
Abstract
This article’s aim is to examine correlates of middle school students’ body mass index (BMI). Little research simultaneously has considered both child and parent correlates in predicting child’s BMI; we examine the interrelationships between middle school students and their parent’s risks and protective factors and their impact on the child’s BMI. The study is based on a cross-sectional survey of 161 parent-middle school child pairs living in a large school district in Northwest Arkansas. The analysis finds that while parent BMI is an important correlate of student BMI, other parental risks and even parental protective factors’ impact on student BMI were, in part, minimized by the risk and protective factors of students. Important differences emerged between parent and child correlates of student’s BMI scores. More comprehensive joint assessments of parent and child social contexts and their role in determining weight status seem clearly warranted from this exploratory analysis.
Keywords
Introduction
Childhood obesity is a growing public health problem due to its connections with a number of health risks such as diabetes, hypertension, and heart disease (Freedman, Mei, Srinivasan, Berenson, & Dietz, 2007; Schwimmer, Burwinkle, & Varni, 2003). Currently, more than one in three school-aged children in the United States are overweight and nearly one in five are obese (Ogden, Carroll, Kit, & Flegal, 2012). Although it has been documented that the family plays an important role in exacerbating and/or moderating health behaviors and food choices leading to significant weight gain in children (Fisher, Mitchell, Smiciklas-Wright, & Birch, 2002; Gibson, Wardle, & Watts, 1998), few studies have taken the next step and examined the role of parents’ health and social contexts on their children’s body mass index (BMI) (Davison & Birch, 2001; Gable & Lutz, 2000). In addition, even fewer health-focused studies have examined both child and parent contexts as determinants of childhood obesity, despite evidence suggesting that parents and children may experience their food environments in qualitatively distinct ways (Fram et al., 2011; Hadley, Lindstrom, Tessema, & Belachew, 2008) and that children’s self reports of stressors, peer relationships, and resources can be important predictors of obesity (Fitzpatrick, Willis, & O’Connor, 2014; Lohman, Stewart, Gundersen, Garasky, & Eisenmann, 2009). This gap in the literature is ripe for the type of empirical inquiry presented in this study. Moreover, this focused work in Northwest Arkansas is particularly poignant given that the state of Arkansas is ranked third in the United States for state-level obesity rates (Trust for America’s Health and Robert Wood Johnson Foundation, 2013).
Broadly, this study builds on the theoretical frameworks of two sociological approaches for understanding health in a developmental context. First, we borrow the notion that our social worlds and connections are evolving and, therefore, distinct during various points in life from the life-course perspective (Umberson, Crosnoe, & Reczek, 2010). Unlike many who work from a life-course perspective, our data are not longitudinal. However, from this fundamental idea that our social worlds change throughout our lives and that the types of salient social ties may shift during these changes, we can begin to understand the methodological and theoretical importance of collecting data from both children and their parents rather than making inferences about child health from information only parents have reported. Parents and children share many aspects of their social worlds; yet, their experiences, social locations, and their worlds are not the same. Thus, any comprehensive understanding of childhood obesity will be more complete when both experiences are taken into consideration.
Moreover, the framework of this study, and subsequent method of data collection and analysis, respects the agency of the child as an actor within constraining, and sometimes enabling, social structures, rather than characterizing them as wholly passive components caught up within larger social machinery controlled or manifested solely by their parents. Parents can be reliable spokespersons for their children when they are younger, but as they age, they start to acquire friendships and resources outside of the family context (Umberson et al., 2010); thus, the reliability of parents acting as respondents for their children likely decreases as the child’s age increases. Previous work on the discordance between ratings of health-related quality of life among parents and children suggests that differing responses are primarily due to different experiences and reasoning between parent-child pairs, not different interpretations of the question (Davis et al., 2007). Developmentally, adolescents are beginning to articulate clear ideas about what is important to them and what impacts them directly beyond their parents’ context.
The second important framework utilized for this study is social capital theory. Social capital, as an individual’s resource, has been defined as “the aggregate of actual or potential resources linked to possession of a durable network” (Bourdieu, 1986, p. 248). The central idea of social capital theory is that within our relationships lie varying degrees of value; resources are embedded in, and flow through, these social networks characterized by varying norms and levels of trust (Lin, 1999). Coupled with a life-course perspective, social capital theory highlights, again, the value of social relationships as well as the periods in life that may be distinct in the type of relationships that matter most. For example, advanced social network analyses have already provided compelling evidence that (among adults) obesity spreads through social networks and travels more effectively across ties that are characterized by esteem; that is, if you identify someone as a friend but they do not identify you as one, then their weight is more likely to affect you rather than vice versa (Christakis & Fowler, 2007). Simply put, the people we call friends play a significant role in our weight status. However, as social capital theory and the life-course perspective, together, would suggest; relationships change, and so do the directions and locations of esteem (Umberson et al., 2010). With this in mind, for children and particularly pre-adolescents, obesity may become a question of how well connected they are to their peers—the focus of our present study—rather than a question of how well connected their parents may be.
Given these theoretical backdrops, two primary research questions are explored in this study:
In other words, is there reason to argue we should be moving beyond the trend of exclusively collecting parent survey responses without directly asking children any questions themselves? Is there something unique about the social experiences and contexts of children entering into adolescence, which can provide additional insight into understanding their weight status? We argue that child responses are likely to be better predictors of children’s BMI because their responses more closely reflect their own unique experiences and reasoning, as others have shown with certain health-related measures (Davis et al., 2007). When interested in a child outcome, measures most proximate to the child’s own experiences are likely to be the better predictors.
In an effort to answer these questions, we analyze the role of parents’ BMI, sociodemographic factors, and social capital, along with children’s self-reported social capital and sociodemographic factors in determining child BMI scores. We argue that there is a clear need to include self-reported data from children in future research—at least by the time they are in middle school and developing into adolescence. As Lohman et al. (2009) suggested in their previous obesity research, it is during this time in the life course that the social worlds/contexts and peer networks of adolescents are becoming increasingly crucial to their everyday lives and decision-making processes.
Childhood obesity has been associated with a number of parent-related risk factors—parent BMI, social class (Gable & Lutz, 2000), and food insecurity (Casey et al., 2006). We include these previously explored risk factors in the present study. However, we explicitly distinguish some of them as potential risk factors—parent BMI and food insecurity—while categorizing others as primarily sociodemographic/control factors (i.e., social class). Although we build on previous work, we are also entering slightly uncharted territory with our exploration of using the exact same indicators for children and parents; thus, we explore each of these explanatory parent indicators for children as well—excluding child BMI, of course, which is the dependent variable.
Among sociodemographic factors, previous studies lead us to hypothesize that subjective class will be negatively associated with BMI—As perceived social class of children and parents increases, the BMI of the child is expected to decrease (Fitzpatrick et al., 2014; Goodman et al., 2001). We hypothesize positive relationships between each of the three risk factors—parent BMI, parent food insecurity, and child food insecurity—and child BMI scores. In addition, we also hypothesize that among sociodemographic and risk factors, children’s own reports of their social context will have stronger predictive value than reports from their parents. Again, we make the argument, as others have (Umberson et al., 2010), that early adolescence is a particularly vulnerable period of development when youth are beginning to establish their own peer relationships in different social contexts than their parents. This matters for child obesity because risks and resources important to weight status may be embedded within these peer relationships of which only children themselves have a proximate experience and knowledge.
In addition to risk factors, research suggests that there are also social resources that can protect children against negative health outcomes like obesity (Fitzpatrick et al., 2014). Thus, we also consider protective factors related to parental context that have been significant in previous research on childhood nutritional health and obesity, including indicators of a healthy parent lifestyle (Fogelholm, Nuutinen, Pasanen, Myöhänen, & Säätelä, 1999), as well as a measure of their social capital (De Silva & Harpham, 2007). We also contribute to this extant research a new and insightful consideration of child indicators of healthy lifestyle and social capital alongside the parent indicators of protective factors. We hypothesize each of these protective factors—parent healthy lifestyle, child healthy lifestyle, parent social capital, and child social capital—to have negative relationships with child BMI. In addition, as with our risk factors, we hypothesize that protective factors reported by the children themselves should have a stronger predictive value for child BMI scores than will parent resources.
Method
A major methodological strength of this study—the simultaneous examination of parent and child responses to the same questions—permits substantive theoretical insights into any distinctive, or similar, roles that parent and child contexts may play in the formation of weight status outcomes—an area largely ignored by a voluminous health literature even while there is empirical support for its importance (Davis et al., 2007; Eiser & Morse, 2001). The major limitation of previous obesity research has been its nearly exclusive use of parent self-reporting, gaining child information either from only the parents, or only including observational or outcome-related data from the children (Gable & Lutz, 2000), thus ignoring the food-related experiences and perceptions of children themselves which have been found to be significant in previous research (Fitzpatrick et al., 2014; Fram et al., 2011).
Participants
Cross-sectional data were collected from fifth- to seventh-grade students in a local middle school located in Northwest Arkansas. A letter was sent home informing parents of the upcoming survey. Data were collected in fall 2012 with 361 students enrolled in these grades at the time of the survey. Three hundred thirty-four surveys were completed in 15 classrooms (92% completion rate). The 8% of students not completing surveys were either absent because of illness or some other excused absence. Only 3 students refused to complete the survey. Approximately 65% of all students in the surveyed school were free/reduced lunch eligible compared with 56% in the school district, though that number is lower for fifth- to seventh-grade students in the surveyed school. When students were asked how they paid for their lunch, 57% of those surveyed responded by saying they received free- or reduced-price lunches at the school. This percentage is also similar to the percentage reported for the entire state of Arkansas’ K-12 student population.
The sub-sample of parent-student pairs used in the present analysis (N = 161) represents approximately half of the original sample. A parent survey was sent home to all 334 households. The content of the parent survey mirrored much of the content of the student survey. As the matched student-parent sub-sample did not represent the entire sample of students, we systematically compared the background characteristics of those students participating along with their parents with those students whose parents did not respond to the survey. In an effort to check for any sampling bias that might have arisen from only certain families responding to the survey, we examined group differences (race, age, gender, free/reduced lunch status, household composition, and Hispanic status) and found that in all of the background characteristics examined, there were no significant differences between the two groups except that a slightly larger number of students whose parents were Hispanic responded to the joint survey. Thus, we concluded that the sub-sample was an unbiased representation of the larger group originally surveyed.
Procedure
All fifth- to seventh-grade students were eligible to participate in the survey. The written survey was read aloud during first period in all 15 classrooms by trained interviewers. Students were asked if they preferred a Spanish version of the survey and were provided one upon request. Teachers were asked not to participate in the administration to increase student’s comfort in answering questions honestly and left their rooms for that period. In a few cases (3), teacher’s aides were made available to assist any special needs students, but trained interviewers were still responsible for the administration of the survey. Students had the freedom to withdraw at any point in the survey simply by raising their hand and asking not to participate. Their decision to opt out of the study was without penalty. This study was reviewed and approved by the University of Arkansas Institutional Review Board including the informed consent procedure used for children under the age of 14.
A self-administered questionnaire was sent home with the students for parents to respond. A Spanish version was sent, in addition to the English written survey, with those students who, after being asked, felt that their parents might prefer the Spanish translation. Parents were given approximately 3 weeks to return the questionnaire and informed consent; those parents who responded in a timely manner were sent a US$25.00 gift card for their participation. Again, despite the incentive, there were no significant differences found between students whose parents participated compared with students whose parents did not. The University of Arkansas Institutional Review Board approved the parent protocol.
Measurement
Child body mass index
Height and weight were self-reported by students, and BMI was calculated per standard definitions and percentage grouping (Strauss & Pollack, 2003). Although subject to some disagreement, studies have found that self-reported height and weight provide accurate assessments for BMI calculations among student-age populations (Centers for Disease Control [CDC], 2010; Goodman, 1999; Kubik, Lytle, & Story, 2005). In 2007, Arkansas passed an act that required that all students (Grades K, 2, 4, 6, 8, and 10) have their height and weight assessed by trained personnel. The state reports these findings in aggregate by grade only; for those students in Grades 4 and 6 in 2011 in the surveyed school (Grades 5 and 7 in the current study), healthy student BMI scores were found in 65% and 61%, respectively. These percentages are very close to what we report in the current study and provide further evidence that self-report height and weight used to calculate BMI scores appear to be valid. There were no significant differences noted in across gender or age groups, so the decision was made to merge all students into a single group.
Parent and child sociodemographic variables
In the current analysis, several sociodemographic variables were introduced. These variables, in many cases, have been discussed elsewhere (Frank, Kerr, Sallis, Miles, & Chapman, 2008; Goodman et al., 2001) as important to determining both child and adult BMI scores. For this analysis, we introduced the following for both students and parents: age (in years), gender (1 = female), and Hispanic origin (1 = yes). In addition, a subjective assessment of student and parent’s social standing/class was used. Both students and parents were asked, “Thinking about the money your family has and the things your family owns, would you think of your family as” upper class = 5, upper-middle class = 4, middle class = 4, middle-lower class = 2, and lower class = 1. This subjective assessment of class provides some insight into how both students and their parents see their family circumstance regardless of objective indicators like income, occupation, and so on, that are often very hard for students to assess accurately and for parents to respond to. A look at the descriptive statistics for this measure suggests students tend to overestimate their social class standing; parents reported lower evaluations of subjective social class than their children.
Risk
Parent body mass index
BMI was mapped using the CDC (2010) charts that provide estimates based on gender and age for parents in the same way that students were assessed. Like students, there were no significant BMI differences across age groups or gender, and thus, parents were treated as a single group.
Parent and child food insecurity
Drawing from the U.S. Department of Agriculture (USDA) food security module, Connell, Nord, Lofton, and Yadrick (2004) used cognitive interviewing methods to develop a module for assessing food insecurity through direct survey of children. Five items from the original USDA module were deemed appropriate for administrating the survey to children. Following the prompt, “Thinking about your experience with food over the past year,” children were asked the following questions: Did you worry that food at home would run out before your family got money to buy more? Did the food that your family bought run out and you didn’t have money to get more? How often were you not able to eat a balanced meal because your family didn’t have enough money to buy food? Did your meals include a few kinds of cheap foods because your family was running out of money to buy food? Have your meals been smaller because your family didn’t have enough money to buy food? Possible responses included “never,” “sometimes,” and “a lot.” These items were coded from 0 to 2 in the order listed, beginning with “never” coded as 0. From these five items, a composite food insecurity scale was computed ranging from 0 to 10; both scales were moderately reliable with a Cronbach’s alpha = .84 (
Protection
Parent and child healthy lifestyles
In addition to food insecurity, both parents and students were asked a series of 10 questions related to healthy eating behaviors in the week prior to the survey. How much (0 = not at all, 1 = 1-3 times, and 2 = 4+ times) they had eaten certain types of foods (vegetables, potatoes, carrots, salads, etc.), drank specific drinks (milk, fruit juice, soda, etc.), had breakfast, and exercised vigorously including physical education (PE) class. The healthy lifestyle scale ranged from 0 to 20; both scales for students and their parents were moderately reliable.
Parent and child social capital
To assess social relationships/friendships, similar social capital indices were developed for both parent and child. The four variables included in the social capital index for students asked the following questions: How often did they see their best friend? How often did they have other types of contact with their best friend? How often did they eat meals with their best friend? and How often did they have meals at a friend’s house? Possible responses for the first three questions included never or hardly ever, several times a year, at least once a month, once a week, several times a week, and every day. These responses were coded from 1 to 6 in the order they have been presented, beginning with “never or hardly ever,” coded as 1 and ending with “every day,” coded as 6. The last question had a different, though similar, set of responses, including never, few times, some of the time, most of the time, and all of the time. These were coded from 1to 5 in the order they are listed, beginning with “never,” coded as 1 and ending with “all of the time,” coded as 5. This left us with a social capital scale ranging from 4 to 24 that was moderately reliable (
Likewise, we asked parents, How often they see their best friend? How often they had other types of contact with their best friend? and How often they ate meals with a friend? Possible responses for these questions included never or hardly ever, several times a year, at least once a month, once a week, several times a week, and every day. These responses were coded from 1 to 6 in the order they have been presented beginning with “never or hardly ever,” coded as 1 and ending with “every day,” coded as 6. A fourth and final question asked parents how many close friends they had. Those responses were broken into five groups ranging from 1 = 2 or fewer close friends to 5 = 10 or more close friends (
Data Analysis
The intention of the analysis for this project was largely exploratory. Although a significant amount of research has examined childhood obesity, few if any studies have developed a systematic pair-approach to looking at both child and parent responses in determining BMI. The analysis provides descriptive statistics for the variables used in the models; ordinary least squares (OLS) regression is the primary analytical tool for this study. A series of regression models are developed where each block of variables (risk and protection) is entered separately to examine the significance of variable groupings for both students and parents. Although we examine these blocks for significant change in R2, we also pay close attention to the differences in individual size and significance of the predictor variables between students and parents. Both standardized and unstandardized regression coefficients are included for each of the predictor variables.
Results
Nearly one third of both parents and students in the sample met the weight status requirements to be considered overweight; parents reported more food insecurity than their children, more social capital, and a less healthy lifestyle. The majority of parent respondents were female (85%) and non-Hispanic (90%). Nearly 4 times the number of parents described themselves as lower class (20.0%) compared with their child (5.5%); the opposite was true for students describing themselves as upper class where 4 to 5 times more often than their parents they described themselves as the same. Overall, this sub-sample was representative of the larger student sample that was acquired; the demographic composition of the sub-sample looks very much like the overall school characteristics and those of the school district for this age group (see Table 1).
Descriptive Statistics for Student and Parent Variables (N = 161).
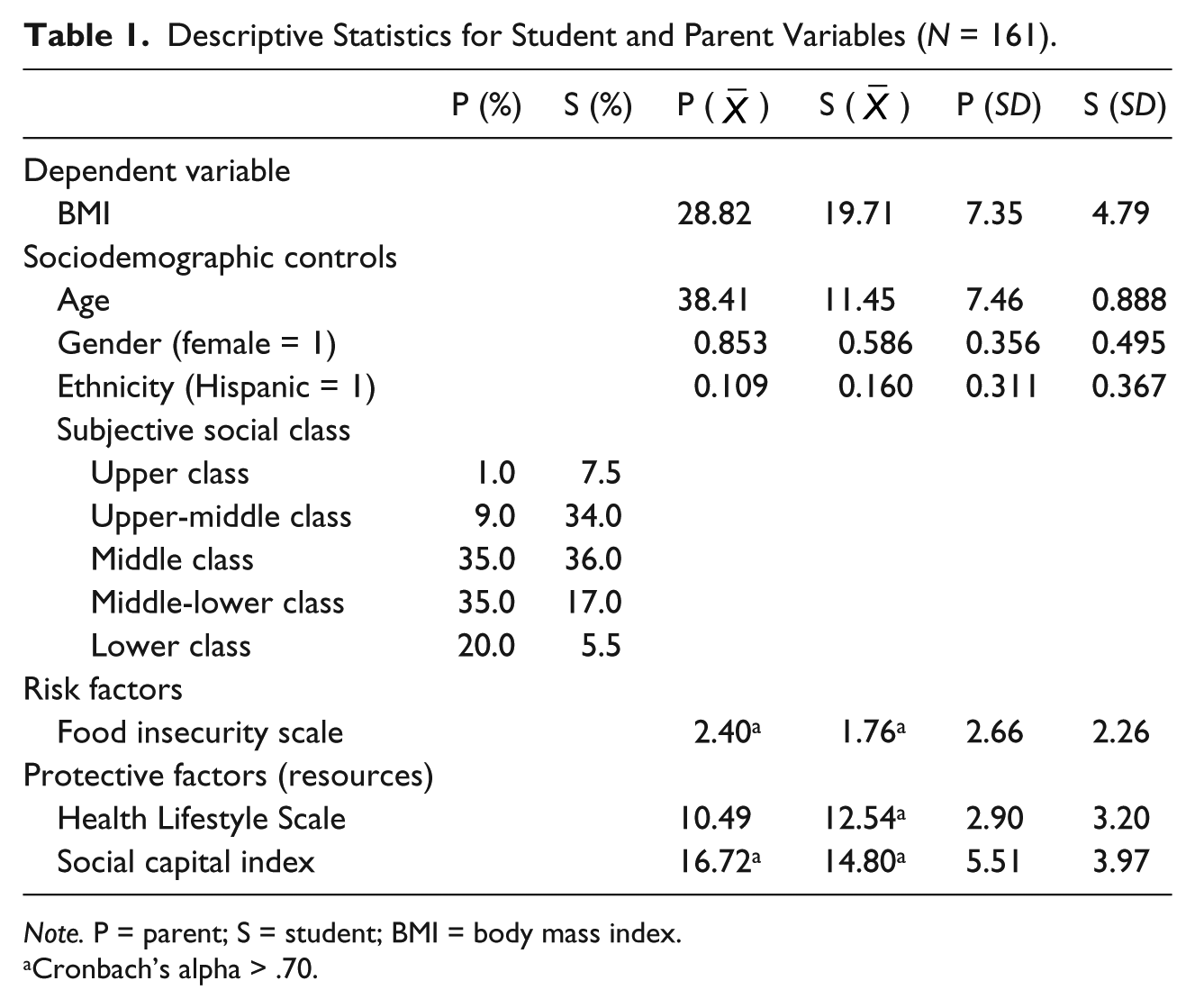
Note. P = parent; S = student; BMI = body mass index.
Cronbach’s alpha > .70.
In an effort to look more closely at the differences between student and parent predictors, the findings are presented in six separate blocks. The first two blocks (Models 1 and 2) of the multiple regression findings (sociodemographic background characteristics) in Table 2 suggest that older parents have a positive impact on their child’s BMI; student’s age was not significant. Like their parents, students with a lower subjective perception of their social class tended to have higher BMI scores. Neither ethnicity nor gender was significant for either students or their parents. Only the student block of sociodemographics (Model 1) showed a significant change in R2.
Child BMI Regression Models.
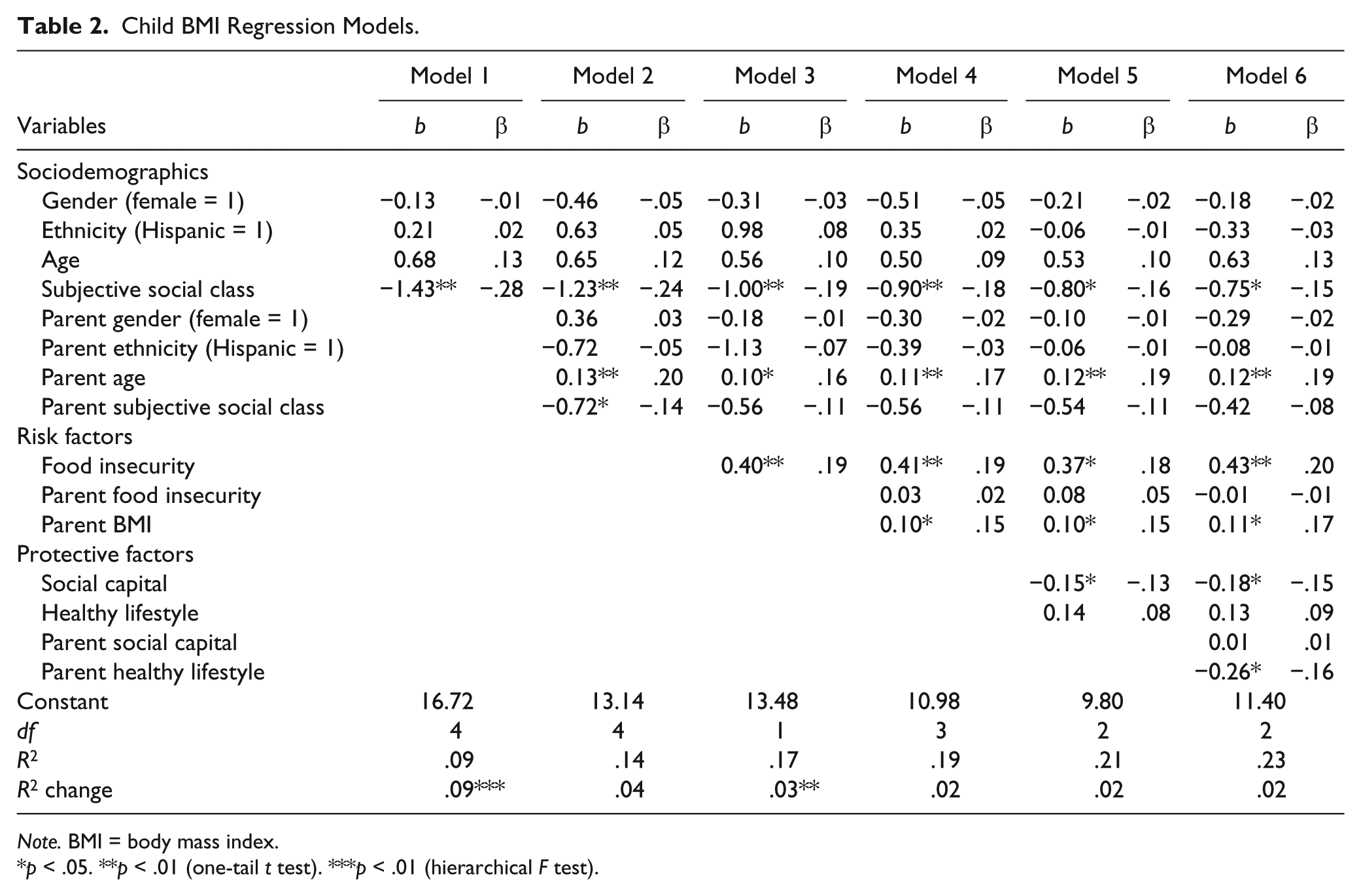
Note. BMI = body mass index.
p < .05. **p < .01 (one-tail t test). ***p < .01 (hierarchical F test).
With regard to risk (Models 3 and 4), clearly parents’ BMI (predominantly mothers) were important correlates of their child’s BMI. Information provided by students regarding food insecurity appeared to be a stronger correlate of their BMI than the food insecurity reported by their parents. For example, Table 2 shows a significant relationship between student’s reports of more food insecurity and higher BMI, while parents’ reports of food insecurity were not significant in the analysis. Overall, we find support for both hypotheses proposed for the influence of risk factors: (a) All of these risk factors are positively associated with child BMI, and (b) student-reported risk factors showed a better predictive value than parent reports in instances where both were measured. Only the student block of risks (Model 3) showed a significant change in R2.
Turning to the resource results (Models 5 and 6), only parent reports of a healthy lifestyle were a significant predictor of child BMI; healthier lifestyles are correlated with lower child BMI scores. Finally, unlike parents’ social capital, students’ social capital was related to lower BMI scores; students with more friends and particular types of support as it related specifically to eating had lower BMI scores than their counterparts. Parents’ social capital, while present, was not significant. Again the amount of resources/capital may not be as important as the type of resources and capital when it comes to determining weight status outcomes. Overall, the results from this model are mixed in their support for the proposed hypothesis, although they generally indicate what we hypothesized. Although all of the resources did show a negative association with child BMI, student social capital had better predictive value than its parent counterpart and parent’s healthy lifestyle was a better protective factor than student’s healthy lifestyle. Although R2 increased with the addition of both sets of protective factors, neither model showed any significant change in the F value.
There was clearly some predictive utility in all three groups of models; successive models increased an R2 of .09% to nearly 23% after all the variables were controlled for. However, while some parent-reported variables (age, BMI, and healthy lifestyle) remained significant predictors even in the final model, only the models including student variables (Models 1 and 3) produced a significant change in R2. Thus, we conclude that significant variation in child BMI can be explained by considering both child and parent contexts of risk and protection.
Discussion
Clearly, childhood weight status develops within the context of the family. Parents’ health lifestyle, their own weight status, and age were related to childhood BMI scores. This finding is important and confirms what others studies have reported (e.g., Gable & Lutz, 2000; Lohman et al., 2009). Perhaps more interesting is that, in some cases, childhood characteristics were more important determinants of BMI than parental ones. Student’s subjective social class, food insecurity, and social capital were all significant correlates of their BMI scores—the equivalent parent variables either lost significance in subsequent models (parent social class) or were not significant in any of the final models (parent food insecurity and social capital). Likewise, age and healthy lifestyle were significant parent variables that were not significant as student-reported variables in the final models.
Previous research that had found no direct relationship between food insecurity and childhood obesity had suspected the non-significance in their analysis might be due to data limitations—only collecting food insecurity reports from parents and not the children themselves (Lohman et al., 2009). Our findings support this earlier suspicion because, as our results show, student-reported food insecurity is a significant predictor of child BMI scores while parent reports of food insecurity are not. Moreover, while the adults in our own study were reporting their own food insecurity—not the food insecurity of their children as was done by Lohman et al. (2009)—it is telling that parents’ experiences with food insecurity did not impact children’s BMI scores while child food insecurity did. One possibility is that a certain amount of the negative influences associated with food insecurity are shielded from the children by their parents—for example, parents might be skipping meals themselves (increasing their level of insecurity) in order to provide more consistent or healthier meals for their children (decreasing their insecurity). This sort of buffering behavior could help explain why parent and child experiences are different, as well as why the consequences of food insecurity might be different in terms of childhood obesity. While a number of studies have produced results that support this idea, the details of this buffering process remain vague and obscure. This is an area begging to be explored further by future research.
The distinctive influences of parent- and child-reported measures on child BMI have several implications for how we understand the internal dynamics of the family as well as family members’ differentiated experiences with food and health. First, our findings support the basic assumptions of the life-course perspective regarding the developing structure of social networks and relationships as people age as well as the idea that people at different ages experience similar worlds differently. Considering this, it is not too surprising that children’s self-reported information often yields better correlates of their BMI than parental reports. Second, these findings complicate further what previous research has found regarding the influences of social capital on health. Although some have found a relationship between parents’ (maternal) social capital and child nutritional health in developing countries (De Silva & Harpham, 2007), we know little about how social capital might influence adolescent health differently when held by adolescents than it does when held by parents. Moreover, the social context of parents and children in the developing world is likely to be substantially different than it is in the United States. Thus, the present study helps fill in some blank spaces in a still incomplete picture of adolescent health by showing that pre-adolescence/adolescence may be a period when the social connections your parents have might matter less than the connections you have with your own friends—This is supported by our results. Finally, the fact that food insecurity is a significant correlate of child BMI when reported by children but not by their parents has multiple implications: First, the distribution of household resources is uniquely experienced by different members of the household; second, children likely have a more accurate understanding of their own experience than their parents do; and third, this supports the continued surveying of both children and their parents in research concerned specifically with adolescent health.
We recognize that despite these promising preliminary findings, this study is not without limitations. Research continues to debate the validity of self-reported BMI, and while our results closely mirror the statewide levels for weight status, we recognize this limitation. As mentioned earlier, the cross-sectional approach is also limiting as we examine developmental changes and their impact on health outcomes. Nevertheless, there is some utility in exploratory examination of these relationships, which provide important findings to consider in any longitudinal work. Finally we recognize that this is a limited sample with limited generalizability. While the results from one school in a single geographic location are limiting, they are not without important utility in advancing our basic understanding of the relationships that we hypothesize regarding student and parent contexts and their impact on student BMI. Even in the context of these limitations, our study provides an important set of findings regarding the role of parents’ and children’s characteristics, social contexts, and their relationship to individual child BMI scores. Although the study design itself provides the strength of paired students and parents, we were unable to match siblings to gain a more complete picture of the household; however, we were able to gain confirmation from the school administrators that very few sibling pairs existed within the grades we had chosen to sample. Overall, the strengths of this study and its unique contributions to the literature on childhood obesity far outweigh its limitations, which certainly could be improved upon by future research.
Study Summary and Future Research
Several important conclusions can be made from the current analysis. First, a significant proportion of variation in childhood obesity can be explained by risk factors like parent BMI or student food insecurity, as well as protective resources such as student social capital or parent healthy lifestyles. Second, and perhaps most importantly, students and parents within the same household have different experiences with social class, food insecurity, and social capital such that these factors only become significant predictors of child BMI when reported by students themselves. This leads into the final conclusion; future research on childhood obesity, and childhood health more generally, must continue to develop ways of surveying children themselves that is age appropriate and meaningfully related to previous scholarship. We hope that the present study has contributed some momentum to the beginnings of this process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.