
Abstract
Using a school-based sample of fifth graders (mean age = 10.38, SD = 0.66) and their parents (N = 408) from Washington, D.C., the authors examine associations of pubertal development with early adolescents’ sexual and nonsexual risk behaviors and their caregivers’ parenting behaviors and of these risk behaviors with parenting behaviors. Results indicate that youths reporting signs of pubertal development were more likely to engage in these risk behaviors than were students reporting no signs. Pubertal development is not related to parenting behaviors; however, parents of youths who reported multiple nonsexual risk behaviors reported more parent–child communication about sexual topics. These results highlight the need to begin risk prevention efforts early, prior to pubertal development. Research is needed to understand how parents can help youths better cope with pubertal development to avoid involvement in sexual and nonsexual risk behaviors.
National secular trends in the timing of pubertal development among U.S. adolescents indicate that youths may be experiencing an earlier onset of pubertal development compared with previous generations (Slyper, 2006). Studies also reveal racial/ethnic differences in pubertal timing. As reported by Chumlea et al. (2003), the median age for achieving menarche is 12.06 years for non-Hispanic Black girls compared with 12.55 and 12.25 years among non-Hispanic White and Mexican American girls, respectively. Similarly, non-Hispanic Black boys tend to develop secondary sexual characteristics at younger ages than non-Hispanic White and Mexican American boys (Sun et al., 2002). Some theorize that earlier pubertal development may be contributing to a “growing mismatch between biological and social maturation,” which may play an important role in the increasing trends of youth psychosocial disorders and risk behaviors (Patton & Viner, 2007, p. 1130).
A growing body of research demonstrates a highly consistent relationship between pubertal development and increases in adolescent risk behaviors, including initiation of early sexual activity (Kirby, Lepore, & Ryan, 2005). With 10% of high school boys and 4% of high school girls reporting initiation of sexual intercourse before 13 years of age (National Campaign, 2008), the potential implications of the trend toward earlier puberty for adolescent risk behaviors cannot be understated. Rates of early sexual activity are even higher among non-Hispanic Black students (16%) compared with non-Hispanic White (4%) and Hispanic students (8%; National Campaign, 2008).
Biro and Dorn (2005) highlighted research suggesting that the increased risk of sexual and other “delinquent behaviors” may be associated with the hormonal increases (e.g., testosterone and estradiol levels) that trigger pubertal development. Others suggest a more complex “biopsychosocial” model in which physical changes associated with puberty affect how an adolescent self-perceives and is perceived by others (e.g., parents, peers, teachers). Thus, physical signs of development are likely to influence an adolescent’s socioemotional state and interpersonal interactions, which may then affect the adolescent’s self-concept, cognitive processes, and subsequent behaviors (Paikoff & Brooks-Gunn, 1991; Steinberg & Morris, 2001).
Although the nature of the parent–child relationship may be especially vulnerable to change as a young adolescent begins puberty, and potentially lead to increased parent–child conflict (Paikoff & Brooks-Gunn, 1991; Sagrestano, McCormick, Paikoff, & Holmbeck, 1999), research also suggests parents can play an important role in helping youths to prepare for the changes associated with puberty (Teitelman, 2004) and to avoid engaging in sexual and other risk behaviors (Miller, Benson, & Galbraith, 2001).
Among urban, minority youths who are at increased risk for engaging in early sexual activities and other risk behaviors, protective parenting behaviors include authoritative parenting styles, characterized by high levels of parental warmth, supervision, and appropriate limit setting (Pittman & Chase-Lansdale, 2001); perceived parental trust and parent–child connectedness (Borawski, Ievers-Landis, Lovegreen, & Trapl, 2003; Rose et al., 2005); parental monitoring and appropriate role modeling (DiClemente et al., 2001; Li, Feigelman, & Stanton, 2000; Rose et al., 2005; Stanton et al., 2002; Yang et al., 2007); and more frequent parent–child communication and fewer communication barriers (DiIorio, Kelley, & Hockenberry-Eaton, 1999; Rose et al., 2005). However, there is little research available on whether urban minority parents help youths cope with the changes associated with puberty to avoid engaging in sexual and nonsexual risk behaviors. Research conducted among African American adolescent males suggests that parents are most aware of the pubertal changes during early adolescence (Cunningham, Swanson, Spencer, & Dupree, 2003). However, research also indicates that few parents are adequately educating their adolescents about puberty (Cooper & Barthalow Koch, 2007) and that parents need assistance in developing the knowledge, comfort, skills, and confidence to talk with their early adolescents about sexual topics (Miller et al., 2009; Walker, Rose, Squire, & Koo, 2008). Research also indicates that parents of urban youths tend to grossly underestimate their adolescents’ sexual and other risk behaviors (O’Donnell et al., 2008), and some argue that more “adaptive parenting strategies” may be needed for youths living in high-risk neighborhoods (Cunningham et al., 2003).
The purpose of this study is first to investigate whether the relationship between puberty and sexual and nonsexual risk behaviors found in other studies holds for a sample of mostly low-income, African American, early adolescents in Washington, D.C. We then extend this research to examine whether early adolescents’ pubertal status and sexual and nonsexual risk behaviors are each independently associated with differences in their parents’ parenting behaviors. Pubertal development may be related to parenting behaviors via its association with the children’s risk behaviors; in addition, puberty may also be directly related to parenting behaviors independent of its link to risk behaviors. Having established whether the link between pubertal development and risk behaviors exists for this sample, we then investigate whether pubertal development has independent, direct relationships with parenting behaviors. The limited available research suggests that pubertal development may engender conflict between children and their parents, but parents may adapt their parenting behaviors to help their children cope with puberty and avoid risk behaviors.
Specifically, we first hypothesize that among low income African American young adolescents, those who report signs of pubertal development will be more likely to have experienced adolescent sexual and nonsexual risk behaviors. Second, we hypothesize that pubertal development among fifth graders, independent of their risk behaviors and of the hypothesized link between pubertal development and these behaviors, is directly associated with decreased quality of the parent–child relationship, and increased parental monitoring and parent–child communication about sexual topics, with fewer parental barriers to such communication. Besides responding to their children’s pubertal development, parents are likely to also respond to any increased risk behaviors during this period of development. Therefore, we also hypothesize that independent of pubertal development, early adolescents’ risk behaviors are also associated with these same outcomes in the parenting variables.
Method
The data used in this article come from the Building Futures for Youth (BFY) Study, an evaluation of the effectiveness of a school-based, adolescent pregnancy prevention program. Launched during the 2001-2002 school year, the BFY Study implemented and evaluated a classroom-based intervention to delay sexual initiation starting with fifth graders in 16 Washington, D.C., schools. Eight schools each were randomly assigned to the intervention and control conditions. This study also included an intervention for the children’s primary caregivers (hereafter referred to as “parents” regardless of relationship). This article uses baseline data from the children and their parents at all 16 schools prior to intervention activities. Although we collected longitudinal data from the students at three later time points during the fifth and sixth grades, we were unable to obtain longitudinal data from enough parents for analysis (see Koo et al., 2011; Rose et al., 2005 for information on the study design and school selection).
Sample
We asked each fifth grader’s parent to complete a survey and sign an informed consent form allowing his or her child to participate. Of 793 students in the 16 schools, 620 (89.5%) received parental consent. Of these, 562 (90.6%) completed the students’ baseline survey. Also, 475 parents completed a baseline survey. This article’s data include only those cases in which both a child and his or her parent completed a survey (N = 408). Analysis of basic demographic characteristics revealed that the sample is representative of all students at the selected schools in terms of being mostly African American (99% vs. 97% in the 16 schools), gender (54% female vs. 52% female in the 16 schools), and low income, as represented by receipt of free or reduced priced school lunch (75% vs. 76%). Caregivers who completed the baseline survey included mostly women (92%), with 82% being the child’s mother. The majority of caregivers reported being employed (64%) and single or never married (57%; see Rose et al., 2005 for a more complete description of the study sample).
Survey Instruments
A 70-item children’s questionnaire was administered to groups of students in their schools. Each student listened to the questions and response options using an individual audiocassette recorder while marking his or her answers on a hard-copy version of the questionnaire. We used gender-specific questionnaires to tailor the wording to boys versus girls. Parents completed a self-administered, 85-item questionnaire on basic demographic information and parenting variables thought to influence adolescent sexual behavior. Parent survey questions reflected many of the same questions in the children’s survey but were reworded slightly to suit parent respondents (see Rose et al., 2005 for further information on the development and testing of the survey instruments).
Measures
Pubertal development
Because we collected information in an open classroom setting and could not perform physical examinations of students to determine Tanner stages (Marshall & Tanner, 1969, 1970), we were limited to asking questions on students’ pubertal status, the primary independent variable. Given the challenges in maintaining classroom discipline and the developmental stage of the fifth graders, it would have been too disruptive to ask these students to choose their own stage from a picture of the Tanner stages. Even with self-report on pubertal status, the students’ age and limited understanding of pubertal terminology were further constraints. Furthermore, the survey administration had to be completed in one class session; based on pretests, the total number of questions could not exceed 70 for the majority of students to be able to complete the questionnaire. Consequently, given the survey’s objectives, no more than two questions focused on pubertal status, a survey approach consistent with other studies (Coleman & Coleman, 2002).
We determined that the girls would understand and could answer the following questions: (a) “Have you started growing breasts or body hair?,” and (b) “Have you ever had a period or menstruated?” (These self-reported markers were also asked by Brooks-Gunn, Warren, Rosso, & Gargiulo, 1987, and by Petersen, Crockett, Richards, & Boxer, 1988). It was more difficult to identify two questions about pubertal status that the boys could understand and answer because compared with girls, boys do not have as easily self-identifiable physical changes or defining pubertal incidents such as menarche. We decided to ask: (a) “Have you started growing body hair or has your voice started to change?” (Petersen et al., 1988), and (2) “Have you ever had a wet dream?” (Kaiser & Gruzelier, 1999; also see Downs & Fuller, 1991). Given the limitations of two survey questions for measuring pubertal development, our goal was not to place students in a stage of pubertal development or to place boys and girls in comparable stages. Rather, it was to obtain an indicator of whether the students had experienced some signs of puberty.
The boys’ responses to the wet-dream question suggested that this question was not well understood, as 33% reported they had had wet dreams (perhaps an inflated result 1 ), and 16% reported they were not sure. Therefore, we decided to base the pubertal development variable only on the other question (body hair or voice change) for boys and, correspondingly, only on the question about breasts or body hair for girls. 2 Thus, if youths responded “yes” to this question, they were coded as having experienced some pubertal development, and having no pubertal signs if they answered “no” or “not sure.” We use this labeling for convenience; some youths thus classified as having no pubertal signs may have experienced other signs not included in the question. However, as a group, they can be assumed to be less likely to have experienced the onset of puberty (or to be in earlier stages of pubertal development). Students who answered “yes” can be assumed to have begun puberty or be in more advanced pubertal development than the other group.
Response choices to the puberty questions were “yes,” “no,” and “not sure.” We grouped the “no” and “not sure” responses so that only if students were certain they had experienced the change (“yes”) would they be assigned to having that change. (We confirmed that grouping the “not sure” with “no” responses was valid by estimating models two ways—one in which this grouping was done and one in which the “not sure” responses were omitted from the analyses. The results from the two sets of models were similar.)
Student’s age and gender
It was important to control for age to distinguish between associations with outcomes due to age differences in social and behavioral development and those due to pubertal development. Because the students were fifth graders, nearly all were either 10 (59.1%) or 11 (30.8%) years old; only 3.9% of the students were ≤ 9 years (the youngest-age response category), and 6.1% were 12 years old (the oldest-age response chosen). Therefore, we grouped age into two categories: ≤ 10 and ≥ 11. It was also important to take gender into account because the levels of risk behaviors are higher for boys and parent–child relationships and parenting behaviors may also differ by the child’s gender.
Students’ risk behaviors
To assess students’ involvement in sexual and other risk behaviors, we used three variables (see Table 1): virginity status, anticipated level of sexual activity in the next 12 months, and involvement in other risk behaviors. Virginity status is a binary variable coded “0” for students who reported not having initiated sexual intercourse and “1” for those who had ever had sex. Anticipated level of sexual activity in the next 12 months is a three-level ordinal variable coded “0” for students who did not anticipate any sexual activity, “1” for those who anticipated kissing or touching under their clothes, and “2” for those anticipating having sex. Involvement in other risk behaviors is a three-level ordinal variable representing experience with “0,” “1,” or “2” (two or more) behaviors, including having consumed more than just one or two sips of alcohol; tried marijuana; sniffed or inhaled something like glue, gas, or paint to feel high; or hung out with a “mob, crew, or gang.”
Children’s and Parents’ Outcome Variables
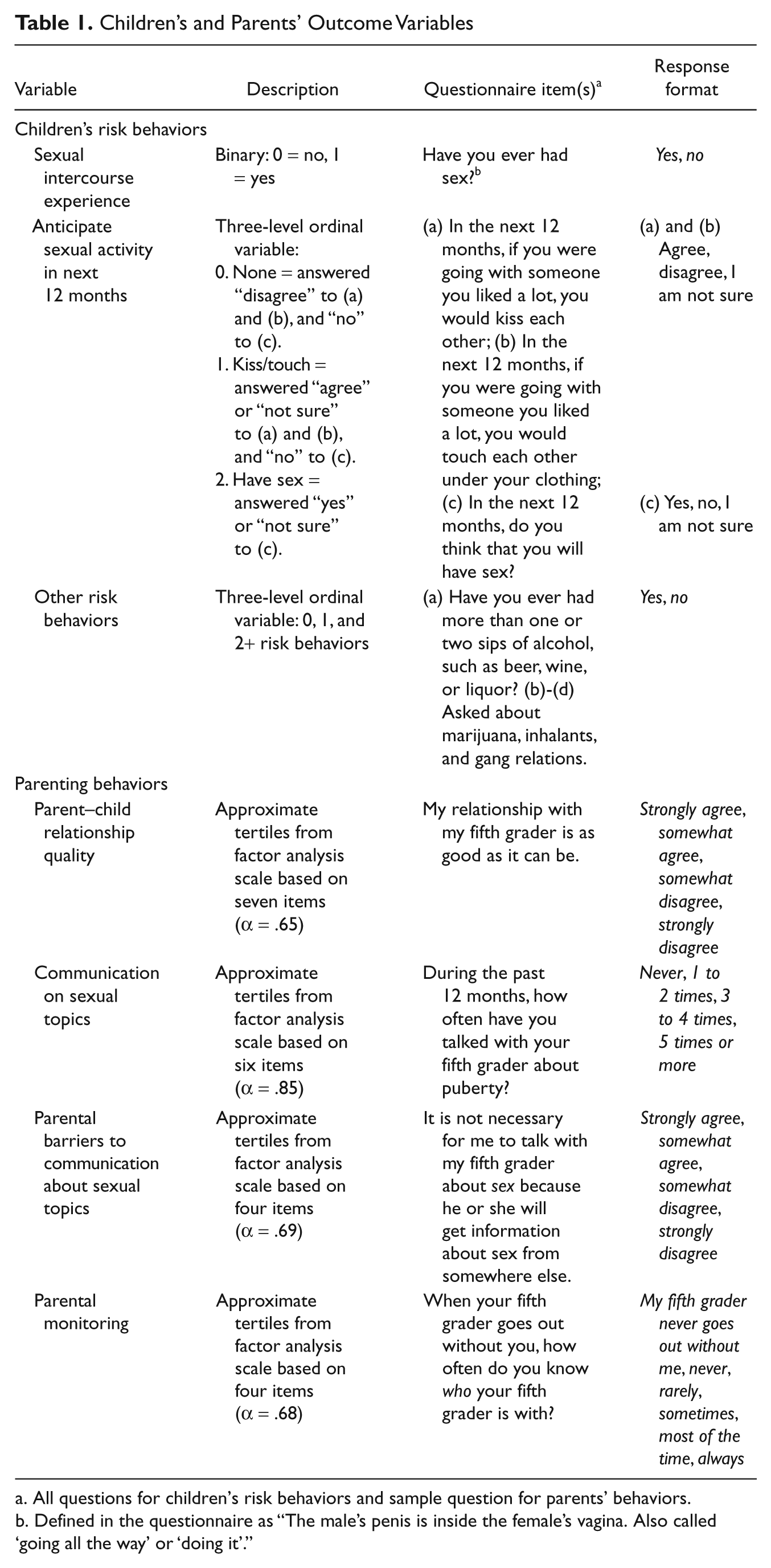
All questions for children’s risk behaviors and sample question for parents’ behaviors.
Defined in the questionnaire as “The male’s penis is inside the female’s vagina. Also called ‘going all the way’ or ‘doing it’.”
Parenting behaviors
We examined parenting behavior with four variables on the basis of scales created through a factor analysis of parent questionnaire responses (see Table 1): quality of parent–child relationship, parent–child communication about sexual topics, parental barriers to communication about sex, and parental monitoring of child’s activities. Because the reliability of three scales was not as high as desired (three had Cronbach’s alpha in the range of .65 to.69) and the distribution of scores in each scale deviated greatly from normality, we grouped each scale’s scores into three categories that are as close as possible to tertiles (i.e., indicating low, medium, and high levels of the variables of interest). We judged that the data quality supported at least three categories and that three levels captured the important distinctions of parenting characteristics. For quality of relationship, communication, and monitoring, higher levels indicate better relationships, more communication, and more monitoring. A higher level in communication barriers indicates more barriers to communication (see Rose et al., 2005 for details regarding the development and psychometric properties of these scales).
Control variables
We controlled for four parental sociodemographic factors that may also affect parenting behaviors and children’s risk behaviors: parent’s education, whether the parent was employed outside the home, frequency of parental attendance at religious services, and number of children < 18 years old in the household (all coded as categorical variables).
Statistical Analysis
We first examined bivariate associations of the independent variables (pubertal development, gender, and age) with the students’ risk behaviors and caregivers’ parenting behaviors, as well as their bivariate association with several parents’ sociodemographic characteristics expected to be also related to these outcomes. We used Pearson’s chi square to test the significance of associations between pairs of cross-classified nominal or ordinal variables (Fienberg, 1980). Subsequently, we estimated multivariable models (discussed later). In these models, we included as control variables four parental sociodemographic characteristics (listed above) whose bivariate relationships with at least one of the outcome variables achieved a p value of .10 or less in the chi-square tests.
For the binary dependent variable—whether the child had ever had sex—we estimated binary logistic regression models. For the other two children’s risk behaviors and the four parenting behaviors (all three-level ordinal variables), we estimated ordered logistic regression models (Agresti, 1990). For the two ordinal students’ risk behaviors, we modeled the odds of higher-risk versus lower-risk behaviors. For the parenting outcomes of relationship quality, communication, and monitoring, we modeled the odds of having higher levels (more desirable) to lower levels of these outcomes. For barriers to communication, we modeled the odds of having lower levels (more desirable) of barriers to higher levels.
Because the puberty variable was based on different questions for boys and girls, we first estimated models separately by gender. The results were similar for the two genders. Thus, we estimated the models for the two genders combined, and to check that the pubertal development variable was associated with the various outcomes in the same way for the two genders, we included an interaction between puberty and gender. The interaction was not significant in any of the models. (In the regression of sexual experience, too few girls had had sex to support the estimation of the model including the interaction. However, the results for the puberty variable were similar in the model for boys and the model for the combined genders.) Thus, having confirmed the similarly of the puberty variable’s associations with the various outcomes across gender, we present the results for the models for the genders combined (without the interaction).
To test the first hypothesis, we estimated three regression models of the three children’s risk behavior outcomes; to test the second and third hypotheses, we estimated four models of parenting behaviors in which both pubertal status and risk behaviors were included in the models. To correct for the increased probability of finding significant results by chance due to multiple testing, we applied the Bonferroni correction (Miller, 1981). In the three models of risk behaviors, for a given α, we set the significance level at α
Results
Pubertal Development and Other Sample Characteristics
A majority (69%) of the children reported some signs of puberty (Table 2). Pubertal status differed by gender (results not shown). A higher proportion of boys reported not having had the pubertal changes in the questionnaire (41%) than girls did (22%).
Sample Characteristics
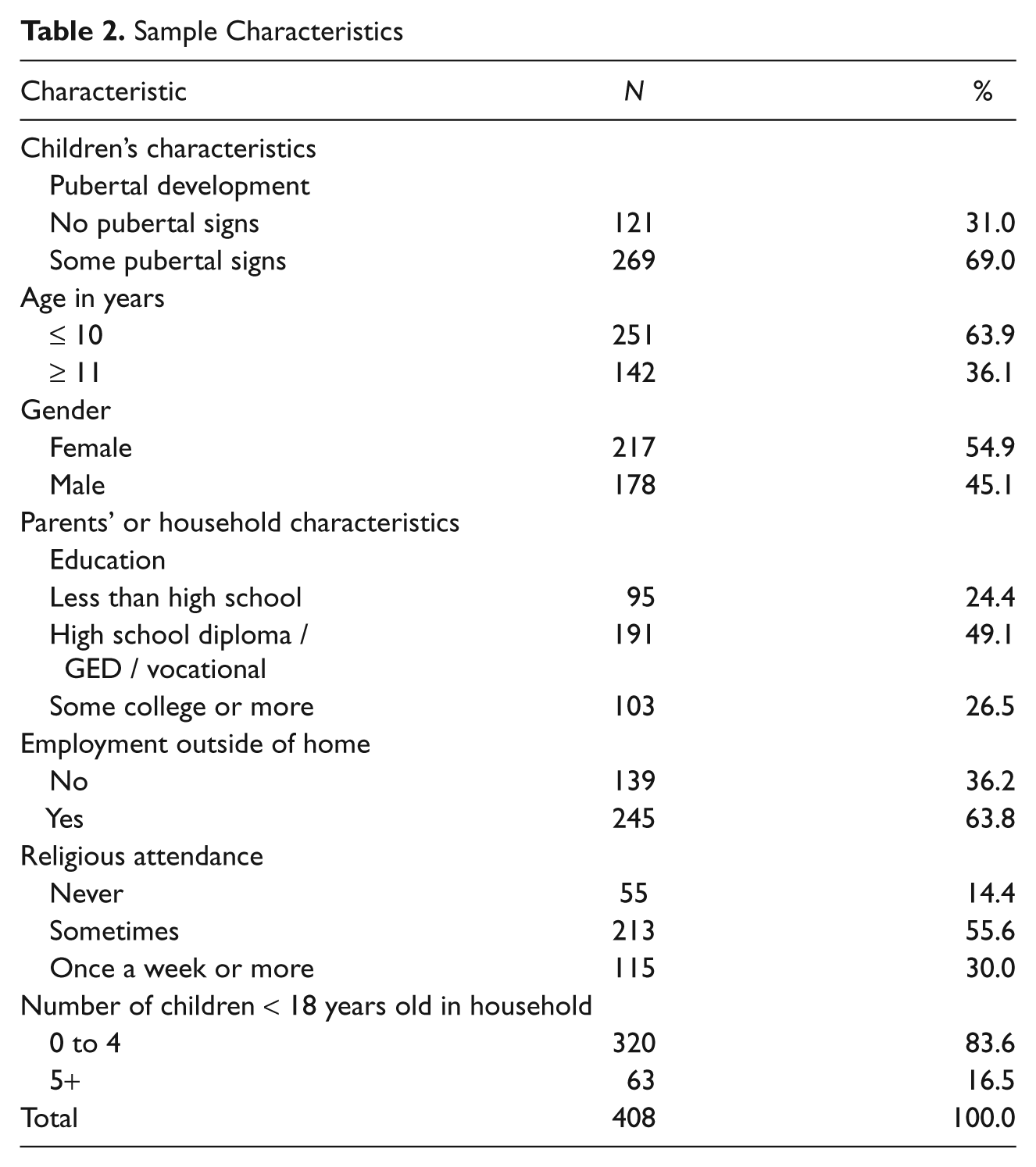
Nearly two thirds of the students were ≤ 10 years of age, and 55% were female. About half of the parents had a high school degree or equivalent, and 64% worked outside the home. Most parents (86%) attended religious services “sometimes” or more frequently, and most (84%) had four or fewer children < 18 years old in the household.
Bivariate Relationships of Pubertal Development and Outcomes
One in 10 students had had sex, 39% anticipate having sex in the next 12 months, and one third had participated in one or more nonsexual risk behaviors (first column of Table 3).
Relationships of Pubertal Development With Children’s Risk Behaviors and Parenting Characteristics
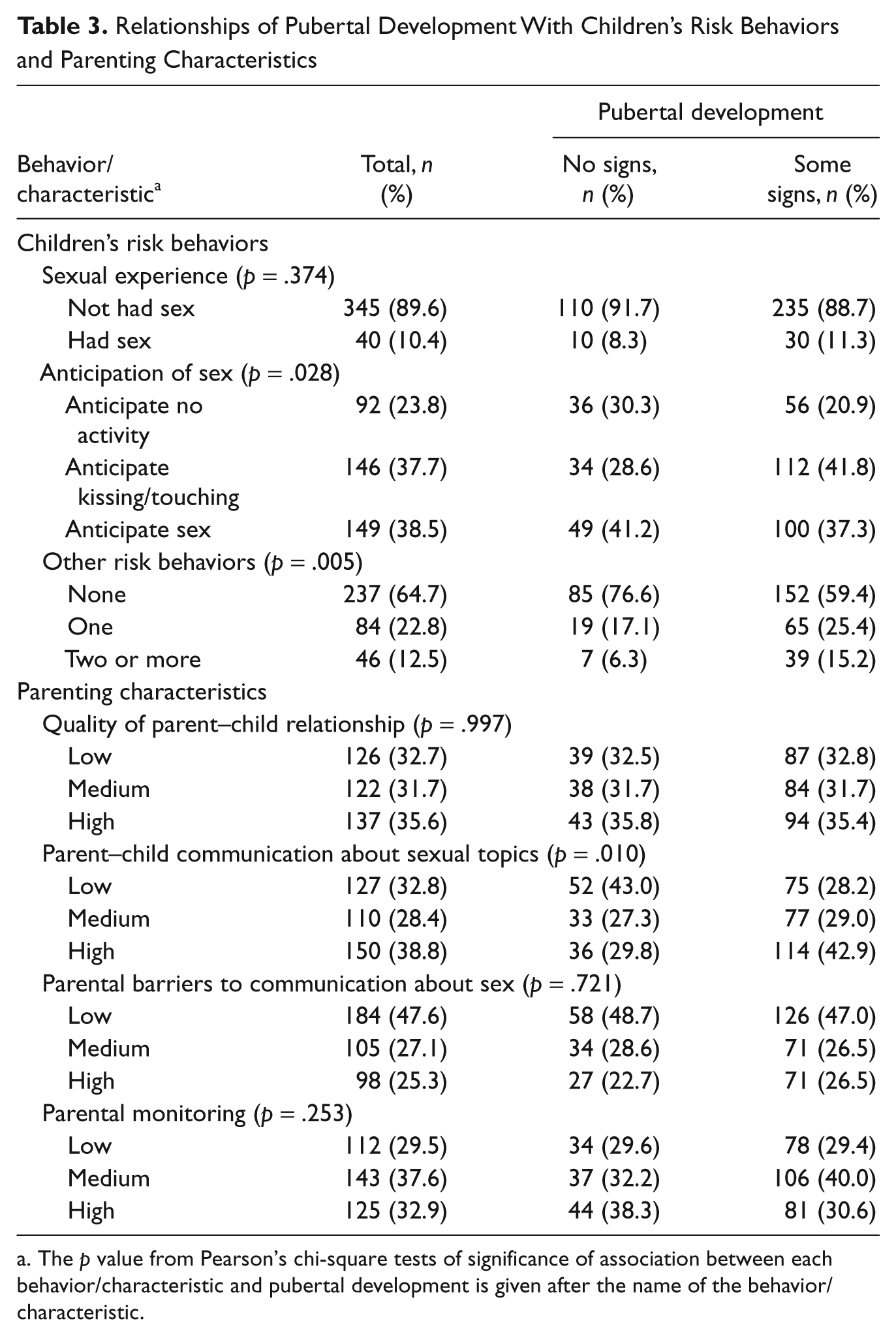
The p value from Pearson’s chi-square tests of significance of association between each behavior/characteristic and pubertal development is given after the name of the behavior/characteristic.
Eight percent of students who reported no pubertal signs, and 11% of those who reported some signs had already had sex, a difference that was not statistically significant (Table 3). Students who reported some pubertal signs were less likely to anticipate no sexual activity in the next 12 months (21% vs. 30%) and more likely to anticipate kissing or touching under clothes (42% vs. 29%), though they were slightly less likely to anticipate having sex (37% vs. 41%, p = .028). Higher proportions of students reporting some pubertal signs had participated in one (25% vs. 17%) and two or more other risk behaviors (15% vs. 6%, p = .005). In contrast, pubertal development was not significantly associated with parent–child relationship quality, communication barriers, or parental monitoring. However, the relationship between pubertal status and parent–child communication about sexual topics was significant (p = .010). Students with some pubertal signs were more likely to have “high” levels of communication about sexual topics (43%) than those with no signs (30%).
Results of Multivariable Models
Relationships of puberty to students’ risk behaviors
As shown in Table 4, students who reported some pubertal signs had 2.6 times the odds of having initiated sexual intercourse than those who reported no pubertal signs, though this result was marginally significant (Bonferroni-corrected p value = .0912). Girls had 83% lower odds of having initiated sexual intercourse than boys (p < .0003).
Relationships of Pubertal Development With Children’s Risk Behaviors: Results of Logistic Regressions
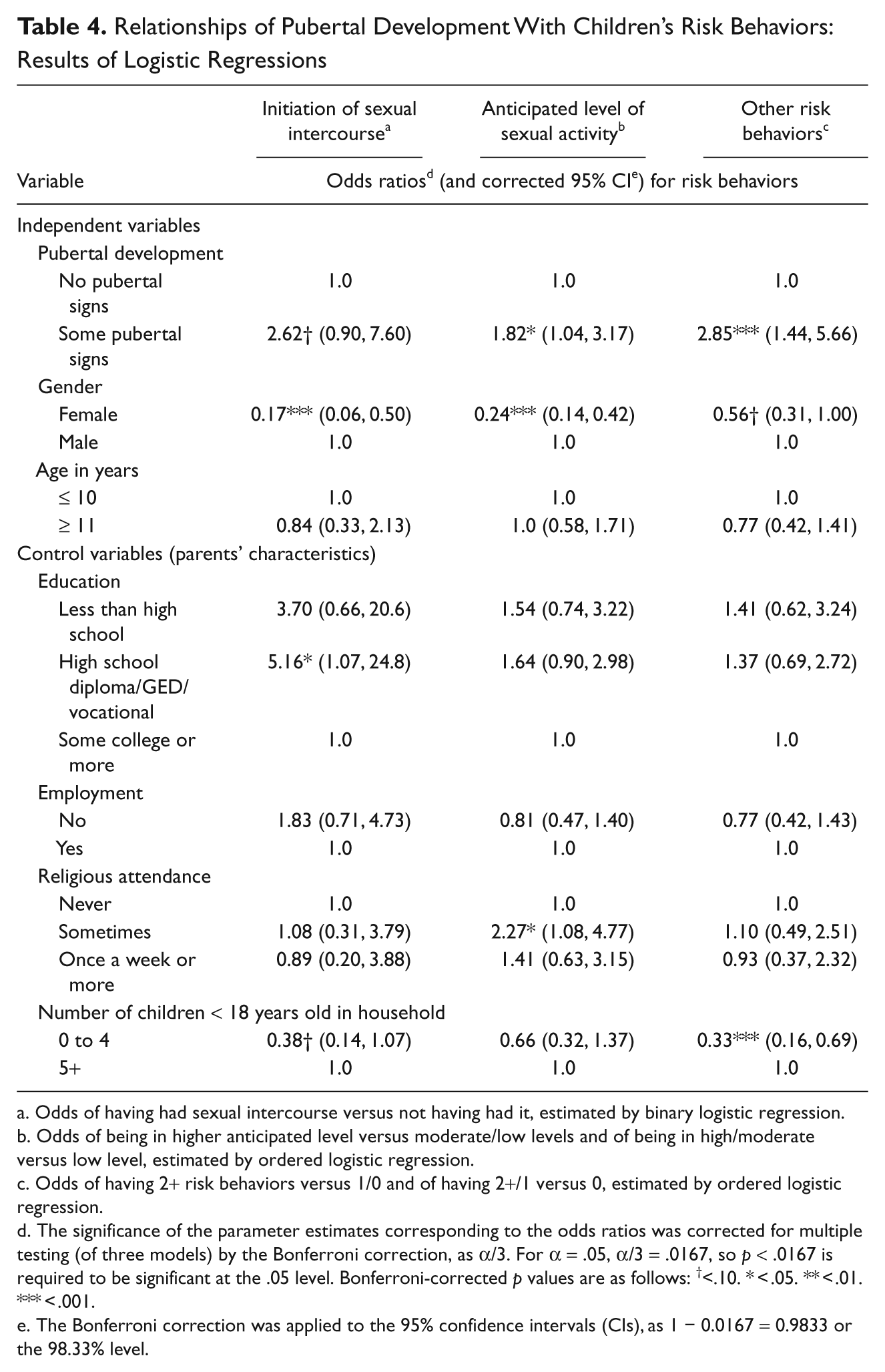
Odds of having had sexual intercourse versus not having had it, estimated by binary logistic regression.
Odds of being in higher anticipated level versus moderate/low levels and of being in high/moderate versus low level, estimated by ordered logistic regression.
Odds of having 2+ risk behaviors versus 1/0 and of having 2+/1 versus 0, estimated by ordered logistic regression.
The significance of the parameter estimates corresponding to the odds ratios was corrected for multiple testing (of three models) by the Bonferroni correction, as α
The Bonferroni correction was applied to the 95% confidence intervals (CIs), as 1 − 0.0167 = 0.9833 or the 98.33% level.
Students reporting some pubertal signs had 1.8 times the odds of anticipating higher levels of sexual activity than those reporting no signs (p = .0303). Girls had 76% lower odds of anticipating higher levels of sexual activity than boys did (p < .0003).
Those reporting some pubertal signs had 2.9 times the odds of having participated in more nonsexual risky behaviors (p = .0027; Table 4). Girls had 44% the odds of having participated in more of these risky behaviors (p = .0504).
Relationships of pubertal development and students’ risk behaviors with parenting behavior
Table 5 shows the results of regressions of parenting behaviors on pubertal development and children’s risk behaviors. Pubertal development was not significantly related to any of the parenting variables. (The same results obtained when children’s risk behaviors were omitted from the regressions, except that the relationship of pubertal development with parent–child communications was marginally significant; p = .0705.) Students’ risk behaviors were not significantly related to parent–child relationship quality, barriers to communication, or parental monitoring. However, students reporting two or more nonsexual risk behaviors had 2.8 times the odds of having more parent–child communication about sexual topics than did students with no risk behaviors (p = .0168). In addition, girls had 2.1 times higher odds than boys of having more communication about sexual topics (p = .0054).
Relationships of Pubertal Development and Children’s Risk Behaviors With Caregivers’ Behavior: Results of Ordered Logistic Regression Models

Odds of being in higher relationship or communication or monitoring group versus moderate/low groups and of being in high/moderate versus low group.
Odds of being in low-barriers group versus moderate/high-barriers groups or of being in low/moderate groups versus high-barrier group.
The significance of the parameter estimates corresponding to the odds ratios was corrected for multiple testing (of four models) by the Bonferroni correction, as α/4. For α = .05, α/4 = .0125, so p < .0125 is required to be significant at the .05 level. Bonferroni-corrected p values are as follows: †<.10. *<.05. **<.01. ***<.001.
The Bonferroni correction was applied to the 95% confidence intervals (CIs), as 1 − 0.0125 = 0.9875 or the 98.75 level.
None of the variables in Table 5 was significantly related to parents’ monitoring behavior.
Discussion
Consistent with other research, in this sample of African American, low-income, urban fifth graders, those who reported having experienced some pubertal changes were more likely to have engaged in sexual and nonsexual risk behaviors. However, the data did not support the hypothesis that pubertal development (apart from its effect on risk behaviors) is directly associated with lower parent–child relationship quality, increased parent–child communication about sexual topics, reduced barriers to such communication, or increased parental monitoring. Also unexpectedly, we found that with one exception, children’s risk behaviors themselves were not related to parent–child relationship quality or parenting behaviors. The exception was that parents of children who reported two or more nonsexual risk behaviors were more likely to have more frequent conversations on sexual topics with their children. (Our data do not allow us to determine whether these conversations included both sexual and nonsexual risk behaviors.) This connection between nonsexual risk behaviors and communications about sexual topics may have arisen because the multiple nonsexual risk behaviors alerted parents to the potential for sexual risk behaviors as well. To our knowledge, no previous study has reported such an association. Thus, it is important to investigate this link further in future research to learn if it is confirmed in other populations. Such a connection is reasonable, however, because (as many studies have shown) nonsexual risk behaviors are associated with early sexual initiation (Forehand et al., 2005; Raine et al., 1999; Santelli et al., 2004; Stueve & O’Donnell, 2005; Weden & Zabin, 2005), and parents may be aware of this.
It is noteworthy that the students’ sexual risk behaviors themselves were not associated with increased communication about sexual topics. This may be in part because parents were not aware of their children’s loss of virginity or their anticipation of engaging in sexual behaviors at such a young age. (As demonstrated by O’Donnell et al., 2008, parents tend to underestimate their young adolescents’ risk behaviors.) However, it may also partly be explained by the great difficulty many parents have in discussing sexual topics with their children, especially those as young as 13 or younger (DiIorio, Pluhar, & Belcher, 2003; Guilamo-Ramos, Jaccard, Dittus, & Collins, 2008; Wilson, Dalberth, Koo, & Gard, 2010). Furthermore, pubertal development was not associated with increased communication about sex; this result suggests that parents’ higher level of communication was associated with their children’s enacted risk behaviors rather than with their beginning pubertal development. Also, contrary to our expectation that pubertal development would stress the parent–child relationship, we found that neither pubertal development nor risk behaviors was related to parents’ perceived quality of the parent–child relationship.
The unexpected findings, however, are consistent with other research among African American adolescent males, which found that neither pubertal development nor pubertal timing is related to a measure of “family hassles,” a variable shown to be positively and highly correlated with increased parental monitoring (Cunningham et al., 2003). Furthermore, Cunningham et al. reported that almost 70% of parents indicated that their childrearing strategies were unaffected by their children’s pubertal changes because their neighborhood’s dangers required specific childrearing strategies regardless of the child’s physical development. In addition, many parents from the schools in the present study stated that they lacked basic knowledge about puberty, including pubertal signs (Walker, Rose, Squire, & Koo, 2008); thus, it is possible that some parents were unaware of early pubertal changes in their children and, therefore, did not respond in their parenting behaviors. Furthermore, the fifth graders were in early stages of pubertal development and experimentation with risk behaviors; some parents may have thought it was not yet necessary to alter their parenting behaviors.
In contrast, other research suggests that among urban, low-income, African American youths, early pubertal development is associated with increases in parent–child conflict (as measured by frequency of “hot discussions”; Sagrestano et al., 1999). Similarly, another study found that among urban African American adolescents, increased family conflict predicted early sexual debut, and the association between family conflict and sexual debut was greater among those with more advanced pubertal development (McBride, Paikoff, & Holmbeck, 2003).
The effects of pubertal development on children’s risk behaviors, however, may depend on parenting style: Among African American children aged between 10 and 12 years and their caregivers (mostly mothers), early maturing boys and girls were more likely to associate with deviant peers and display externalizing behaviors when they reported having “harsh-inconsistent” parents, but they were less likely to do so when they reported having nurturant-involved parents (Ge, Brody, Conger, Simons, & Murry, 2002).
Our study has some limitations. Specifically, our cross-sectional data did not allow us to determine the direction of causality and possible reciprocal causality between pubertal development and children’s risk behaviors and parents’ parenting behaviors. Our sample was drawn from disadvantaged neighborhoods in Washington, D.C., the participants were nearly all African Americans, and only adults and children whose parents gave parental consent to participate were included. Therefore, the generalizability of our study to other fifth-grade populations and their parents may be limited; however, the high-risk nature of the sample makes it of particular interest to study. Furthermore, in this young sample, only 10% (4.3% girls, 17.8% boys) had had sex, limiting the statistical power of the analysis of nonvirginity. However, in the multivariable analysis, the association of pubertal development with sexual experience was marginally significant (p = .0912) with the Bonferroni correction, which is a conservative adjustment; the p value was .0304 without the correction. Therefore, our result is consistent with the findings of many studies (cited earlier) that pubertal development is associated with the initiation of sexual intercourse. In common with all studies based on survey data, the responses of our respondents were subject to biases (e.g., social desirability bias) and error (e.g., errors of recall and knowledge). In particular, the measure of pubertal development for girls and boys was each based on a survey question that we felt would be understandable and answerable by fifth graders in a classroom setting. We could not validate these answers with external measures (such as physical examinations). However, after the baseline survey, the questions were repeated in the spring of the fifth-grade year and in the fall and spring of the sixth grade. The proportions answering “yes” to each of the puberty questions increased over time, indicating a degree of consistency in the students’ understanding of the questions. Nevertheless, our measure of pubertal development is a conservative one, as students with earlier signs of puberty than those included in the questions (one each for each gender) would be classified as not having any pubertal signs, and this would decrease the association between pubertal development and parenting behaviors.
Further investigation of the relationships between pubertal development, adolescent sexual risk behavior, and parenting behaviors is clearly needed. The development of better puberty measures for use in surveys, to allow the study of large samples, would greatly aid the investigation of many issues. In particular, future research should investigate the directions and dynamics of causality among these factors. A better understanding is required of whether and how parents try to adapt their parenting behaviors to their children’s pubertal development, at what stage, and among which subgroups. Improved knowledge is required to identify particular parenting behaviors and parenting styles that help children to avoid risk behaviors as they undergo pubertal development. The role of contextual factors (such as characteristics of neighborhoods, race, and ethnicity) in moderating these connections is also needed. A greatly improved knowledge base would inform the development of effective interventions for parents to help their children deal with pubertal changes and avoid harmful sexual and other behaviors that are often associated with pubertal development.
Conclusion
U.S. adolescents experience very high rates of pregnancy and sexually transmitted infections (Alan Guttmacher Institute, 2006; Centers for Disease Control and Prevention, 2009; Forham et al., 2008; Weinstock, Berman, & Cates, 2004). The association between pubertal development and adolescent sexual activity cannot be overlooked as health professionals and researchers continue to face challenges in improving the sexual and reproductive health of early adolescents and adolescents in the United States. Our study’s results suggest that children may require help in coping with pubertal changes so as to avoid sexual and other risk behaviors that increase during pubertal development and that parents may need assistance to be more sensitive to the pubertal changes their children are undergoing and understand how they can help prepare their children for these changes and steer clear of these risk behaviors. Furthermore, as has been noted, U.S. adolescents are experiencing an earlier onset of pubertal development compared with previous generations. Consequently, it is likely that such preparations may need to take place at an earlier age than parents may expect. African American parents, whose children begin puberty at earlier ages than other groups (as already discussed), may especially benefit from being alerted to the need to start preparing their children at very young ages. Such preparation of children may decrease the level of anxiety around these developmental changes and help adolescents make better choices regarding sexuality (Omar, McElderry, & Zakharia, 2003). Programs designed to reduce sexual intercourse among early adolescents need to consider addressing the potential lack of preparation by parents to guide their children through puberty and to consider implementing interventions to aid the parents as well as the early adolescents.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grants 3U18HD030445, 3U18HD030447, 5U18 HD31206, 3U18HD031919, and 5U18HD036104 from the Eunice Kennedy Shiver National Institute of Child Health and Human Development (NICHD) and the National Center on Minority Health and Health Disparities (NCMHHD) funded the research. RTI International, Howard University, Georgetown University, George Washington University, and NICHD were the participating institutions. ClinicalTrials.gov Identifier: NCT00341471.