
Abstract
This multiple baseline design study examined the effects of a Tier 3 early literacy intervention on low-income preschool children’s phonological awareness (PA). Seven preschool children who did not make progress on identifying first sounds in words during a previous Tier 2 intervention participated in a more intensive Tier 3 intervention. Children listened to stories and participated in early literacy activities led by an interventionist for approximately 15 min, 3 to 4 days per week for up to 8 weeks. Weekly progress monitoring data showed that five of seven children made progress on first sound identification as a result of the Tier 3 intervention. Children who made progress on first sound identification generally demonstrated gains on more distal measures of PA. Results demonstrate the potential benefit of providing children with multiple tiers of instruction to facilitate academic success.
Keywords
Considering the salience of language and literacy in our society, learning to read may be the most important achievement in children’s lives. Among U.S. fourth-grade students, only 34% read at the proficient level or above (National Center for Education Statistics, 2011), indicating that this critical achievement is not always easily acquired. There is perhaps no greater risk factor for reading difficulty than living in poverty. Preschool children from low socioeconomic status (SES) families are less prepared for formal reading instruction than children from middle and high SES families (Lonigan, Burgess, Anthony, & Barker, 1998; Roseberry-McKibbin, 2008). Insufficient preparation through rich language and literacy experiences in the home often sets young children on a trajectory toward reading failure (Bracken & Fischel, 2008; Hart & Risley, 1995).
Due to widespread recognition that early intervention has the greatest potential to compensate for the damaging effects of poverty (Bus & Van Ijzendoorn, 1999; Justice, 2006; Vellutino, Scanlon, Small, & Fanuele, 2006), many children from low-income backgrounds qualify for early childhood education such as Head Start and income-based prekindergarten. The development of reading skills can be enhanced in early childhood education programs if emergent literacy skills are taught. An extensive literature documents relations between emergent literacy skills of 4- and 5-year-old children and future reading success (Justice, Chow, Capellini, Flanigan & Colton, 2003; Lonigan, Schatschneider, & Westberg, 2008; Missall, McConnell, & Cadigan, 2006; National Early Literacy Panel [NELP], 2008; Roseberry-McKibbin, 2008; Storch & Whitehurst, 2002).
Of the major emergent literacy skills, phonological awareness (PA) is most strongly related to future reading (Adams, 1990; Ezell & Justice, 2005; Lonigan et al., 1998; NELP, 2008). PA refers to children’s ability to attend to the auditory aspects of language, without attending to meaning (Koutsoftas, Harmon, & Gray, 2009; Trehearne, Williams, & Moore, 2003). PA involves a metalinguistic understanding of the structure of oral language, including the ability to recognize and manipulate parts of oral language, that is, sentences, words, syllables, and phonemes (Adams, 1990). In preschool, instruction in this domain typically consists of such skills as rhyming, blending, segmenting, and first sound identification. Trehearne and colleagues (2003) found that having adequate PA skills at the time of school entry gives children an advantage in learning to read. Thus, concentrated efforts to develop PA in preschool can enhance school readiness (Carlton & Winsler, 1999; Justice & Kaderavek, 2004).
Although some emergent literacy skills may be learned implicitly through repeated exposure to books (e.g., print knowledge), PA typically requires deliberate, explicit instruction (Justice et al., 2003; Petursdottir et al., 2009; Phillips, Clancy-Manchetti, & Lonigan, 2008; Stahl & Murran, 1994). Instruction should include features such as multiple opportunities to respond with a variety of examples (Gardner, 1999; Merrill, Tennyson, & Posey, 1992; Perkins & Unger, 1999), careful modeling and scaffolding (Archer & Hughes, 2011; Johnson, 1998), and response-dependent (i.e., contingent) feedback (Andre, 1997; Gagné, 1985).
Despite attendance in preschool and the potential of emergent literacy skills to build a foundation for reading, many children do not receive sufficient emergent literacy instruction early enough. In a recent survey of early childhood education programs (Greenwood et al., 2011), school administrators indicated that a lack of evidence-based instruction in the classroom is a major concern. Furthermore, the What Works Clearinghouse found that less than 10% of the preschool curricula they evaluated showed strong positive effects on literacy outcomes. This may be due to insufficient emergent literacy content in most early childhood curricula. Some curricula teach skills related to emergent literacy but lack explicit PA instruction. Children living in poverty often are disadvantaged because of poor literacy opportunities at home as well as limited instruction on PA in preschool.
Response to Intervention (RtI)
RtI is a differentiated instruction and problem-solving process that uses increasingly intensive teaching conditions and ongoing assessments aimed at providing effective instruction to all children (Fuchs & Fuchs, 2006; Fuchs, Mock, Morgan, & Young, 2003; Gettinger & Stoiber, 2008). RtI is an educational tool and philosophical perspective that promotes children’s individual response to high-quality instruction within a context that seeks to determine when children need supplemental instruction. An RtI framework only recently has been extended to early childhood education as a means of promoting early literacy development (Greenwood et al., 2011; VanDerHeyden & Snyder, 2006).
Although models of RtI vary, levels of instruction most often are organized into at least three tiers, each increasing in intensity (Fletcher & Vaughn, 2009). Tier 1 refers to the everyday core instruction that all children receive from their classroom teacher. This involves classroom-wide teaching procedures using curricula designed to foster multiple domains of child development and meet early childhood learning standards (Coleman, Buysse, & Neitzel, 2006; Fox, Carta, Strain, Dunlap, & Hemmeter, 2010). Universal screening in curriculum-relevant domains for all children is a key feature of Tier 1 instruction. Based on universal screening or progress monitoring results, children who perform below expectations or who show minimal progress qualify for additional instruction. These Tier 2 interventions typically supplement Tier 1 instruction and are characterized by instructional arrangements with smaller groups, more frequent or longer lessons, more prompting, and more opportunities to respond. Regular assessment is continued with children who receive Tier 2 intervention so that their progress and response (or lack thereof) can be monitored. Children who continue to struggle may warrant a Tier 3 intervention designed to be the most intensive instruction in a three-tiered model. Tier 3 interventions typically feature more frequent and longer small-group or individualized sessions. The focus may be restricted to essential academic targets. The instruction is likely to be more teacher-directed and explicit, and involves contingent feedback and systematic prompting and fading procedures (Berkeley, Bender, Peaster, & Saunders, 2009; Bursuck & Blanks, 2010).
Previous PA Interventions
A number of empirical studies of PA interventions have been conducted that seem applicable to RtI systems in early childhood education. For example, van Kleeck, Gillam, and McFadden (1998) evaluated the effects of PA training with two classrooms of eight preschool children diagnosed with communication disorders. Activities used to promote phoneme awareness included modeling, judging and correctly identifying initial sounds, and matching initial sounds and used simple games with puppets and pictures. A series of rhyming and phoneme awareness pre- and posttest measures indicated that participants demonstrated gains in rhyming and phoneme awareness skills. When participants were compared with an older group of children (graduates of the preschool classrooms), participants in the treatment groups demonstrated phoneme awareness skills at post-test significantly above the comparison group. However, the participants’ rhyming posttest scores fell well below the mean of the comparison group, suggesting that the intervention was not responsible for the observed gains in rhyming.
Ziolkowski and Goldstein (2008) demonstrated learning of rhyming and initial sound identification in 15 children with language delays using a single-case experimental design. O’Connor, Jenkins, Leicester, and Slocum (1993) assigned 47 preschoolers with developmental delays and low PA scores to a control group or to one of three treatment groups that focused on rhyming, blending, or segmenting. After 7 weeks of treatment, children showed improvements on researcher-developed measures for the targeted skills, but showed limited generalization to unfamiliar words or to other PA skills.
Justice et al. (2003) implemented an emergent literacy intervention for 6 weeks with 18 preschool children. Two conditions (explicit instruction vs. shared book reading) were compared. Results indicated significant growth from pre-test to post-test on all five measures (i.e., alphabet knowledge, print awareness, name writing, phonological segmentation, and rhyme production) for the explicit instruction group. Improvement was shown only for phonological segmentation for the comparison group.
Larger scale studies focused on classrooms of children and did not select children based on PA skill deficits. For example, Byrne and Fielding-Barnsley (1991) randomly assigned 126 preschoolers to either a 12-week, small-group intervention (Sound Foundations) or to a control group. Children in the treatment group outperformed children in the control group on a researcher-developed measure of phoneme-identity (e.g., identifying which picture started with the same sound as a target). Nancollis, Lawrie, and Dodd (2005) compared a PA training program with 99 preschoolers to a control group (n = 114). Intervention focused on promoting syllable, rhyme, and initial phoneme discriminations. The treatment group demonstrated significantly greater improvements from pre- to post-test on rhyme awareness, nonword spelling, and phoneme segmentation compared with the control group. Children who participated in the intervention demonstrated improved rhyming skills 2 years post-intervention compared with control peers. Despite these studies’ positive outcomes, the application to an RtI model is limited because the participants were not identified as having early literacy deficits prior to the treatment.
In addition to the studies described above, many other researchers have demonstrated various levels of success in teaching PA skills (Blachman, Tangel, Ball, Black, & McGraw, 1999; Gillon, 2000; Laing & Espeland, 2005; Whitehurst et al., 1999). However, previous interventions often did not provide multiple tiers of instructional intensity and frequency based on children’s needs. Some studies were conducted with preschoolers who might be considered Tier 1 candidates as they were not selected because of delays in PA skill development (e.g., Bowyer-Crane et al., 2008; Byrne & Fielding-Barnsley, 1991) and often were conducted in a large-group (whole class) setting (e.g., Lefebvre, Trudeau, & Sutton, 2011; Massetti, 2009). Other interventions might be considered “low-intensity” classroom interventions (Laing & Espeland, 2005), often conducted only 1 or 2 days per week (e.g., Gillon, 2000; Koutsoftas et al., 2009; Nancollis et al., 2005). However, interventions conducted by trained professionals (e.g., speech-language pathologists [SLPs]; Nancollis et al., 2005), involving lengthy daily sessions (Justice et al., 2003; Roth, Troia, Worthington, & Dow, 2002), or extending for many weeks (e.g., 24 weeks; van Kleeck et al., 1998), may not be feasible in many preschool settings. Although these interventions certainly benefit many children, they are not sufficient for other children who may respond to a more intense, Tier 3 intervention.
Purpose
Despite the promise of PA interventions in early childhood, the bulk of the interventions investigated are most consistent with Tier 1 or Tier 2 arrangements. Although such interventions have produced favorable results and may be economically prudent, they are insufficient for some children. There is little known about explicit, individually tailored interventions that may be needed for children requiring a higher tier of instruction. Given the essence of the RtI philosophy, the field needs to develop effective instruction that meets the needs of all children, especially those at greatest risk for developing reading problems. In particular, children from low SES backgrounds and children for whom previous intervention has been unsuccessful deserve empirically supported interventions that address their needs.
Hence, the purpose of the present study was to examine the effect of a Tier 3 PA intervention on the emergent literacy of preschool children from low-income backgrounds who did not make assessment gains following a less intense Tier 2 intervention. The current Tier 3 intervention was designed to include many elements of PA instruction identified in the literature, such as instruction at the phoneme level (Lundberg, Frost, & Petersen, 1988; Nancollis et al., 2005; van Kleeck et al., 1998); direct, explicit teaching procedures (Ayres, 1995; Justice et al., 2003); combining PA instruction with instruction on alphabet knowledge (Justice et al., 2003); and inclusion of manipulative, engaging materials (Cunningham, 1990; Gillon & Dodd, 1995). In contrast to participants’ experience with a Tier 2 intervention with prerecorded lessons delivered to small groups of preschoolers, this intervention included a live interventionist and feedback that were contingent on individual responses. It was hypothesized that this carefully constructed Tier 3 intervention would result in improvements in emergent literacy skills for a group of struggling children. Specific research questions included the following:
Method
Participants
Participants attended public preschool in a large urban district in the Midwest. The preschool classrooms served primarily children at risk of academic failure due to low income. Children attended full-day preschool 5 days a week. Children with identified disabilities were not served in these classrooms. Preschool teachers held valid early childhood teaching certificates. They used the district-adopted Harcourt Storytown curriculum. This is a comprehensive literacy curriculum that includes PA instruction throughout the school year. Thus, children were expected to receive a fair amount of PA instruction during Tier 1 instruction.
All children in each class participated in the comprehensive curriculum. Following classroom-wide screening in fall of the academic year, children with relatively low PA scores participated in a small-group Tier 2 PA intervention. This intervention was more intense than the classroom curriculum because it took place in a separate location with fewer children, focused on key PA skills (e.g., blending, segmenting, first sound identification), and provided frequent opportunities to respond. Interactive PA lessons were embedded within prerecorded book readings. Children listened to stories and participated in the interactive lessons with supervision of an adult who provided encouragement, but not contingent reinforcement. Following 8 weeks of supplemental PA intervention, children who did not make meaningful gains on the primary dependent measure, First Sound Fluency (FSF; Good & Kaminski, 2002) were eligible to participate in the present study.
Immediately prior to the start of the present study, children’s PA skills were reassessed to confirm that they continued to need intervention. Children were administered FSF once a day over 3 days (first 3 days of baseline data). Because identification of initial sounds in words was the primary outcome of interest, any child who had consistently scored above 5 on FSF was excluded. Consistent scores above five would indicate a child has some degree of ability to perform the task. Some children occasionally scored between 1 and 5 points by responding with the same sound for each item (i.e., saying the /s/ sound repeatedly, some of which were correct by chance). All children who were screened for the present study qualified to participate in the Tier 3 PA intervention.
Seven children (three boys, four girls) attending three different preschool classrooms qualified for inclusion. Children’s ages ranged from 52 to 60 months at the start of the study (M = 55.9 months, SD = 2.9). Five children were African American and two were Caucasian. Descriptive data, obtained using family surveys and standardized norm-referenced instruments, are presented in Table 1.
Family Survey and Descriptive Data.
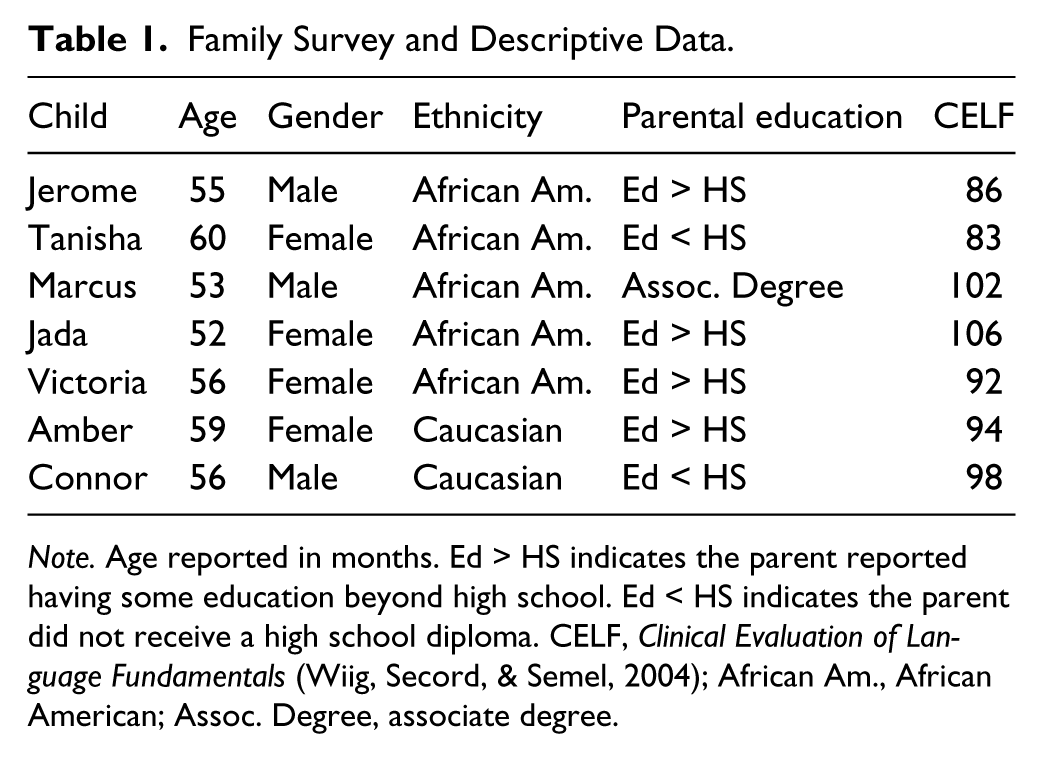
Note. Age reported in months. Ed > HS indicates the parent reported having some education beyond high school. Ed < HS indicates the parent did not receive a high school diploma. CELF, Clinical Evaluation of Language Fundamentals (Wiig, Secord, & Semel, 2004); African Am., African American; Assoc. Degree, associate degree.
Setting
All testing and intervention sessions took place in a room or hallway near the children’s classrooms. Location of the intervention was dependent upon available space in the school. On occasion, distractions occurred (e.g., children walking in the hall). In such cases, the interventionist redirected the students to the task as soon as possible. Children were taken from the classroom to the nearby, designated area for daily sessions. Children were not removed during large group or circle time because the majority of explicit language and literacy instruction by the classroom teacher was scheduled to occur during these activities.
Experimental Design
We implemented a multiple baseline design across groups of children (2–3 participants in each group) to examine the effects of the Tier 3 PA intervention on first sound identification. The design included three phases. During the baseline phase, children were tested in a multiple probe fashion to avoid testing fatigue and reduce unresponsiveness due to repeated testing of absent skills. One testing session was eliminated after the first two to three sessions for the group that began treatment first. For the remaining groups, two testing sessions were eliminated; the first eliminated session came after the first three sessions, and the second eliminated session came immediately prior to the final two baseline sessions. Throughout the 2- to 3-week baseline phase, children participated in a minimum of five testing sessions while receiving only Tier 1 classroom instruction. During the initial treatment phase, instruction focused on blending and segmenting (four testing sessions). During the second treatment phase, instruction focused on initial sounds. Staggered entrance of groups into the treatment phase was based on stability of probed baseline data. Once the treatment phase began, FSF was administered after every third intervention session. The schedule for testing was approximately weekly.
Dependent Variables
PA is a metalinguistic ability that includes a variety of skills. Blending, segmenting, and manipulation of phonemes are often considered most critical for literacy development (Gillon, 2005; Schuele & Boudreau, 2008). Adequate identification of initial sounds in words is a common indicator of readiness to read (Gillon, 2005) and was selected as our primary outcome. Blending and segmenting word parts and sounds are earlier developing skills and were included in the intervention to provide children with sufficient practice manipulating words prior to isolating the first sounds in words.
Three types of measures were used in this study: proximal, distal, and descriptive. A proximal measure (that assesses specific skills taught in the intervention) was used to answer Research Question 1. Distal measures that assessed skills related to the intervention, but that were not directly taught, were used to answer Research Question 2. One descriptive measure was used to assess language ability.
Proximal measure
FSF is a 1-min timed measure that required children to produce the first sounds of words. To administer this test, the examiner introduced the task, provided orally presented words (without pictures), and asked the child to provide the first sounds (e.g., “I will say a word, you tell me the first sound . . . can . . . wave . . . etc.”). There are multiple versions of the measure designed according to curriculum-based measurement conventions (Deno, 2003), so that repetition of forms can be avoided. Children earned 2 points for providing the initial phoneme (e.g., /k/ for cat) and 1 point for providing the initial blend (/ka/ for cat) of a word. The number of points accumulated in 1 min determined children’s total scores. Alternate-form reliability was reported at r = .82 with a sample of preschoolers. Furthermore, FSF showed medium to large correlations with another measure of initial sounds, Initial Sound Fluency, with correlations ranging from .30 to .62 (Cummings, Kaminski, Good, & O’Neil, 2011). The cut-point for high risk is 4 or below and the benchmark goal is 10 or above for the beginning of kindergarten (Dynamic Measurement Group, 2010).
To calculate scoring reliability for FSF, 20% of all assessments (from baseline and treatment) were randomly selected and scored by an independent scorer. As all assessments were audio recorded, secondary scoring was completed by listening to the audio files. Interobserver agreement (IOA) was calculated on an item level by taking the total number of agreements divided by the total number of agreements plus disagreements, multiplied by 100. An agreement occurred when both scorers recorded the same score for an item (e.g., 0, 1, or 2), and a disagreement occurred when the scorers did not record the same score for an item. Mean IOA was 97% for FSF.
Distal measures
Distal measures were administered before and after the intervention as a means of measuring generalization of treatment effects. These included the Print Knowledge (PK) and Phonological Awareness (PA) subtests of the Test of Preschool Early Literacy (TOPEL; Lonigan, Wagner, Torgesen, & Rashotte, 2007), Rhyming Individual Growth and Development Indicator (IGDI), First Sounds IGDI, Sound Identification (ID) IGDI (McConnell, Bradfield, & Wackerle-Hollman, in press), and Word Parts Fluency (WPF; Kaminski & Powell-Smith, 2011).
TOPEL
The TOPEL (Lonigan et al., 2007) was a standardized measure of PK, vocabulary, and PA designed to identify children at risk for early literacy problems. Low standard scores (below 90) for each subtest serve as general indicators of reading-related literacy problems. For the present study, only the PK and PA subtests were administered; internal consistency was high (α = .93 for PK and α = .86 for PA). The PK subtest consists of items related to knowledge about letter names, letter–sound correspondence, and the use of print in text. The PA subtest consists of items measuring blending (e.g., What word do these make: horse–shoe; What word do these make: /b/ all?) and elision (e.g., Say horseshoe without shoe; Say bike without /k/.) with compound words and one-syllable words. Alpha reliability coefficients for the TOPEL ranged from .87 to .96. Criterion validity estimates ranged from .59 to .77.
Rhyming IGDI
The Rhyming IGDI 2.0 consisted of 15 items that required the child to identify pairs of rhyming words on stimulus cards. Each card contained three pictures (one picture on top, two pictures on the bottom). The examiner pointed to and named the pictures and asked the child to select the pair that rhymes on each card. For example: “Bees, cat, cheese. Which two rhyme? Is it bees, cat or bees, cheese?” The Rhyming IGDI was untimed and had a maximum score of 15. The reported estimate of internal consistency based on congeneric reliability was 0.90 (Bradfield, McConnell, Rodriguez, & Wackerle-Hollman, 2013). Concurrent construct-related validity correlation with the TOPEL-PA was .49.
First Sounds IGDI
The First Sounds IGDI consisted of 15 items that required a child to identify which picture, of two, on the stimulus card begins with a target sound. The examiner pointed to and named both pictures, then asked the child to identify the correct word or point to the correct picture. For example, “Duck, cat. Which one starts with /k/?” The First Sounds IGDI was untimed and had a maximum score of 15. The reported estimate of internal consistency based on congeneric reliability was 0.76 (Bradfield et al., 2013). Concurrent construct-related validity correlation with the TOPEL-PA was 0.61.
Sound ID IGDI
The Sound ID IGDI consisted of 15 items on stimulus cards. Each card had three printed letters, presented in one row in the middle of the card. The examiner pointed to the letters and asks the child to identify the letter that makes the target sound. For example, “Look at these letters. Which one makes the sound /f/?” The Sound ID IGDI is untimed and had a maximum score of 15. The reported estimate of internal consistency based on congeneric reliability was 0.81 (Bradfield et al., 2013). Concurrent construct-related validity correlation with the TOPEL-PA was .71.
WPF
WPF (under development at Dynamic Measurement Group) was a 1-min timed task designed for preschoolers that required children to produce the first parts of words. Following sample items, children received the following instructions: “I will say some more words. You tell me the first part of the word.” Then words were presented orally to children for 1 min. Children earned one point for producing the first syllable, blend, or phoneme of words (e.g., /peng/, /pe/, or /p/ for penguin).
Descriptive measure: Clinical Evaluation of Language Fundamentals Preschool–2nd Edition (CELF Preschool-2)
To assess children’s language ability, the CELF Preschool-2 (Wiig, Secord, & Semel, 2004) was administered. Children’s Core Language scores, which consist of Sentence Structure, Word Structure, and Expressive Vocabulary subtest scores, were computed. These subtests require children to interpret spoken sentences of various length and complexity (Sentence Structure), use correct morphology and pronouns (Word Structure), and orally label a series of pictured items (Expressive Vocabulary). Alpha reliability coefficients for the CELF P-2 ranged from .77 to .95 and split-half reliability ranged from .80 to .97. Criterion validity estimates ranged from .57 to .84.
Intervention
The Tier 3 PA intervention consisted of three main components: (a) researcher-developed children’s books to facilitate delivery of the intervention, (b) scripted PA instructional trials embedded in the books, and (c) teaching procedures based on the effective teaching literature.
Children’s books
Twelve children’s books were designed for the previously delivered automated PA intervention (Tier 2), and the same books were used in the intensified PA interventions. Each book included approximately 15 pages of rhyming stanzas and colorful pictures created by a professional illustrator. Six books featured “Jungle Friends” such as an elephant and lion as characters and six featured “Forest Friends” such as a fox and a porcupine as characters. Story content featured familiar, preschooler-appropriate events (e.g., going to the doctor, first day of school, etc.). Additional intervention materials included picture cards and simple game boards to promote interest and active engagement.
Embedded instruction
The reading of books was interrupted 5 to 6 times for brief sets of instructional trials. Practice words were often related to the events in the story to promote interest and story comprehension. Trials were scripted using carefully scaffolded teacher-directed interactions. Instructional trials used a model, guided practice, and independent practice format, and children had many opportunities to practice the target skills. Trials were systematically sequenced within and across books to allow children to build upon previously practiced skills. The general scope and sequence of the targeted skills began with blending a variety of word types (Books 1–3), which gradually transitioned to segmenting lessons (Books 4–6), that in turn were used to teach identification of first sounds in segmented words (Books 7–9) and whole words (Books 10–12). Prior to reading each story, a few scripted instructional trials related to alphabet knowledge also were delivered.
Teaching procedures
Repeated opportunities to respond, explicit teacher-led interactions, and immediate, contingent feedback are three teaching procedures identified in the literature as critical for teaching struggling children and were assembled strategically to intensify the intervention for the current study (Archer & Hughes, 2011). Although the prior Tier 2 PA intervention offered children repeated opportunities to respond, the prerecorded audio delivery format did not ensure children took advantage of those opportunities and the adult was not able to provide differentiated feedback based on students’ responses. Through explicit, teacher-led interactions, interventionists of the Tier 3 PA intervention ensured children were engaged and participating. By following the simple script, they ensured active practice of the target skills using explicit prompting and prompt-fading sequences. The following is an example of an early first sound identification trial: Children were presented with a picture of a kite and 3 boxes, representing the 3 phonemes. “I’m going to tap the first box and say the first sound I hear in /k/ /ī/ /t/. Watch: /k/. (Tap first box.) /k/ is the first sound I heard in kite. Now, you try it. Tap the first box and say the first sound you hear in /k/ /ī/ /t/. ”
An example of a late first sound identification trial is Let’s listen for the first sound in some words. Say zip. (pause) The first sound you hear in zip is /z/. Say /z/. (pause) Now it’s your turn. What is the first sound you hear in bed?
Motor movements were incorporated into games to enhance motivation and engagement, and to draw attention to auditory (vs. visual) stimuli.
Importantly, children received immediate feedback contingent upon their responses. Feedback was differentiated so that when children responded correctly, praise was delivered and the lesson continued; when children (or any one child in the group) responded incorrectly, the interventionists modeled the correct response, helped the children make the response, and then re-presented the trial. When children (or any one child in the group) did not respond, the interventionists simply re-presented the trial.
Procedures
The ultimate goal of the Tier 3 intervention was to improve FSF scores among children who had previously struggled to learn this task. To reach this goal, children participated in intervention 3 to 4 days per week for up to 8 weeks. To facilitate learning PA as a metalinguistic skill, books were repeated within target sets. For example, Books 1 to 3 targeted blending and were administered in subsequent days in 1 week and following a testing day the sequence (Books 1–3) was repeated. After the second cycle of Books 1 to 3 and another testing day, Books 4 to 5 were delivered in the same fashion. In this manner, children received 6 days of blending instruction, 6 days of segmenting instruction, and 12 days of instruction on first sound identification, with approximately 9 testing days.
Children participated in 15- to 20-min intervention sessions in small groups of two or three children and one adult. Each intervention day, the interventionist set up materials prior to bringing children to the designated area. Intervention materials included one book that the interventionist read, pictures and/or game cards, and scripts for embedded instructional trials. Prior to beginning instruction, interventionists taught or reminded children about the rules (e.g., we help each other learn by listening during the story). During the session, children were rewarded for following the rules using stamps, stickers, and/or pencils.
Children’s attendance during intervention sessions was monitored to help determine the amount of intervention children received. Children attended approximately four sessions per week for an average of 24 sessions (range = 22–26). Amber had the lowest total attendance (22 days), and Marcus had the highest total attendance (26 days). When a child was absent, the session was conducted as long as at least two children were present in the group. When only one child was present in a group, intervention was delayed until the following day or when at least two children were able to attend.
Interventionist Training and Treatment Fidelity
Three research assistants with bachelor’s degrees in education or human development served as interventionists. Prior to data collection and program implementation, all interventionists participated in Tier 3 PA intervention training. The first and third authors conducted training. Training included a live demonstration of intervention and assessment procedures followed by independent practice among interventionists. The trainers coached the interventionists during their practice. Finally, the trainers used fidelity checklists for intervention procedures and assessment procedures to “check out” the interventionists. All interventionists demonstrated an adequate level of skills determined necessary for each component of the study by achieving 100% fidelity on both checklists.
To ensure intervention fidelity, 17 of 81 (20%) lessons delivered (minimum of 4 lessons per interventionist) spread across the treatment phase were video recorded and reviewed by a second interventionist. A researcher-developed fidelity checklist, with eight items related to the setup and implementation of the lessons was scored through video observations. Items included stating the rules to be followed during the lesson, correctly reading the story and intervention script, correctly addressing both correct and incorrect responses, and providing reinforcement. Each interventionist correctly completed all eight items during 100% of observed lessons.
Results
Figure 1 presents the children’s performance on FSF, with baseline phases reflecting the staggered initiation of PA treatment for the three groups of children. The first group consisted of two children (Jerome and Tanisha), the second group included three children (Marcus, Jada, and Victoria), and the third group consisted of two children (Amber and Connor).
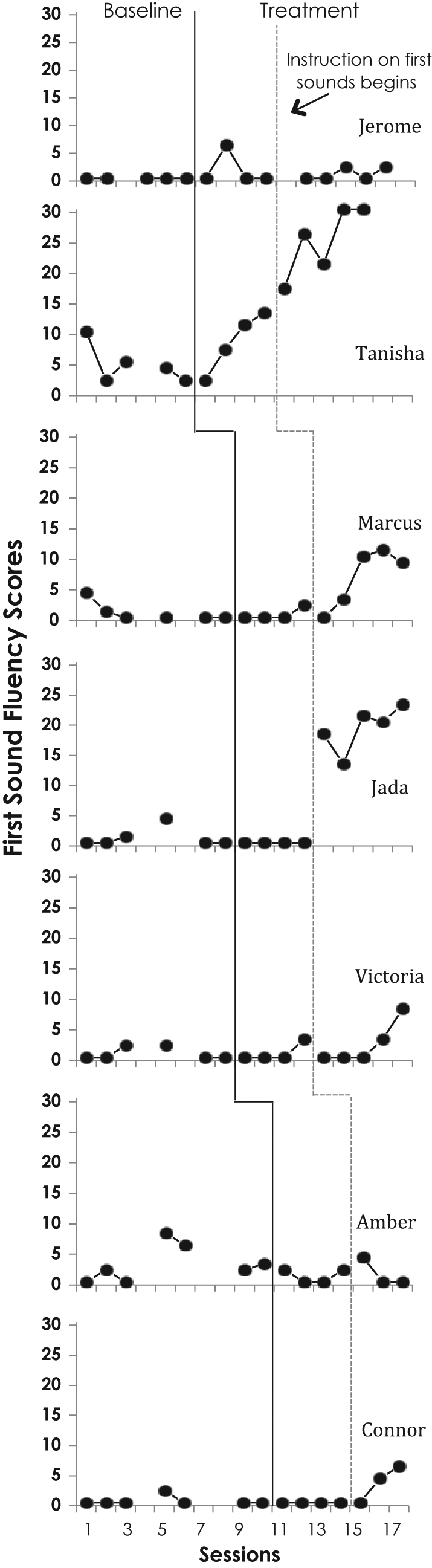
Number correct on First Sound Fluency measure in 1 min during baseline and Tier 3 phonological awareness conditions.
Children’s baseline scores were generally low and stable. Although FSF was the intended primary outcome, identification of first sounds was not introduced in the intervention until after several sessions of work on blending and segmenting, indicated by the dotted vertical lines in Figure 1. Tanisha showed a steady ascending trend immediately following the onset of intervention, whereas improvements in Marcus, Jada, Victoria, and Connor’s FSF scores did not improve until identification of first sounds was targeted during intervention sessions. Only Jada’s data pattern for FSF shows a sharp level change corresponding to instruction on first sounds.
Five of the seven children demonstrated discernible improvements on FSF. Two children, Jerome and Amber, showed no improvement in their low FSF scores and remained in the high risk area (scores of 4 or below). Tanisha, Jada, and Marcus performed above the DIBELS FSF benchmark for the beginning of kindergarten (scores of 10 or above), whereas Victoria and Connor were demonstrating emerging growth approximating the beginning of kindergarten benchmark goal.
Six distal measures were administered at pre- and post-intervention: TOPEL (PA and PK subtests), WPF, Rhyme IGDI, First Sounds IGDI, and Sound ID IGDI. Three of seven children improved on all six measures from pre- to post-test, and all children made gains on at least three measures (see Table 2). Of the five children who showed progress on FSF (Tanisha, Marcus, Jada, Victoria and Connor), only Jada and Victoria made gains of at least a half standard deviation on the TOPEL-PA subtest. However, four of the five made gains of at least a half standard deviation on the PK subtest (only Marcus did not). Surprisingly, Jerome demonstrated improvements of 12 and 21 scale score points on the TOPEL-PA and TOPEL-PK subtests, respectively. A gain of a half standard deviation within 4 months would indicate the child is making progress much faster than the expected growth rate. Jada, Victoria, Tanisha, and Jerome scored above the 90 scale score cutoff for risk on the PA and PK subtests at post-test.
Distal Outcomes.

Note. Gains are over a period of approximately 8 weeks. TOPEL-PA, Test of Preschool Early Literacy (Lonigan, Wagner, Torgesen, & Rashotte, 2007) Phonological Awareness subtest; TOPEL-PK, Test of Preschool Early Literacy Print Knowledge subtest; IGDI = Individual Growth and Development Indicator (McConnell, Bradfield, & Wackerle-Hollman, in press); ID, identification; WPF, Word Parts Fluency (Kaminski & Powell-Smith, 2011).
Improvements also were seen in General Outcome Measures. Jada, Victoria, and Tanisha scored above 10 on WPF (not Connor). On IGDIs with a maximum of 15, all children performed at 10 or above on Rhyming; all children except Amber performed at 10 or above on Sound Identification; Jada, Tanisha, Victoria, and Marcus scored at 10 or above on First Sounds.
Both children who failed to make gains on FSF (Jerome and Amber) made gains on the TOPEL-PA subtest and Jerome also made gains on the PK subtest. Neither child made progress on WPF or on the First Sounds IGDI, which are more closely related to FSF.
Discussion
This study was designed to examine the effects of a Tier 3 intervention on preschool children’s PA skills being taught with the objective of preventing reading difficulty when they begin kindergarten. Children participated in a less intensive prerecorded PA intervention prior to their inclusion in the current study and all showed minimal response to the prerecorded intervention. We intensified the current intervention by delivering explicit teaching interactions with a live interventionist who provided carefully sequenced prompting, fast-paced repeated opportunities to respond, and immediate contingent feedback.
Our approach to intervention was to intentionally bolster blending and segmenting skills so that they could be used to foster identification of the first sounds in words. Explicit instruction on identification of first sounds, our targeted skill, did not begin until Book 7. Initially, we hypothesized that due to the metalinguistic nature of PA, some children may show improvements on FSF before intervention explicitly targeted identification of first sounds. Interestingly, only one of our participants (Tanisha) showed a pattern of responding that would suggest such a general metalinguistic effect. Of all the participants, Tanisha had the highest FSF scores during baseline suggesting these skills were emerging (but not consistent) in her repertoire. Four other participants’ FSF improved once explicit instruction on first sound identification was initiated; two showed robust effects and two were showing gradual improvements when the school year ended. Two participants showed minimal improvements on FSF.
Results suggest that the Tier 3 intervention delivered in this study is an effective procedure for improving identification of first sounds. However, the various patterns of responding indicate that it was not effective for all children. When compared with the prerecorded intervention (Tier 2), substantial improvements were documented for five participants. For two children (Jerome and Amber) who continued to demonstrate limited PA based on their FSF scores, additional instruction needs to be considered. For these children, it is likely that a more intense and perhaps a longer or differently sequenced intervention may be successful in teaching these PA skills.
There are many ways the intervention applied here can be further intensified. For example, it is possible that Amber and Jerome would benefit from one-on-one intervention sessions. Based on anecdotal reports, they had significantly more attention and motivation challenges during the small-group sessions than other children. It is also possible that committing more time to blending and segmenting or ensuring mastery before introducing first sound identification would increase the likelihood of subsequent learning. Finally, it might have been more beneficial to provide a larger number of trials on first sound identification as opposed to dedicating so much time to blending and segmenting. In short, an additional tier of instructional support within an RtI framework would entail greater individualization by a skilled teacher.
In addition to weekly progress monitoring, we examined whether performance on our primary outcome (FSF) generalized to performance on several distal measures. Children with the strongest gains tended to show the most generalized outcomes (Tanisha, Jada, and even Victoria), whereas performance on distal measures was more inconsistent among children with emerging skills (Marcus and Connor). The two children who did not improve on FSF during the intervention nevertheless demonstrated some improvement on the TOPEL and IGDIs.
We examined available information to try to gain insight on reasons why two children did not improve on FSF. Amber and Jerome differed demographically in their gender, age, and ethnicity, but they had similar standardized test scores. Amber and Jerome had two of the three lowest CELF scores (94 and 86, respectively), indicating they had relatively limited language skills. Amber’s score fell nearly a half standard deviation below the mean, and Jerome’s score fell nearly one standard deviation below the mean. Similarly, Amber and Jerome had two of the three lowest scores on the TOPEL-PA (79, 87) and TOPEL-PK (84, 88) subtests. Such a finding is not surprising, as the relation between language and literacy has been well documented (Bishop & Adams, 1990; Justice et al., 2003). Furthermore, Amber was the only child to score more than a standard deviation below the mean on both subtests of the TOPEL. Moreover, Amber displayed the most frequent behavior problems of all participants. Her behavior typically reflected an inability to focus during intervention activities as well as during assessments. A combination of limited language and literacy ability and behavioral challenges may have hindered their ability to benefit fully from the intervention.
Although general classroom instruction (Tier 1) may be sufficient for many children, other children need supplemental instruction (Tier 2), while still others may need intensive, targeted intervention (Tier 3) to acquire key skills such as PA. Previous research has failed to address the needs of those children who did not benefit from Tier 2 PA interventions. Indeed, most studies only include group mean data and do not include data for individual children. Therefore, it is difficult to interpret the findings in the context of RtI. For example, Koutsoftas and colleagues (2009) reported significant gains due to their Tier 2 intervention on PA skills. However, they also noted that 29% of their participants did not make progress. The current study indicates that many of those children may benefit from a Tier 3 intervention as implemented here. Future research needs to explore other modifications within a multitiered system of instruction that may be successful in teaching critical PA skills to children, such as Amber, whom Tier 3 intervention failed to reach. An additional tier of intervention (e.g., one-on-one focused intervention) may be useful before students are referred for special education services. The key is to ensure that students receive the support they need, in the form of an additional tiers of intervention or potentially in the form of special education services.
Limitations and Future Directions
There are several limitations that are worth mentioning. Because the body of literature on tiered interventions is relatively small, the challenges experienced in the current study can help inform areas for future research. For example, there were occasional issues with intelligibility of preschool children’s speech. This made FSF difficult to score and required scorers to listen to the audio recording several times. However, IOA for this measure indicated that scorers generally agreed on most items.
Another challenge related to assessment was that children were less consistent during assessment sessions than they were during intervention sessions. Children often performed well during intervention and poorly on the subsequent probe. Even though the items measured on the assessments were similar to those taught during the lessons, we sometimes see a problem with transfer. There are a couple of possible reasons for this. First, testing is unfamiliar to young children. During assessment, examiners do not readily provide the reinforcement children are used to and preschoolers may not rapidly acclimate to an unusual arrangement of one-to-one testing in a novel setting. Second, baseline testing may establish a pattern of responding (stereotypic or nonresponding) that may be difficult to overcome. Third, young children may be confused by changes in verbal directions and tasks; testers noted that some children did not always understand what they were supposed to do. Working with preschoolers on skills that are not simple and discrete poses many challenges to assessment. Future research should explore the potential of using more authentic approaches to assessment (e.g., embedded in storybooks) to minimize challenges associated with testing young children.
Another limitation involves the interpretation of the distal measures of PA. The pre- and posttest assessments of distal measures should be interpreted as descriptive and exploratory information. Without a basis of comparison that a group design would provide, such information is not readily interpretable. Thus, conclusions about generalized effects should be considered cautiously.
Finally, trained research assistants implemented the intervention. Although this ensured high fidelity of treatment in an early efficacy study, it will be necessary to examine the feasibility of the intervention when conducted by teachers or classroom assistants. Previous studies have demonstrated that it is feasible for teachers to implement supplemental interventions as well as their everyday curriculum. However, the interventions typically require the use of costly materials, extensive training, and often ongoing coaching to ensure fidelity (see Justice et al., 2010). Whereas previous teacher-implemented interventions have required extensive training and ongoing coaching, the fully scripted nature of this intervention should allow teachers to implement the intervention with minimal training.
Conclusion
RtI is a promising approach to meeting the individual needs of all children. The main goals of RtI are to identify children who need additional instruction and to provide that support so that all children reach their full potential. Varying instruction depending on children’s needs should increase the likelihood that each child will be successful in school. This study adds to the evidence supporting the potential of using RtI models to meet the needs of more children. The various levels of instruction the participants were exposed to can be likened to a three-tiered RtI model. All children in this study had previously received general classroom instruction (Tier 1) as well as small-group instruction with several opportunities to respond to PA targets (Tier 2). However, to make progress on more advanced skills, such as identifying initial phonemes in words, some children required additional instructional support (Tier 3).
Despite the growing evidence that RtI can address the needs of more struggling children, the debate continues as to whether policies should encourage its widespread implementation. Rather than teaching all children the same way and viewing learning difficulty as the shortcomings of individual students, a more scientifically grounded prevention approach is to modify our teaching strategies to give each child the instruction he or she needs to be successful. This study begins to demonstrate the feasibility of modifying our teaching strategies to better support children’s learning abilities. It is imperative that we not give up on struggling children, but instead strive to find ways to provide them with the level of instruction they need. Providing evidence of the efficacy of Tier 3 strategies may be a critical step in promoting widespread implementation of RtI models in early childhood settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Cooperative Agreement R324C080011 for the Center for Response to Intervention in Early Childhood from the U.S. Department of Education, Institute of Education Sciences awarded to The Ohio State University.