
Abstract
This study researched the predictive impact of developmental screening results and the effects of child and family characteristics on completion of referrals given for evaluation. Logistical and hierarchical logistic regression analyses were used to determine the significance of 10 independent variables on the predictor variable. The number of concerns was the most significant variable in predicting screening referral outcomes. Health concerns noted in child screening results were highly predictive of having no referral evaluation completed. Social-emotional concerns had a less striking but consistently negative relationship with referral completion. Speech-language delays and developmental concerns were not significant predictors. Being female and White were strong predictors of completed referrals. The findings have implications for the timing of referrals for children’s atypical screening results and underscore the importance of follow-up in developmental screening referrals made for children with multiple areas of concern and for those who have specific health concerns.
Children who have delays or atypical behaviors can benefit from participation in developmental screening programs to determine whether additional evaluation to establish eligibility for early intervention or educational services is needed. Developmental screening is the preliminary process for identifying areas of concern in young children (American Academy of Pediatrics [AAP], 2006). Recent research demonstrated an encouraging trend in the provision of screenings (Bruder, Dunst, & Morgo-Wilson, 2009; Kaye & May, 2009), as an increase in screenings has identified more children who need diagnostic evaluations and, subsequently, may become enrolled for appropriate services (Hallam, Rous, Grove, & Lo Bianco, 2009).
Although an earlier study found as little as 20% of clinicians screening as part of regular care routines and with the majority reporting a “wait and see” approach to developmental delays (King & Glascoe, 2003), a recent survey of pediatricians reported they assessed developmental risk in 96% of their patients under 3 years of age (Marks, Hix-Small, Clark, & Newman, 2009). The pediatricians in this survey study estimated 9% of children screened had a referral for evaluation or specialized services. More screening opportunities means more children can be identified and referred for diagnostic evaluations (Earle, Andrews, & Hay, 2009).
However, a meta-analysis of longitudinal research conducted on children who participated in developmental screening programs failed to document a direct link between the screenings and improved child outcomes (Nelson, Nygren, Walker, & Panaoscha, 2006). As reported to U.S. Preventive Services Task Force, Nelson and colleagues (2006) found insufficient evidence of any effects of wide-spread screening of young children for delays and suggested more studies on potential benefits of development screening. This lack of efficacy in developmental screenings for improved child performance levels may be due to shortcomings in the referral tracking process that results in children who need services lost to follow-up (King et al., 2010). A decade earlier, a cost-effectiveness study of developmental screening found long-term benefits of screening were only realized when they resulted in young children with delays receiving needed services earlier (Dobrez et al., 2001).
Referral completion tracking may be critical to the efficacy and cost-effectiveness of developmental screening, but seldom practiced. In developing a framework for the screening process, Dunst and colleagues asked whether referral tracking was even possible given numerous limitations of professionals, agencies, and families (Dunst, Trivette, Appl, & Bagnato, 2004). Although tracking referrals is a Child Find function of IDEA and is a recommended practice in developmental screening (AAP, 2006; King et al., 2010), referral follow-up is usually done on a case-by-case basis (Trivette & Dunst, 2006). Most programs report the lack of staff, funds, or authorization for reimbursement to coordinate referrals between screening programs and community agencies are barriers (Fagan & Montgomery, 2009).
In light of these shortcomings, one approach to maximize the effectiveness of referrals is to identify child and family characteristics that predict poor outcomes in referral completion 1 and focus on tracking children with these characteristics to be sure the child is evaluated for service eligibility (Giannoni & Kass, 2012). This can allow for more efficient use of limited resources while decreasing the number of children with developmental, behavioral, or health concerns lost to follow-up.
Very little has been published on completion of developmental screening referrals. Four studies of screening referral tracking that were located indicated significant numbers of referrals are not completed. One study found 52% of referred children completed their recommended evaluation (Schonwald, Huntington, Witt, Silver, & Cox, 2008), whereas Rushton, Bruckman, and Kellerher’s (2002) research on behavioral referrals in young children reported 61% of referrals were evaluated within 6 months of screening. A study by Meisels and Margolis (1988) of Medicaid Early and Periodic Screening, Diagnosis and Treatment (EPSDT) program determined 63% of children referred had received services. Another study of EPSDT referrals for speech-language by Richardson, Selby-Harrington, Krowchuk, Cross, and Williams (1994) concluded that 71% of referred children received recommended evaluations. This composite data indicates an estimated one half to one third of young children identified with developmental or behavioral concerns in screening are not receiving evaluations or services to address these problems.
What is missing in the body of information about developmental screening referrals is research into the increased use of electronic medical and educational records to track referred children post-screening, and guidance for conversations between screening providers and parents who have a child referred for evaluation. Research is needed about what is important in child screening results and child and family factors that can be related to referral completion.
This research project investigated how referral completion differs based on screening results and child and family characteristics. To understand how screening programs can support referral completion, these results and factors were examined for their predictive relationship to referral completion. Therefore, in this study, the following research questions were asked:
Research Question 1: Does the number of developmental domain concerns in child screening results predict referral completion?
Research Question 2: Do the developmental domains of concerns in child screening results predict referral completion?
Research Question 3: What selected child and family characteristics are related to screening referrals that are completed and those that are not?
Method
Design
An ex post facto design was used in this study. Child records from a community developmental screening program (2010–2011) were searched for records that met criteria for inclusion, that is, those records with child screening results which yielded a referral for evaluation of developmental concerns that could be tracked to the agency to which the child was referred. Children who were referred for diagnostic evaluations were classified by number of child concerns noted, types of concerns, and child and family characteristics. In child records with two or more referrals for the same child, each referral was tracked separately using child concerns and family characteristics as predictors for that individual referral completion.
Developmental Screening Program and Procedures
Research was conducted in an early childhood developmental screening program organized by a regional coalition of health, education, and social service agencies. This screening program serves children from birth to 5 years old who are not currently receiving special education, early intervention, or Head Start services. Screening days are scheduled twice a year in a community clinic site staffed by volunteer professionals who donate their time for that day. There is no cost to families or health insurance providers for screening.
The clinic rotates children and parents/guardians through a series of exam rooms with dentists, nurses, doctors, psychologists, speech-language therapists, social workers, and teachers. Each screening professional conducts specific assessments in one of seven developmental and health domains: language, overall development, social-emotional development, vision, hearing, growth, and dental. Results from all domains are entered into child records on a Developmental Screening Summary Form. When a professional finds questionable or atypical results in any developmental domain area, a recommendation for a diagnostic evaluation in that area is indicated on the form. The results of the screening are discussed with parents in each session during and after the specific testing, and then reviewed after completion of all areas with a trained family facilitator and if referred, with staff from the referral agency who is available on-site at the screening. The child’s doctor is sent a report of screening results and any referrals made from the screening. After clinic days, child records are kept by the regional agency for special education diagnostic and evaluation services, a partner in the regional coalition and who has lead responsibility for child find and assessment activities under IDEA.
Participants
Participants were children who attended a community developmental screening event within the 2-year period of the study. Parents of children were recruited to participate in the study as part of the intake procedure in the screening program registration. Parents who choose to participate agreed to the researcher’s use of information from their child’s screening records for a post hoc study. The consent form did not specify what information in the records would be studied. There were 133 children screened during the study period. Within this population, 84 children were identified as having areas of concern and received at least one referral for further evaluation. Of these children, 55 had more than one referral, with 125 referrals in the sample to track for completion. However, 9 child records that met criteria but did not have signed consent forms had to be excluded, leaving a total of 75 child records with 112 referrals for analysis.
The 112 children with referrals included 81 (72%) boys and 31 (28%) girls. The percent of referred children’s racial/ethnic backgrounds were (a) White (45%), (b) Black (34%), (c) Latino (11%), (d) biracial (7%), and (e) Asian (4%). Referred children who received Medicaid coverage (59%) were categorized with family incomes at or below federal poverty-level (FPL) socioeconomic status (SES) and children covered by private insurance (36%) were counted as above poverty-level SES. A small number (5%) had no health insurance.
The ages of children referred ranged from 18 months to 5 years. Most referrals were for children between ages of 3 and 4 years. The span of referred child ages was (a) 9% infants under 18 months (n = 1), (b) 9% toddlers between 19 and 24 months old (n = 10), (c) 18% toddlers between 25 and 30 months old (n = 20), (d) 10% preschoolers between 31 and 36 months old (n = 11), (e) 26% preschoolers between 37 and 42 months old (n = 29), (f) 5% preschoolers between 43 and 48 months (n = 6), (g) 16% preschoolers between 49 and 54 months (n = 18), (h) 3% preschoolers between 55 and 60 months (n = 3), and (i) 13% children above 5 years old (n = 14). Referrals grouped by child care experience were (a) 50% of referred children cared for in their home (n = 56), (b) 42% in a child care center (n = 47), (c) 5% in babysitter or child care provider’s home (n = 6), and (d) 3% no child care information given (n = 3).
Data Collection
Data were collected from child records in reviews using an Excel checklist of the identified data measures for the analysis with codes developed by the researchers. Each record included in the study had a subject number and a referral number assigned and recorded on a separate encrypted Excel file. Information from these records was entered into an encrypted Excel folder and verified by another researcher against the original child record. Information was collected from records approximately 60 days after a community developmental screening clinic was held.
Outcomes and Variables
Predictor or independent variables (all categorical variables) were the child’s screening summary results (type of concerns and number of concerns) and selected child and family characteristics (age, gender, race/ethnicity, SES, child care). The main outcome or dependent variable was the child referral outcome (dichotomous: completed or not completed).
Child Screening Summary Results
Developmental domain screening results were recorded for language, social-emotional, overall development, and health and growth. These areas of concern were based on child developmental screening recommendations from the AAP (2006).
Speech-language domain
Children’s preverbal and verbal skills and interactions were assessed by a speech-language pathologist using either the Rossetti Infant-Toddler Language Scale (Rossetti, 2006), Battelle Developmental Inventory-2 Screener (BDI-2 Screener; Newborg, 2004), or Preschool Language Scale–4 (PLS-4; Zimmerman, Steiner, & Pond, 2002). Speech-language concerns were coded as one area whether they were in expressive or receptive language or in both expressive and receptive language.
Social-emotional domain
Children’s social-emotional skills were screened by a clinical psychologist or social worker using the Ages & Stages Questionnaire: Social Emotional (ASQ: SE; Squires, Bricker, & Twombly, 2002). This instrument is a social-emotional screen developed for age span 6 months to 60 months (5 years). ASQ: SE is provided in English and Spanish language and has been tested as valid in both languages.
Overall development domain
Children’s global developmental progress (including motor, cognitive, language, self-help, and social development) were screened by early childhood teachers using instruments based on the age of the child. Children under 3 years of age were screened using the Ages & Stages Questionnaire–Third Edition (ASQ-3; Squires, Twombly, Bricker, & Potter, 2009) and preschool aged children were screened using the Developmental Indicators for the Assessment of Learning–Third Edition (DIAL-3; Mardell-Czudnowski & Goldenberg, 1998).
Health domain
Pediatricians check the children for poor or questionable results on vision and hearing, and nurses record height and weight >25th percentile based on the Centers for Disease Control and Prevention Growth Charts for Children by gender and age (Kuczmarski, Ogden, & Guo, 2002). All children were screened by dentists for decay and infection. Areas included in health concerns were based on screening exams in dental, growth, vision, and hearing, but were all coded as one area of concern.
Child and Family Characteristics
Child and family demographic information (age, gender, race/ethnicity, SES, child care) was collected from screening records using the program’s Telephone Pre-Screening form and Screening Registration Information form. Age and gender of each child and his or her ethnicity were categorized by birth date in 6-month intervals. Ethnic identification was recorded as what was verbally or in writing provided by the parent during registration for screening. Data on family SES were not included in the child record, so information on health insurance coverage was used as a proxy for family income, as Medicaid insurance status substituting for low SES has proven to be a valid indicator of family income (Liberatos, Link, & Kelsey, 1988). Children covered by Medicaid or without insurance were assumed to be below poverty level and those with private health insurance counted as above poverty level. This information came from the Community Child Screen Telephone Pre-Screening form based on parent or guardian report. Early care experience was recorded at registration for participation in the developmental screening program.
Child Referral Outcomes
Referral completion was determined by requesting follow-up information on children referred. Agencies receiving developmental referrals from the screenings were given a list of children referred to cross-check against their client database and asked to indicate whether this child had been evaluated or was in process of being evaluated. This measure was categorized as completed or not completed based on whether the child received evaluation services from the referral. Completed was defined as the child having been (a) evaluated for eligibility by the agency and was receiving services, (b) evaluated and eligible but the family declined services, (c) evaluated and determined not eligible, or (d) being scheduled for evaluation. Not completed was defined as the child not having an evaluation by the referral agency or no record of the child in the agency’s system.
Data Analysis
Ten predictor variables were considered in analysis with the outcome variable for each referred child record: age, gender, race/ethnicity, SES, experience with child care, speech-language concern, social-emotional concern, developmental concern, health concern, and number of concerns. Child referral outcome (completed or not completed) was the dependent variables in the analysis. Data were entered into an Excel spreadsheet and verified by another researcher against the original child record. Data entry errors were corrected. The statistical analysis program SPSS 19.0 was used for data analysis. Descriptive statistics, including frequencies percentages, were calculated and included a comparison of percentages of completed referrals with referrals not completed by screening results and child and family characteristics. Logistic regression analysis was conducted using all variables to determine which were significant in terms of predicting completion referral rates.
A correlation matrix was calculated to test for associations between the 10 categorical variables listed above as predictors or independent variables and the strength of relationships between them and the dependent variable. High correlations between several independent variables indicated a need to test for multicollinearity to determine whether any highly intercorrelating variables needed to be removed to achieve an accurate equation model for prediction. One variable from child screening results indicated a strong degree of correlation (<.60) with several predictor variables in the correlation matrix and was tested for colinearity. Results showed the variable “number of concerns” strongly significant in the colinearity tests for tolerance (.054, p > .10) and variance inflation factor (VIF; 18.365, p < .10). Therefore, this variable was removed from further data analysis in the equation model for referral completion to increase validity of the predictive significance of other independent variables.
A hierarchical logistic regression analysis was conducted to allow for an evaluation of the predictive effect of one group of independent variables, screening summary results, on the dependent outcome of referral completion, separate from other independent variables of child and family characteristics. The analysis was run with one variable excluded from the equation model (number of concerns). The standardized residuals were plotted and showed normal distribution.
Because the first two research questions focused on predictive abilities of screening summary results and the third question explored significance of child and family characteristics to the outcome of referral completion, a subsequent analysis was conducted where screening results (minus the number of concerns variable, removed for multicollinearity) were entered at the first block, and child and family characteristics were entered at the second block. Output from this analysis provided a model equation, model fit, classification of cases, and information about all variables used in the equation, including regression coefficients (B), significance (p), and odds ratio (B squared) with 95% confidence intervals.
Results
Descriptive statistics were conducted to determine frequencies for referral completion and all variables of interest. Data analyses identified number of children referred for evaluation services and proportion of elements in sampling.
Referral Completion
Variables of screening results and child and family characteristics were compared with data by referral completion information. Data analysis of referrals revealed 62.5% (n = 70) were categorized as completed, meaning agency data records showed the child received or was receiving recommended evaluation services, and 37.5% (n = 42) were not completed, meaning the child was not in agency data records or had not received evaluation services from them.
The percentage of completed referrals for a child with one area of concern, female, above 3 years old, White, or cared for in a sitter’s home were significantly larger than for children without these characteristics. Referral completion was least likely for boys, a child with four or more areas of concern, specific health concerns, less than 3 years old or staying at home with a family member. There was not a notable difference between SES levels in percentage of referral completion. Table 1 includes each independent variable by outcome of the predictor variable “referral completion.”
Summary of Referrals Completed by Variable (N = 112).
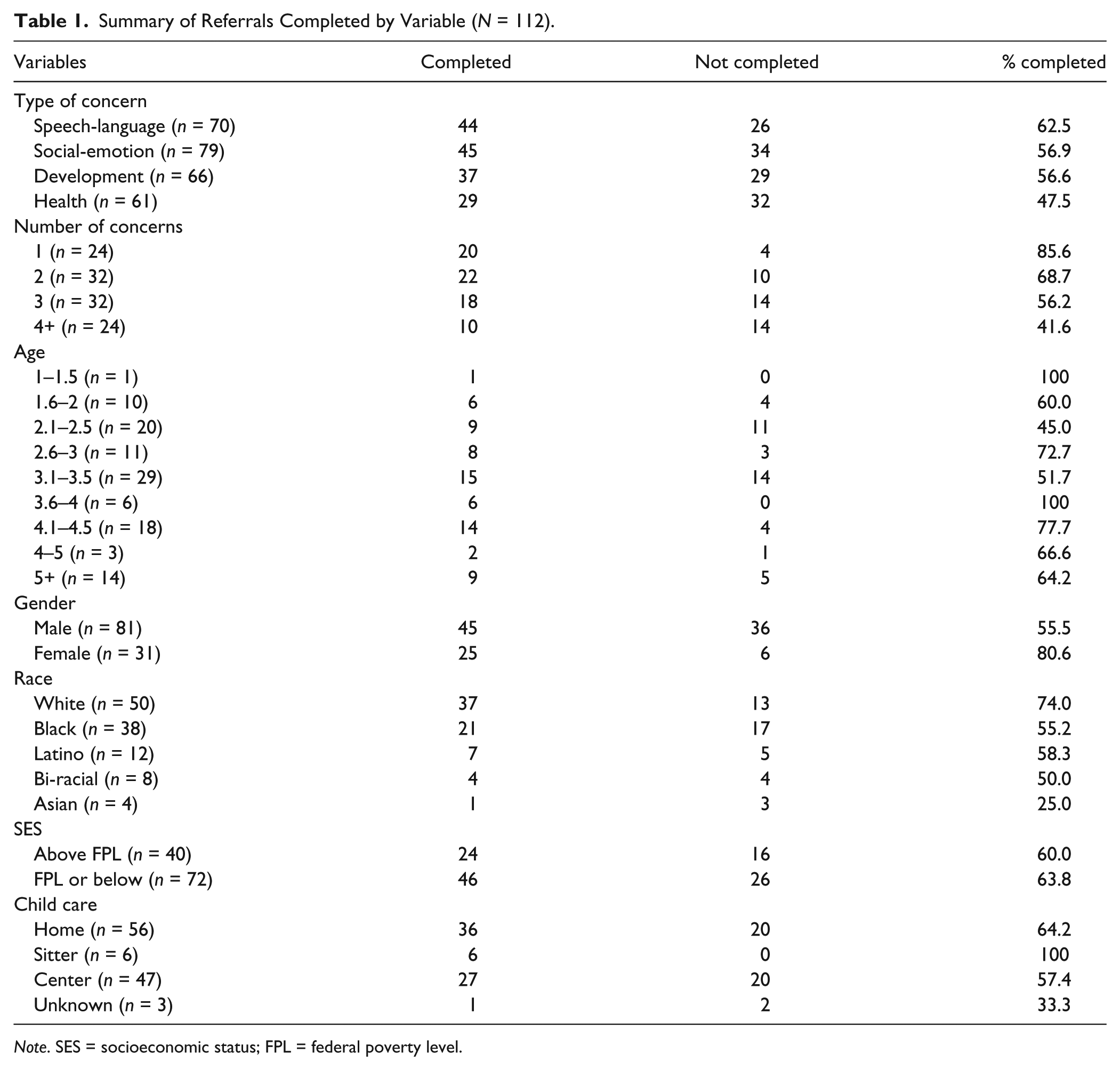
Note. SES = socioeconomic status; FPL = federal poverty level.
Predictors of Referral Completion
Logistic regression analysis between screening results and referral outcomes found the type of concern noted for the child related to a significant but negative influence whether or not they received evaluations. Children with social-emotional or health concerns were less likely to complete referrals than those with speech-language or developmental concerns. Completion varied dramatically by the number of concerns in screening results, with odds ratios decreasing as concerns increased. Table 2 gives the results of the regression coefficient, standard error, significance, and odds ratios. Variability in referral completion explained by independent variables from screening summary results ranged from 23% to 32% (Cox & Snell R2 = 2.36; Nagelkerke R2 = 3.32).
Screening Results Associated With Referral Completion.
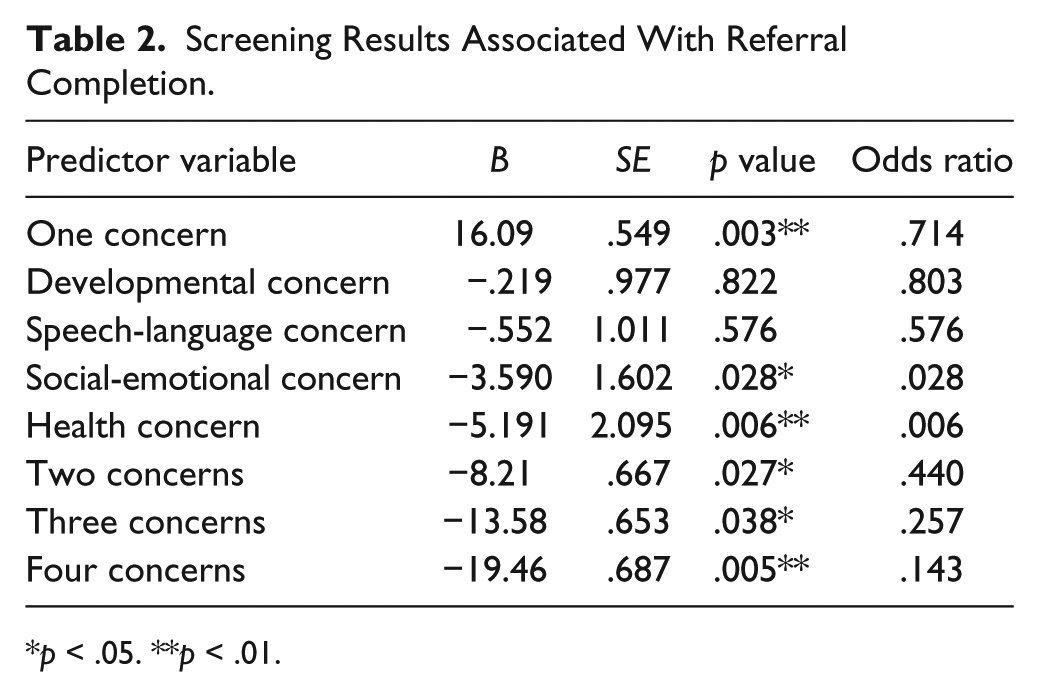
p < .05. **p < .01.
Areas of Concern
There were differences in percentages of referral completion shown across kinds of concerns noted. All area of concerns had negative regression coefficients, meaning the relationship of these variables to the outcome is about the relative likelihood of not completing a referral rather than predicting referral completion. Referred children with health concerns had six times the odds of not completing referrals compared with children who did not have health concerns noted in screening results. Children with social-emotional concerns or overall developmental concerns were two times less likely to complete referrals than those without these areas of concern noted on screening results.
Number of Concerns
The number of concerns was eliminated from the regression analysis due to high risk of multicollinearity with other predictor variables. Number of concerns was identified in the correlational matrix having high correlation with developmental concerns (R = .621, p < .01), health concerns (R = .605, p < .01), social-emotional concerns (R = .437, p < .01), speech-language concerns (R = .368, p < .01), gender (R = −.249, p < .01), day care (R = −.289, p < .01), and referral completion (R = .251, p < .01). Multicollinearity tests conducted found the variable “number of concerns” very significant in tests for tolerance and variance inflation factor and contributed an imbalanced weight in analysis with other data.
Child and Family Characteristics
Logistic regression analysis was conducted using all child and family characteristics added to variables from screening results, except the variable “number of concerns” removed for multicollinearity. Table 3 indicates several characteristics had predictive significance at .01. This significance is positive and negative; female gender and above poverty-level SES were significant predictors of referral completion. However, non-White race, below poverty-level SES, and the presence of health concerns or social-emotional concerns was predictive of not completing referrals.
Predictor Variables Related to Referral Completion.
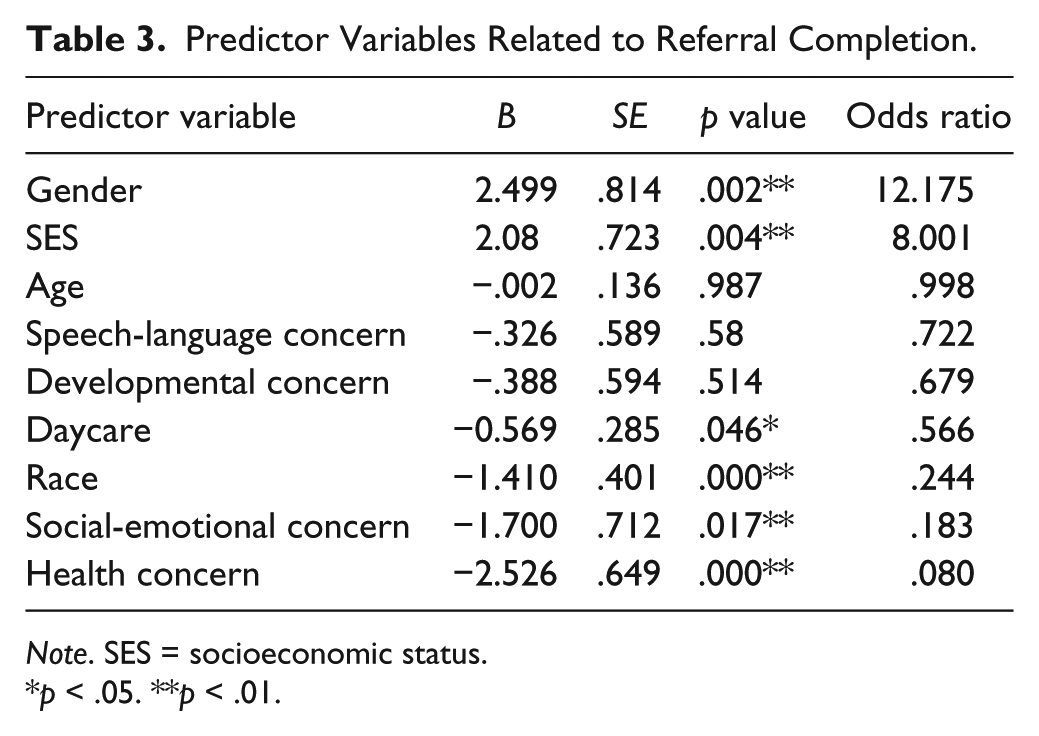
Note. SES = socioeconomic status.
p < .05. **p < .01.
To examine the effect of child and family factors on prediction of referral completion, hierarchical logistic regression was conducted using first, screening results alone, and second, screening results with child characteristics added to determine the R2 variability in the two equation models. Table 4 presents the change to R2 value and degree of significance to the first block of predictor variables “areas of concern,” when the second block “child and family characteristics” are included in the regression model equation. The R2 variability using only screening summary results ranged from 23% to 32% of referral completion explained by these predictor variables. The addition of Block 2 child characteristics increased the R2 up to 55% of variance in referral completion explained. The model including all predictive variables more accurately predicted referral completion than a model based on child screening results alone. The addition of child and family factors slightly decreased the regression coefficient for health concerns as a predictor but increased the coefficient of social-emotional concerns as a predictor.
Change in Significance of Predictors Between Block 1 and Block 2.
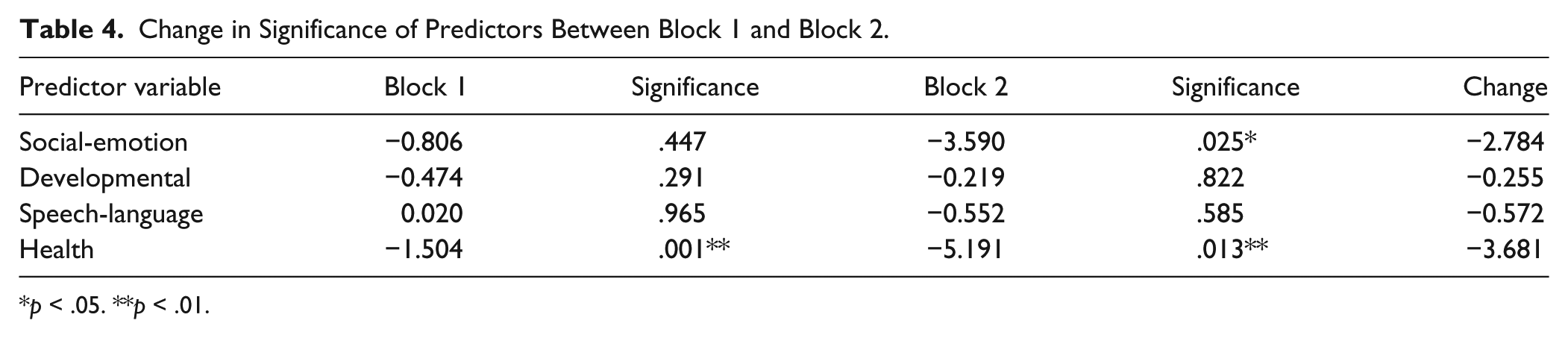
p < .05. **p < .01.
Results can be summarized as (a) the number of concerns was correlated with all predictor variables for referral completion and, with each increase in the number of concerns noted, the percentage of referrals completed decreased; (b) children with health concerns were less likely to complete referrals; (c) children with social-emotional concerns were less likely to complete referrals; (d) girls were 12 times more likely than boys to complete referrals; (e) White children were more likely to complete referrals than children of other races or ethnicities; (f) a child with higher SES was 8 times more likely to complete their referral than a child with SES at or below FPL; (g) children cared for at home were less likely to complete a referral than those in other settings; (h) children with their early care and education provided by a home care provider or babysitter were more likely to complete referrals than those in other settings; and (i) age of child, speech-language concerns, and overall developmental concerns were not predictors of referral completion in this sample.
Discussion
The purpose of this study was to determine what family and child factors predict referral completion for young children who were given referrals to community service delivery agencies from a developmental screening program. Data collected from 75 child screening records with a combined number of 112 referrals for diagnostic evaluations were analyzed for predictive ability. Results from this research are based on a small group of young children who participated in one kind of a developmental screening program in a mid-size community with limited resources available for diagnostic services. Given these sampling parameters, it is encouraging the majority of children (62.5%) with screening referrals received evaluation services. The percentage of completed referrals for evaluations is within range established in literature (52%–73%). However, in this study, referral completion was more than an outcome measure—It was used as a dependent variable to calculate the predictive values of child screen results and family characteristics on this outcome.
Variables Predicting Referral Completion
Although removed from the logistic model summary due to multicollinearity, the number of concerns was strongly correlated with referral completion, but with an inverse relationship. That is, as the number of concerns increased, the completion of referrals decreased. This is consistent with published studies finding a greater number of health and developmental concerns is not indicative of receiving more services (Pizur-Barnekow et al., 2010). However, research done with pediatricians found multiple areas of concern was a critical factor in deciding to make a referral for evaluation (Earle et al., 2009). This phenomenon may be seen as a vicious cycle where children with a single concern and possibly a higher probability of referral completion are not as likely to be recommended for evaluation as children with more complex concerns and who are less likely to complete diagnostic referrals. The “wait and see” approach of providers reported in research (e.g., King & Glascoe, 2003) may unwittingly contribute to missed opportunities for early intervention before delays or behaviors become compounded.
Children with health concerns noted at screening were six times less likely to complete a referral than children without health concerns, which is very important because 55% of child screens had health concerns noted. One study of children referred for early intervention services found no significant differences in participation in services between groups based on reason for referral (Malone & Gallagher, 2008), but others have found significance between developmental delay concerns and referrals (Cox, Huntington, Saada, Epee-Bounya, & Schonwald, 2010).
The third most significant factor in referral completion was race and ethnicity. White children were three times more likely to have completed referrals than Black, Latino, or biracial children. Black children were overrepresented in the referral sample when compared with census data, but underrepresented in referral completion. Research has documented disproportional numbers of developmental referrals for children from culturally diverse racial or ethnic families (Wanless, McClelland, Tominey, & Acock, 2011) but also decreased rates of referrals related to cultural and language differences (Earle et al., 2009).
Being female was significantly related to referral completion in this study. The finding adds to information on the influence of gender as a factor, as previous research has found boys were more likely to receive follow-up evaluations than girls (Schonwald et al., 2008). Other research found gender was not significant in percent of referrals given (Hallam et al., 2009). It is possible gender may not be a reliable factor in predicting referral completion because of the higher ratio of boys to girls receiving screening referrals (Earle et al., 2009).
Children in families with SES above poverty level were eight times more likely to receive evaluations than children in families with low SES. This finding is similar to recent studies identifying low SES and family instability as predictors in screening and in referrals to community agencies (Glascoe & Leew, 2010). Low SES is an established risk factor for increased developmental concerns and number of referrals than for children in higher income families (Mann, McCartney, & Park, 2007). A study of parents as participants in preschool health and educational services found lowest rates of participation among children from low-income families, even when services were free (Arcia, Keyes, Gallagher, & Herrick, 1993). The relationship between SES and referral completion in this research replicates other studies, but also indicates the complexity of this variable, as SES reliably and strongly correlates with other predictor variables such as number of concerns, health concerns, child gender, and race.
Children with social-emotional concerns were less likely to complete referrals for evaluation than children without this concern. This expands existing research findings that children with social-emotional concerns are less likely to receive referrals from providers than children with motor or speech concerns (Sices, Feudtner, McLaughlin, Drotar, & Williams, 2003). These results suggest identification of children’s challenging behaviors or atypical responses are difficult for parents in responding to referrals, perhaps because they feel personal responsibility for this kind of concern or they anticipate judgmental reactions from professionals. It might be that, like screening providers, parents are not sure what resources are available or what is effective for their child’s behavior problems (Malone & Gallagher, 2008).
Limitations
A number of limitations existed within this study. The greatest limitations were in the sample. The small size means interesting findings about referral completion do not allow for generalization. Furthermore, it was not representative of the larger population of young children screened, as these families intentionally registered for and attended a community screening event targeted for parents who had concerns for their child’s development. A third limitation for generalization is the time frame; the records reviewed were from 18 months of the first 24 months at the start of the program and the referral follow-up procedures could be changed through time and process of volunteers. Another limitation was the use of agency self-report for child referral completion data. The referral agency data collection were conducted and coded by the researcher and re-coded by another researcher to enhance the validity of the results. However, this does not replace having information from parents as confirmation of referral completion information provided by the evaluating agency. A parent survey or focus group post-event added as a component to this study would help clarify and expand understanding of referral completion variables.
Implications for Practice
If we are only interested in the results of child developmental screenings, the hierarchical perspective of this research into referral completion can be ignored, and we will continue practicing with conventional, but ineffective, referral models. However, this study offers hope for producing different results from screening referrals by focusing on child and family characteristics as well as specific assessment concerns which increase the chances for referred children to miss follow-up services. Identification of child and family characteristics that predict referral completion is a step toward making needed changes in screening programs’ referral process to track young children evaluated for services following screening. The AAP recently published a technical report regarding the lifelong effects of disadvantage and adversity in the lives of young children (Shonkoff, Garner, & Committee on Psychosocial Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care, and Section on Developmental and Behavioral Pediatrics, 2012) and called for an increased awareness of children at risk of developmental disorders and for the need to follow-up and intervene early.
A recent research synthesis of developmental screening instruments made the point that, given the importance of the screening results in helping parents address concerns for their children, it is imperative screening results are valid and reliable (Macy, 2012). This study found having one area of concern was positively related to referral completion. Utilizing reliable and valid screening measures and evidence-based practices could raise providers’ confidence to identify and refer children earlier for a single area of delay. In turn, families would be more likely to complete their referral rather than waiting for additional areas of concern to develop.
Summary
Developmental screening providers must follow up on referrals made to ensure children get the benefits from evaluations and services recommended. This study found a substantial proportion of children who did not access referral services were those with the highest number of developmental concerns noted in their screenings. Because referral completion occurs in the context of young children’s family systems and community environments, the development of linkages between families and service providers to obtain their recommended evaluations and services are critical. The developmental needs of young children with delays or atypical behaviors are often greater than what a family alone can address.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.