style of interaction when one person, such as a home visitor, helps another person, such as a parent, acquire desired skills. Key to coaching is the coach’s promoting “a learner’s ability to reflect on his or her actions as a means to determine the effectiveness of an action or practice and develop a plan for refinement and use of the action in immediate and future situations” (Rush & Shelden, 2005, p. 1).
An approach to home visiting that brings together many of the advances mentioned here is participation-based early intervention (Campbell & Sawyer, 2007). Campbell and Sawyer have described this approach as “recommended early intervention practices [emphasizing] family-centered approaches provided within natural settings through interventionist interactions with caregivers” (p. 287). It differs from traditional interventions in location, focus, purpose, activity, the interventionist’s role, and the caregiver’s role. For example, in these researchers’ study of 50 home visits, the role of the caregiver in 62.9% of traditional home visits was observation, whereas the role of the caregiver in 100% of the participation-based home visits was directly interacting with the child. Campbell’s line of work is providing a welcome set of data about Part C home visiting, even though it reveals a considerable challenge in battling beliefs hindering the implementation of participation-based practices.
What Important Home Visiting Issues Face the Field
The three most important issues facing the field with respect to home visiting are about dosage, actual practices during home visits, and service delivery models for home-based early intervention. Children and families have been reported to receive an average of 1 to 2 hr of Part C service per week (Buysse, Bernier, & McWilliam, 2002; Harbin & West, 1998; Hebbeler et al., 2007; Raspa, Hebbeler, Bailey, & Scarborough, 2010). In home-based early intervention, however, this is the amount of service the adults in the family receive. The intervention the child receives is not really the home visit time (e.g., 1 hr a week, if the family is lucky) but all the time between home visits. Understanding this distinction between service and intervention and capturing the dosage of intervention are vital.
The second issue is what actually occurs during home visits. Recent studies by Campbell and colleagues (Campbell & Sawyer, 2007) are tackling this question. Considering the issue of dosage just mentioned, the extent to which practitioners actually work with adult family members to help them take advantage of the child’s learning opportunities is key. The days of home visitors going into homes with a curriculum and, regardless of the child’s or family’s interest, directly attempting to teach skills to the child should be over.
The third issue is the organization of professionals on the IFSP team. Are they all seeing the family independently, as suggested by a multidisciplinary approach? Are IFSPs listing high frequencies for two or more disciplines? On what basis are service decisions—decisions about adding services, and decisions about frequency and intensity—being made? Considering most states are having difficulty funding Part C services, it is astonishing that many of them are using the multidisciplinary approach, which is expensive. It is likely this is because costs are divided among third-party payers and the State (with federal funds) and also because professionals with a financial and professional interest are unwilling to contemplate a different model.
What Do We Need to Learn About Home Visiting?
The earlier descriptions of what we have learned and what important issues face the field lay the groundwork for what we need to learn. First, we need to know how to individualize home visits—how to make them work for different types of situations. Different family circumstances, child characteristics, caregiver characteristics, and patterns of IFSP outcomes/goals might dictate different approaches. Understanding more about who is participating in Part C and what statistical clusters of families and children exist might help in the development of types of home visits, rather than relying on individual home visitors to figure out their approach.
The second type of information we need is about dosage of intervention children are receiving from their natural caregivers and how that is related to the dosage of service the family is receiving. One promising technological tool for capturing these elusive data is the Language ENvironent Analysis (LENA) System, which some researchers are in the early stages of using to capture the amount and quality of families’ talk with their children (Zimmerman et al., 2009).
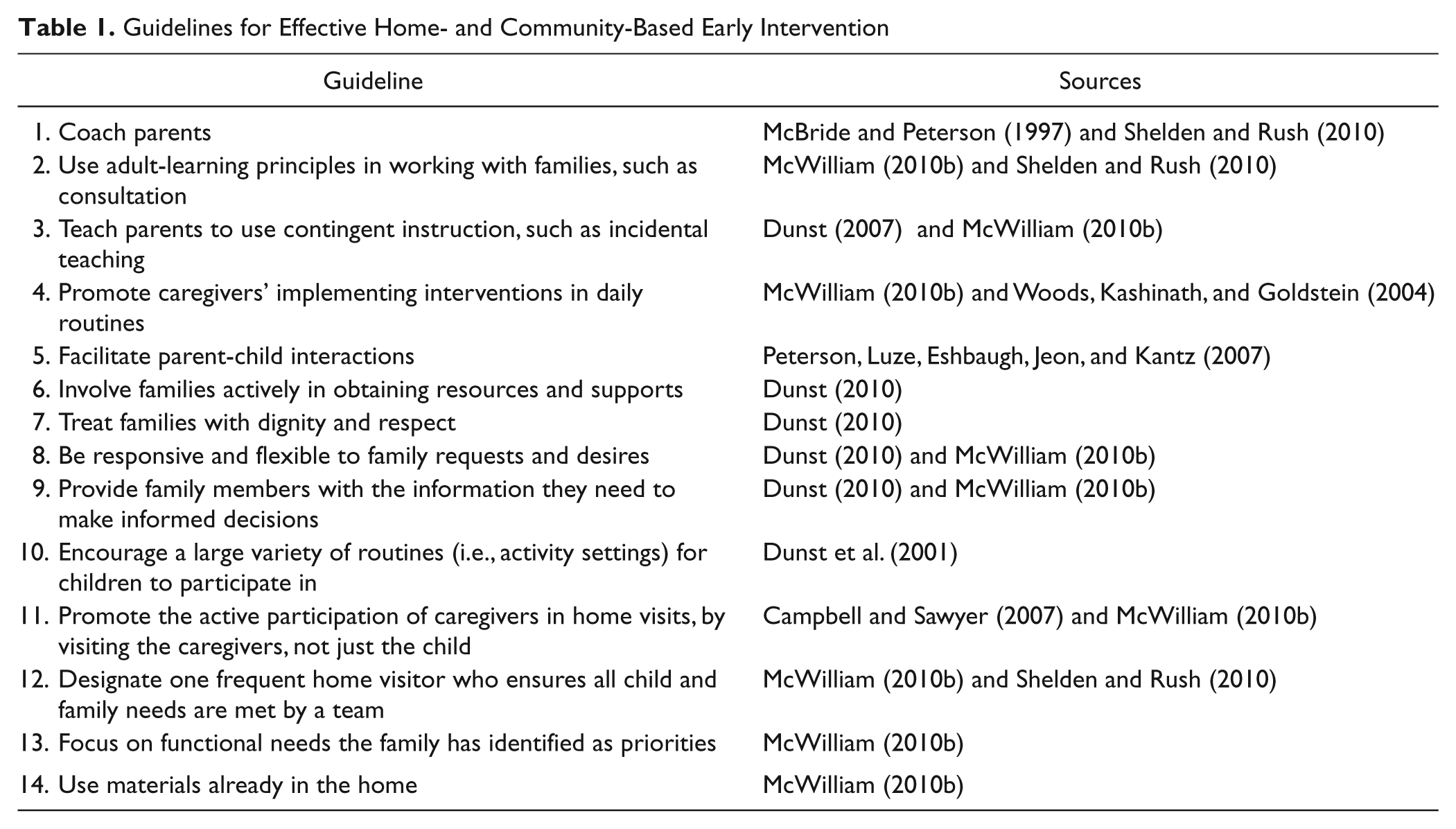
The third missing research is on specific consultation or coaching behaviors. To what extent do home visitors follow adult-learning principles? What types of consultative behaviors do they use? What is the quality of their suggestions? Do they provide consultation in all areas of development and on family-level needs? Detailed examinations need to accompany the more general but highly relevant measures such as Campbell and Sawyer’s (2007) Home Visiting Observation Form–Modified. Examining (a) the research on home visiting, (b) theory-based models for home visiting, and (c) early intervention practices that experts agree on, guidelines for effective home visiting can be provided (see Table 1). These will be followed by concluding remarks on the potential impact of home visits.
Guidelines for Effective Home- and Community-Based Early Intervention
Potential Impact of Home Visits
Home visiting might be the most misunderstood and oversimplified issue in early intervention. First, the dosage of intervention is a constant point of confusion, with people wondering how a 1-hr weekly home visit can possibly be enough help for the child. As stated earlier, however, the child does not receive just 1 hr a week of intervention. Second, families vary widely in the amount of intervention they provide children, and children vary widely in the amount of targeted intervention they need. We do not yet have good methods for determining the amount of support (e.g., service) individual families (caregivers and children) need. Third, our service delivery systems and methods are hampered by bureaucratic rigidity and slavery to the payment source. Families are receiving dosages of home visits, personnel to do home visits, and methods of home visiting that often have nothing to do with individualized needs or recommended practice. Fourth, the stuck natural-environments pendulum has decimated classroom-based options. What happens when families need the help of a classroom-based program, whether specialized (one hopes inclusive) or not, and the system won’t provide it? Fifth, effective home visits have not been institutionalized for long enough (although ineffective ones have been) to really know their strengths and weaknesses for different families and different children. States need to pay as much attention to the quality of their services as they do to compliance with Individuals With Disabilities Education Act (IDEA), which does not address methods.
Home visiting can be powerful in its effects on families and thereby on children. The good home visitor, in collaboration with the service coordinator, if that’s a different person, should ensure that the quantity and quality of intervention the child receives through home visiting is likely to be effective. If not, they should work with the family to explore additional or other supports. Perhaps the home-visiting approach should change. Perhaps the child should be enrolled in a classroom program. Perhaps other family members can help. True support-based home visiting should be able to work it out. States and local agencies need to make it happen.
What we have learned, therefore, is that home visiting practices are still evolving, that there is not much research on such practices, and that there is a gap between what experts recommend and what happens in the field. Promising practices, however, are those that take advantage of naturally occurring learning opportunities and a participation-based approach.
What Have We Learned About IFSP Development?
Considerable research has been conducted on IFSP development. In the 1990s, parents were observed to have only partial decision-making power in IFSP meetings (Minke & Scott, 1993), which might be explained by a subsequent study showing professionals had concern about whether families had the necessary skills for full participation in IFSP development (Minke & Scott, 1995). Concerns about going too far into families’ lives and about families’ abilities to participate fully in developing the IFSP might explain why IFSPs have been found to have overwhelmingly more child-related goals than family-related goals (Bailey, Winton, Rouse, & Turnbull, 1990; McWilliam et al., 1998). In a qualitative study using focus groups comprised of family members as well as professionals, including national and state leaders, participants agreed strongly that informal methods should be used to gather information about families to develop the IFSP (Summers et al., 1990).
The quality of IFSPs has indicated that the methods for developing it leave something to be desired. An analysis of the family dimensions of early examples of IFSPs showed that criteria for goal attainment were generally absent (Bailey et al., 1990). Jung and Baird (2003) found, however, that experience and attendance at training were related to IFSP quality.
Despite the cautions of early experts that professionals should not delve too deeply into families’ lives and despite the fact that IFSPs are still predominantly child focused (Krauss, 2000), the RBI is designed to capture children’s and families’ needs related to everyday routines, so families have a structure for identifying the child-level and family-level outcomes they would like on their IFSPs (McWilliam, 2010b, 2010c). Preliminary evidence about the RBI, which is all that exists, showed that it produced better outcomes than did the traditional approach to IFSP development, more satisfaction by families, more outcomes/goals, and more functional outcomes/goals (McWilliam, Casey, & Sims, 2009).
IFSP development is important because theoretically it is the agreement about what needs will be tackled by the team and it also lists the services that the system will marshal to do. Therefore, the first important issue facing the field is that professionals need to develop serious attempts to ascertain family-level needs.
Perhaps all the cautions in the early days after the passage of the law were taken too much to heart, but the IFSP’s team by and large are not completing the concerns, priorities, and resources section of the IFSP with any rigor. I am not arguing for a formal assessment process (Cox, Keltner, & Hogan, 2003), but I am arguing for teams to take the time to do this assessment properly.
The second issue regarding IFSP development is the definition of functionality. It is now received wisdom to claim we are assessing and working on functional skills, so a definition is needed. Globally, the World Health Organization’s definition of functioning as participation in home, school, and community has had an impact on some countries’ early intervention policies and practices (Perenboom & Chorus, 2003; Simeonsson et al., 2003; World Health Organization, 2007).
The importance of engagement, a form of participation (McWilliam & Casey, 2008; Pinto, Barros, Aguiar, Pessanha, & Bairrão, 2006), constitutes the third issue. A number of reasons can be claimed for focusing on engagement. First, children cannot learn if they are not engaged (McWilliam, Trivette, & Dunst, 1985). Second, some conceptualizations of engagement include a developmental continuum of sophistication, so caregivers and professionals can work toward the differentiation and complexity of engagement (McWilliam, Scarborough, & Kim, 2003); it is not simply a dichotomous (engaged vs. nonengaged) construct. Third, engagement is an exhaustive construct, in that all behaviors can be classified as some type and level of engagement (de Kruif & McWilliam, 1996). This allows interventionists to focus on the big picture (i.e., engagement or participation), without getting bogged down in the minutiae of the individual skills being taught.
What Do We Need to Learn About IFSP Development
The three questions about IFSP development, specifically the RBI, are the impact of this process on (a) interventions conducted by natural caregivers, (b) family outcomes, and (c) child outcomes.
One of the rationales for conducting an RBI is to hear from natural caregivers (i.e., family adults and teachers) about what happens in routines and to allow families to select contextually relevant outcomes/goals. This makes the support provided by professionals salient for the child’s and family’s everyday routines, which theoretically increases the likelihood that caregivers will carry out interventions. This theory needs to be tested empirically: Does (a) the RBI lead to (b) outcomes/goals that lead to (c) consultation/coaching that leads to, (d) a high rate and quality of intervention delivered by the caregiver to the child?
Because the RBI produces more family-level outcomes/goals than traditional IFSP development practices do (McWilliam et al., 2009), the impact on family outcomes should be examined. The question of impact on the family can be asked in three ways: (a) Does the RBI identify family-level needs in a way the family desires? (b) Does the RBI itself have a positive impact on families (e.g., feeling listened to, confidence in the team)? and (c) Does use of the RBI lead to attainment of the federally mandated family outcomes?
Similarly, questions remain about the impact of the RBI on child outcomes: (a) Does the RBI identify more meaningful, functional needs than do other assessment procedures used for IFSP development? and (b) Does the use of the RBI lead to attainment of the federally mandated child outcomes? It is likely to do so because of the conceptual alignment between the three functioning areas addressed during the RBI (engagement, independence, social relationships) and the three federal child outcomes (using knowledge and skills, taking action to meet needs, and engaging in social relationships).
IFSP development is characterized by poor attention to family needs and has been shown to result in low-quality plans. The RBI is a useful practice to generate a family’s true priorities, to establish a positive relationship with the family, and to obtain a rich and thick description of child and family function.
As the most common method for providing early intervention services, home visits need to be explored and tested. Especially with the federal requirement to provide services in the natural environment, home- and community-based early intervention can no longer be a mystery. Furthermore, IFSP development has the potential to shape how services are provided, and the RBI is a promising process for making the IFSP and the subsequent interventions relevant.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.