
Abstract
Interpersonal traumas experienced early in life adversely impact psychological well-being in children and adolescents, yet the specific role that social support can have in reducing negative outcomes following trauma exposure is unclear. Using a general population sample of seventh-grade students in an urban public school district in the South Central United States (n = 1,712), we examined the effects of early life interpersonal trauma exposure on adolescents’ depressive symptoms and examined moderating effects of two types of social support, perceived parent and school connectedness. Findings suggest that early life trauma is common among young urban adolescents. Linear regression findings indicate that cumulative trauma exposure is associated with greater levels of depressive symptoms. Greater parent and school connectedness are associated with reduced depressive symptoms, and there was a moderating effect for parent connectedness; trauma exposure was significantly associated with depressive symptoms only when parent connectedness was low, indicating a protective effect of high parent connectedness for early adolescents exposed to trauma.
The experience of traumatic events early in life is prevalent among youth (Costello, Erkanalli, Fairbank, & Angold, 2002) and can lead to long-lasting negative psychosocial consequences. Research suggests that more than two thirds (68%) of children experience at least one traumatic event by 16 years of age, with roughly 14% of those children developing posttraumatic stress symptoms (Copeland, Keeler, Angold, & Costello, 2007). Although several early life experiences may trigger trauma-related consequences among adolescents, the most traumatizing events experienced by youth tend to involve interpersonal traumas, such as abuse, domestic violence, and violent crime, in which a child directly experiences or witnesses victimization in the home or community (Charuvastra & Cloitre, 2008). While research has identified significant gender differences in exposure to and consequences of trauma for adolescents (Sieger, Rojas-Vilches, McKinney, & Renk, 2004), additional research is needed that explores how resilience is fostered in sensitive developmental periods (D’Andrea, Ford, Stolbach, Spinazzola, & van der Kolk, 2012).
The current study extends prior literature in several ways. Using a general population sample of seventh-grade students in an ethnically diverse urban school district, we first explore the prevalence of reported exposure to different types of interpersonal traumas for the full sample and by gender. While other studies have looked at these factors, many have relied on clinical populations and retrospective reports by adults, which are subject to issues of recall (Pratchett & Yehuda, 2011). Second, we examine the relationships between interpersonal trauma exposure, background characteristics, and two types of social support (i.e., parental and school connectedness) on early adolescents’ self-reports of depressive symptoms. Finally, we examine interactions between these two types of support and cumulative interpersonal trauma exposure to determine whether parent and/or school connectedness moderate the impact of interpersonal trauma exposure on depressive symptoms, and we further explore whether these differ by gender in a three-way interaction.
Early Adolescence
Marked by rapid and significant growth and change, early adolescence is identified as a distinctive developmental stage situated between childhood and adolescence. Early adolescents (10-14 years of age) experience rapid transformation in physical, cognitive, emotional, and social domains (Dahl & Gunnar, 2009; Eccles & Roeser, 2009). These unique developmental characteristics have led researchers, clinicians, and educators to identify early adolescence as a formative period distinct from late childhood and later adolescence and adulthood.
Extensive research has identified the transition to adolescence as a critical period marked by increased rates of depressive symptoms (Hankin et al., 1998). Depressive symptoms are an important precursor for depressive syndrome, which is the most prevalent mental health problem among adolescents, particularly girls (Birmaher, Arbelaez, & Brent, 2002; Rushton, Forcier, & Schecktman, 2002). Significant gender differences in rates of depression begin to emerge around 13 years of age and remain consistent throughout the life span, with more females than males experiencing depression (Hankin & Abramson, 1999). While research has identified when gender differences in depression emerge, less is known about the mechanisms that may serve as protective factors for depression for girls or boys.
Interpersonal Trauma Among Early Adolescents
The opportunities for stress and growth during early adolescence have unique implications for risk and resilience for early life interpersonal trauma survivors. Keyser, Seelaus, and Kahn (2000) suggest that for the adolescent, interpersonal trauma may constitute any event that is experienced as unmanageable and challenges the adolescent’s sense of safety and security. Experiencing interpersonal traumatic events by early adolescence is common. As many as one quarter to one third of adolescents in the United States have been victims to or witnessed significant early life interpersonal trauma in the form of intrafamilial abuse and/or community violence (Lorion & Saltzman, 1993; Saltzman, Pynoos, Layne, Steinberg, & Aisenberg, 2001). Taylor and Weems (2009) found witnessing community violence and separation and loss of primary caregivers among some of the most commonly reported interpersonal traumas in youth.
While some research suggests that adolescent males experience more trauma overall than adolescent females (Breslau, Peterson, Poisson, Schultz, & Lucia, 2004; Zona & Milan, 2011), interpersonal traumatic events are for the most part prevalent across genders. However, general gender differences in types of interpersonal trauma experiences have been found. In general, females are more likely to be exposed to interpersonal forms of trauma such as sexual assault, molestation, and partner violence in adulthood, as well as child abuse (physical or sexual), while males are more likely to be exposed to fires, disasters, combat, accidents, and physical assaults at the hands of strangers (Breslau, 2001; Flett, Kazantzis, Long, MacDonald, & Millar, 2004; McGruder-Johnson, Davidson, Gleaves, Stock, & Finch, 2000). Minority, low-income, and inner-city youth are disproportionately affected when compared to their peers (Richards et al., 2004; Sedlak et al., 2010). Results from a national survey of youth in the United States found that African American children are 2 times more likely than White children and 1.7 times more likely than Hispanic children to experience interpersonal trauma in the form of abuse or neglect (Sedlak et al., 2010). In a study of children in the sixth through eighth grade in an inner-city neighborhood in Brooklyn, New York, only 12% of children reported that they had not experienced or witnessed any interpersonal violence (Mazza & Reynolds, 1999).
The impact of early life interpersonal trauma has been found to lead to a wide range of negative mental health outcomes, including posttraumatic stress disorder (PTSD; American Psychiatric Association [APA], 2000), substance abuse, suicide attempts, and depressive disorders (Brewin, 2003; Kendall-Tackett, Williams, & Finkelhor, 1993; Kendler et al., 2000; Koenen, Moffitt, Poulton, Martin, & Caspi, 2007). In fact, recent research indicates that depressive symptoms are a more common outcome of trauma than PTSD (Bryant, 2010). The experience of violent interpersonal trauma has been identified as a major risk factor for the development of depression in adolescents (Sieger et al., 2004). Gender differences are apparent in postinterpersonal trauma outcomes for adolescents. In general, research suggests that girls may be more likely to display internalized symptoms, whereas boys are more likely to display externalized symptoms (Pine & Cohen, 2002).
Research examining early life interpersonal trauma also has consistently demonstrated that adolescents who experience one type of traumatic event are likely to experience other types of life course stressors and traumas (Amstadter et al., 2009; Finkelhor, Ormrod, & Turner, 2007). Felitti and colleagues (Chapman et al., 2004; Edwards, Holden, Felitti, & Anda, 2003; Felitti et al., 1998) have found a significant relationship between the number of early life interpersonal trauma experiences (e.g., childhood physical abuse, sexual abuse, witnessing of domestic violence) and the extent of physical and depressive symptoms in adulthood. These findings highlight the importance of understanding and accounting for the cumulative impact of multiple events when exploring the impact of early life interpersonal trauma throughout the lifespan.
Interpersonal traumas represent extremely adverse experiences that challenge and may impair an adolescent’s mental—and possibly physical—health (Cicchetti & Toth, 1995). However, not all adolescents who have experienced interpersonal trauma experience poor mental health outcomes. In this study, we explore factors that protect against the negative consequences (e.g., depression) following interpersonal trauma exposure. The stress-buffering hypothesis asserts that social support mitigates the relation between early life interpersonal trauma and depression (Windle, 1992). Theoretically, this model asserts that if individuals are accepted and valued in their social environments, they may be more likely to feel greater esteem, confidence, and efficacy—factors that could guard against the development of depressive symptoms and other negative posttraumatic outcomes (Nezlek, Kowalski, Leary, Blevins, & Holgate, 1997). Developmental psychologists have delineated three levels of protective factors that promote adaptive coping in adolescents facing adversity and stress. Protective factors in the development of adaptive coping include attributes of the adolescent, aspects of their families, and characteristics of adolescents’ social environments. How adolescents respond to adversity, such as exposure to interpersonal trauma, is impacted by the dynamic interaction between risk and protective factors (Cicchetti, 2011).
Parent Connectedness as a Protective Factor
Empirical literature exploring risk and resilience factors of interpersonal traumatic experiences among children and adolescents has found parental support to be an important factor impacting the response following interpersonal violence and abuse (Paxton, Robinson, Shah, & Schoeny, 2004). Pynoos, Steinberg, and Goenjian (1996) note that family functioning and relationships mediate posttraumatic responses in children and adolescents. In general, studies have found that higher levels of parental connectedness and support are associated with lower levels of posttraumatic stress symptoms (Cohen, Berliner, & Mannarino, 2000). Higher levels of family support have also been associated with lower levels of anxiety and depressive symptoms in children and adolescents exposed to community violence (Gorman-Smith & Tolan, 1998; Kliewer, Lepore, Oskin, & Johnson, 1998). In a study of urban African American youth, Li, Nussbaum, and Richards (2007) found that the quality of adolescents’ family support and helpfulness served as a protective factor against internalizing symptoms, but only when risk factors (e.g., poverty and exposure to violence) were low. Research also has revealed that negative social support (e.g., criticism, blaming responses) or a lack of social support following trauma exposure is associated with increased rates of depression in adolescents (Bal, De Bourdeaudhuij, Crombez, & Van Oost, 2005; Lee, Detels, Rotheram-Borus, & Duan, 2007). These findings suggest that the perceived presence of parental support and care may be critical to youth adjustment following a range of interpersonal traumatic experiences. We expect to find that parent connectedness will be negatively associated with depressive symptoms and that it moderates the negative consequences of interpersonal trauma exposure for early adolescents.
School Connectedness as a Protective Factor
Connection to school is another potential factor for resilience argued to be particularly important for adolescents as they begin the individuation process in which they begin to rely less on family supports and more on extrafamilial relationships (Goodenow, 1993). Perceptions of support and safety within the school environment, frequently referred to as school connectedness, have been found to be positively related to self-esteem, academic achievement, and motivation (Anderman & Freeman, 2004; Osterman, 2000; Whitlock, 2006), whereas low levels of school connectedness have been associated with depressive symptoms in adolescence (Shochet, Dadds, Ham, & Montague, 2006). School connectedness has also been found to serve as a significant protective factor against various negative behavioral outcomes in adolescents, including interpersonal violence, substance use, and school dropout (Henrich, Brookmeyer, & Shahar, 2005; Ozer & Weinstein, 2004).
School connectedness may also serve as a protective factor guarding against the development of depressive symptoms following interpersonal trauma. For instance, Ozer and Weinstein (2004) found that perceived school connectedness with teachers had significant protective effects in the relationship between exposure to interpersonal violence and specific dimensions of psychological functioning. We therefore expect to find that school connectedness is negatively associated with depressive symptoms and that it moderates the negative consequences of interpersonal trauma exposure for early adolescents.
Gender Differences and the Role of Potential Protective Factors
Early research exploring social support and connectedness among adolescents found consistent gender differences, with adolescent girls reporting consistently higher levels of nonfamily social support (e.g., school personnel and peers) than boys (Vaux, 1985). While these general gender differences in the levels of parent and school connectedness have not been consistently supported in more recent studies, possible gender differences in the effects of social support from parents and the school environment on adolescent well-being following interpersonal trauma is an important aspect to consider. Separate studies have found positive social support immediately following trauma to be correlated with decreases in internalizing symptoms in adolescent girls (Bal et al., 2005) and reduced the risk of delinquency and violent behaviors in adolescent boys (Maschi, Bradley, & Morgen, 2008). Research is needed that explores the potential gender differences in the effects of parent and school connectedness among adolescents with early life interpersonal trauma exposure.
Statement of the Problem
The purpose of the current study is to provide a better understanding of the key factors that mitigate the relationship between early life interpersonal trauma experiences and depressive symptoms in early adolescence. Although prior studies have examined the effect of parent and school factors on adolescent mental health following specific types of traumatic violence (e.g., Henrich et al., 2005; Ozer & Weinstein, 2004), research has not yet explored these factors following cumulative interpersonal trauma exposure in a large, population-based urban sample of youth in early adolescence. Further, prior studies have not examined how parent and school connectedness may moderate depression for early adolescent boys and girls following a broad range of interpersonal traumas in early life. The primary objective of this article is to examine how perceived parent and school connectedness moderate the effects of cumulative interpersonal trauma exposure on depressive symptoms among a nonclinical sample of seventh-grade students. It is expected that greater perceived social support, through connectedness to parents and school, serves as a protective factor against depressive symptoms in early adolescent boys and girls.
Method
Sample
The sample includes seventh-grade students enrolled in an urban school district in a state in the South Central United States (N = 1,736). Because of low levels of missing values (percentages missing range from 0.9 to 2.8) and because no systematic patterns were detectable using Bonferroni adjustments, missing values were considered missing completely at random and treated using listwise deletion. Listwise deletion is considered a nonbiased means of handling missing data when missing completely at random is a legitimate assumption (Allison, 2002). This resulted in a final sample of 1,615 participants in the current study, including 779 boys and 816 girls. Participants were racially/ethnically diverse (43% Hispanic, 32% Black, and 22% White; “other” students were removed from the sample due to small cell counts).
Procedures
The University’s Office of Research Compliance; the public school district’s Planning, Research, and Evaluation Department; and the principal of each school reviewed the study protocols and granted permission to conduct the study, which included the approved parent consent and adolescent assent forms. Parental permission forms were sent home for parents to review, and copies of questionnaires were available at local libraries and at the school offices, as well online for parents to view. A passive parental consent process required parents to return the permission form only if they did not want their child to participate. All students whose parents did not object to their participation, and were present and gave assent to participate the day of data collection at each school were surveyed, resulting in a participation rate of 98% of seventh-grade students present the day of data collection and a total response rate of 83% of all possible seventh-grade student participants. Data were collected from 12 schools over a 2-week period in May 2009 using standardized self-report surveys in English or Spanish. Forty-two students (2.41%) completed the Spanish version. Students completed all surveys during a regular class period. Students who did not participate were sent to the school libraries or computer labs during data collection. Questions were read to students to avoid confounding due to literacy. Students with learning disabilities severe enough to be exempt from annual end of instruction exams were excluded from the study. Students were orally debriefed following completion of research procedures and received US$5 each for participating in the study.
Measures
Early life interpersonal trauma exposure
Trauma exposure was measured using a seven-item modified version of the Traumatic Events Screening Inventory–Child Report Form (TESI-CRF; Ribbe, 1996). The modified inventory included seven items assessing interpersonal traumatic life events: crime-related events (i.e., witnessed mugging, stabbing), interpersonal violence (i.e., assaulted with a weapon, domestic violence), and loss of a caregiver. Specific items are listed in Table 1. The response set was “Yes” and “No.” Items were reverse-coded and summed to compute a cumulative early life interpersonal trauma exposure score ranging from 0 to 7 with higher scores indicating greater trauma exposure.
Means and Standard Deviations of Study Variables by Gender (N = 1,615).
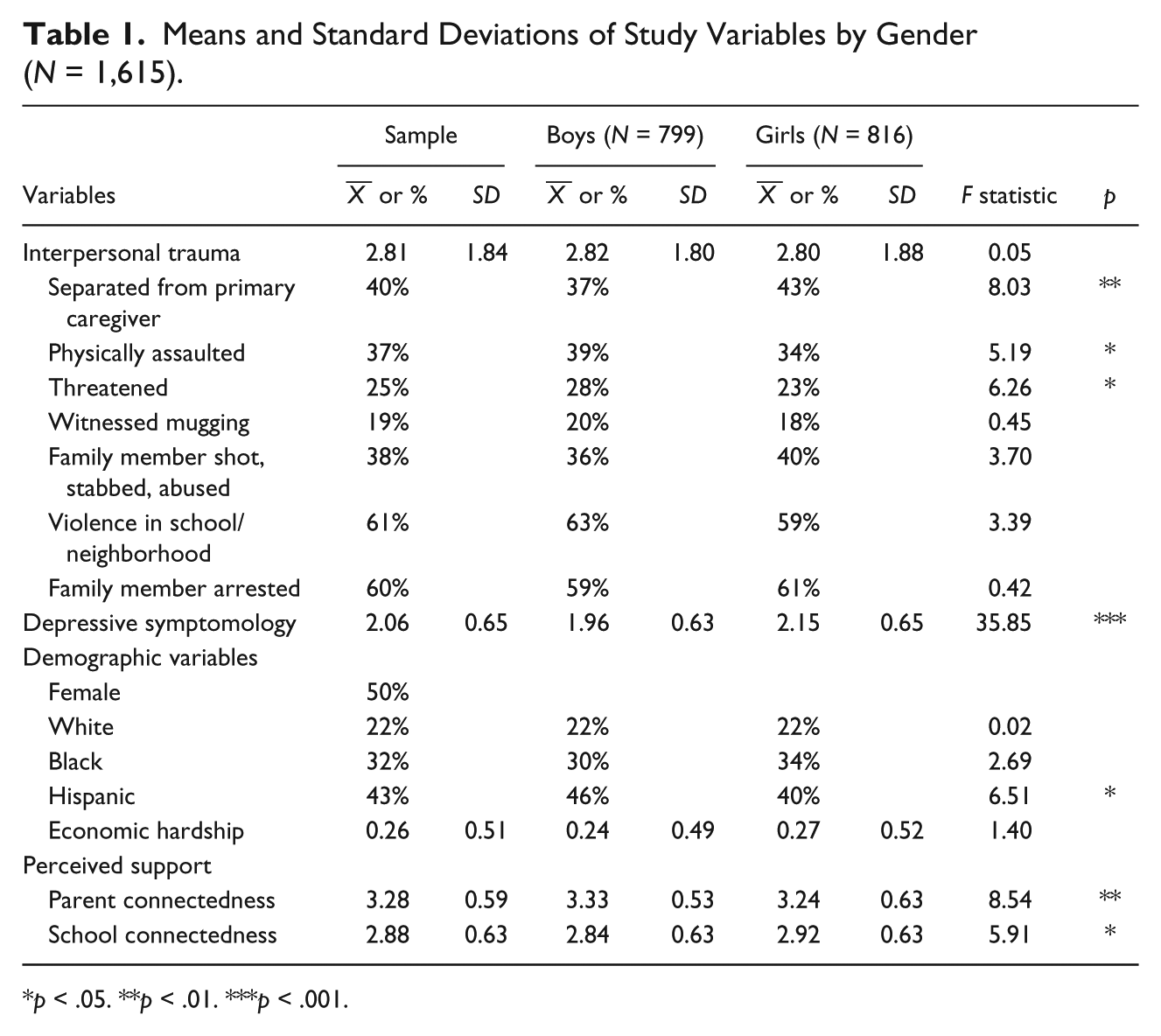
p < .05. **p < .01. ***p < .001.
Depressive symptoms
As the primary outcome variable, depressive symptoms were assessed using the 10-item version of the Center for Epidemiologic Studies–Depression Scale (CES-D; Andresen, Malmgren, Carter, & Patrick, 1994). The 10-item version of the CES-D has acceptable validity and reliability among adolescents and has been used in numerous community samples (e.g., Bradley, Bagnell, & Brannen, 2010; Cheung, Liu, & Yip, 2007). The measure asked respondents to identify how often in the past 2 weeks they agreed with the statements, which included items such as “I felt depressed,” “My sleep was restless,” and “I felt that everything I did was an effort.” The 10-item CES-D was measured on a 4-point Likert-type scale with responses ranging from 0 (never/rarely) to 3 (most/all the time). Items were coded or reverse-coded, so that higher scores indicate more depressive symptoms. The means of at least seven available items were utilized to create a scale ranging from 0 to 3 and then logged to reduce the effects of outliers. Internal consistency for the scale was α = .76.
Social support
Parent connectedness was assessed with four items adapted from measures of parental care and support used in prior survey research with adolescents (Resnick et al., 1997). The items included the following statements: “My parents/guardians know how I think or feel about things important to me”; “In general, my parents/guardians know where I am and what I am doing”; “I feel important to my parents”; and “My parents/guardians talk to me about drugs and alcohol.” The items were designed to capture the adolescents’ perceptions of the quality of the relationships with their parents and the extent to which their parents care and support them. Responses ranged from strongly disagree to strongly agree. Items were coded or reverse-coded, so that high scores indicate greater parent connectedness, and a scale was created with mean scores on at least three items ranging from 1 to 4. Cronbach’s alpha for the items was .72.
School connectedness was measured by four items assessing students’ feelings regarding a range of school climate issues, including perceived safety and satisfaction of their schools. Items include “I feel close to people at this school,” “I feel happy to be at this school,” “I feel safe at this school,” and “I feel like I am part of this school.” A similar measure has been used in previous studies to assess youth’s perceived school connectedness (McNeely, Nonnemaker, & Blum, 2002). Scores on each item ranged from 1 (strongly disagree) to 4 (strongly agree), and a scale was created using mean scores on at least three items, also ranging from 1 to 4. These four items formed an internally consistent scale, α = .77.
Demographic and control variables
Race was assessed using one standard question: “With which race/ethnicity do you most closely identify?” Dummy variables were constructed for African American, Hispanic, and Other compared to White, the reference category. Due to small cell counts, youth reporting “other” racial/ethnic category were subsequently dropped from the sample. Gender was coded as “1” Female and “0” Male. Economic hardship was assessed using three modified questions from the 1990 survey of Work, Family, and Well-Being (WFW; Ross & Wu, 1995) and the 1995 Survey of Aging, Status, and Sense of Control (ASOC; Mirowsky & Ross, 2005). Specific questions included the following: “In the past year . . . Did your family go without meals?” “Did you receive welfare or assistance from church or community organizations?” and “Did you live outdoors, in a shelter, or a transitional housing facility?” The response set was “Yes” and “No.” Items were summed to construct a scale from 0 to 3, with higher scores indicating more economic hardship.
Analytic Strategy
Linear regression models were used to examine the associations between cumulative trauma exposure, social support, and depressive symptoms for early adolescent girls and boys. Table 1 estimated mean differences by gender for the study variables using F tests. Table 2 examines the bivariate correlations of the study variables. We then ran a series of linear regression models to assess the relationships between study variables and early adolescents’ reports of depressive symptoms. Interpersonal trauma, demographic characteristics, and social support variables (parent and school connectedness) were mean-centered for the analyses, and the dependent variable (CES-D scale) was log transformed to reduce the impact of outliers on results. Model 1 includes only the trauma and demographic variables. Model 2 added the social support variables. The two-way interactions between interpersonal trauma and social support were tested in Model 3, and Model 4 includes a three-way interaction between interpersonal trauma, gender, and social support (parent connectedness and school connectedness were examined in separate three-way interactions).
Correlation Matrix of Study Variables (N = 1,615).
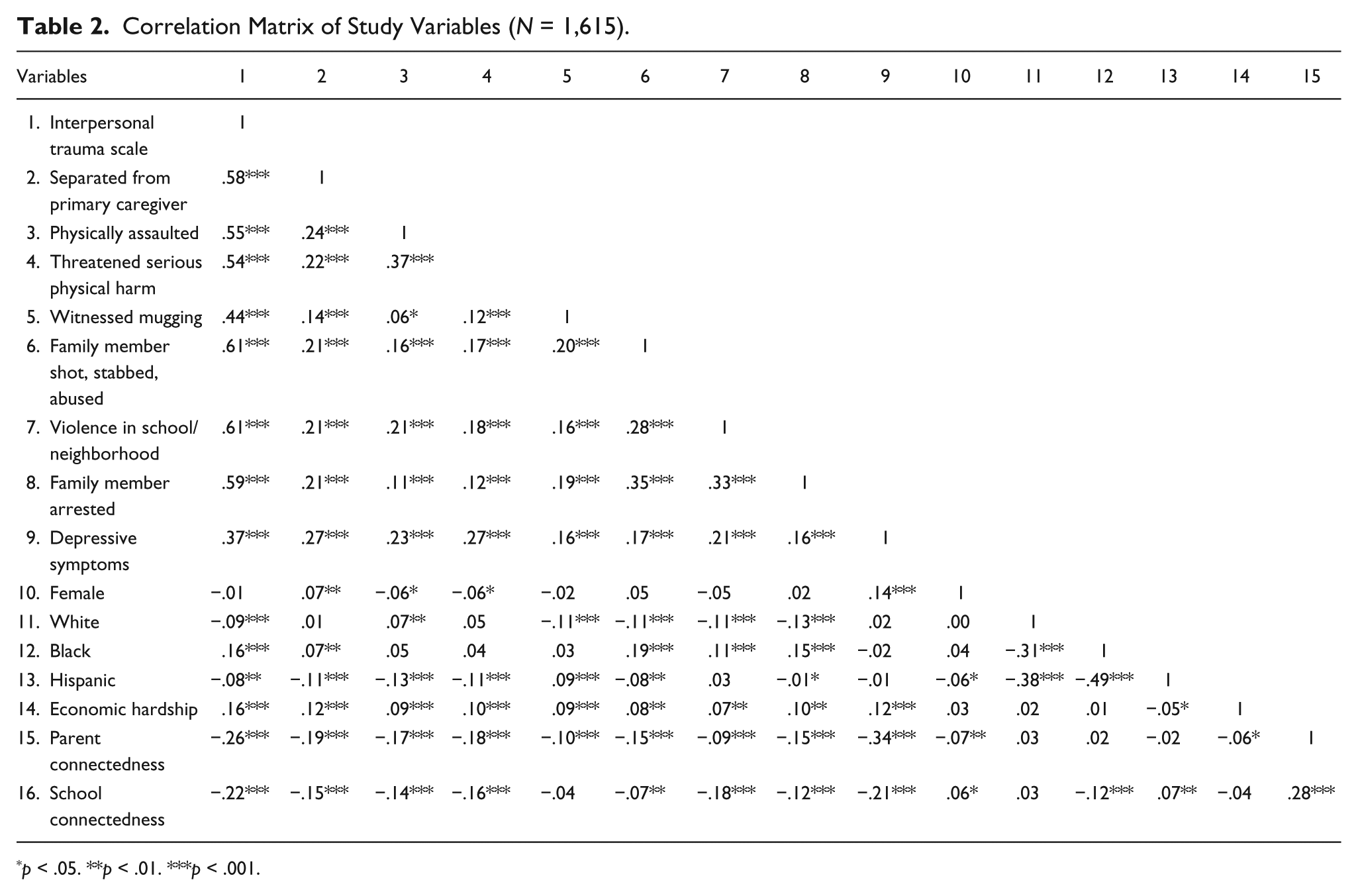
p < .05. **p < .01. ***p < .001.
Results
Table 1 lists the percentages/means and standard deviations for the variables in this study for the full sample and by gender. A majority of the sample (87.5%) reported experiencing at least one early life trauma that was interpersonal in nature, with students in our sample averaging nearly three traumatic events. Of those reporting a traumatic experience, 40% reported being separated from a primary caregiver; 37% reported having been the victim of previous physical assault; 25% had been threatened with serious physical harm; 19% had been present when someone was mugged; 38% had witnessed a family member being shot, stabbed, or violently abused; 61% reported having seen or heard interpersonal violence in their school or neighborhood; and 61% had witnessed a family member being arrested.
While findings suggest no significant differences between boys and girls in the number of overall interpersonal trauma experiences, consistent with previous studies (Breslau, 2001; Flett et al., 2004; McGruder-Johnson et al., 2000), girls reported significantly more experiences with traumatic separation from a caregiver (43% vs. 37%), and boys reported significantly more experiences with being physically assaulted (39% vs. 34%) and threatened of serious physical harm (28% vs. 23%). Findings also indicate significant differences between boys and girls in depressive symptoms and levels of parent and school connectedness; girls reported significantly higher levels of depressive symptoms and school connectedness, whereas boys reported significantly higher levels of parent connectedness.
Table 2 presents the bivariate correlations between all study variables. Results indicate significant positive correlations between the various trauma experiences, indicating that youth who experience one type of trauma are more likely to experience other types as well. Cumulative trauma exposure is significantly associated with depressive symptoms, racial/ethnic minority status, economic hardship, and lower parent and school connectedness, but not gender. Gender is significantly correlated with the type of social support; girls report significantly more school connectedness, while boys report significantly more parent connectedness.
Early Life Interpersonal Trauma and Depressive Symptoms
Table 3 presents results of linear regression analyses conducted to examine differences in depressive symptoms depending on trauma experience, demographic characteristics, and perceived social support. Results of Model 1 indicate that greater interpersonal trauma experience is associated with significantly higher depressive symptoms for early adolescents. Girls also reported significantly higher depressive symptoms, and compared to White students, Black students reported significantly lower depressive symptoms, and there were no significant differences for Hispanic students. Greater economic hardship was associated with higher depressive symptoms. Model 2 included perceived social support from parents and schools. The associations for trauma exposure and demographic variables remained the same, and both higher parent connectedness and school connectedness were associated with significantly lower depressive symptoms.
Multiple Linear Regression Analysis of Depressive Symptomology by Cumulative Interpersonal Trauma, Demographic Characteristics, and Social Support (N = 1,615).
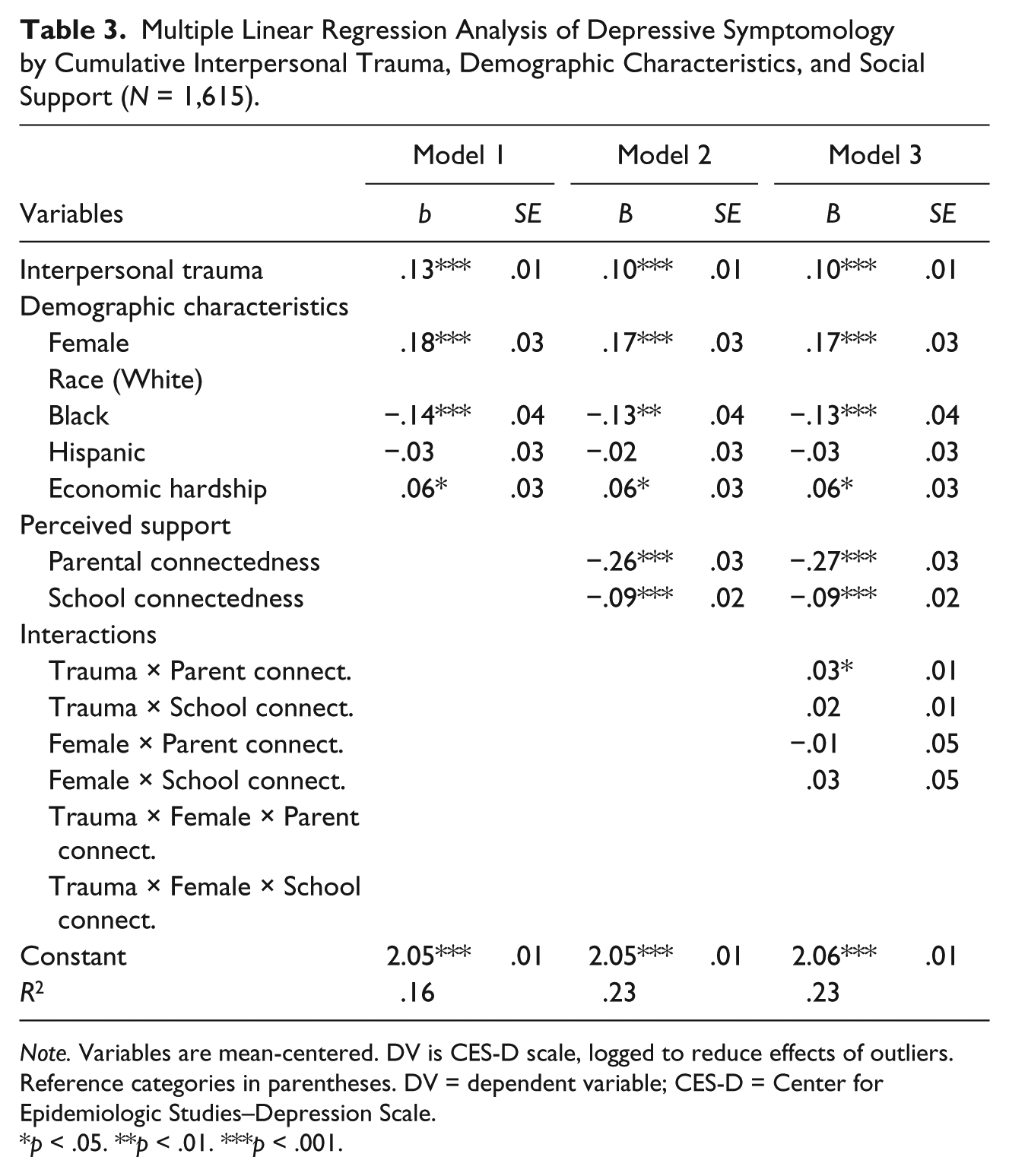
Note. Variables are mean-centered. DV is CES-D scale, logged to reduce effects of outliers. Reference categories in parentheses. DV = dependent variable; CES-D = Center for Epidemiologic Studies–Depression Scale.
p < .05. **p < .01. ***p < .001.
Model 3 included two-way interactions between interpersonal trauma experiences and parent connectedness and school connectedness, as well as gender and parent connectedness and school connectedness, respectively, to test for protective effects of social support for early adolescents who have experienced interpersonal trauma and for gender differences. There was a significant positive interaction between interpersonal trauma and parent connectedness, but the interaction between interpersonal trauma and school connectedness did not reach significance. Figure 1 shows the moderating effects of low (−1 SD below the mean) versus high (+1 SD above the mean) parent connectedness on the relationship between interpersonal trauma and depressive symptoms. Additional analyses of simple slopes (Aiken & West, 1991) revealed that adolescents who experienced more trauma reported higher depressive symptoms, but the association was stronger for youth with higher levels of parent connectedness (β = .30 vs. β = .06; both p < .01). As the figure shows, higher parent connectedness was more protective against depressive symptoms at lower levels of trauma exposure compared to high levels of trauma.

Moderating effects of parent connectedness on early adolescents’ depressive symptoms (CES-D, log transformed) by trauma history.
Model 4 included a three-way interaction between interpersonal trauma, gender, and social support (parent connectedness and school connectedness, respectively). Neither of the three-way interactions was significant, suggesting that the combined effects of trauma and connectedness do not vary by gender.
Discussion
We examined the associations between early life interpersonal trauma experience and depressive symptoms among a district-wide sample of seventh graders in an urban school district in the South Central United States. Results indicate that experiences with early life interpersonal traumatic events are common among this population; similar to previous studies (Mazza & Reynolds, 1999), the large majority of students in our sample (87.5%) had experienced at least one traumatic event, with students averaging nearly three interpersonal traumatic events. While there were some differences in regard to type of interpersonal trauma experienced by gender, overall levels of trauma exposure were not significantly different for boys and girls. Consistent with previous studies, we found gender differences in depression rates; girls reported significantly greater depressive symptoms than boys. We also found differences in perceived social support; girls reported greater school connectedness, whereas boys reported greater parent connectedness.
The associations between interpersonal trauma, perceived social support, and level of depressive symptoms in the current study offer interesting insights. As expected, we found that the experience of early life traumatic events is associated with higher levels of depressive symptoms and that greater parent and school connectedness is associated with lower levels of depressive symptoms for early adolescents. Two-way interactions and tests of simple slopes found that youth who report greater parent connectedness do not report significantly higher depressive symptoms; however, higher parent connectedness was more protective against depressive symptoms at lower levels of trauma exposure compared to high levels of trauma. The three-way interactions did not find significant gender differences.
Results from the interaction and tests of simple slopes indicate that adolescents with lower levels of trauma exposure are at greater risk for higher depressive symptoms when they have lower levels of parent connectedness. We did not find a buffering effect of parent connectedness for adolescents with greater trauma exposure. Though this finding seems counter-intuitive, it is consistent with prior research indicating that at high levels of risk (e.g., higher cumulative trauma exposure) protective factors are overwhelmed (Li et al., 2007; Luthar, Cicchetti, & Becker, 2000). For example, Li and colleagues (2007) found a similar pattern in an interaction between exposure to violence and family support on youth internalizing symptoms; at low levels of violence, internalizing symptoms were lower when family support was higher, but the effect of family support reversed for youth exposed to greater violence. They referred to this as “overwhelming-risk.” However, given the low number of adolescents in the current study who reported high levels of trauma exposure, it is also likely that the slopes of the lines are driven by those youth with lower levels of interpersonal trauma exposure.
Still, the results from this study have several important implications for practice and research. First, findings within the current study reconfirm the high level of exposure to potentially traumatic events among young urban adolescents and indicate that early adolescence may be too late for some preventive efforts and certainly not too early for intervention. The strong positive association between interpersonal trauma exposure and depressive symptoms among the youth in our study highlights the necessity of assessing for interpersonal trauma exposure when trying to understand and reduce the occurrence of depressive symptoms in early adolescence. Additionally, it brings to attention the necessity of considering various protective factors in addition to social support, which may buffer the psychological consequences associated with certain levels of trauma.
Second, our findings suggest that more attention is needed for those early adolescents who have been exposed to high levels of interpersonal trauma. Perceived social support did not continue to protect against the negative mental health consequences of trauma exposure among those with high levels of exposure. Exposure to multiple, repeating interpersonal traumas, particularly in childhood, has been proposed to result in complex, severe psychological symptoms (Briere & Scott, 2006; Cook et al., 2005). Referred to as complex traumas, these traumatic events often occur within the context of a child or adolescent’s relationship with a primary caregiver. The interpersonal nature of complex trauma often leads to maladaptive functioning in multiple domains, including cognitive, behavioral, psychological, and most importantly affective and social (Cook et al., 2005). Girls and boys in early adolescence who have been exposed to complex trauma experiences may need additional supports, such as therapeutic or psychiatric, to reduce depressive symptoms. This suggests the importance of a screening mechanism to identify children who might need additional services so they do not fall victim to the negative effects of complex, interpersonal traumas.
Limitations and Recommendations for Future Research
While the use of a large, diverse, nonclinical, population-based sample of early adolescents (median age of 13) increases the utility of the findings, several limitations of the current study need to be taken into account when interpreting the findings. First, the current findings are solely based on self-report measures, which may be biased. Prior research suggests that children exposed to trauma may underreport or report more socially desirable responses when self-report measures are used (Sawyer, Bradshaw, & O’Brennan, 2008). Second, recognizing gender differences in psychopathology, with externalizing problems more prevalent in boys (Pine & Cohen, 2002) as well as the widespread consequences of complex interpersonal trauma (Briere & Scott, 2006; Cook et al., 2005), it is possible that the current measure may not have picked up on the primary psychological symptoms among boys or complex trauma survivors. Future studies would benefit from the use of additional measures to capture various domains of depressive symptoms and maladaptive coping. Additionally, the use of limited four- and six-item scales to assess parent and school connectedness may not fully capture the connections between youth and their parents and social environments. For adolescents who have experienced long-standing interpersonal trauma within the family, the social support relationships thought to serve as potential protective factors may in fact present additional risk and impact parent connectedness and depressive symptoms. Future studies should include more thorough measurement of parent and school connectedness, as well as other protective factors to assess possible causal mechanisms and guide interventions that reduce depressive symptoms following trauma exposure. Finally, although theory suggests that exposure to trauma leads to mental health symptomatology such as depression, this study’s use of a cross-sectional design cannot rule out that the reverse is true. Thus, the relationships found cannot be considered causal and an alternative interpretation to the findings cannot be ruled out. It is equally plausible that depression causes lower perceived parent or school connectedness. Additionally, it is plausible that the interactions might be more powerful when predicting changes in depression, given that depression begins to emerge during this age period (Hankin et al., 1998). Future longitudinal research is needed to fully understand the factors that increase risk and resilience for adolescents who experience trauma, as well as the causal mechanisms linking trauma exposure, social support, and depressive symptoms over time.
Conclusion
The current study of a large, diverse sample of seventh-grade students expands on previous research using smaller, homogeneous samples and explores the relationship among early life trauma, parent and school connectedness, and levels of depressive symptoms among young adolescent boys and girls. Findings suggest that early life trauma is common among young urban adolescents, and cumulative exposure is associated with greater levels of depressive symptoms. Greater parent and school connectedness are associated with lower depressive symptoms for early adolescents. However, the protective effect of parent connectedness is diminished at high levels of trauma exposure. Interventions may target building parent and school connectedness for prevention and intervention in an effort toward reducing depression in early adolescence, but additional work is needed to identify mechanisms that promote resilience among girls and boys with high levels of early life interpersonal trauma exposure.
Footnotes
Authors’ Note
An earlier version of this article was presented at the 2010 National Council on Family Relations Annual Conference in Minneapolis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided in part by the College of Human Sciences, Oklahoma State University.