
Abstract
The interest in fathers as active parents has increased dramatically over the past 30 years among researchers and the popular press with considerable attention given to direct child-rearing activities; however, mothers continue to be the most likely participants in early intervention (EI) services. Using thematic analysis, we explored providers’ perceptions (N = 511) of father involvement in EI regarding (a) the impact of increased father involvement, (b) how father involvement could be increased, and (c) the role of culture in father involvement. Providers believed more involvement was better and identified several ways in which fathers made a difference. Some providers believed it was not in their hands to increase involvement; however, other providers identified systems-level and direct approaches. Providers preponderantly reported culture as a barrier to involvement but there were notable exceptions. We recommend providers receive professional development to support family-centered philosophies and practices that are inclusive of fathers.
Keywords
Both seminal frameworks and modern recommended practices affirm the role of families in early intervention (EI). Family-centered EI is a philosophy that reflects the belief that the family is at the center of a child’s learning environment and thus is integral to the EI process (Bruder, 2000). This philosophy is central to Part C of the Individuals With Disabilities Improvement Education Act (2004), which asserts that parents are one of the most important influences on early childhood development (Keilty, 2010). Family-centered EI is also a set of practices for facilitating family involvement in EI. The Division for Early Childhood (DEC) outlines 10 recommended family engagement practices, which encompass the themes family centered, family capacity building, and family–professional collaboration (DEC, 2014). In addition, family engagement is a component of practices in each of the topic areas. Family-centered practices are often associated with positive parent, family, and child outcomes (Dunst, Trivette, & Hamby, 2007). Furthermore, when EI providers support responsive parent–child interaction, children have more success in meeting developmental outcomes (Mahoney, Wheeden, & Perales, 2004).
Despite family-centered services being a foundational tenet of the field and associated with positive developmental outcomes, components of service delivery continue to be professionally centered and parents are not always the primary decisions makers in their children’s care (Crais, Roy, & Free, 2006). Moreover, mothers are often the exclusive participants in EI services (Flippin & Crais, 2011), suggesting that both philosophy and practice may need to change to include fathers in EI. This is important as emerging evidence suggests father involvement with young children with disabilities can have positive outcomes on family well-being including lower maternal stress (Saloviita, Itälinna, & Leinonen, 2003), lower maternal depression (Laxman et al., 2015), increased maternal marital satisfaction (Simmerman, Blacher, & Baker, 2001), and higher parenting quality (Keller & Honig, 2004).
Father Involvement
Fathers, as active, involved parents, began to attract the attention of social scientists in the 1970s (e.g., Lamb, 1975). This interest was in contrast to research on fathers conducted in the prior few decades that, for the most part, focused on the consequences for children of father absence (Biller, 1971). The refocused interest on fathers as active parents increased dramatically in the ensuing years with considerable attention given to father involvement in direct child-rearing activities (e.g., Adamsons, O’Brien, & Pasley, 2007; Brown, McBride, Bost, & Shin, 2011; Lamb, 2010; McBride et al., 2005). In the past decade, researchers were joined by policy makers and the popular media in an explicit focus on fathers and fathering (Lamb, 2010). As outlined by Lamb (2010), this refocused interest has led to a shift in societal expectations for men to be more active participants in child rearing than previous generations of fathers. Although these shifts have had some impact on federal and state policy-making arenas (Cabrera, 2010), changes in the orientation and implementation of “family supportive” policies and practices that include fathers are often slow and controversial.
Although policy and practice changes have been slow, the body of evidence supporting father involvement has been growing. Father involvement with young children has been associated with positive early learning outcomes (McWayne, Downer, Campos, & Harris, 2013), improved language and cognitive development (Roggman, Boyce, Cook, Christiansen, & Jones, 2004), and positive peer relationships (Frosch, Cox, & Goldman, 2001). In addition, father involvement may prevent negative outcomes such as challenging behaviors (Frosch et al., 2001) and emotional difficulties (Flouri & Malmberg, 2012). There is some evidence that these patterns of influence are also associated among families with children with disabilities (Keller & Honig, 2004; Laxman et al., 2015; Saloviita et al., 2003). Unfortunately, the current father involvement policy efforts and the establishment of family-centered practices do not seem to have increased the participation of father involvement in EI (Flippin & Crais, 2011).
Fathering practices are highly variable by culture and the United States has a heterogeneous cultural environment marked by economic stratification, an urban–rural divide, a variety of religious traditions, immigrant populations, and a racially and ethnically diverse population (Pleck & Pleck, 1997). From an anthropological perspective, culture is manifested in an infinite number of ways. Culture is how an individual classifies and understands the world (Hewlet, 2017). From this perspective, culture affects the beliefs fathers have about children, their own roles, and appropriate parenting behaviors. Examining cross-cultural differences in father involvement can expose how these beliefs manifest in specific practices.
There is a long ethnographic and empirical history of examining cultural differences in fatherhood (e.g., Fouts, 2008; Hewlett, 1987; LeVine et al., 1994; Whiting & Whiting, 1975). For example, a study of 199 African American, European American, and Lumbee American Indian parents found ethnic differences in emotional socialization (Brown, Craig, & Halberstadt, 2015). As another example, a study of the infant-directed speech of 30 father–infant dyads from Vanuatu and North America found mean differences in pitch variation and range (commonly referred to as motherese) across cultures (Broesch & Bryant, 2018).
It is often difficult for cultural differences in parenting behavior to be incorporated into intervention efforts. For example, Forehand and Kotchick (2016) conducted a review of the literature and found that there were no empirical studies of the cross-cultural effectiveness of behavioral parent training programs. As recognized by the DEC (2014) recommended practices, for EI to be family centered, it must also be culturally appropriate; however, understanding what it means to be culturally appropriate and to incorporate that understanding into practices is very complex. Yet, there has not been a systematic evaluation of providers’ thoughts on the influence of culture in EI services. For the purposes of this study, culture includes beliefs, attitudes, and roles varying across racial/ethnic, socioeconomic, religious, and rural/urban boundaries. Culture also includes the professional culture of service providers.
At this point, there has been no systematic evaluation of providers’ thoughts regarding how to increase father involvement. Their input would be particularly valuable as practitioners are the ones who are directly responsible for building partnerships with fathers. The purpose of this study was to understand the attitudes of providers regarding father involvement in EI. Specifically, we posed the following questions:
Our aim was to gain insights into how to support family-centered interventions that are inclusive of father involvement.
Method
Sample and Procedures
This cross-sectional needs assessment was based on the online survey responses of EI providers in the Midwest who subscribed to a statewide training network. The network provided in-service EI providers with professional development and resources. As part of delivering these services, the network maintained an email listserv. Professional development is critical to many EI providers to maintain their credentials, and providers are motivated to enroll in the listserv. Consequently, the training network administrators estimated that most EI providers were represented. We used this listserv to sample participants by emailing them an invitation to participate with a link to the survey. Institutional review board (IRB) approval was received from the principal investigator’s institution. The administrators of the training network also approved the survey instrument and the research project. The survey was emailed to 9,380 network subscribers of whom 3,073 opened the email, 582 clicked on the link to the survey, and 511 agreed to participate and answered at least the first question. The entire survey took approximately 20 min to complete. Participants were compensated by entry into six raffles for a US$30 Amazon® gift card.
The respondents (N = 511) were predominately female (94.3%), Caucasian (83.8%), and had achieved a master’s degree (62.2%). According to the training network we partnered with, these demographic variables are consistent their overall listserv. The age of participants ranged from 22 to 71 years with a mean of 43.13 years (SD = 11.45 years); the majority were between the ages of 30 and 39 years (31.5%). Respondents had been working in EI for 0 to 41 years with a mean of 9.51 years (SD = 6.79 years); the majority had been working in EI for 2 to 5 years (27.0%). There was a fairly even amount of providers who worked independently (42.7%) and who worked at an agency (45.4%). There were some providers who did both (11.1%) and some respondents who were not currently working in EI (0.4%). The training program specified 21 different EI professions, which we consolidated into six categories: speech and language pathologists (35.4%); developmental therapists or special instructors (18.1%); nonclinical team members such as parent liaisons, translators, and service coordinators (15.3%); physical therapists (11.5%); occupational therapists (10.5%); and mental, behavioral, or physical health professionals such as nutritionists, socioemotional consultants, and behavior specialists (9.3%). Some respondents did not maintain a caseload (7.9%), others had small caseloads (one to five children: 20.4%), medium caseloads (six to 14 children: 24.6%), large caseloads (15–25 children: 30.9%), and very large caseloads (more than 25 children: 16.2%). Respondents provided services in rural areas (18.8%), small communities (23.3%), small cities (26.4%), midsize cities (17.2%), suburban cities (38.7%), and metropolitan cities (32.1%). These are not mutually exclusive categories; many providers served multiple communities of varying size (33.4%).
Measures and Questions
Only the measures and survey questions used in this analysis are reported. Not all respondents went on to answer the open-ended questions; however, there were no significant differences between those who did and did not; thus, we included the demographic characteristics for all respondents to be consistent with other publications from this survey. The number of responses for each of the open-ended questions is given below. For more information on other results from the needs assessment, contact the primary author.
Demographics questionnaire
Participant demographic characteristics were assessed with 11 items regarding gender, ethnicity, education, age, years working in EI, profession, working situation (e.g., at an agency or as an independent provider), the number of children on caseloads, and community size.
Open-ended questions
We used three open-ended questions to assess EI providers’ thoughts on father involvement for this analysis: “What would be the impact of increased father involvement in EI services” (n = 307), “What would you need to increase father involvement in EI services in the families that you work with” (n = 380), and “How does culture play a role in father involvement in EI services?” (n = 347).
Data Analytic Plan
Descriptive statistics were used to report the demographic measures. The answers to the open-ended questions were coded using thematic analysis (Braun & Clarke, 2006). Thematic analysis was selected as an appropriate methodological approach because the data provide a great deal of breadth due to the number of respondents. Thematic analysis provides a systematized method to organize, describe, recognize patterns, and interpret qualitative data to present the myriad of responses as a cohesive story (Braun & Clarke, 2006).
We followed Braun and Clarke’s (2006) six-step outline for conducting thematic analysis. First, we familiarized ourselves with the data. Two members of our research team read the data and separated each response into individual idea units (incidents). Second, we generated initial codes: “a feature of the data that appears interesting” (Braun & Clark, 2006, p. 89). Two members determined codes from a subset of responses, discussed the codes, agreed upon names for codes, and started to form definitions. Then, these members went through the entire data set and assigned codes to incidents. Third, we identified themes. We searched, reviewed, defined, and named themes: A theme is something that “captures something important about the data in relation to the research question and represents some level of patterned response” (Braun & Clark, 2006, p. 82). Thus, a theme reflects a greater degree of interpretation than a code.
We then moved on to the fourth phase: reviewing themes. The coding team examined patterns across these codes to interpret the data more concisely and with greater meaning. The codes were grouped into themes for each question. At this point, there were data that did not fit with any code, data that seemed to contain more than one incident, codes that described only a small amount of data, one code that described large quantities of data, and codes with unclear boundaries (the conditions under which data would or would not be considered for the code). To resolve these issues, our interpretive process was largely guided by Corbin and Strauss’s (2008) writings on constant comparisons, “as the researcher moves along with analysis, each incident in the data is compared with other incidents for similarities and difference. Incidents found to be conceptually similar are grouped together under a higher-level descriptive concept” (p. 72). Through the use of constant comparison, the coding team moved on to the fifth phase: defining and naming themes. Each theme was given a name, definition, and boundaries. This information along with data examples were brought to the entire research team for review. During the reviews, names of themes were critiqued, definitions were refined, and boundaries were tested. The data were then recoded to reflect changes in the themes.
Credibility and Trustworthiness
Credibility and trustworthiness in qualitative inquiry are parallel concepts to reliability and validity in quantitative research. We followed recommendations by Brantlinger, Jimenez, Klingner, Pugach, and Richardson (2005) for establishing credibility and trustworthiness, which included the dimensions reflexivity, evidence, collaboration, debriefing, and description. We sought to be reflexive, referring to attempts to understand the assumptions and bias of the researchers. During initial coding, we talked through assumptions of the coders, and each coder would bring attention to the biases of the other. Biases were also examined by the research team at large. Often, these discussions would clarify important nuance and variation within themes. We looked for disconfirming evidence: data that were inconsistent with the codes or themes. Initially, not all data fit the codes. Codes were expanded, collapsed, and eliminated based on disconfirming evidence to create themes. Disconfirming evidence was then used to test and clarify the boundaries of each theme.
We used a collaborative approach to coding. One member of the coding team was the leader and the other was the secondary coder. These members read and reread the data multiple times and discussed the codes and themes at length. The lead coder was responsible for making revisions and decisions, but the secondary coder was charged specifically with challenging the lead coder’s ideas. Both members needed to come to a consensus for each piece of data. We also used peer debriefing by presenting our preliminary results to experts to provide critical feedback. The rest of the research team, which comprised experts in EI and father involvement, served in this capacity. They critiqued each theme until all members were satisfied that it should remain in the final interpretation of the data. Finally, detailed description was used to provide evidence for interpretations and in outlining the interpretive process.
Results
We report the thematic results of our analysis of participants’ responses to the questions, “What would be the impact of increased father involvement in EI services,” “What would you need to increase father involvement in EI services in the families that you work with,” and “How does culture play a role in father involvement in EI services?” In each case, the results reflect our interpretations of EI provider perceptions regarding father involvement.
A number of responses for each subtheme are reported. Reporting the numbers for each code also helps to put into context the diversity of the responses (Maxwell, 2010). These numbers, however, should be interpreted with caution. They do not reflect the relative importance of each code; rather, a preponderance of responses in a specific code suggests this subtheme was proportionately reported by providers. An additional consideration when interpreting the number of responses is that the codes vary greatly in the degree of breadth of the responses. For example, a very specific code may have relatively few responses but reflect a clear and concise idea. Another code may have a greater number of responses, but this is due to the subtheme representing a broader concept.
The Impact of Increased Father Involvement in EI
The first research question asks in what ways do or do not providers value father involvement and consider how EI could be enhanced through father participation in services, which yielded 17 subthemes describing 587 incidents of data. An additional 11 incidents could not be coded because they could not be interpreted. Data were thematically analyzed and grouped into three major themes: more is better, affects the entire family, and how dads make a difference. Each theme will be described. See Figure 1 for a summary of the responses to the impact of increased father involvement and examples of quotes coded as each subtheme.

The impact of increased father involvement.
More is better (n = 205)
The major theme, more is better, was about the perception that there would be more people involved in EI when fathers were involved and that this would lead to positive outcomes for children. Providers believed that increased father involvement would lead to enhanced child outcomes (n = 83) in the forms of increased child progress and development. Three subthemes suggest specific mechanisms that could cause more to be better and enhanced child outcomes. Outcomes could be enhanced through increased involvement because there is faster child success (n = 21) as children may progress more quickly through objectives. Another mechanism for enhancing outcomes was more opportunities (n = 34) for the implementation and utilization of strategies. The third subtheme suggests there could be greater carryover (n = 67) when fathers were involved. Greater carryover refers to the idea that father involvement in EI facilitates skills learned during EI visits to generalize to other environments. From providers’ perspectives, it seemed greater carryover of skills learned during therapy sessions was related to more opportunities as fathers were able to provide more opportunities for what happened during visits to happen at home and other environments.
Affects the entire family (n = 162)
Providers also recognized that father involvement in EI affects the entire family. In this theme, the focus was on the impact to the family unit as a whole, specific dyads, and individual members of the family. Providers suggested that father involvement in EI benefits the family (n = 33) through decreasing family stress, promoting happiness, building cohesion, and improving familial relationships. The next two subthemes describe didactic impact. Enriched father–child bond (n = 43) described the benefit to families when father involvement in EI helped build and strengthen the relationship between the father and child. The enriched bond was clear in this comment from a speech and language pathologist about the impact of increased father involvement: “it could help fathers understand their child better and deepen their bond.” Providers also suggested that the parent relationship could benefit, noting that it could cause strengthened marital relationships (n = 18) by bringing parents closer together, reducing stress, and building their bond. There were several responses that referred specifically to a reduced chance of divorce such as in this response from a speech and language pathologist that increased father involvement, “could eventually lead to decreased chance for marital disruption if both parents are supported in the EI process.” The subthemes support for mom (n = 49) and father empowerment (n = 20) suggest ways in which father involvement in EI had benefits for each parent. For example, a developmental therapist suggested that increased father involvement would lead to support for mom in her comment, “I think it would also help ease the overwhelming feelings of responsibilities the mothers have.” Providers believed that father involvement could lead to positive outcomes for the fathers themselves in the form of father empowerment (n = 20) as indicated by an occupational therapist in her comment, “fathers would understand the strengths they bring to their child’s development.”
Whereas the preponderance of the responses suggested that the impact of father involvement in EI would be positive, some providers responded that there could be negative or varied impact (n = 19) as father involvement in EI may actually be harmful. Most of these responses focused on complex family dynamics. For example, a parent liaison reflected the belief that increased involvement was not always positive: Involvement is only as good as what is brought. I would hope that most fathers would bring positive modeling and engagement; however, a majority of parents do not engage in a positive manner with their children regardless of the marital state so when adding the complexity of the parental relationship and dynamic, simply increasing father involvement isn’t a necessarily a positive move.
How dads make a difference (n = 200)
In the first two major themes, the emphasis was outcomes. Each of the subthemes in how dads make a difference suggested ways in which child and family outcomes were facilitated through father involvement in EI. Some providers responded that fathers were learning about EI (n = 22) when they were involved. As dads came to learn instructional strategies, reasons for EI services being necessary, and how to be active participants, they were better able support their children. For example, a developmental therapist indicated her perception that increased father involvement would make a difference, “dad would understand more about child and their development and what they could do for their child.” Some providers expressed a belief that a father’s unique influence (n = 33) was a support to a child’s life, which enhanced a child’s development and would, thus, enhance EI. For example, a physical therapist focused on the way dads play and set expectations, Dads have a different play attitude and kids know it. Sometimes if Dad is doing it, the child accepts the more difficult activity from him, where they would fight mom more. I have had moms say a kid will only do certain things for Dad.
In addition to play and setting expectations, providers mentioned a father’s unique influence in terms of motivation, being a role model, that kids want attention from dad, dad seeing the child more realistically, and discipline. An additional benefit to father’s unique influence was that the child received a more balanced approach (n = 38). Providers reported that father involvement could lead to the child receiving support services from both parents, which may be different but complement one another. For example, a service coordinator’s comments reflected her belief that increased father involvement in EI would lead to a more balanced approach: “the child would have balanced therapy sessions and daily living strategies that give two different approaches to the same strategy.” Some providers responded with a concept similar to balanced approach, but instead of focusing on two different approaches, focused on how parents can work together. Getting on the same page (n = 59) suggested how father involvement could get the parents, or the family, to a shared understanding in regard to the child and EI, thus enhancing the consistency of services provided. For example, a developmental therapist described her view of the impact of increased father involvement, “Everyone would be on the same page, working to maximize the child’s potential.” The responses in these two subthemes emphasized providers’ beliefs that it was important for both parents to work together to support the child.
In addition, providers suggested that children may also benefit as fathers contributed insights for providers (n = 21). Providers responded that fathers could give providers a better understanding of the child or family. For example, a developmental therapist said that a positive impact of father involvement in EI would be, “a greater understanding of each child’s strengths and areas to build on.” Some providers made the link between child outcomes and father participation clear. They responded that father involvement in EI could lead to better service planning (n = 27) in terms of more cohesive treatment and better individualized family service plans (IFSPs).
How to Increase Father Involvement in EI
The second research question asks how do providers think they could increase father involvement, if, in fact, they think they are capable of engaging fathers, which yielded 12 subthemes describing 492 incidents of data. An additional two incidents could not be coded because they did not reflect a way to increase father involvement that could be interpreted (e.g., “keeping IT devices”). Data were thematically analyzed and grouped into three themes: it is not in my hands, a systems-level approach, and direct intervention by providers. See Figure 2 for a summary of the themes and subthemes in response to how to increase father involvement and examples of quotes coded as each subtheme.
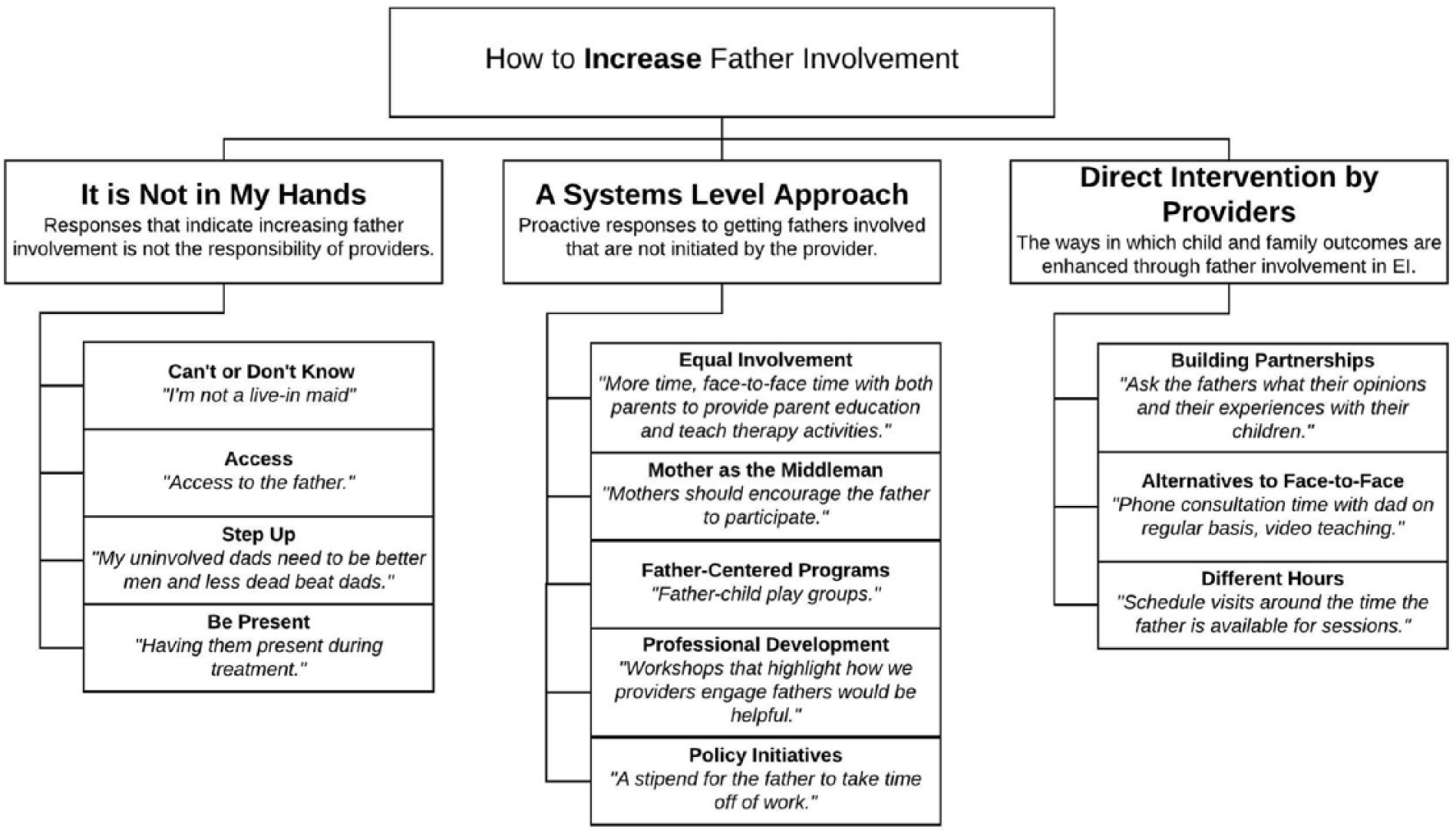
How to increase father involvement.
It is not in my hands (n = 132)
Each of the subthemes in it is not in my hands suggested that providers believed that increasing father involvement was not the responsibility of the providers and little effort on their part could make a difference. Cannot or do not know (n = 58) was the most concrete form of this sentiment. It referred to respondents who did not know how to increase father involvement or thought doing so was impossible. For example, one developmental therapist responded to the question of what she would need to increase father involvement with the statement, “[I would need] a live-in maid—I cannot provide services for all kids on my caseload in evenings or on weekends.” Similarly, several providers responded that they would need access (n = 11) to fathers to increase involvement in EI. For example, a developmental therapist said to increase father involvement, she would need “contact information for fathers so I could contact them to address their needs.” For these providers, it was not in their hands to get contact information, so they could have access to the father.
The next two subthemes, step up and be present, emphasized the onus on fathers to increase their own involvement, but each subtheme has a unique tone. Step up (n = 14) suggested a bias on the part of providers that fathers were not interested in being involved in EI (or the child more generally) and that they should be more motivated and willing. For example, a speech language pathologist said to increase father involvement, “I would need the father to want to be involved.” Many respondents wrote that fathers simply needed to be present (n = 49) to be involved. Although this does not indicate as much bias, it still implies they are not taking responsibility for father involvement and placing the burden on fathers. These responses reflected a belief that fathers should take off from work, arrange their schedules, and be present when EI providers are available. For example, a mental health professional said that to increase father involvement she would need, “[fathers’] flexibility with employment to attend important appointments with the doctors, schools, therapists, or other providers.”
A systems-level approach (n = 112)
Unlike the previous major theme, a systems-level approach reflected proactive responses to getting fathers involved in EI; however, the provider was not the initiator of the change. In this theme, responses referred to efforts of others to get father involved in EI. These responses reflected multiple ecological levels of intervention: familial (mother as the middle man and equal involvement), institutional (professional development and father-centered programs), and societal (policy initiatives).
The first subtheme, mother as the middle man (n = 17), referred to some providers’ ideas about the mother’s role in getting fathers involved by acting in between the father and the provider. The mother, not the provider, should engage the father in EI through encouraging direct participation, valuing the father’s role, not being a barrier, and relaying information. For example, an occupational therapist said that to increase father involvement, she would need to “have the mother report to the father about therapy sessions.” The next subtheme, equal involvement (n = 32), referred to responses that specifically mentioned both parents instead of fathers and that a change to the parental system could increase father involvement by the nature of promoting equal involvement. For example, a speech and language pathologist said to increase father involvement, she would need “more time, face-to-face time with both parents to provide parent education and teach therapy activities/strategies.” The majority of the responses seemed to suggest that both parents needed to be more involved (not that fathers should be just as involved as mothers). The data in this subtheme emphasized the difficulty on the part of providers to consider fathers’ involvement independently of mothers’ involvement.
The next two subthemes related more directly to provider performance, but suggested changes at the institutional or organizational level. Providers reported that they need more professional development (n = 15) such as workshops or trainings to learn how to reach dads and better meet their needs. Providers also reported that they felt father-centered programs (n = 29) would increase father involvement. Some of these responses suggested father-centered programs in the form of male role models as indicated as part of this response by a mental health professional, “male providers, role models, parent liaisons.” At the societal level, providers thought policy initiatives (n = 19) could increase father involvement. These initiatives usually included some sort of compensation either for the provider (e.g., “since this involves extra-time, providers should be compensated for this time of outreach to fathers,” as said by a mental health professional) or for the father to participate in EI (e.g., “a stipend for the father to take time off of work,” as said by a speech and language pathologist). Occasionally, policy ideas included mandating father involvement or work leave: “mandatory attendance to annual/6 month meetings,” as said by an occupational therapist.
Direct intervention by providers (n = 248)
This major theme reflected strategies for increasing father involvement that were directly the result of specific actions on the part of the providers. Building partnerships (n = 59) referred to efforts on the part of providers to communicate, reach out, build relationships, and help fathers to understand EI. The implication was that reaching out to fathers would create successful relationships between providers and fathers, which would make fathers feel important. One example by a social–emotional consultant was to increase father involvement, she would need to “ask the fathers what their opinions and their experiences with their children.” Another type of direct intervention by providers was to use other methods such as phone calls, communication logs, and emails as alternatives to face-to-face (n = 23) involvement and thus increase overall involvement. For example, an occupational therapist said she would need “phone consultation time with dad on regular basis, video teaching” to increase father involvement. Similarly, a mental health professional had a suggestion from her own experience, “I try to include all fathers. I encourage team providers to do so via direct service sessions, written correspondence, videotaping, etc.” The third direct intervention was that different hours (n = 166) were needed to meet with families when fathers are at home. This reflected the idea that providers need more flexibility in their own work schedules. As said by one physical therapist that, to increase father involvement, she would need to “schedule visits around the time the father is available for sessions/meeting.”
The Role of Culture
The third research question asks what the role of culture is on providers’ philosophies and practices regarding father involvement in EI, which yielded 14 subthemes describing 470 incidents of data. Data were thematically analyzed and grouped into four major themes: family culture is not a major factor, culture is a barrier to father involvement, culture facilitates father involvement, and the role of culture is ambiguous. See Figure 3 for a summary of participant responses and examples of quotes coded as each subtheme regarding how culture influences father involvement in their EI contexts. It was clear that providers had a wide range of interpretations of the word “culture” as evidenced in the subthemes. Providers touched on aspects of culture related to ethnicity, religion, socioeconomic status, their own work culture, and American culture. Each of the major themes and subthemes will be discussed in more detail.
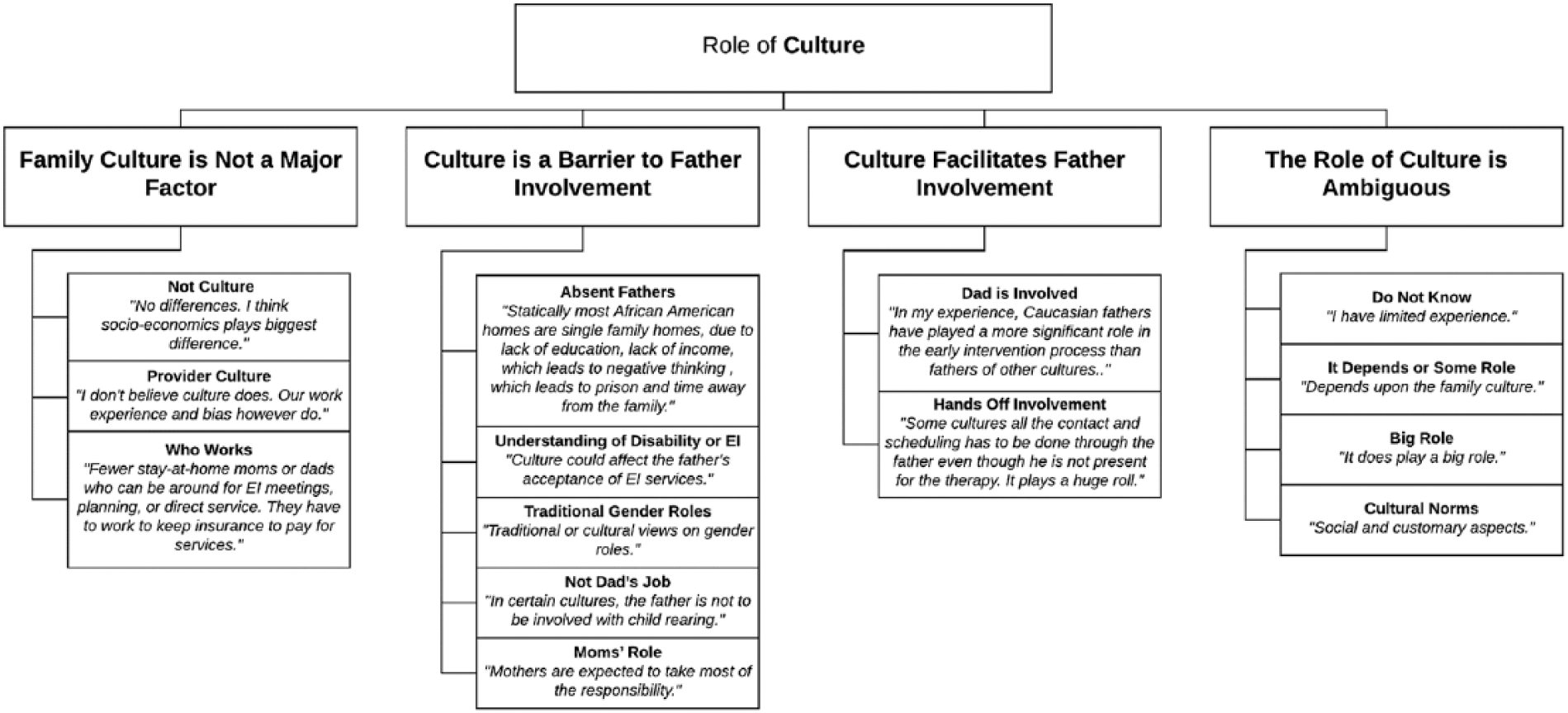
The role of culture.
Family culture is not a major factor (n = 91)
Responses in this theme suggested that the family’s culture is not a major factor in determining whether or not fathers were involved in EI and included the subthemes. The responses coded as not culture (n = 49) reflected the responses of providers who did not believe that culture determines father involvement in EI. Some of these responses focused on individual differences such as this response from a developmental therapist: “Expectations of the father’s role in caregiving vary greatly between cultures and from family to family even within the same cultural background.” Some respondents listed other factors that they did not consider to be cultural as determinants of father involvement such as socioeconomic status or education, such as this speech and language pathologist: “No differences. I think socioeconomics plays biggest difference. My families that are more financially well off tend to have more involved fathers. These families also typically have a nuclear structure (bio/adopted mom and dad) living in same home.” Notably, even though this provider did not interpret socioeconomic status to be a cultural factor, other providers did.
Some responses highlighted provider culture (n = 14) instead of family culture. These responses reflected the idea that the provider culture could dictate whether the provider believed it was his or her role to get fathers involved. For example, a socioemotional consultant suggested that culture plays a role in that “Some families have the expectation that this is the ‘female’s’ responsibility which is important for early interventionists to consider. We should not push our expectations or values onto another family.” These responses also acknowledged that providers had biases, which could affect their ability to get fathers involved. For example, an administrator reflected her belief regarding the impact of culture, “I don’t believe it does [play a role]. Our work experience and bias however do. There is absolutely something every father can do to participate in EI, be it very little or great.”
In the third subtheme, who works (n = 28), the responses focused on whether mother, father, or both work as the greatest determinant of involvement. For example, a developmental therapist responded to the question about the role of culture with her belief that “whoever the stay at home parent is (I have had mom’s and dad’s in this role) is primary. In those situations, I think the parent that is home sees it as part of their ‘job’.” Although work was the primary determinant, some of these responses touched on the role of culture, it was just not the primary factor. For example, an occupational therapist touched upon American culture: “Our American culture of ‘work, work, work’ to survive limits parents’ ability to participate in therapy sessions”; however, the focus is on the role of work in determining father involvement.
Culture is a barrier to father involvement (n = 227)
This major theme suggested a deficit orientation to culture—participants evoking culture as a barrier. The preponderance of responses was in this theme. Culture was amorphous in providers’ responses; it could mean a specific cultural group, an unnamed other or “them,” or refer to a set of values or behaviors that pose a barrier. Some providers believed the father involvement was limited because the father is not part of the family. Being an absent father (n = 29) was the response to how culture plays a role. For example, a developmental therapist said she believed that, “Statistically most Afro [sic] American homes are single family homes, due to lack of education, lack of income, which leads to negative thinking, which leads to prison and time away from the family.” The tie to culture was not usually so specific and was often implied.
Other providers saw culture as a barrier, not because fathers were absent, but rather because culture influenced their understanding of disability or EI (n = 27) in ways that were barriers. For these providers, culture seemed to influence the father’s ability to accept a child with a disability, understand a disability or delay, or understand EI. For example, a speech and language pathologist reflected her views about the role of culture: “In my experience many of them are not worried about their child until the age of three. They tend to say they are still a baby/young. I’m not worried they aren’t talking.”
The remaining codes in this theme all addressed how culture affected roles in such a way as to be barriers to involvement. According to providers, some families’ traditional gender roles (n = 61) were a barrier. In this case, father involvement was limited due to the cultural standard that men provide and women care for children or that men are disciplinarians and women are nurturers. Not all respondents mentioned both the dynamic between mothers and fathers; they only focused on one role. Some providers focused on fathers’ roles and how culture can preclude involvement in EI because it is seen as not dad’s job (n = 21). For example, an occupational therapist described her thoughts on the role of culture in father involvement in EI, “In certain cultures, the father is not to be involved with the child rearing.” Other providers focused on mom’s role (n = 89), which was to participate in EI, thus precluding fathers from participating. A speech and language pathologist said the role of culture was such that “not always, but often the mother is the one involved with scheduling and being present only.”
Culture facilitates father involvement (n = 52)
Although most providers used a deficit model for understanding culture, some identified culture as an asset. Father involvement in this theme takes two forms: dad is involved and hands-off involvement. The first code, dad is involved (n = 39) refers to cultural factors enabling father to be part of EI. These responses sometimes indicated fathers from one cultural group were more involved than other cultural groups. For example, a speech and language pathologist stated her view as follows: “In my experience, Caucasian fathers have played a more significant role in the EI process than fathers of other cultures.” Although a few responses mention specific forms of active involvement, such as being at EI sessions, they typically reference involvement generically such as this response from an occupational therapist: In my experience, even in families where the father would not normally do any child-rearing (and I’m thinking of a specific Nigerian dad), a child with a disability and the emotional turmoil it brings can push people beyond traditional roles.
Some providers mentioned a specific form of hands-off involvement (n = 13). This involvement varied in form such as scheduling, decision-making, general understanding of what is happening, or enhancing the child’s life through play (not specific to EI). Some providers recognized this as a different form of involvement compared with mothers, such as this speech and language pathologist: “I have found that in some cultures, fathers make the final decision on the amount and type of EI services even though the mothers have been more involved and express more concerns.”
The role of culture is ambiguous (n = 72)
Compared with the responses to the other open-ended questions, responses regarding the role of culture were shorter and vaguer. There were several responses where the role of culture was ambiguous. For example, several providers said they do not know (n = 9) the role that culture plays. These were not blank responses, but rather, the respondent wrote in a variation of, “I don’t know.” Other providers indicated that it depends or some role (n = 21) without any other elaboration (e.g., “depends on family culture”). Although several responses throughout the other themes suggest the magnitude of the role of culture in father involvement, several providers said that culture plays a big role (n = 28) with no other context (e.g., “very much so,” “significantly,” “it plays a definite role,” and “important”). Some providers were vague and alluded to cultural norms (n = 14), but in such a way that the role of father involvement was difficult to determine. For example, a physical therapist said, “People’s values and expectations are often influenced by culture.” With a lack of any substantive context, these responses were difficult to interpret.
Discussion
The goal of this article was to understand provider attitudes regarding father involvement in EI in terms of their philosophies and practices. We used qualitative methods to analyze open-ended responses to questions in an online survey and identified key findings regarding the perceived impact of father involvement, how providers believe they can increase father involvement, and the role of culture in father involvement. To understand our findings in the context of family involvement in EI, we will discuss how these results inform our understanding of provider philosophies and practices. We will also discuss how culture informs both philosophies and practices regarding father involvement in EI.
Understanding Provider Philosophies: The Impact of Father Involvement in EI
Providers identified many benefits to fathers being involved in EI at both the child and family levels. Providers believed that father involvement in EI would lead to enhanced child outcomes as well as benefits to mothers, fathers, and the entire family unit. Moreover, providers saw specific mechanisms by which father involvement would promote child outcomes such as by providing insights to everyone being on the same page. Some outcomes suggested by providers have been confirmed in the literature. For example, providers expressed that the impact of increased father involvement would be support for mom and a strengthened marital partnership. Previous research has found that father involvement leads to lower levels of maternal depression (Laxman et al., 2015) and higher levels of marital satisfaction (Simmerman et al., 2001). Other suggestions from providers should be considered in future research on father involvement in EIs. For example, researchers could examine whether faster child success and greater carryover mediate the relation between father involvement and enhanced child outcomes.
Understanding Provider Practices: How to Increase Father Involvement in EI
With regard to increasing father involvement in EI, the preponderance of responses was that providers should offer services during different hours. Parents have reported that it is important to them for providers to consider the family needs when scheduling interventions and fit therapy into family routines (Campbell, Chiarello, Wilcox, & Milbourne, 2009). Unfortunately, the barriers to working nonstandard work hours may be too great for many providers (McBride et al., 2017). Thus, even though working different hours may be the simplest solution to increasing father involvement, some of the other suggestions that providers had may be more effective. For example, policy initiatives, father-centered programs, and alternatives to face-to-face participation may lead to father involvement within the current work constraints. That these types of solutions were not particularly salient to providers suggests they may need professional development to implement strategies for father engagement. This is consistent with other research that has found that although providers do wish to increase parent participation, they view the impetus for increasing participation to be on the parent (Campbell & Halbert, 2002). In addition, from our data, it is unclear the degree to which cultural or gendered connotations influenced the ways in which providers understood increasing father involvement. More research is needed to evaluate the inclusivity of various strategies when promoting involvement in EI.
How Culture Is Reflected in Provider Philosophies and Practices
The discourse in many fields related to EI largely relies on family interactions as being a key difference in outcomes for ethnic minority youth; however, many studies use culturally biased methods (Jarrett, Hamilton, & Coba-Rodriguez, 2015). A deficit orientation to culture was also seen in the responses to how culture affects father involvement in this study. For most providers, culture was only considered when it was a barrier to involvement.
The responses, however, were not without nuance. For example, through the cultural lens, providers were able to see multiple dimensions of father involvement beyond direct involvement during sessions. A dimensional approach is consistent with how involvement is examined in the broader fatherhood literature (Dyer, Day, & Harper, 2013).
Participants in our study largely focused on how culture affects gender roles. This may be a unique contribution of asking providers to consider father involvement and not just parental involvement. In this study, we only accounted for provider perspectives, and not the dynamic relationships between families and providers. Perspectives from fathers and their partners are important for full understanding of father involvement, especially as provider demographics (e.g., female, Caucasian, highly educated) may be different from the families with whom they work. When considering how to increase father involvement, one of the suggestions was for providers to build partnerships with fathers: to communicate, engage, build relationships, and facilitate understanding of EI. Future research can explore effective strategies for building partnerships with fathers, especially when there are cross-cultural differences between fathers and providers.
Limitations
Unlike quantitative research for which the sample should be large, representative, and random to support generalizability, qualitative samples should be purposeful and maximize variation to support analytic conclusions (Sandelowski, 1995). Although there were theoretical strengths to our sample, for example, the inclusion of providers from both rural and urban settings, all the participants in this study came from the same state. Because EI is legislated differently from state to state, policy-level differences could affect provider philosophies and practices. Therefore, we could not account for regional differences. However, the state we selected has several strengths, in that it was economically and culturally diverse, meaning that the providers interact with a diverse sample of fathers.
As another limitation, there may be systematic differences between the participants who choose to participate compared with those who did not; however, given this limitation, we were able to achieve a great deal of variation within our sample. In terms of the size of our sample, the large sample size allowed us to report on the breadth of provider attitudes, but not necessarily the depth. Future research could use interview techniques to better understand the processes underlying provider attitudes. For example, this study did not account for family structure and asked providers to consider father involvement generally. Father involvement in EI may be different depending on the context and should be examined in future research.
Implications
This study represents the first attempt to systemically collect and analyze providers’ thoughts and experiences regarding father involvement on a statewide scale. Although there was great variation in the ways in which providers perceived the impact of father involvement, the overwhelming majority of providers thought increased father involvement would be positive.
When considering how to effectively create change from a theory of planned behavior framework (Ajzen, 1991), often one of the initial efforts is to raise awareness, change attitudes, or get buy-in. Our data suggest that many providers already hold attitudes consistent with increasing father involvement. Practitioners may be lacking specific strategies by which they can effectively increase involvement. To that end, our analysis identified strategies that practitioners believed could be useful for increasing father involvement, which could be incorporated into professional development efforts. Our results provide insights that can be integrated with other research and incorporated into a process of creating professional development focused on increasing father involvement in EI. The degree to which father involvement can be incorporated into family-centered practices should be explored in future research. One facet that will need attention in future research is the intersecting roles of culture, parenting, gender, and services.
Conclusion
For providers in this study, father involvement in EI was seen as a positive asset with many benefits for children receiving services and their families. Providers also had several suggestions for increasing father involvement in EI. Although some of these suggestions showed negative biases toward fathers (e.g., that fathers should step up), many of their insights can be used to inform how to best engage fathers. Not all providers saw culture as influencing father involvement in EI. Providers were most likely to evoke a deficit orientation toward culture, only evoking culture if it was perceived as a barrier to involvement. The philosophies and practices of providers regarding father involvement in EI can inform how best to implement family-centered services that include the entire family.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by a grant from the Institute for Education Sciences of the U.S. Department of Education to B. McBride, R. Santos, S. Hong, and W. J. Dyer (R324A120174).