
Abstract
Using the Early Childhood Longitudinal Study–Birth Cohort (ECLS-B), a nationally representative data set, we examined the extent to which mothers of preschool children with and without the diagnosis of an Autism Spectrum Disorder (ASD) reported stress and depressive symptoms prior to and following diagnosis of ASD. At 4 years, approximately 100 children were parent-identified as diagnosed with ASD. Mothers of children with ASD at 9 months and 4 years had significantly higher incidence of depressive symptoms and stress than mothers of typically developing children. Mothers of children with ASD experienced higher levels of depressive symptoms than mothers of children with disabilities, but the difference was not statistically significant. Using linear regression, a within-group comparison of depressive symptoms of mothers of children with ASD indicated no differences based on child gender, ethnicity, number of children in the family, or partnership status. Implications are presented.
The challenges to family life of raising children with Autism Spectrum Disorders (ASD) are well detailed in the literature. Less understood is the impact on maternal well-being, particularly in families of very young children with autism (Herring et al., 2006). From a practitioner’s perspective, helping families successfully adapt to the stressors of caring for children with ASD first requires identification of those stressors followed by intervention to reduce or eliminate those with negative impact on family function (e.g., family relationships in daily activities). The current research on ASD indicates that families often recognize something is amiss when their children do not reach communication and social interaction milestones at typical ages (Osterling & Dawson, 1994; Ozonoff et al., 2010; Robins, Fein, Barton, & Green, 2001). Families are faced with mobile children who often exhibit behaviors that can be isolating from social interactions with friends, extended family, and society at-large (Cassidy, McConkey, Truesdale-Kennedy, & Slevin, 2008; Hastings et al., 2005; Trute & Hiebert-Murphy, 2005; Woodgate, Ateah, & Secco, 2008). Davis and Carter (2008) pointed out that when autism is diagnosed in early childhood, “the very high parenting stress levels observed may be in part due to what has been considered a crisis period of the early adaptation to the diagnosis” (p. 1289).
Definitions of Depression and Stress
The primary reason to study stress and depression is to analyze the link between those conditions and detrimental individual, familial, and societal outcomes (Singer, 2006). Particularly in young children, the effect that stress and depression can have on the mother–child bond is pertinent. Addressing the question of whether mothers of children with disabilities (and in this case, ASD) experience more stress and depression than mothers of children without disabilities may assist researchers to better understand the etiology of depression in women in general (Singer, 2006). Finding the root of the depressive symptoms and stress may guide practice in intervention with families of children with ASD.
The World Health Organization (2001) defined depression as,
(A) common mental disorder that presents with depressed mood, loss of interest or pleasure, feelings of guilt or low self-worth, disturbed sleep or appetite, low energy and poor concentration. These problems can become chronic or recurrent and lead to substantial impairments in an individual’s ability to take care of his or her everyday responsibilities . . . Depression can be reliably diagnosed in primary care. (p. 1)
Furthermore, the National Institute of Mental Health (NIMH; 2008) asserted that diagnosis and treatment of depression require a complete diagnostic evaluation by a doctor or mental health professional and may include physical examination, an interview with complete history of symptoms, and/or laboratory tests. Although the research literature written prior to the 1990s used the term depression with little regard to a clinical or medical diagnosis, current thinking supports use of the term depressive symptoms, particularly when information is from a one-time screening tool.
The term stress is a more general term for physical, mental, or emotional response to events that cause bodily or mental tension. Lazarus and Folkman (1984) emphasized “psychological stress is a particular relationship between the person and the environment that is appraised by the person as taxing or exceeding his or her resources and endangering his or her well-being” (p. 19). Due to a similarity between stress and depressive symptoms in impairment to daily functioning and personal well-being, studies using either term were reviewed.
Child Traits and Behavior That Affect Maternal Stress
The difficult traits and behaviors exhibited by children with autism, and the corresponding contribution to maternal stress, are a common theme in the literature (e.g., Baker-Ericzen, Brookman-Frazee, & Stahmer, 2005; Davis & Carter, 2008; Herring et al., 2006; Hoffman et al., 2008; Hoppes & Harris, 1990; Tobing & Glenwick, 2006; Tomanik, Harris, & Hawkins, 2004). The difficulties in communication, social interaction, and even sleep take a toll on the child with autism, as well as on his or her mother. In a few longitudinal studies (Baker-Ericzen et al., 2005; Herring et al., 2006), the importance of addressing emotional and behavioral problems associated with autism during early childhood was highlighted. As Baker-Ericzen and colleagues found, a child’s level of social skills was a significant predictor of child-related maternal stress for mothers of children with autism. Likewise, Herring and colleagues found that emotional and behavioral problems of children with autism contributed at a significantly higher rate to maternal stress, parent mental health problems, and perceived family dysfunction when compared with children with developmental delay without a diagnosis of autism. Studies provide persuasive data that “parents of children with autism experience more stress and are more susceptible to negative outcomes than parents of children with other disabilities” (Dunn, Burbine, Bowers, & Tantleff-Dunn, 2001, p. 39). Hastings and Brown (2002) found that feelings of isolation and overburdened responsibility may occur when raising a child with ASD and coping required positive self-efficacy to counteract the stressful effects. Not only is stress reported at a higher level, but potential mental health problems like depression are also higher, particularly for mothers of young children with ASD (Hastings & Brown, 2002).
Because ASD occurs at a rate of 3 to 4 times higher in males than in females (NIMH, 2004), all the studies reviewed have a high percentage of mothers raising sons with autism. Little is known whether there are differences in maternal stress between raising boys and girls with ASD. As the current trend toward early diagnosis continues, there has been an increase in studies focusing on the family impact of raising toddlers and preschoolers with ASD (Baker-Ericzen et al., 2005; Cassidy et al., 2008; Davis & Carter, 2008; Herring et al., 2006). A number of studies reviewed contained samples that were homogeneous in race (i.e., Caucasian) and socioeconomic status (SES; middle to high income), making generalizations to other populations difficult (e.g., Davis & Carter, 2008; Dunn et al., 2001; Smith, Seltzer, Tager-Flusberg, Greenberg, & Carter, 2008; Tobing & Glenwick, 2006; Wachtel & Carter, 2008). Within these studies, maternal adaptation to the diagnosis of a child’s ASD and perceived social support were found to be consistently correlated to levels of maternal stress.
Limitations of Current Research
While significant research over the past 10 years has identified early characteristics of young children with ASD, current knowledge of the effect ASD has on family function and maternal stress and depression in the early years is based largely on studies that utilize small or unrepresentative samples (e.g., samples that include both toddlers and teenagers) with minimal controls for salient variables such as family demographics including SES (e.g., Duarte, Bordin, Yazigi, & Mooney, 2005; Ekas, Lickenbrock, & Whitman, 2010; Hastings, 2003; Johnson, Frenn, Feetham, & Simpson, 2011; Olsson & Hwang, 2001; Tehee, Honan, & Hevey, 2009).
Among other limitations noted, researchers recommend caution in interpreting the representativeness of a sample population to all parents of young children with ASD, as it is unknown whether parents with depression or high levels of stress were more likely or less likely to respond to surveys (e.g., Olsson & Hwang, 2001) or whether parents are those with the time, energy, and resources needed to participate in a longitudinal study (e.g., Estes et al., 2009). In addition, single administration of the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977), the Parenting Stress Index–Short Form (PSI-SF; Abidin, 1990), or other measures of stress or depression may not give a complete picture as times of stress and depressive symptoms may vary considerably depending on how recently a diagnosis of autism was made (Davis & Carter, 2008; Gill & Harris, 1991). As Hastings and colleagues (2005) suggested, family adaptation may change over time and it is important to ask whether similar results on measures of maternal stress and depression are seen at different time points in the life of a child with autism.
Such limitations reduce the ability to draw conclusions about very young children with autism and their families. This gap in the knowledge base hampers the efforts of researchers, policy makers, and early intervention service providers as they seek to develop and implement initiatives designed to address the social support needs of families of young children with autism. This study builds upon existing research literature by using the Early Childhood Longitudinal Study–Birth Cohort (ECLS-B) data set. The ECLS-B is a nationally representative, longitudinal data set of approximately 11,000 U.S. children born in 2001. Indeed, the size and longitudinal nature of ECLS-B allows for statistically rigorous analyses. With diagnosis of ASD by a physician, reported at 4 years of age, and data collected at 9 months, 2 years, and 4 years, maternal well-being can be studied at multiple time points before and at the time of parent report of diagnosis. In addition, identifying the depressive symptoms of parents raising children with ASD at specific ages eliminates the problems inherent in small sample studies with large age ranges of children. The ECLS-B provides concrete data for this early childhood group, when families are coping with a diagnosis of ASD.
Purpose of the Study and Research Question
The purpose of this exploratory study was to examine factors that affect the functioning and outcomes for families and for children with ASD using the ECLS-B data set. Measures of maternal well-being before and at the time of reported diagnosis of ASD were examined. Specifically, the following research questions were addressed:
Research Question 1: Do mothers of preschool children with diagnoses of ASD report more stress and depressive symptoms than mothers of children with other disabilities and mothers of typically developing children, prior to diagnosis and/or following diagnosis?
Research Question 2: Concerning mothers of children with ASD, is there a difference between levels of stress and depressive symptoms before and at the time of report of diagnosis of ASD?
Research Question 3: Are there differences between mothers of children with ASD on measures of depressive symptoms based on characteristics of the child or the family (e.g., gender of the child, race or ethnicity of the child, number of children in the family, presence of a parenting partner)?
Method
Sample
The ECLS-B is a nationally representative, longitudinal data set of approximately 11,000 U.S. children born in 2001. The data set includes oversamples of Asian and Pacific Islander children, American Indian and Alaska Native children, Chinese children, twins, and children who were low/very low birth weight. Data for the ECLS-B were gathered from children, parents, child care providers, teachers, and school administrators (Snow et al., 2007). Data collection methods used in the ECLS-B included parent interview, self-administered survey questionnaire, and observational data collection formats, in addition to direct assessments of children’s growth and development by trained field interviewers and observers (for a complete discussion of training of these data collectors see Snow et al., 2007). Diverse socioeconomic and racial/ethnic backgrounds are represented in the data. The use of the weights provided by National Center for Educational Statistics (NCES; Nord, Edwards, Andreassen, Green, & Wallner-Allen, 2006) reduces any bias associated with missing data, including bias due to attrition.
As required by the NCES, researchers using the ECLS-B data report all sample sizes (including the sample of children with ASD) rounded to the nearest 50. In accordance with existing Institutional Research Bureau protocol regarding analysis of a data set already collected, this study focused on a subsample of families of children diagnosed with autism. The data packets available to researchers have been de-identified and are without any key linking identifiers to participants. In addition, using an inferential study design on the longitudinal data found in the ECLS-B, we can infer the characteristics of all children born with ASD in 2001 from the nationally representative sample of nearly 100 children with ASD. Comparison groups with sufficient data for comparison with the children with ASD included a sample of all children with typical development (approximately 8,500 children) and a sample of children with disabilities not including ASD (approximately 900 children). The ECLS-B data set contains sufficiently robust information to compare children with certain disabilities versus children with other disabilities or without disabilities on measures of development on norm-referenced assessments, observations, and parent surveys (Livermore, Whalen, Prenovitz, Aggerwal, & Bardos, 2011).
To derive a sample of 100 children diagnosed with ASD, parents reported to ECLS-B interviewers at the third data collection point (at approximately 4 years old) whether a doctor had told them that their child has autism or Pervasive Developmental Disorder (PDD). Increasing use of large data sets available through online registries such as the Interactive Autism Network (IAN) requires parent report of child’s diagnosis of ASD to be valid and reliable. In a recent study by Daniels and colleagues (2012), parent report of diagnosis of ASD was verified by medical diagnosis documentation in 98% for the study sample participants drawn from the IAN. Likewise, the Center for Disease Control (2006) noted the consistency in reports from the National Health Interview Survey (NHIS) and the National Survey of Children’s Health (NSCH) suggests high reliability for parental report of autism. This study sample of approximately 100 children is characterized in Table 1.
Sample Demographics of Children Diagnosed With ASD at 4-Year-Old Time Point.
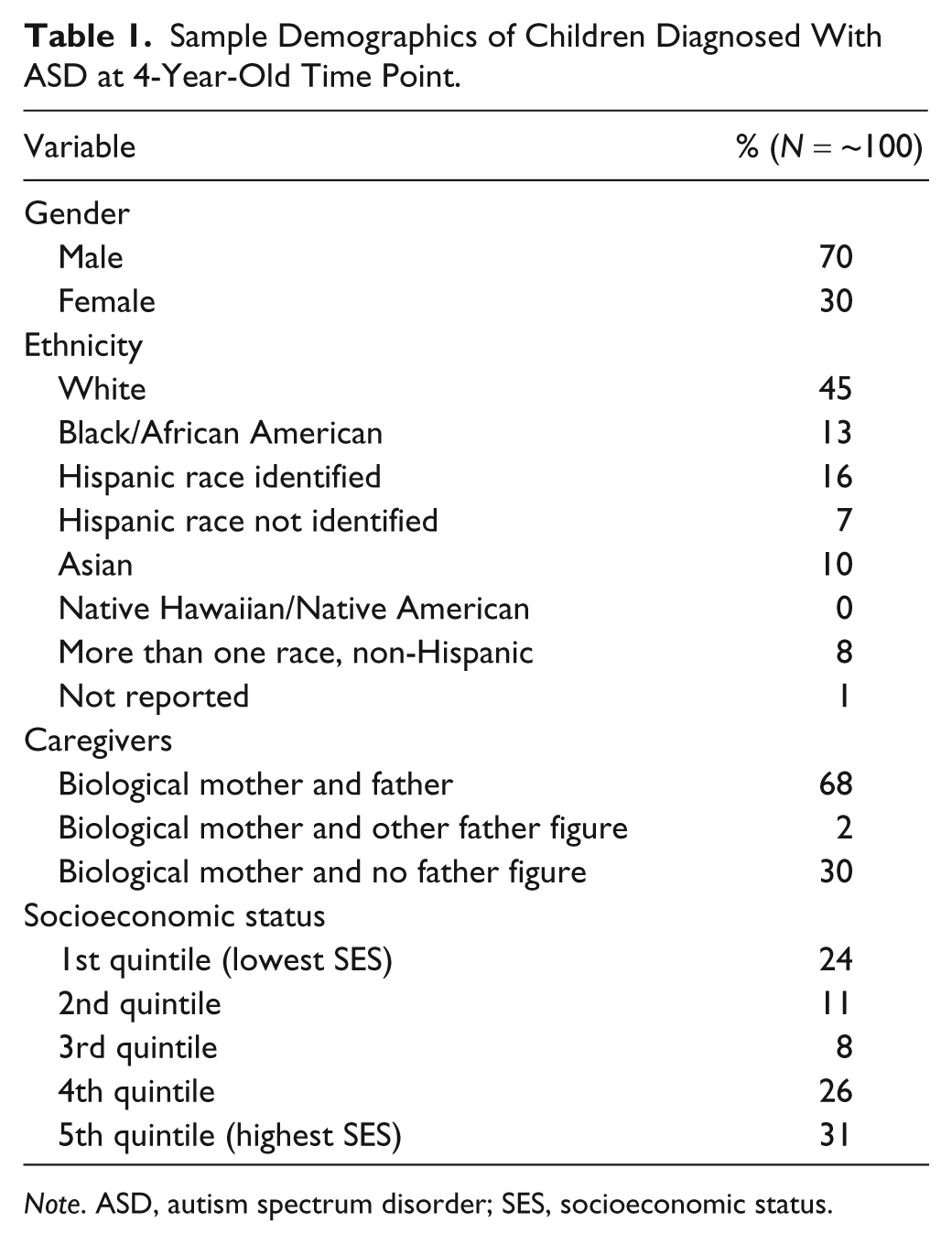
Note. ASD, autism spectrum disorder; SES, socioeconomic status.
Characteristics of the children with ASD in the ECLS-B mirror other research to date. The NIMH (2004) found a much higher prevalence of males (3–4 times as many) diagnosed with ASD versus females. The study sample drawn from the ECLS-B comprises 70% males. As numerous researchers indicate, there is a strong occurrence of autism in families of Caucasian ethnicity (Hastings et al., 2005; Herring et al., 2006). In the ECLS-B sample, 45% of the children with ASD were Caucasian, yet unlike other studies, the presence of other ethnicities (e.g., Hispanic and African American) may provide future insights into unique characteristics of families of young children with ASD.
Data Set Design
The ECLS-B data set uses a complex survey design with a multistage cluster sample (Nord et al., 2006) where the selection of one participant is related to the selection of another participant and, therefore, not a random selection. As most statistical analysis assumes random sampling, it is necessary to adjust the estimate of SE when using the ECLS-B data set. The data set provides variables for the jackknife method to adjust SEs when estimating variance, as outlined by the NCES (Nord et al., 2006). The ECLS-B also provides full sample weights and 90 replicate weights that are used when analyzing data to reduce bias introduced by differential selection probabilities and nonresponse. Furthermore, by adjusting SEs and applying appropriate weights, the findings from the project analyses can be generalized to the U.S. population of children born in 2001.
The statistical software Stata (StataCorp, 2007) was used to compute basic descriptive statistics and more complex statistical models (i.e., multinomial logistic regression). Stata is one of the three programs suggested for analysis of the ECLS-B data set (Snow et al., 2007). Given the ECLS-B uses a complex survey design, Stata has the flexibility to take this into account using its “survey” command.
Measures of Stress and Depressive Symptoms
For the first research question, we examined the severity of maternal depressive symptoms and the extent to which mothers of preschool children with diagnosis of ASD reported more stress and depressive symptoms than their counterparts (i.e., mothers of children with other disabilities and mothers of typically developing children) prior to diagnosis and at the time of reported diagnosis. The ECLS-B version of the CES-D (Radloff, 1977) measured depressive symptoms in mothers at the 9-month and 4-year time points. Unfortunately, a longer diagnostic interview tool, the Composite International Diagnostic Interview Short Form (CIDI-SF; Kessler, Andrews, Mroczek, Üstün, & Wittchen, 1998) was used at the 2-year time point and scores were not comparable. Based on CES-D scores, mothers were assigned 0 to 3 to indicate the severity of depressive symptoms (0 = no depressive symptoms to 3 = severe depressive symptoms). Percentages of mothers were calculated for each of the four levels of severity of the depressive symptoms for each group of mothers. Multinomial logistic regression analysis was used to compare children with and without disabilities (0 = child with no disability, 1 = child with other disability, 2 = child with ASD) at the 9-month and 4-year time points, controlling for child gender, average parent age, birth weight, SES, race/ethnicity, and age of child at assessment.
For measures of stress at the 9-month time point, in addition to depressive symptoms scores on the CES-D (Radloff, 1977), mothers were asked two “yes–no” questions in a self-administered questionnaire: “In the past 12 months, have you talked with a psychiatrist, psychologist, doctor, or counselor for any emotional or psychological problem?” and “During the past 12 months, have you felt, or has anyone suggested, that you needed help for any emotional or psychological problem?” Logistic regression was used to analyze these dichotomous variables for comparisons of mothers of children with ASD to mothers of children with other disabilities and children who were typically developing. At the 4-year time point, the ECLS-B adaptation of the PSI-SF (Abidin, 1990) was used to measure mothers’ report of stress. Multiple linear regression analyses were used to analyze the scores of the PSI-SF at the 4-year time point and the CES-D (Radloff, 1977) at both time points for comparisons of all three groups of mothers.
Linear regression was used to conduct a within-group comparison of the mothers of the children with ASD at the 9-month and 4-year time points using the outcome of depressive symptoms, as measured on the CES-D. In an effort to examine the level of depressive symptoms at the time point of diagnosis (i.e., the 4-year point) and at an earlier time (i.e., the 9-month time point), the mothers of the children with ASD were compared based on child gender (e.g., females vs. males with ASD), ethnicity (e.g., White vs. non-White), number of children in the family (e.g., only child vs. siblings), partnership status (e.g., single parent vs. partnered parenting). In addition to controls added to the regression models (e.g., ethnicity, SES quintile, birth weight, average age of parents, and child’s age at assessment), the standard errors were adjusted and appropriate weights were applied with p values of t tests and confidence intervals (CIs) calculated.
Results
Across-Group Comparisons
Mothers of children with ASD reported more moderate and severe depressive symptoms than their counterparts at both time points (see Table 2). At the 9-month time point, a higher percentage of mothers of children with ASD reported moderate and severe levels of depressive symptoms (30.4%) than mothers of children with disabilities (21%) and mothers of children who were typically developing (16.7%). Very similar figures were obtained from the 4-year time point with mothers of children with ASD having higher percentage of members with moderate and severe levels of depression (32.1%) when compared with mothers of children with disabilities (23.3%) and mothers of children who were typically developing (18.1%).
Percentage of Mothers With Symptoms of Depression on CES-D.
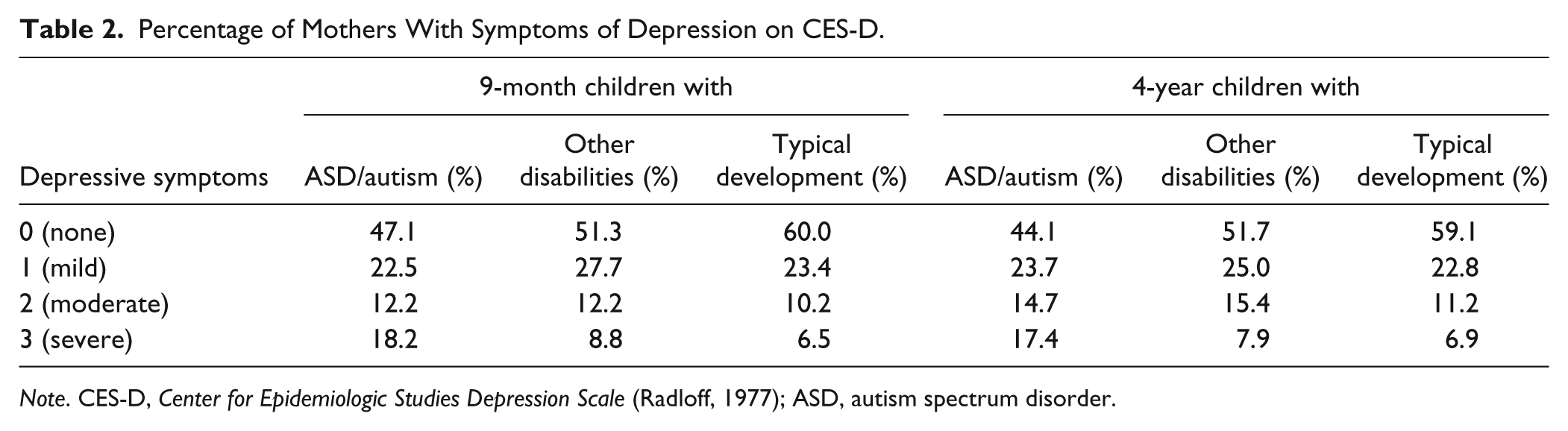
Note. CES-D, Center for Epidemiologic Studies Depression Scale (Radloff, 1977); ASD, autism spectrum disorder.
Means and standard deviations of scores for maternal symptoms of depression, emotional concerns, and stress for mothers of children with ASD, children with disabilities, and typically developing children at two time points are reported in Table 3.
Means and Standard Deviations of Scores for Maternal Symptoms of Depression, Emotional Concerns, and Stress for Mothers of Children With ASD, Children With Disabilities, and Typically Developing Children at Two Time Points.

Note. ASD, autism spectrum disorder; CES-D, Center for Epidemiologic Studies Depression Scale (Radloff, 1977); PSI-SF, Parenting Stress Index–Short Form (Abidin, 1990).
To examine measures of depressive symptoms and stress across all three groups of mothers (i.e., mothers of children with ASD, mothers of children with other disabilities, and mothers of children who were typically developing), several analyses were conducted and can be found in Table 4. When using large data sets like ECLS-B, it is critical to apply appropriate weights for the assessment age of the children and for missing data, in addition to the controls for variables such as race/ethnicity, SES quintile, average age of parents, and birth weight, to minimize the risk of bias. Using logistic regression analysis, we found mothers of 9-month-old children with ASD reported seeking help (or were told they should) from health care professionals for emotional or psychological concerns more often than mothers of typically developing children but not more than mothers of children with disabilities. Through multinomial logistic regression analyses, we found that mothers of children with ASD (at both time points) had significantly higher incidence of depressive symptoms and stress than mothers of typically developing children but not more than mothers of children with disabilities. Mothers of children with ASD experienced higher levels of depressive symptoms than mothers of children with disabilities, but the difference was not statistically significant.
Analysis of Depressive Symptoms, Emotional Concerns, and Stress for Mothers of Children With ASD, Children With Disabilities, and Typically Developing Children at Two Time Points.
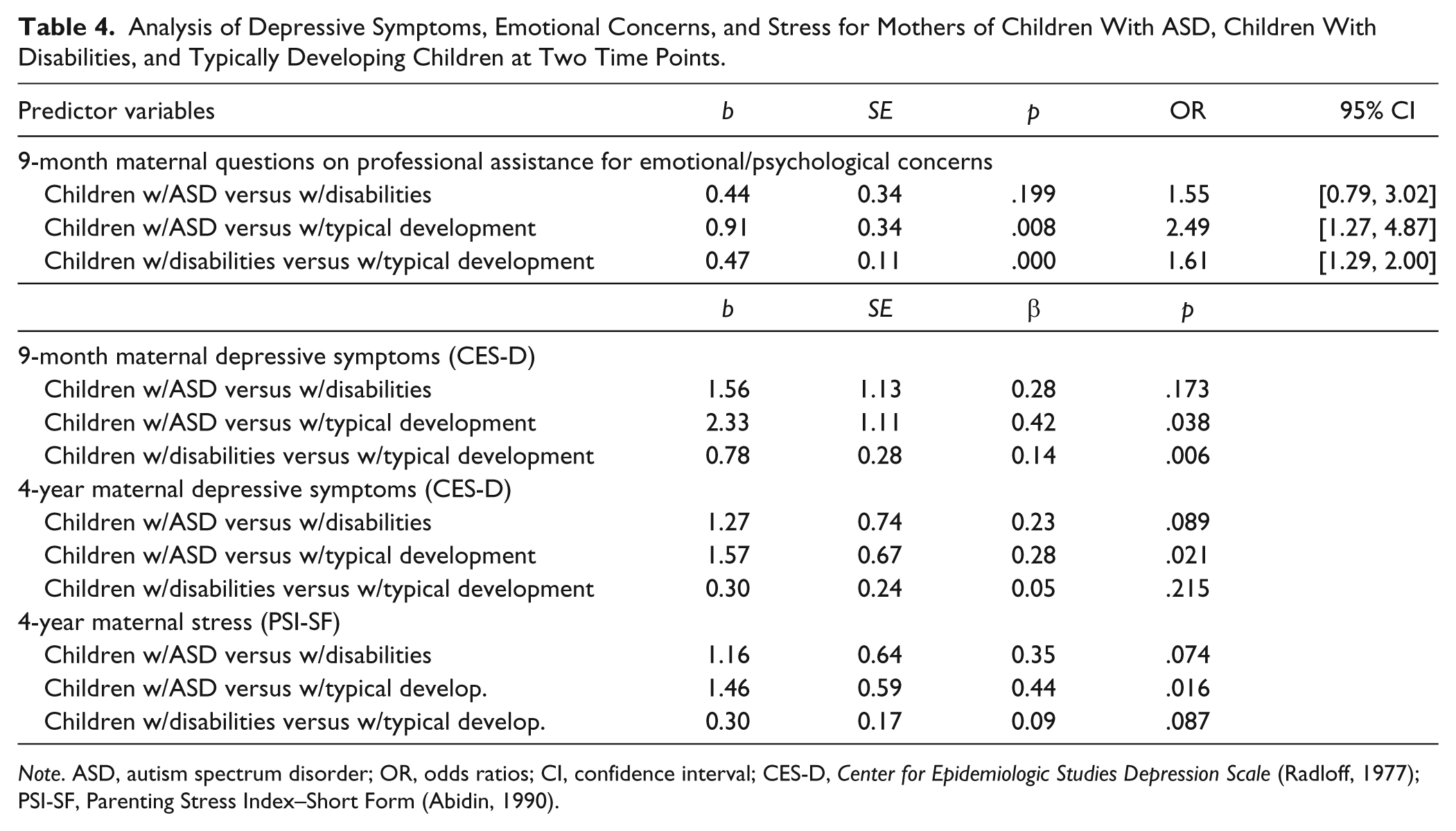
Note. ASD, autism spectrum disorder; OR, odds ratios; CI, confidence interval; CES-D, Center for Epidemiologic Studies Depression Scale (Radloff, 1977); PSI-SF, Parenting Stress Index–Short Form (Abidin, 1990).
Maternal depressive symptoms were significantly correlated from 9 months to 4 years for all mothers. A comparison of the partial correlation coefficients (controlling for demographic characteristics) using Fisher’s r-to-z transformation indicated that the across-time stability of depressive symptoms was stronger for mothers of children with ASD than for mothers of children with other disabilities (z = 2.04, p = .041) and mothers of typically developing children (z = 1.88, p = .060). The stability of depressive symptoms did not differ significantly when comparing the other two groups (z = −0.75, p = .453).
Within-Group Comparisons
To examine other factors affecting the level of depressive symptoms at the time point of report of diagnosis (i.e., the 4-year point) and at an earlier time (i.e., the 9-month time point), the mothers of children with ASD were compared based on child gender (e.g., females vs. males with ASD), race/ethnicity (e.g., White vs. non-White), number of children in the family (e.g., only child vs. siblings), partnership status (e.g., single parent vs. partnered parenting). Recommended weights and controls (e.g., race/ethnicity, SES quintile, age of parents, birth weight, and child age at assessment), were used in our analyses to minimize the risk of bias, and p values of t tests and CIs were calculated, using linear regression. There were no significant differences found in measures of maternal depressive symptoms of mothers of children with ASD based on child gender (p = .978 at 9 months and p = .344 at 4 years), race/ethnicity (p = .892 at 9 months and p = .814 at 4 years), number of children in the family (p = .280 at 9 months and p = .292 at 4 years), or partnership status (p = .637 at 9 months andp = .170 at 4 years).
Discussion
Findings from this study confirm the findings of Estes and colleagues (2009) and Davis and Carter (2008) who reported significantly high levels of stress and depressive symptoms in mothers of children with ASD compared with mothers of children with other disabilities and those with typically developing children. Based on our analyses, the major findings of this study indicate that mothers of preschool children with diagnosis of ASD report significantly more stress and depressive symptoms prior to diagnosis and following diagnosis when compared with mothers of typically developing children. Mothers of children with ASD reported more stress and depressive symptoms before and after diagnosis in comparison with their counterparts raising children with other disabilities, but the difference was not statistically significant.
In addition, we found that when mothers of young children experience stress and depressive symptoms in the early months of their children’s lives, they were more likely to continue to experience stress and depressive symptoms into the preschool years, particularly when parenting children with ASD. The notably moderate and severe levels of depressive symptoms observed at 9 months and at 4 years in mothers of children with ASD (see Table 2) suggest the need for supportive interventions focused on mother and child.
Among the mothers of children with ASD, we found no significant differences on measures of depressive symptoms when compared for characteristics of the child or the family. In other words, no difference was found between levels of depressive symptoms based on the gender of the child, the race or ethnicity of the child, the number of children in the family, or the presence of a parenting partner. Guided by this information, practitioners working with families of young children with ASD are cautioned against making assumptions based on these child and family characteristics and encouraged to examine the individual family features that may be contributing to maternal stress and depressive symptoms.
The ECLS-B data set is nationally representative and contains a large collection of mothers of children with disabilities (including ASD) and who are typically developing. Because mothers of children with ASD are not specifically targeted for participation, the potential biases associated with self-selection for participation in a study of maternal stress and depressive symptoms are greatly reduced. The ongoing levels of moderate to high depressive symptoms found in the mothers of children with ASD is an area of concern, and future research following these mothers as the children enter kindergarten would be useful for identifying coping strategies and outside assistance that may have been utilized.
Mothers of children with ASD in this study had more symptoms of depression than their counterparts. As the literature suggests, the predictor characteristics of children (e.g., communication and social skills) as well as the actual diagnosis of ASD by a physician can have an effect on the presence or absence of maternal stress and symptoms of depression, and in addition, predict the child and family outcomes measured (e.g., maternal involvement, intact marriage, and preschool skills). Future research should examine whether maternal stress and symptoms of depression have a direct effect on child and family outcomes or have an indirect moderating or mediating influence on child and family outcomes.
Trivette, Dunst, and Hamby (2010) described a family-systems model that may be useful in intervention practices when working with families raising young children with ASD, particularly with the presence of high levels of maternal depressive symptoms found in this study. The model uses capacity building, help-giving practices where family members identify their needs, the supports and resources to meet those needs, while using the family members’ existing strengths, as well as constructing new abilities to obtain support and resources to meet their needs. Germane findings from the Trivette et al. study suggest parents’ beliefs in their ability to control life events (self-efficacy) and overall well-being directly and indirectly affect their interactions and with their child. Consequently, the presence of stress and depressive symptoms evident in mothers in this study should be addressed for the sake of the optimal development of children with ASD.
Limitations
Unfortunately, the second time point of data collection in the ECLS-B used the CIDI-SF (Kessler et al., 1998) for measures of depressive symptoms and was not comparable with scores using the CES-D (Radloff, 1977) at the first and third time points. Future longitudinal research on depressive symptoms should use consistent measures to effectively follow the trajectory of symptoms over time.
The first time a question concerning diagnosis of an ASD appears in the ECLS-B questionnaires is at the third time point. No information is available concerning the possibility of diagnosis at the second (2 year old) time point, making it difficult to determine how long individual mothers and families have been coping with a diagnosis of ASD. Currently in the United States, the median age of diagnosis of ASD is 4 years (Center for Disease Control and Prevention, 2012) and given the data set is nationally representative, we suggest the majority of families are relatively new to the diagnosis at the third (4 year old) time point. Future research should examine the influence of time since diagnosis on levels of parent stress and depressive symptoms.
Conclusion
“Research has shown that the interactions of parents with their children with disabilities can have a profound impact on the progress that a child makes in his or her therapeutic or educational programs” (Lessenberry & Rehfeldt, 2004, p. 231). With that impact in mind, researchers have explored the factors that have contributed to the stress of raising children with ASD (e.g., Baker-Ericzen et al., 2005; Cassidy et al., 2008; Davis & Carter, 2008; Hastings et al., 2005; Hoffman et al., 2008). Cassidy and colleagues (2008) found the two most commonly mentioned impacts on family life were the stress and strain of parenting a young child with ASD and the social restrictions placed on the family. Multiple studies indicate that a child’s behavior does play a role in increasing maternal stress and depressive symptoms (Boyd, 2002; Cassidy et al., 2008; Hastings et al., 2005; Herring et al., 2006; Olsson & Hwang, 2001; Tomaniket al., 2004). In addition, the difficulties, and the associated stress, faced by mothers of children with ASD are universal and cross cultures (Dabrowska & Pisula, 2010).
While our study has focused on maternal stress and depressive symptoms when raising young children with ASD, it is important for future research to examine the roles fathers play in the function of families faced with this challenging disability. As Flippin and Crais (2011) noted in their review of the literature, fathers of children with ASD are underrepresented in research and early intervention. Furthermore, the research is mixed as to whether fathers of young children with ASD experience similar levels of stress to mothers (Davis & Carter, 2008; Hastings, 2003; Hastings et al., 2005) or lower levels of stress (Dabrowska & Pisula, 2010; Olsson & Hwang, 2001; Tehee et al., 2009). Yet when compared with fathers of typically developing children, fathers of young children with ASD experience significantly higher stress levels (Flippin & Crais, 2011). Clearly any family-focused intervention must account for the well-being of all parenting partners.
The higher levels of maternal stress and depressive symptoms at the first time point for mothers of children with ASD, when compared with mothers of typically developing children, may be indicative of concerns they are already experiencing related to their child’s development. Conversely, as suggested by Duarte and colleagues (2005), mothers of children with ASD may have innate factors that make them more prone to experience stress. By understanding maternal personality factors, family interventionists may gain a better understanding of maternal stress as they develop interventions for families of young children with ASD (Duarte et al., 2005).
Examining the influence of time since diagnosis on parenting behaviors is a direction for future research. With the current uncertainty of the cause(s) of ASD and the multiple treatment interventions available, parents are faced with a large quantity of information in the few months following diagnosis, as well as increases in stress levels. More longitudinal studies would allow researchers to view coping strategies used by parents over time. In addition, more comprehensive interviews of parents, including the use of focus groups (i.e., parents facing similar difficulties raising toddlers with ASD), would guide future practitioners on the resources and supports that families would like available to assist in their parenting a child with ASD.
As reported by Steiner, Koegel, Koegel, and Ence (2012), parent education is a universal element of interventions designed for young children with ASD, yet more work is needed to develop effective ways to conduct these sessions, particularly as new technology-based formats become available. Parent education, individualized to match specific family needs and empower parents with strategies to address challenges, has the potential of reducing parenting stress (Koegel et al., 2005; Steiner et al., 2012). While mothers spend the most time with their young children with ASD, when compared with service providers, the stress and strain of providing full-time intensive intervention (as in Applied Behavior Analysis [ABA] therapy) suggests that programs should not rely heavily on mothers at therapists (Schwichtenberg & Poehlmann, 2007).
Furthermore, the literature indicates that informal social support can have an impact on reducing stress in mothers of children with autism (e.g., Boyd, 2002; Ekas et al., 2010; Gill & Harris, 1991; Twoy, Connolly, & Novak, 2007). Herring and colleagues (2006) recommended that “an emphasis on providing early intervention for behaviour and emotional problems, along with additional support, education and skills training for parents, is justified” (p. 880) when addressing needs of families of young children with ASD. The importance of the immediate family in providing social support to its members when raising a child with ASD is repeatedly mentioned in the literature (Bristol, 1987; Dunn et al., 2001; Ekas et al., 2010), but more research is needed to determine the most effective informal social supports.
Identifying stressors associated with caring for young children with ASD is the first step toward designing interventions to reduce or eliminate factors that negatively affect family function and maternal well-being. In a bidirectional impact of identified stressors and maternal stress, “it seems reasonable to expect that the levels of stress a parent experiences may affect the frequency and quality of interactions with their child” (Lessenberry & Rehfeldt, 2004, p. 232). Future investigation should assess maternal well-being at all phases of an intervention program (e.g., before, during, and after) in an effort to provide empirical evidence of useful practices. Assessment of stress and depressive symptoms might reveal aspects of a mother’s relationship with her child, which are stress provoking. These areas can then become the focus of intervention research and development. Helping families cope with the stressful challenges of raising their young children with ASD would be a valuable target area for future intervention work.
Footnotes
Authors’ Note
Opinions reflect those of the authors and do not necessarily reflect those of the granting agencies (Office of Special Education Programs and IES).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a leadership grant from the Office of Special Education Programs (Project FOCAL, H325D070061) and an IES grant to B. McBride, R. Santos, S. Hong, and W. J. Dyer (R324A120174).