
Abstract
Reviewers analyzed studies published from 1990 to 2012 to determine early childhood practitioner involvement in functional behavioral assessment (FBA) and function-based behavioral intervention plans (BIP) for children with challenging behavior, age 6 and younger. Coding of 30 studies included practitioner involvement in FBA and BIP processes, training received to conduct FBAs and implement BIPs, and social validity and treatment integrity data. Findings indicate that early childhood practitioners had a limited role in FBAs and BIPs. Practitioner training occurred more often for the BIP than for the FBA. Approximately one fourth of the studies included a description of practitioners in a collaborative role with researchers during the FBA, and approximately one-half during the BIP process, even though practitioners implemented the BIP in the majority of studies reviewed. More than one half of the studies included social validity and/or treatment integrity measures.
Keywords
Severe challenging behaviors displayed by young children can adversely affect not only their social and academic development but also the adults and peers with whom they interact in early childhood programs. Early childhood practitioners have reported an increase in job stress (Strain & Joseph, 2004) and a decrease in job satisfaction due to such behaviors (Hemmeter, 2006). In addition, Gilliam (2005) found that prekindergarten programs were three times more likely to expel children with challenging behaviors than K-12 programs. With limited access to professional development addressing challenging behaviors and the resources to support effective implementation of those strategies, high rates of student expulsion from early childhood programs will most likely continue as practitioners continue to struggle with challenging behaviors (Fox & Little, 2001).
An effective strategy for addressing the severe challenging behaviors of young children is the use of interventions based on functional behavioral assessment (FBA; Dunlap et al., 2006). Commonly accepted FBA procedures include direct and indirect methods of data collection, such as classroom observations and interviews with parents and teachers, to determine why a challenging behavior occurs (Bambara & Kern, 2005). FBA data are used to develop a function-based behavioral intervention plan (BIP) which includes elements addressing environmental factors that trigger challenging behaviors, and consequences maintaining those behaviors (Horner, 1994). FBA and function-based interventions are effective in changing a variety of behaviors displayed by children (Deaver, Miltenberger, & Stricker, 2001; Lerman, Iwata, & Wallace, 1999; Richman, Wacker, Asmus, & Casey, 1998) in both natural (Derby et al., 1997) and clinical settings (Kern, Ringdahl, Hilt, & Sterling-Turner, 2001). Early childhood practitioners have successfully implemented researcher-developed BIPs with a variety of children in various early childhood environments. Ellis and Magee (1999) and LeGray, Dufrene, Sterling-Turner, Olmi, and Bellone (2010) had practitioners use multicomponent BIPs developed by researchers to decrease aggressive, noncompliant, and disruptive behaviors of young children in Head Start and general education classrooms. Reeve and Carr (2000) trained practitioners to implement BIPs to decrease the disruptive behaviors of eight young children with disabilities.
Although researchers continue to demonstrate the effectiveness of function-based interventions in changing behavior (Dunlap et al., 2006), inclusion and training of practitioners in the FBA and BIP processes in early childhood environments continues to be a challenge (Dunlap & Fox, 2011). Within the research literature, early childhood practitioners tend to have a limited role in FBA and/or BIP development, with researchers maintaining a lead role (Lane, Weisenbach, Phillips, & Wehby, 2007). In a review of 35 articles in which FBAs and BIPs were conducted with young children, Wood, Blair, and Ferro (2009) found that within various capacities, early childhood practitioners conducted FBAs in 46% of the studies reviewed, and implemented interventions within 37%. Of those studies, only 7 reflected practitioner involvement in the FBA and BIP processes. Similarly, in a review of positive behavior support strategies used with young children with challenging behavior, Conroy, Dunlap, Clarke, and Alter (2005) identified the number of early childhood practitioners who implemented interventions but did not include information about practitioner involvement beyond the role of intervention agent. While Wood et al. (2009) reported practitioner involvement in FBA and BIP processes, they did not go into detail about level of practitioner involvement in those processes, or training provided.
Inclusion of early childhood practitioners in FBA and BIP processes is important. Reliance on outside behavioral support, with little or no involvement of those who work most closely with a child may result in missed information essential to the development of the most effective function-based BIP. Practitioner involvement in the planning and implementation of a BIP increases the likelihood of a good contextual fit, increased levels of social validity, and maintenance of the BIP in the absence of outside behavioral support. Further review of the type of early childhood practitioner involvement during FBA and BIP processes within the research literature will provide researchers, teacher educators, and early childhood program administrators with the details needed to increase practitioner involvement in the development and implementation of effective BIPs.
In addition to inclusion of practitioners in the FBA and BIP processes, practitioners identify training in strategies to address chronic challenging behavior (e.g., FBA/BIP) as a major professional development need (Snell, Berlin, Voorhees, Stranton-Chapman, & Hadden, 2011). A lack of training in FBA procedures and BIP development and implementation affects the reliability of FBA data, the effectiveness of interventions developed from those data, and the quality of intervention implementation (i.e., treatment integrity). To address these concerns, Dunlap and Fox (2011) suggested a need for more research to identify a systematic approach that would make FBA and BIP procedures accessible to early childhood practitioners. Of literature reviews focusing on the use of positive behavioral interventions and/or FBA and BIP processes (i.e., Blakeslee, Sugai, & Gruba, 1994; Conroy et al., 2005; Lane, Umbreit, & Beebe-Frankernberger, 1999; Nelson, Roberts, Mathur, & Rutherford, 1999; Wood et al, 2009), none provide details of training or supports practitioners received. Identifying studies in which early childhood practitioners received explicit training in FBA and BIP processes will provide needed information about effective strategies promoting practitioner inclusion and active participation in FBA and BIP processes. Early childhood practitioners play an important role in the creation of effective interventions, quality of implementation, and an intervention’s sustainability over time. Analysis of published studies including a description of practitioner involvement and training procedures for FBA and BIP processes will provide important details needed to promote early childhood practitioners’ future involvement in these processes.
The purpose of this literature review was to analyze reported practitioner involvement and training in FBA and BIP processes for young children with challenging behavior. The following questions guided the current analysis: How are early childhood practitioners reported to be involved in FBA and BIP processes? When practitioners are involved in a team effort to conduct FBAs and develop BIPs, in what types of teams are they involved? When provided, what types of training or support do practitioners receive from researchers? Do practitioners complete social validity measures? Are treatment integrity data collected on practitioner implementation of BIPs?
Method
Articles included in this literature review met the following criteria: (a) published between 1990 and 2012 in peer-refereed journals; (b) discussed early childhood practitioner involvement in FBA resulting in the development and/or implementation of a BIP in a school or child care program; (c) included a child participant 6 years of age or younger, displaying a challenging behavior; and (d) included a description of FBA and/or BIP procedures.
We used three processes to locate peer-reviewed articles for the current literature review. First, we conducted an electronic search of studies published between 1990 and 2012 using the databases Academic Research Complete, PsycINFO, and ERIC, and the Internet search engine Google Scholar. Within these sources, we completed a document search using variations and combinations of the following descriptors: early childhood, preschool, kindergarten, child care, teacher, young children, functional assessment, functional analysis, function-based intervention, behavior, disruption, tantrums, self-injurious behavior, and aggression. To ensure inclusion of all articles meeting the criteria, we also conducted a hand search of the following journals, which in the initial electronic search resulted in the greatest number of studies meeting our inclusion criteria: Topics of Early Childhood Special Education, Journal of Positive Behavior Intervention, and Behavioral Disorders. We added Journal of Applied Behavior Analysis and Journal of Early Intervention to the hand search because the journals were readily available and included behavioral interventions and studies with participants within our criterion age range. During hand searches, the second author looked through each journal issue to locate any articles meeting the inclusion criteria. Upon completion of the electronic and hand searches, we reviewed the reference lists of all articles meeting inclusion criteria to ensure that all possible articles were identified. Articles excluded failed to meet all inclusion criteria. The current literature review resulted in identification of 30 studies.
General Coding Procedures
A coding matrix was developed and used to record study information. Coding categories included child participant characteristics, setting, activity/routine targeted for intervention, practitioner years of experience, type of practitioner participation in the FBA, type of practitioner participation in BIP development and implementation, and if reported, social validity and treatment integrity results.
Thirty percent of the articles (n = 9) were reviewed for interrater agreement. The first two authors independently reviewed each of the randomly selected nine articles. The total number of agreements was divided by the total number of all categories (i.e., 36) and multiplied by 100 (Kazdin, 1982) to determine interrater agreement. Overall, mean interrater agreement was 91.7% (range = 84.8%–100%).
Coding Categories and Procedures
Child participants
Coding categories for child participants included age, disability, gender, and challenging behavior. In the studies reviewed, participants were 6 years of age or younger. This age range was selected for two reasons. First, we wanted to capture data about children in kindergarten because kindergarten programs may have environments similar to those typically found in preschool and child care programs. For example, kindergarten classrooms may include environmental arrangements (e.g., centers, circle time area). In addition, similar to other early childhood settings, kindergartens vary between part-day and full-day programs with only 16 states requiring mandatory full-day or part-time kindergarten attendance (Children’s Defense Fund, 2013). Second, including studies with 6-year-olds ensured review of studies, including children who may have turned 6 during their preschool year.
Disability categories were obtained from descriptions in the reviewed studies and were not mutually exclusive. The second author reviewed operational definitions of challenging behaviors in each article, which resulted in five categories of challenging behaviors: aggression, noncompliance/elopement, off-task behavior, self-injurious behaviors (SIBs), and tantrums/disruptions. Aggression was defined as an attempt by the participant to physically harm another person (e.g., bite, pull hair, kick, hit, throw items). Noncompliance/elopement included behaviors such as verbal refusal to follow directions, and leaving an assigned area without obtaining adult permission. Off-task behavior occurred when the participant was engaged in a task or activity other than the one in which he or she was expected to participate. A code of SIBs occurred when a participant attempted to harm one’s self (e.g., eye poking, biting, head banging). Tantrums/disruption was coded if the participant disrupted an activity by making inappropriate vocalizations (e.g., making animal noises, screaming) or movements (e.g., breaking items, falling to the ground). Reviewers coded each behavior if a participant displayed more than one category of challenging behavior.
Setting
When coding for setting, the authors documented the type of program the child attended, type of activities targeted for intervention, and where the intervention occurred. Possible coding for type of program included general education classroom, Head Start classroom, self-contained classroom, preschool/child care setting, and other. Activity codes included centers, free play, group activities, table activities/academic, transitions between activities, unspecified activities, and other. When participants received intervention during more than one activity, authors coded multiple activities.
Practitioner participants
The authors of this review used the label of practitioner to identify teachers and early childhood providers who worked with young children within child care and school settings. Only the primary person involved in child instruction was included in practitioner coding data, information about classroom aides/assistants was excluded. Coding of practitioner participants included in reviewed studies focused on three specific areas: years of experience reported, descriptions of practitioner involvement in the FBA, and descriptions of practitioner involvement in the BIP.
Practitioner experience
Coded information on practitioner participants included highest education level, if provided, and years of experience.
Practitioner involvement in the FBA process
Coding for practitioner involvement in the FBA process included the following categories: FBA team composition, practitioner role throughout the FBA, type of FBA training the practitioner received, and practitioner involvement in FBA data analysis. All codes described in this section were mutually exclusive.
FBA team composition
For studies in which an FBA team existed, the first two authors coded for FBA team composition. The three coding categories for FBA team composition were team, practitioner/researcher, and researcher only. A code of team occurred when there was involvement by a practitioner, researcher, and at least one other adult during the FBA process. For example, if the practitioner, researcher, and classroom paraprofessional reviewed or developed behavior definitions during the FBA process, a code of team occurred. Excluded from a code of team were those instances when other adults may have been interviewed as part of FBA data collection, but were not included in any other element of the FBA process. A code ofpractitioner/researcher occurred when only the practitioner and researcher were involved in the FBA process. The researcher only code occurred when there was an absence of involvement of a practitioner or other adult in the FBA process.
Practitioner role throughout the FBA
Coding of practitioner involvement during the FBA comprised a range from most involvement (i.e., practitioner conducted the FBA) to least involvement (i.e., researcher conducted the FBA without practitioner involvement). Codes used to define practitioner role throughout the FBA were practitioner as lead, collaboration with researcher, limited involvement, and no involvement. A coding of practitioner as lead occurred when the reviewed study included a description of the practitioner making decisions related to data collection, analyzing the data, and explicitly stated that the researcher was not involved in the FBA. A code of collaboration with researcher indicated interaction between the practitioner and researcher throughout the FBA process or included details that the practitioner took an active role, but relied on the researcher for direction and assistance. For example, the study included a description of the researcher and practitioner meeting to discuss the child’s challenging behavior and collaboratively developing an operational definition. A coding of limited involvement included studies in which an interview of the practitioner and/or practitioner implementation of FBA elements occurred, but lacked any mention of collaboration with a researcher. For example, the practitioner is only mentioned in the description of an interview procedure. A code of no involvement occurred if there was an absence of a description of practitioner involvement in the FBA process. For example, only the researcher, or someone other than the practitioner (e.g., graduate student), is described as the implementer of FBA procedures.
Type of FBA training practitioner received
Coding recorded for type of training received during the FBA process comprised a range from explicit training to no description of training. If the reviewed study included a description of the practitioner receiving training in how to conduct an FBA in its entirety and analyze those data, a coding of explicit training occurred. If the reviewed study included a description of the practitioner receiving training on how to conduct a component of the FBA process, a code of training for FBA implementation occurred. For example, there is a description that the practitioner received training in functional analysis (FA) procedures prior to the FA. A code of coaching/feedback only occurred if there was a description of the practitioner receiving coaching or feedback during any component of an FBA, but there was an absence of a description of any specific training. For example, there is a description that during an FA, the practitioner was told by the researcher to ignore the child. If an article failed to describe the type of training, a coding of no description of training occurred.
Practitioner involvement in FBA data analysis
Coding of practitioner involvement in the analysis of FBA data reflected three levels. A code of Yes indicated that the studies reviewed included a description of the practitioner reviewing FBA results to identify function and/or develop a hypothesis, either alone or with a researcher or team. A code of Reviewed indicated that the study included a description of a researcher reviewing the FBA results with the practitioner, but the researcher identified the function and/or developed the hypothesis. A coding of No indicated the reviewed study lacked a description of practitioner involvement in the analysis of FBA results, altogether.
Practitioner involvement in the BIP process
Coding for practitioner involvement in the BIP process was similar to that used for practitioner involvement in the FBA, and included the following areas: BIP team composition, specific role of the practitioner throughout BIP development and implementation, and type of BIP training the practitioner received. All codes described in this section were mutually exclusive.
BIP team composition
For reviewed studies in which a BIP team existed, the first two authors coded each for BIP team composition. The three BIP team composition-coding categories were team, practitioner/researcher, and researcher only. Similar to the FBA team category, a coding of team occurred if the practitioner, researcher, and at least one other adult were involved in development and/or implementation of the BIP. A code of practitioner/researcher indicated participation of only those individuals in the BIP. A code of researcher only occurred when there was an absence of practitioner involvement in the BIP.
Practitioner role throughout BIP development and implementation
Similar to coding of practitioner involvement during FBAs, coding of practitioner involvement during BIPs consisted of four categories. A code of practitioner as lead occurred if the reviewed study included a description of the practitioner as the lead decision maker during development and implementation of the BIP without guidance from the researcher. A code of collaboration indicated the reviewed study included a variation of the words collaboration with researcher to describe interactions between the practitioner and researcher throughout the BIP process or included details that the practitioner took an active role, but relied on the researcher for direction and assistance. This coding may have included instances when the study included details of the researcher and practitioner discussing possible intervention elements during intervention development. A code of limited involvement occurred if the reviewed study included a description of a practitioner-implemented BIP, but there was an absence of details suggesting practitioner/researcher collaboration during BIP development. For example, the practitioner is only mentioned in the description of BIP procedures with no description of the practitioner and researcher meeting to discuss BIP development. A code of no involvement indicated the reviewed study lacked a description of practitioner involvement in the BIP process.
Practitioner intervention training
Three categories comprised coding for type of training provided to the practitioner during the BIP process. If the reviewed study included a description of the practitioner receiving training in how to develop a BIP using FBA data, a code of explicit training occurred. A code of training for BIP implementation indicated those studies in which a description of specific training to implement the BIP or an element of the BIP occurred. A code of coaching/feedback only indicated the practitioner received coaching or feedback during BIP implementation, but there was an absence of any specific training described in the reviewed study. A code of no description indicated an absence of any description of support.
Social validity and treatment integrity
Coding for social validity included presence or absence of social validity data, social validity measure used, who completed the measure, when data collection occurred, and social validity results. Coding categories for social validity results included, large, moderate, or small. Social validity results were coded based on the narrative in the original reviewed study. For example, if social validity results were described as positive, strong, high acceptability, social validity results were coded large. A code of varied indicated social validity results varied (e.g., moderate to large) between raters. For example, authors of a study reported one practitioner gave the intervention a high rating and another practitioner rated the intervention in the moderate range.
Coding for treatment integrity included presence or absence of treatment integrity data collected during the FBA and BIP phases of the reviewed studies, treatment integrity measure used, whose behaviors were included in the evaluation of treatment integrity, who completed the treatment integrity measure, and treatment integrity results. Treatment integrity results were coded based on the narrative in the original studies reviewed. For example, if treatment integrity results were described as strong, high, treatment integrity results were coded as adequate. A code of low indicated the authors of the original study described treatment integrity results as inadequate and/or addressed treatment integrity results in their limitations section. A code of varied indicated reported treatment integrity results differed between implementers. For example, authors of the original study reported intervention implementation was adequate for one practitioner while another practitioner implemented a different intervention with low fidelity. Not recorded indicated an absence of treatment integrity results.
Results
Participants and Settings
Child participants
Seventy-one children participated in the reviewed studies. The majority of participants (84.5%, n = 60) ranged in age between 3 and 5 years. The remaining 15.5% (n = 11) were 6 years old. Of the 71 participants, 57.8% (n = 41) had been identified as experiencing a disability, with 42.2% identified as typically developing or at risk of a disability. Eighty-five percent were boys (n = 60). Approximately two thirds of children engaged in disruption/tantrums (n = 46) and approximately one-half engaged in aggressive behaviors (n = 37). Researchers also targeted noncompliance/elopement (42.3%, n = 30), SIB (4.2%, n = 3), and off-task (1.4%, n = 1) behaviors for intervention.
Settings
The three most common settings included general education (25.3%, n = 18), preschool/child care (28.1%, n = 20), and Head Start (25.3%, n = 18). The remaining participants received services in self-contained (5.6%, n = 4) or unspecified (15.4%, n = 11) settings. Activities targeted for intervention included, group activities (26.7%, n = 19), table activities/academic (26.7%, n = 19), centers (15.4%, n = 11), free play (5.6%, n = 4), transitions between activities (9.8%, n = 7), and unspecified activities (30.9%, n = 22). Four activities (5.6%) received a code of other (e.g., IEP tasks).
Practitioner Experience and Involvement
Included in analyses of practitioner experience and involvement were practitioner years of experience and level of education, FBA and BIP team composition, specific role of the practitioner throughout the FBA and BIP development and implementation, and type of training the practitioner received during the FBA and BIP processes.
Practitioner experience
A total of 52 practitioners participated in the reviewed studies. Four of the studies failed to report the number of practitioner participants, education level, and experience level. Of the education levels reported (n = 24), 8 practitioner participants earned a bachelor’s degree, 13 attended some college, and 3 earned a high school diploma. In those studies reporting years of experience, the majority of practitioners (n = 16) reported less than 6 years of experience, with the remainder reporting 6 to 10 years (n = 8), and 4 reporting more than 11 years of experience.
Practitioner involvement in the FBA process
During the FBA process (Table 1), studies identifying practitioner involvement with a team (43.3%, n = 13) and one-on-one interactions with a researcher (50.0%, n = 15) varied slightly. A majority of the reviewed studies (73.3%, n = 22) included a description of practitioners in a limited role. For example, many of the practitioners conducted an interview as part of the FBA process but did not analyze FBA data. Collaborative interactions with practitioners and researchers during the FBA process were described in 23.3% of the studies. In one study, practitioner involvement in the FBA process did not occur. None of the reviewed studies included a description of practitioners in a lead role during the FBA process.
Practitioner Involvement During FBA Process and Type of Training Reported.

Note. Bold = Researchers in the study reviewed reported inclusion of a practitioner in FBA data analysis.
In most of the studies (90%, n = 27), a description of the type of training practitioners received during the FBA process was absent. Practitioners in two of the studies received training on how to conduct a specific element of the FBA process (e.g., FA). Strain, Wilson, and Dunlap (2011) were the only researchers who included a description of explicit training early childhood practitioners received to conduct an FBA and analyze FBA data. Although the majority of studies did not include a description of practitioner training during the FBA process, practitioners in 36.6% (n = 11) of the studies participated in FBA data analysis. Of those, 33.3% (n = 10) of the studies included a description of practitioner collaboration with researchers to identify function of the challenging behavior and/or develop a hypothesis statement. Practitioners in 63.3% (n = 19) of the studies were not involved in FBA data analysis.
Practitioner involvement in the BIP process
During BIP development and implementation (Table 2), practitioners in the majority of studies worked one-on-one with researchers (63.3%, n = 19). Practitioner involvement in teams occurred in eight of the studies (26.6%) with no practitioner involvement in the remaining three studies (10%). Descriptions of practitioners’ roles in the BIP process suggest either limited (43.3%, n = 13), collaborative (46.6%, n = 14), or no involvement (10%, n = 3). None of the reviewed studies included a description of practitioners in a lead role during BIP development and implementation.
Practitioner Involvement During BIP Process and Type of Training Reported.
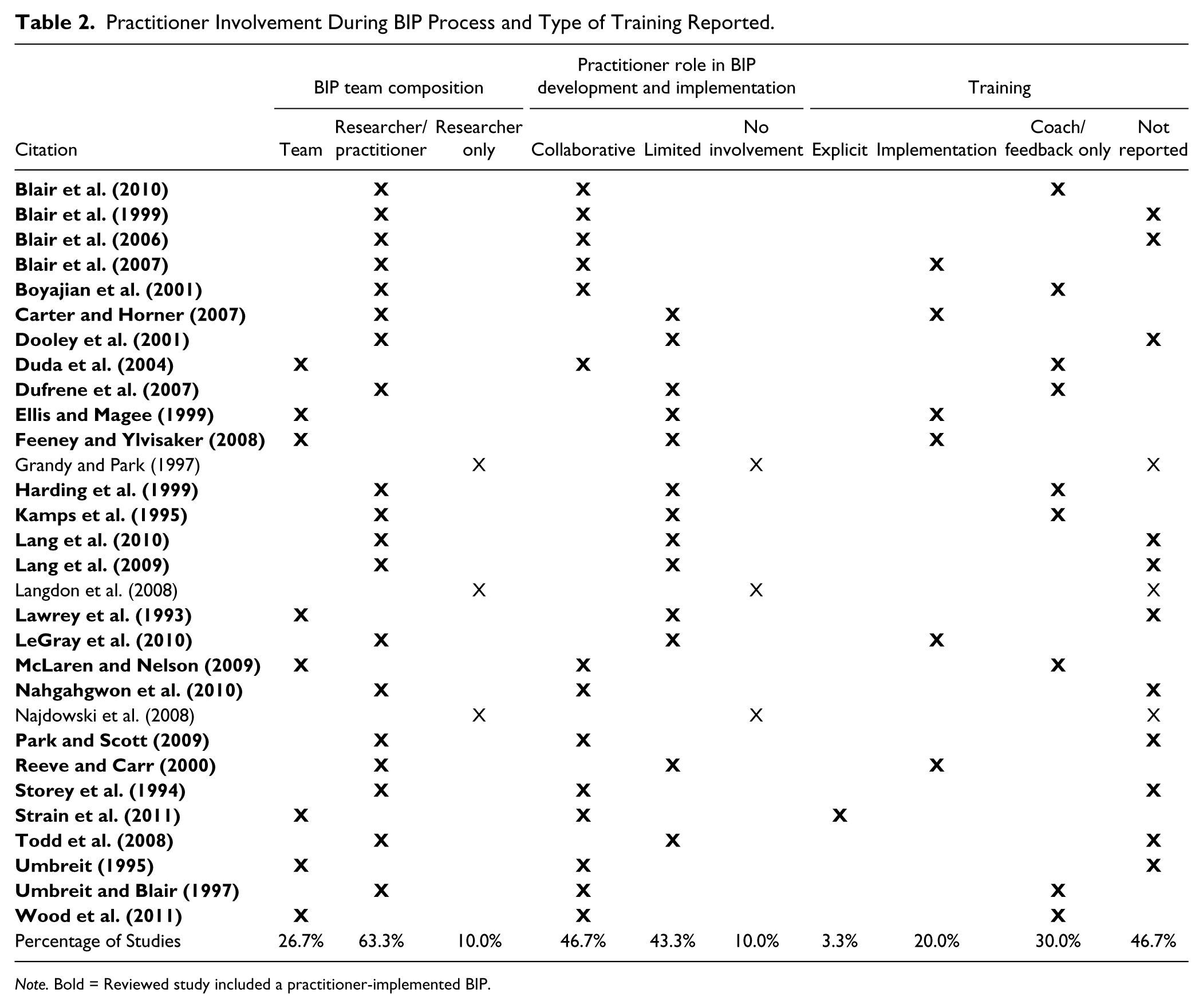
Note. Bold = Reviewed study included a practitioner-implemented BIP.
Forty-six percent (n = 14) of the studies did not include a description of the type of training practitioners received during the BIP process. Of the studies that included a description of training, practitioners received coaching/feedback (30%,n = 9) or specific training (20%, n = 6) to implement the BIP. As with FBA training, Strain and colleagues (2011) were the only researchers who included a description of explicit training practitioners received to develop and implement a BIP. Practitioners implemented BIPs in 90% (n = 27) of the studies reviewed.
Social Validity and Treatment Integrity
Social validity
To examine the extent to which researchers included social validity and treatment integrity, analyses of social validity and treatment integrity data occurred (Table 3). Researchers in 56.6% of the studies (n = 17) included a social validity measure. Of those studies with social validity results reported, 47.1% (n = 8) included results from social validity measurements collected at two different points during the study. Fifty-three percent (n = 9) included only postintervention results. The majority of social validity results were coded as large (88.2%, n = 15) with one coded as small and one coded as varied. Practitioners completed social validity measures in 16 of the studies reviewed. The one study that received a small social validity code (Table 3) reported that, although direct observation data demonstrated an improvement in child behavior following the implementation of the BIP, the practitioner’s social validity rating (i.e., pre = 3.25, post = 2.5) suggested he or she perceived the child’s performance as better prior to the intervention.
Social Validity Data Collection and Result Codes.
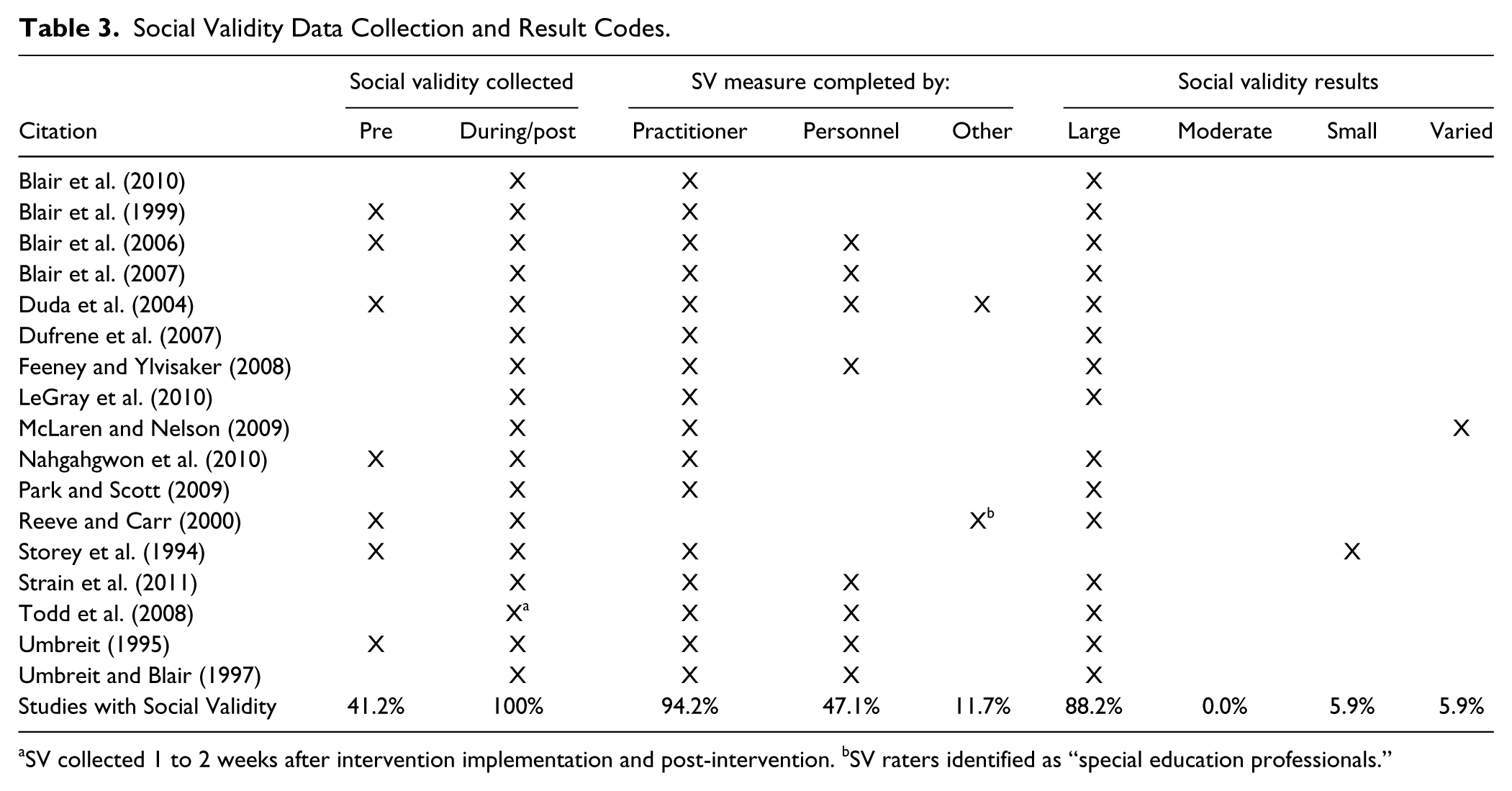
SV collected 1 to 2 weeks after intervention implementation and post-intervention. bSV raters identified as “special education professionals.”
Treatment integrity
Over one half of the studies (53.3%,n = 16) included treatment integrity results on practitioner implementation of BIP procedures, while only 6 studies reported treatment integrity results on practitioner implementation of specific FBA procedures (Table 4). Of the studies including treatment integrity measures, the majority (n = 12) reported adequate results. The remaining studies with treatment integrity reported varied results between participants (n = 3) or unclear (n = 1). Treatment integrity data were missing from 40.7% (n = 11) of the studies in which a practitioner-implemented BIP was discussed. Of the studies including social validity and treatment integrity measures (n = 13), 10 studies reported large social validity results and adequate treatment integrity. Two of the studies reported high or varied social validity results and varied treatment integrity. The remaining study reported adequate treatment integrity data, but unclear social validity results. Approximately one half of the studies with a practitioner-implemented BIP (n = 13) included both measures, while one fourth lacked social validity or treatment integrity results (25.9%, n = 7).
Treatment Integrity Data Collection and Result Codes.
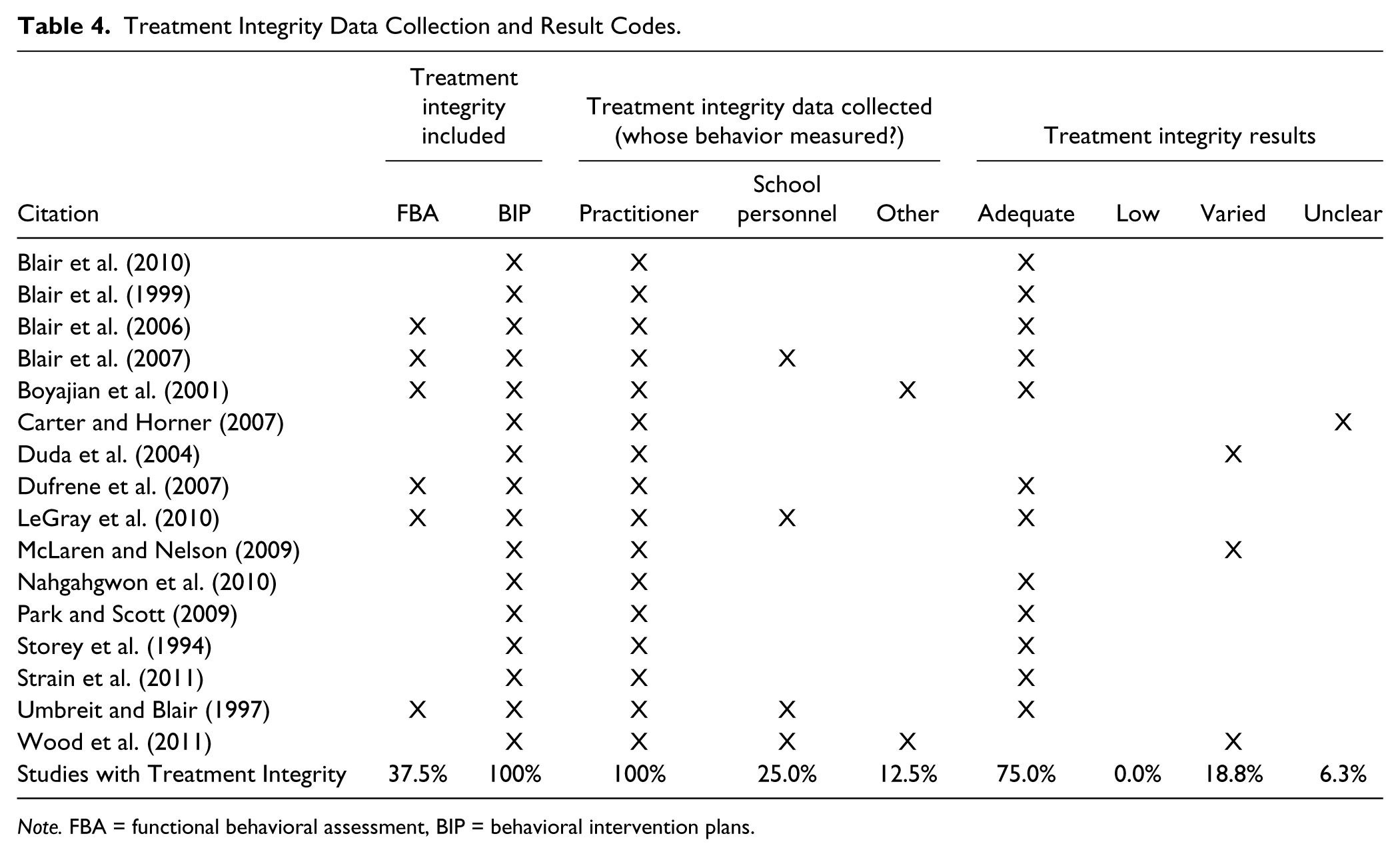
Note. FBA = functional behavioral assessment, BIP = behavioral intervention plans.
Discussion
The purpose of this literature review was to analyze early childhood practitioner involvement in conducting FBAs, and developing and implementing BIPs for young children with challenging behavior. This review adds to existing literature by providing specific details about how early childhood practitioners were involved in FBA and BIP processes.
Findings from this review show the majority of reviewed studies occurred within natural settings and activities. Practitioners worked with a variety of young children with a range of challenging behaviors. The majority of children displayed disruptive/tantrum behaviors and experienced some type of disability. While many of the studies included information about the child participant and setting, most lacked information about practitioner participants. Information about years of experience, training and certification, and education level may help researchers identify practitioner characteristics that support sustained use of FBA and BIPs.
Similar to findings in Wood et al. (2009), practitioner participation during FBA remained limited. Descriptions of practitioner involvement suggest a collaborative role with researchers during the FBA process. Although descriptions of practitioner collaboration with researchers increased during the BIP process, descriptions of practitioners in more than one half of reviewed studies suggest they either participated in a limited role or were not included. This finding is disconcerting when most practitioners were implementing the BIPs.
Teacher involvement in research is essential in improving the quality and suitability of an intervention (Lang et al., 2010; Lang & Page, 2011). Inclusion of practitioners in the development and implementation of a BIP is likely to ensure intervention implementation occurs regardless of the presence or absence of the researcher or behavioral consultant and good contextual fit of elements within the BIP. Equally important, involving practitioners in FBA and BIP processes allows them to develop the knowledge and skills necessary for decreasing challenging behaviors in their classrooms.
With the prevalence of challenging behavior in early childhood environments (Brauner & Stephens, 2006) and limited access to behavioral and mental health supports (Dunlap & Fox, 2011), early childhood practitioners would benefit from training in behavioral support strategies (Gilliam, 2005). Snell and colleagues (2011) suggested the need for a “problem-solving process” (p. 115) that would provide practitioners and school-based teams with the tools to address challenging behaviors and identify effective individualized behavior support strategies. With the need for accessible and comprehensive training programs focused on behavior support strategies, it is of significant concern that 90% of the studies included in the current review did not include a description of training practitioners may have received during the FBA process. When researchers included a description of training, a primary focus was on practitioner implementation of FBA elements or BIP implementation. Only one study (Strain et al., 2011) included a description of Prevent-Teach-Reinforce (Dunlap et al., 2010), a systematic method for training school personnel in conducting FBAs and developing and implementing a BIP. Although their findings were promising, more research is needed on the effects FBA/BIP training programs have on early childhood practitioners.
The role of the early childhood practitioner as lead in conducting FBAs and developing and implementing BIPs is another area for future research. Using the method described in Umbreit, Ferro, Liaupsin, and Lane (2007), Lane, Weisenbach, Little, Phillips, and Wehby (2006) and Lane and colleagues (2007) demonstrated elementary teachers were effective as sole decision maker during FBA and BIP processes. Early childhood programs would benefit from similar training, especially with the limited access to behavior support specialists and the high level of expulsions.
Considering the importance of social validity and treatment integrity data (Horner et al., 2005) and the need for an increased use of these measures (Gresham, Gansle, & Noell, 1993; McIntyre, Gresham, DiGenarro, & Reed, 2007), it is promising that more than one half of the studies included both. The inclusion of treatment integrity data is higher than found in earlier reviews of school-based interventions (i.e., 14.4%, Gresham, Gansle, Noell, Cohen, & Rosenblum, 1993; 30%, McIntyre et al., 2007). Without social validity and treatment integrity data, it is unclear whether the practitioner found the intervention acceptable or whether he or she implemented the intervention with high fidelity. Such data allows one to make adjustments to the intervention that may be more acceptable to the practitioner, thereby resulting in higher levels of social validity and treatment integrity.
Limitations of the review should be considered. First, although the reviewers used methods to ensure identification of all relevant research literature, the hand search was not exhaustive and studies fitting the search criteria may be missing. In addition, descriptions of practitioner involvement in the reviewed studies may not be an accurate representation of what actually occurred during the study. The studies reviewed focused on FBAs and BIPs implemented for young children with challenging behavior rather than practitioner involvement in FBA and BIP processes. Researchers may have limited their description of procedures not directly related to the study’s focus due to page limitation. Finally, treatment integrity and social validity findings should be viewed with caution. Use of original narratives to code level of intervention acceptance and accuracy of intervention implementation may not provide the details needed to accurately assess those data. It was difficult to identify a more accurate method given the limited information reported and the variety of measures used by researchers.
In summary, findings from this literature review suggest early childhood practitioners participate in a limited role during the FBA process and BIP development even though they are the ones implementing the BIPs. FBA and BIP procedures and training need to be more accessible to early childhood practitioners and programs (Dunlap & Fox, 2011). Disseminating these practices to site-based personnel is key to minimizing reliance of early childhood programs and schools on outside behavioral support (Scott & Kamps, 2007). Furthermore, practitioner training and use of FBA and BIP processes will address practitioners’ expressed need for more training in the use of behavioral supports (Snell et al., 2011) and promote the sustained use of these processes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.