
Abstract
A systematic literature review was conducted to assess the utility of Positive Youth Development (PYD) concepts in promoting positive sexual health behaviors in young minority adolescents (n = 12 studies). Interventions reported significant associations between PYD-focused interventions and ever having sex, sexual partners in the last 30 days, using protection at the last sexual encounter, and decreased pregnancy rates. Outcomes were reviewed by age, gender, PYD constructs, cultural tailoring of interventions, and retention rates. Few interventions focused exclusively on young minority adolescents. PYD can be an effective tool in promoting sexual health in younger minority adolescents, but additional research is needed to determine beneficial strategies for this age group and timing of interventions. Recommendations for future studies include additional guidance on operationalization of PYD concepts, effective cultural tailoring methods, dosage of intervention components, and de-linking minority status from socioeconomic status (SES) and high-risk behaviors.
Keywords
Introduction
While teen birth rates in the United States have steadily declined since the 1950s (Martin, Hamilton, Osterman, Curtin, & Mathews, 2013), rates in the United States remain higher than most other developed countries (Hamilton & Ventura, 2012). Decreases in teen birth rates have not been evenly distributed. Decreases in birth rates have primarily occurred in older adolescents, with rates largely unchanged for youth ages 10 to 14 years old (Martin et al., 2013). In 2012, the teen birth rate for 15 to 19 years olds was 29.4 per 1,000 females of that age range, which was a 6% decrease from 2011. However, when examined across a larger age range (11-19 years old), teen birth rates increased with age. There were 0.4 births per 1,000 females 10 to 14 years old, 14.1 births per 1,000 females 15 to 17 years old, and 51.4 births per 1,000 females 18 to 19 years old (Martin et al., 2013). Although birth rates were not as high for 10 to 14 year olds, the notable increases with age emphasize the importance of delaying the onset of sexual activity and preventing pregnancy in the 10 to 14 age range.
Racial and ethnic disparities also remain. For adolescents 15 to 19 years old, birth rates per 1,000 females were highest for Hispanic females (46.3 per 1,000), followed by non-Hispanic Black (43.9), American Indian or Alaska Native (34.9), non-Hispanic White (20.5), and Asian or Pacific Islander (9.7) females (Martin et al., 2013). For adolescents 10 to 14 years old, birth rates per 1,000 were highest for non-Hispanic Black (0.8) and Hispanic (0.6) females, followed by American Indian or Alaska Native (0.5), non-Hispanic White (0.2), and Asian or Pacific Islander (0.1) females (Martin et al., 2013). These disparities highlight the need for targeted public health interventions.
Adolescents are also at increased risk of contracting sexually transmitted diseases (STDs). One fourth of sexually active adolescent females are living with an STD. Half of all new cases of STDs are among young people 15 to 24 years old (Centers for Disease Control and Prevention [CDC], 2013). Those who are infected with an STD, such as Syphilis, Chlamydia, or Gonorrhea, have a higher risk of contracting the Human Immunodeficiency Virus (HIV; CDC, 2013). In addition, STDs can result in infertility issues and may cause ectopic pregnancies. Furthermore, minority groups have consistently higher rates of STDs compared with non-Hispanic Whites. Specifically, non-Hispanic Blacks are more likely to be infected with Chlamydia, Gonorrhea, Syphilis, and HIV/AIDS than any other racial group (CDC, 2013). For example, Syphilis rates for 15- to 19-year-old non-Hispanic Blacks are 16 times higher than those of non-Hispanic Whites (CDC, 2013).
Teen births and STDs have significant short- and long-term effects, as well as social and economic consequences. Teen mothers are more likely to drop out of high school and live in poverty (CDC, 2011; Kost, Henshaw, & Carlin, 2010). Moreover, children of teen parents are more likely to drop out of high school, become incarcerated, have more behavioral and medical issues, give birth as a teen themselves, and be less prepared for school (CDC, 2011). Teen childbearing costs taxpayers more than US$9 billion in health care and foster care costs. STDs also cost taxpayers approximately US$16 billion in health care costs per year (CDC, 2013). Thus, sexual activity among adolescents continues to be an important public health issue. Targeting interventions to young adolescents has the potential to delay onset of sexual activity, and decrease the likelihood of negative health, social, and economic consequences (Albert, Brown, & Flanigan, 2003).
One approach to addressing sexual health outcomes in young adolescents is Positive Youth Development (PYD). The PYD approach focuses on foundational, protective factors that help adolescents avoid health-harming behaviors (Catalano, Berglund, Ryan, Lonczak, & Hawkins, 2004). PYD represents a shift in targeting determinants of adolescent behavior by offering researchers and practitioners the opportunity to conceptualize interventions for adolescents by building on strengths or assets. These assets can be targeted in youth, family, and the community to promote the adoption of healthy behaviors (Lerner, Almerigi, Theokas, & Lerner, 2005; Oman et al., 2002; Scales & Leffert, 1999). This approach differs from previous attempts because rather than focusing on diminishing negative attributes or social forces to prevent unhealthy behaviors, it focuses on positive influences to promote healthy behaviors (Lerner et al., 2005). While the distinction at first may seem subtle, the framework of the intervention components and the messages to adolescents and relevant adults are noticeably different. It is the difference between focusing resources to promote youth development compared with preventing youth problem behaviors (Catalano, Hawkins, Berglund, Pollard, & Arthur, 2002). PYD researchers identify skills, personal qualities and competencies, and relationships that are foundational to successful development. In a review of PYD interventions, Catalano et al. (2004) identified 15 constructs that define these skills, qualities, competencies, and relationships (see Table 1). These constructs are then used to design program components that build an internal infrastructure that may help youth to become more resilient and thus more likely to choose health-promoting behaviors (Catalano et al., 2002; Gillham, Reivich, & Shatte, 2002; Lerner et al., 2005). While PYD interventions typically focus on a specific behavior or cluster of behaviors, the underlying assumption is that by building the core of the youth, the youth will be less likely to engage in other risky behaviors as well. In their review of PYD programs, Catalano and colleagues (2004) found that 24 PYD programs resulted in significant changes in risky behaviors, including changes in sexual behavior, violence, drug and alcohol abuse, school misconduct and truancy, and smoking.
Positive Youth Development Objectives.

Although evidence-based, age-appropriate sexuality education programs have been effective in providing the knowledge and skills necessary to reduce unsafe sexual practices, there is still a need to concentrate efforts on sustaining and prolonging the adoption of healthy sexual behaviors and outcomes (Gavin, Catalano, & Markham, 2010). While there have been considerable declines in teen births, a high prevalence of teen births and STDs remain, notably among minority youth. Comprehensive sexuality education provides adolescents with the knowledge and skills to promote sexual health, including age-appropriate information on abstinence and protection from STDs and unintended pregnancy (Lindberg & Maddow-Zimet, 2012). Adolescents who receive information on abstinence and contraceptive methods are more likely to delay the onset of sex and use protection the first time they have sex; however, sustaining long-term effects have been indirect and significantly moderated by the adolescents’ age at first sex (Lindberg & Maddow-Zimet, 2012). There is a need for efforts that extend beyond traditional sexuality education in the classroom. PYD provides the tools needed to fill the gap left by sexuality education. PYD provides the necessary empowerment, environment, and resources needed to apply the knowledge and skills gained through traditional sexuality education (Gavin, Catalano, David-Ferdon, Gloppen, & Markham, 2010; Lindberg & Maddow-Zimet, 2012; Roth & Brooks-Gunn, 2003). PYD develops essential internal strengths that allow youth to confidently refrain from risky sexual behavior. Gavin, Catalano, David-Ferdon, et al.(2010) found that in 15 PYD programs with significant findings, all allowed the adolescents the opportunity to develop strengths (e.g., self-efficacy and belief in the future) and skills (e.g., decision-making skills and job skills) in a supportive atmosphere and resulted in improvements in sexual health outcomes, including delayed initiation of sex, decreased frequency and recent sex, decreased number of partners, increased contraceptive use, and fewer pregnancies and STDs.
Studies operationalizing PYD concepts have shown an association between PYD and sexual health. Several studies have operationalized PYD concepts in the form of youth assets. Youth assets are individual, interpersonal, and environmental factors that protect youth from engaging in a wide range of risk behaviors. Examples of youth assets include good family communication, nonparental adult role models, peer role models, and aspirations for the future (Oman et al., 2002). Youth assets have been associated with a range of sexual health outcomes in adolescents. For example, six studies illustrated that adolescents with youth assets had significantly lower odds of ever having sexual intercourse than youth without those assets (Aspy et al., 2010; Mueller et al., 2010; Murphey, Lamonda, Carney, & Duncan, 2004; Oman, Vesely, Aspy, McLeroy, & Luby, 2004; Tolma et al., 2011).
Tolma et al. (2011) found that Parental Monitoring was associated with ever having sexual intercourse for African American, Hispanic, and White adolescents. African American adolescents also had a significant association between the Relationship With Mother asset and initiation of sexual intercourse. White adolescents had a significant association with Family Communication and initiation of sexual intercourse.
One asset study also focused on younger adolescents and the ever had sexual intercourse outcome (Doss et al., 2006). The Positive Peer Role Models and Use of Time (Religion) assets, representing attendance at religious activities, were significantly associated with ever having sexual intercourse in 13 to 14 year olds. Those young adolescents with these assets had lower odds of ever having sexual intercourse than those without. However, the Use of Time (Religion) asset was no longer significantly associated with ever having sexual intercourse after controlling for Positive Peer Role Models.
Consistent with PYD approach, the number of assets adolescents have makes a difference in how protected they are against negative sexual health outcomes. Adolescents with larger numbers of assets were less likely to have ever had sexual intercourse (Murphey et al., 2004; Oman et al., 2004) and to delay sexual intercourse until after the age of 17 (Oman et al., 2004). Oman et al. (2004) also found that the more assets adolescents reported, the more likely they were to report birth control use at last sexual intercourse.
By using an asset-focused PYD approach, adolescent health behaviors can be targeted through constructive activities and in turn can strengthen ties between adolescents, important adults, and peers. Furthermore, it can also impact ties between adolescents and influential social environments such as schools and communities, and it can foster building new skills.
A review of interventions using PYD showed that PYD concepts have been significantly associated with a range of health behaviors including increased self-control, decreased substance use, decreased aggressive behaviors, greater self-efficacy in refusal skills, higher reading grades, more tolerance, reduced family conflict, and reduced school suspension or drop-out rates (Catalano et al., 2004). Interventions using PYD concepts have also been shown to increase attitudes and beliefs in adolescents that contribute to health risk behaviors including connectedness to peers, global self-esteem, perceived support from friends (Karcher, 2008), and acceptance of body image (LeCroy, 2004).
While there is a growing body of literature on the association between PYD and sexual health in adolescents (Gavin, Catalano, David-Ferdon, et al., 2010), there is very little information available for minority adolescents, particularly younger minority adolescents 10 to 14 years old. Researchers have also operationalized PYD differently and used different components of PYD to test the influence of PYD on sexual health behaviors. The purpose of this systematic review is to examine interventions based on PYD concepts designed to reduce negative sexual health outcomes in young minority adolescents.
Methods
Studies were identified by searching six search engines: MEDLINE, PsychInfo, CINAHL, ERIC, JSTOR, and Google Scholar. Abstracts were searched for key terms. The original search was limited to articles found through MEDLINE, PsychInfo, CINAHL, and ERIC and published in English between January 1993 and December 2013. The search was then broadened to include articles found through JSTOR and Google Scholar and published in English between January 2003 and December 2013. Search terms included “positive youth development” AND “sexual health,” “adolescent development” AND “sexual health” AND “intervention,” “bonding” OR “positive youth development” AND “intervention” AND “sexual health,” “evaluation” AND “positive youth development” OR “adolescent development” AND “sexual health,” “evaluation” AND “intervention” AND “sexual health” AND “early adolescence,” “evaluation” AND “intervention” AND “sexual health” AND “adolescence,” “evaluation” AND “intervention” AND “sexual health,” “teen pregnancy prevention,” “youth development” AND “pregnancy prevention” AND “evaluation,” “youth development” AND “HIV prevention,” “youth development” AND “STD prevention.” Reference pages and suggested articles were also reviewed for additional articles.
For the purposes of this systematic review, PYD programs were defined by the following characteristics: (a) focused on one or more of the 15 PYD objectives proposed by Catalano et al. (2004), (b) included youth participating in the program who were 10 to 14 years old, (c) focused on minority underserved youth, (d) the intervention included activities on sexual health, and (e) the focus of the intervention outcomes was on sexual behavior.
Additional inclusion criteria for studies included in the review were as follows: (a) written in English, (b) implemented in the United States, (c) published in peer-reviewed journals, and (d) a quasi-experimental or experimental study design. Articles that did not meet the inclusion criteria were excluded. Articles were also not included if the intervention only involved a sexuality education curriculum that did not specifically address one of the 15 PYD constructs. The search resulted in 1,021 articles. The results were then narrowed to include the 15 articles reflecting 12 unique studies that are reviewed here (see Figure 1).
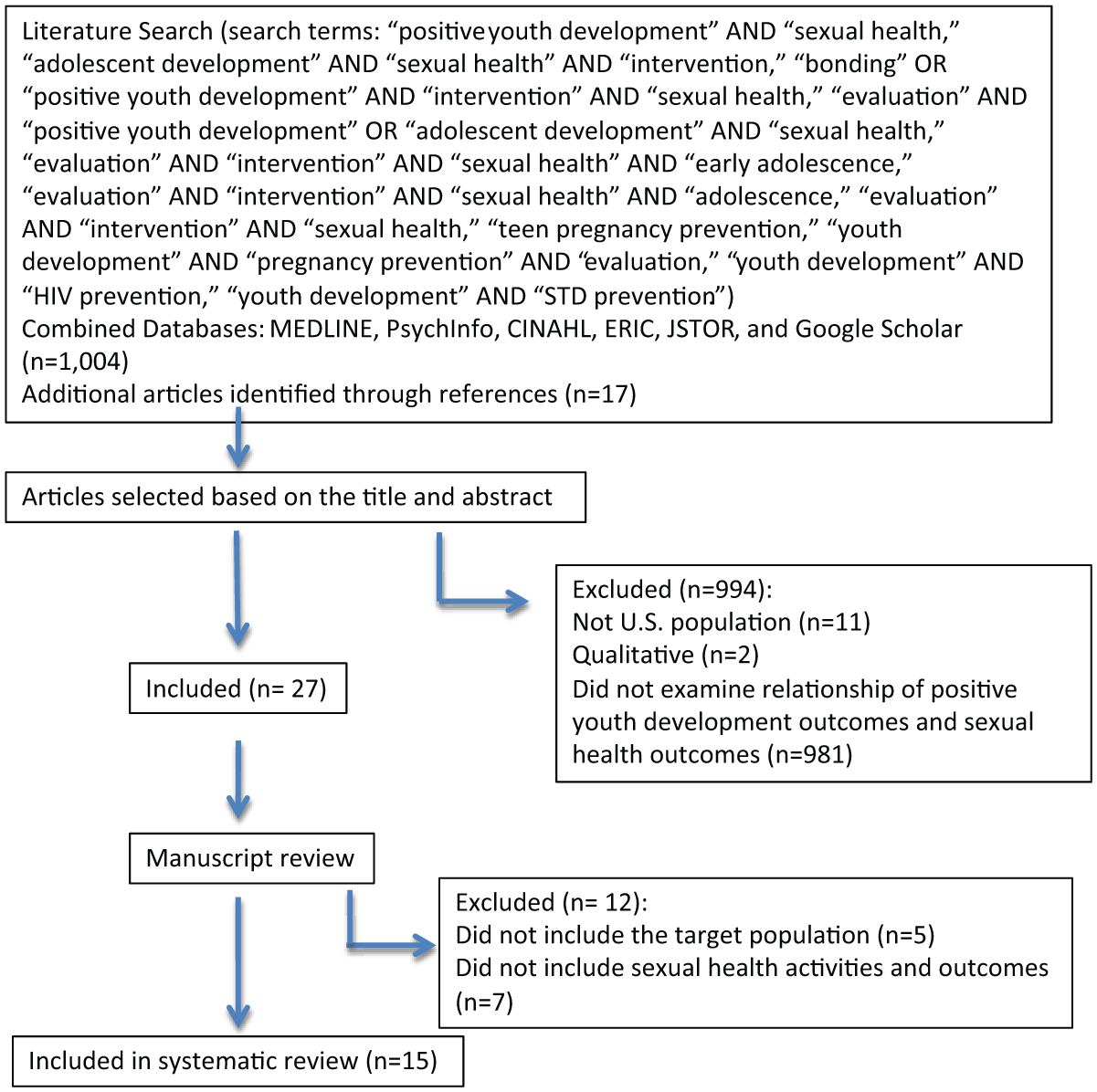
Flow diagram of study selection.
Results
The following section briefly summarizes the included studies, describes study characteristics, outlines the implementation of the studies, and synthesizes study results. Table 2 illustrates the study population, length of intervention, type of study, and results for the 15 articles reviewed.
Summary of Interventions.

Note. STDs = sexually transmitted diseases; SES = socioeconomic status; R.E.A.L.= Responsible, Empowered, Aware, Living; HIV = human immunodeficiency virus; CYS = Community Youth Service; PATH= Parent–Preadolescent Training for HIV Prevention; CAPS= Children and Adolescent Prevention Scale.
Summary of Interventions
Conduct Problems Prevention Research Group (CPPRG, 2014) utilized the Fast Track prevention intervention that followed participants from kindergarten through high school. Students with high rates of aggressive behaviors were recruited for the program and randomly assigned to treatment or control, with predominately African American kindergarten students recruited at baseline. The Fast Track version of the Promoting Alternative Thinking Strategies curriculum was implemented in first through fifth grades by teachers. Supplemental enrichment programs were also offered that provided additional social skills including: controlling emotion, prosocial skills, self-control, parent-child communication, limit setting, and supporting the school. Additional parent-child sessions were also offered. There were a total of 35 sessions in first and second grade and less-intensive monthly boosters for third through fifth grades. In middle school, the program included six child sessions on organization and study skills. It also included parent sessions on school connectedness that focused on developing relationships with counselors and teachers.
The Pursue Your Dreams program incorporated the seven principles of Kwanzaa: unity, self-determination, collective work and responsibility, cooperative economics, purpose, creativity, and faith (Clemons, Wetta-Hall, Jacobson, Chesser, & Moss, 2011). The program featured two main components: the Pursue Your Dreams Educational Program (which included the Choosing the Best abstinence education curriculum and tailored workbooks) and the Career Planning Club. The curriculum was implemented with minority middle school students (predominantly African American) for 6 to 8 days for 45 minutes per day and with high school students for 2 weeks for 90 minutes per day. The Career Planning Club was implemented for a maximum of 100 hours after-school throughout the school year. Additional program components (school assemblies, family program activities, parent network social, and parent education workshops, teen summits) were implemented throughout the school year.
Keepin’ It R.E.A.L. (Responsible, Empowered, Aware, Living)! was a two-pronged, theory-based approach testing the effectiveness of two different HIV prevention interventions implemented with African American mothers and adolescents. One intervention was based on Social Cognitive Theory and the other was based on Problem Behavior Theory (Dilorio et al., 2006; Dilorio et al., 2002). The social cognitive intervention (SCI) focused on promoting cognitive and behavioral competence and strengthening self-efficacy in a supportive environment. The SCI was implemented every 2 weeks for 3 months for 2 hours per session with a total of seven sessions. The intervention included sessions on puberty, peer pressure, communication skills, talking about sex, sexual decision making, condom use skills, and consequences of sex. Role-playing and skits were also utilized to practice these skills. Mothers and adolescents had four joint sessions and three separate breakout sessions. The problem behavior intervention, which was based on the notion that problem behaviors coexist and are based on similar underlying, predisposing factors, had two components: the Life Skills component for the adolescents and the Parenting Program for the mothers. Mothers and adolescents met separately, except for the first and seventh session. The Life Skills component was implemented once every 2 weeks for 2 hours for seven sessions. The Life Skills sessions emphasized tobacco use, alcohol and drug use, violence, sexual intercourse, and school behavior. Adolescents focused on decision-making and skill-building activities (cognitive and behavioral competencies) for each behavior, bonding with their parents and friends, and role-playing various situations. Additional activities included opportunities for prosocial involvement such as visits to senior centers and a college trip. The Parenting Program was implemented at the same time as the adolescent sessions but included sessions on relaxation, setting parenting goals, supportive parenting (bonding with children), understanding, and sharing their values, strengths, and weaknesses of parenting. The control group met for 1 hour, viewed a 20-minute HIV related video, and participated in a discussion about transmission of HIV and protection.
REAL Men was an HIV prevention intervention, based on the social cognitive theory, which focused on developing sexuality-related communication between predominately African American fathers (or father figures) and their sons (Dilorio, McCarty, Resnicow, Lehr, & Denzmore, 2007). The intervention focused primarily on promoting bonding among the fathers and sons, promoting the cognitive and behavioral competencies of the sons through encouragement and facilitation of conversations about delaying sexual activity, and the importance of using condoms if the adolescent chooses to be sexually active. The intervention was implemented once a week, 2 hours per session, for 7 weeks. Six of the seven sessions involved the fathers only, and the last session incorporated the sons as well. The sessions included topics on parental monitoring, peer relationships, sexuality education, with specific emphasis on the transmission and prevention of HIV. Fathers were given the opportunity to role-play and watch video examples of fathers talking to their sons about sexuality-related topics. The control intervention was implemented in seven, 2-hour sessions and focused on exercise and nutrition.
The California Adolescent Sibling Pregnancy Prevention Program was implemented to siblings (predominately Hispanic) of pregnant and parenting teens (East, Kiernan, & Chavez, 2003). Intervention services included case management, academic counseling, decision-making skills, job placement, self-esteem, and sexuality education. On average, program participants participated in approximately 2 hours of programming each month, and over the course of the program received an average of 7 hours of psychosocial skills services. These services included seven components: dealing with peer pressure, decision-making (cognitive competency) skills, life skills, stress/anger management (emotional competency), gang prevention, self-esteem, and bonding with parents. In addition, 5 hours of sexual health education, 4 hours of community service, and 4 hours of recreational activities were completed. Females received significantly more service hours than males. The comparison group was recruited from the program’s wait list.
The Aban Aya Youth Project, culturally tailored specifically for African American adolescents, comprised two experimental conditions: the social development curriculum and the school/community intervention (Flay, Graumlich, Segawa, Burns, & Holliday, 2004). The social development curriculum was a 16 to 21 lesson school-based curriculum in fifth through eighth grades. The main focus of this curriculum was on self-esteem, stress management (emotional competency), social competency, setting goals, and decision- and problem-solving skills. The school/community intervention included the school-based social development curriculum with the addition of parent support programs and a focus on linking parents, schools, and local businesses. The control condition was implemented for the same length of time as the intervention conditions, but focused on nutrition, exercise, and health care.
The Reach for Health Community Youth Service (CYS) learning program was a classroom-based service learning program, implemented by trained schoolteachers to seventh- and eighth-grade predominately African American, urban students (O’Donnell et al., 1999; O’Donnell et al., 2002). The intervention comprised a CYS intervention group, a Reach for Health curriculum-only group, and a control group. The CYS intervention group participated in 3 hours per week of community service/prosocial involvement (e.g., adolescents read to nursing home residents and assisted at child care centers) for the entire school year, for both the seventh- and eighth-grade school years. In addition, the CYS intervention group participated in the Reach for Health curriculum, which was a modified social learning health class curriculum that primarily focused on drug and alcohol use, violence, and sexual behaviors; 10 of the lessons focused on healthy development and sexuality. The curriculum had 40 core lessons in the seventh grade and 34 core lessons in the eighth grade. The Reach for Health curriculum-only group participated only in the curriculum lessons, not in the community service projects. The CYS intervention and the Reach for Health groups were both implemented in one urban school. A second school served as the control school; the population closely matched that of the intervention school.
The Children’s Aid Society’s Carrera Program was a 3-year after-school program, with activities each weekday for 3 hours a day and throughout the school year (Philliber, Kaye, Herrling, & West, 2002). There were seven key components: job club (fostered belief in the future), academic support, family life and sexuality education, arts, individual sports, mental health services (social and emotional competencies), and medical care services. The program was a randomized controlled trial, implemented primarily to African American students, with the control receiving usual care that included homework assistance and recreational activities.
Prado et al. (2007) outlined Familias Unidas and Parent-Preadolescent Training for HIV Prevention (Familias Unidas + PATH), a Hispanic-specific family-oriented risk reduction program. Familias Unidas was mostly focused on reducing adolescent substance use and risky sexual behavior through parental involvement, improving parent-child communication, and overall parental support/bonding. This was a randomized controlled trial with the control groups receiving either the English for Speakers of Other Language (ESOL) component and PATH or HeartPower! (an exercise and nutrition program) and ESOL.
Sieving et al. (2011) and Sieving et al. (2013) both described the Prime Time program. High-risk adolescent girls must have sought clinical care for at least one of the following risk criteria to be included in the program: a negative pregnancy test, treatment for STDs, young age, risky sexual and contraceptive behavior, aggressive behavior, or school disconnectedness. Participants (mostly African American) were randomly assigned to either the intervention or control group, with the control group receiving usual clinical services. Prime Time participants received a combination of case management, peer leadership programs, and clinical services for 18 months.
El Joven Noble (The Noble Young Man) is a 10-week, quasi-experimental PYD program designed for Latino male adolescents that encourages character development of adolescent males (Tello, Cervantes, Cordova, & Santos, 2010). El Joven Noble stressed the following issues: importance of preventing unplanned pregnancies, substance abuse, and community violence. It also heightened the youth’s ability to make responsible choices and have respectful relationships through four core components: acknowledgment (cultural identity), understanding (sacred purpose), integration (integrating values), and movement (safety and trust).
ReCapturing the Vision was an abstinence education program implemented to high-risk, low-income, predominantly African American eighth-grade females (Trenholm et al., 2007). The program was implemented for 1 school year, every day of that year, in an elective class. Identified, high-risk female students were asked to apply for the program and were randomly assigned to either intervention group or the control group. The intervention comprised two curricula: ReCapturing the Vision and Vessels of Honor. The ReCapturing the Vision curriculum focused on understanding personal strengths and resources, strengthening skills, and identifying techniques to accomplish goals and resist negative pressures. The Vessels of Honor curriculum had six key principles: (a) honorable behavior, (b) communication and negotiation skills, (c) healthy relationships and emotions, (d) growth and development, (e) dating violence, and (f) choosing a partner for life and the benefit of a healthy marriage. Additional program services included community service projects, tutoring, a family retreat, an annual rally, and an annual symposium with celebrity guests. The control group enrolled in a different class.
Study Characteristics
Participants
The original intention of the literature search was to identify studies that focused solely on minority adolescents 10 to 14 years old. However, the search did not uncover any studies that met the specified age criterion. Therefore, the criterion was adjusted to incorporate studies that included adolescents 10 to 14 years old, which resulted in a variety of age ranges. One study targeted adolescents that were at the elementary, middle, and high school levels (CPPRG, 2014). Seven studies (nine articles) focused solely on the middle school aged adolescents (Dilorio et al., 2007; Dilorio et al., 2006; Dilorio et al., 2002; Flay et al., 2004; O’Donnell et al., 1999; O’Donnell et al., 2002; Philliber et al., 2002; Prado et al., 2007; Trenholm et al., 2007). Four studies (five articles) focused on middle and high school aged adolescents (Clemons et al., 2011; East et al., 2003; Sieving et al., 2011; Sieving et al., 2013; Tello et al., 2010).
The majority of participants in all 12 studies were minority youth. Four studies (five articles) were targeted to African Americans (Clemons et al., 2011; Dilorio et al., 2007; Dilorio et al., 2006; Dilorio et al., 2002; Flay et al., 2004). Two studies were intended for Latino youth (Prado et al., 2007; Tello et al., 2010). The remaining 6 studies comprised a diverse group of youth but the majority of participants were minority (CPPRG, 2014; East et al., 2003; O’Donnell et al., 1999; O’Donnell et al., 2002; Philliber et al., 2002; Sieving et al., 2011; Sieving et al., 2013; Trenholm et al., 2007). Most studies also characterized nearly all or all of their participants as high risk due to family socioeconomic status (SES). Two studies also targeted recruitment to adolescents with an additional risk factor, either because of past high rates of aggressive-disruptive behavior (CPPRG, 2014) or a sibling was pregnant or got someone pregnant (East et al., 2003). Thus, these studies were implemented with high-risk adolescents who might be less likely than youth in high-resource families and communities to make and sustain positive sexual health behavior changes.
Study design
The 12 studies utilized either a quasi-experimental (Clemons et al., 2011; East et al., 2003; Tello et al., 2010) or experimental (CPPRG, 2014; Dilorio et al., 2007; Dilorio et al., 2006; Dilorio et al., 2002; Flay et al., 2004; O’Donnell et al., 1999; O’Donnell et al., 2002; Philliber et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013; Trenholm et al., 2007) study design. Three studies utilized a pre and posttest design (Clemons et al., 2011; East et al., 2003; Tello et al., 2010), and nine studies evaluated outcomes at multiple time periods (CPPRG, 2014; Dilorio et al., 2007; Dilorio et al., 2006; Dilorio et al., 2002; Flay et al., 2004; O’Donnell et al., 1999; O’Donnell et al., 2002; Philliber et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013; Trenholm et al., 2007). The length of the intervention varied by study, ranging from 7 weeks (Dilorio et al., 2007) to 12 years (CPPRG, 2014).
Intervention settings
The interventions were all delivered in either school-based or community settings. Five of the interventions were predominantly school based (Clemons et al., 2011; CPPRG, 2014; Flay et al., 2004; O’Donnell et al., 1999; O’Donnell et al., 2002; Trenholm et al., 2007). Seven interventions were community based (Dilorio et al., 2007; Dilorio et al., 2006; Dilorio et al., 2002; East et al., 2003; Philliber et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013; Tello et al., 2010).
Intervention components
The 12 identified studies targeting young minority adolescents’ sexual health using PYD concepts varied widely in approach. The PYD organizing framework developed by Catalano and colleagues (2004) served as the organizing framework for this review. The 15 PYD constructs serve as a guideline for developing PYD program components and was used here to organize PYD constructs operationalized across studies. Table 3 provides a summary of the program components along with the authors’ attempt to categorize intervention components by the 15 PYD objectives identified by Catalano et al. (2004). Looking across interventions, the PYD constructs utilized most frequently were as follows: promotes bonding (11 of 12 studies), promotes cognitive competence (11 of 12 studies), promotes social competence (11 of 12 studies), and promotes behavioral competence (11 of 12 studies). In addition, provides opportunities for prosocial involvement was utilized by 10 of the 12 studies, fosters belief in future was utilized by 9 of 12 studies, and two constructs (promotes emotional competence and fosters self-efficacy) were utilized in 8 of the 12 studies.
Study Components and Positive Youth Development Constructs.
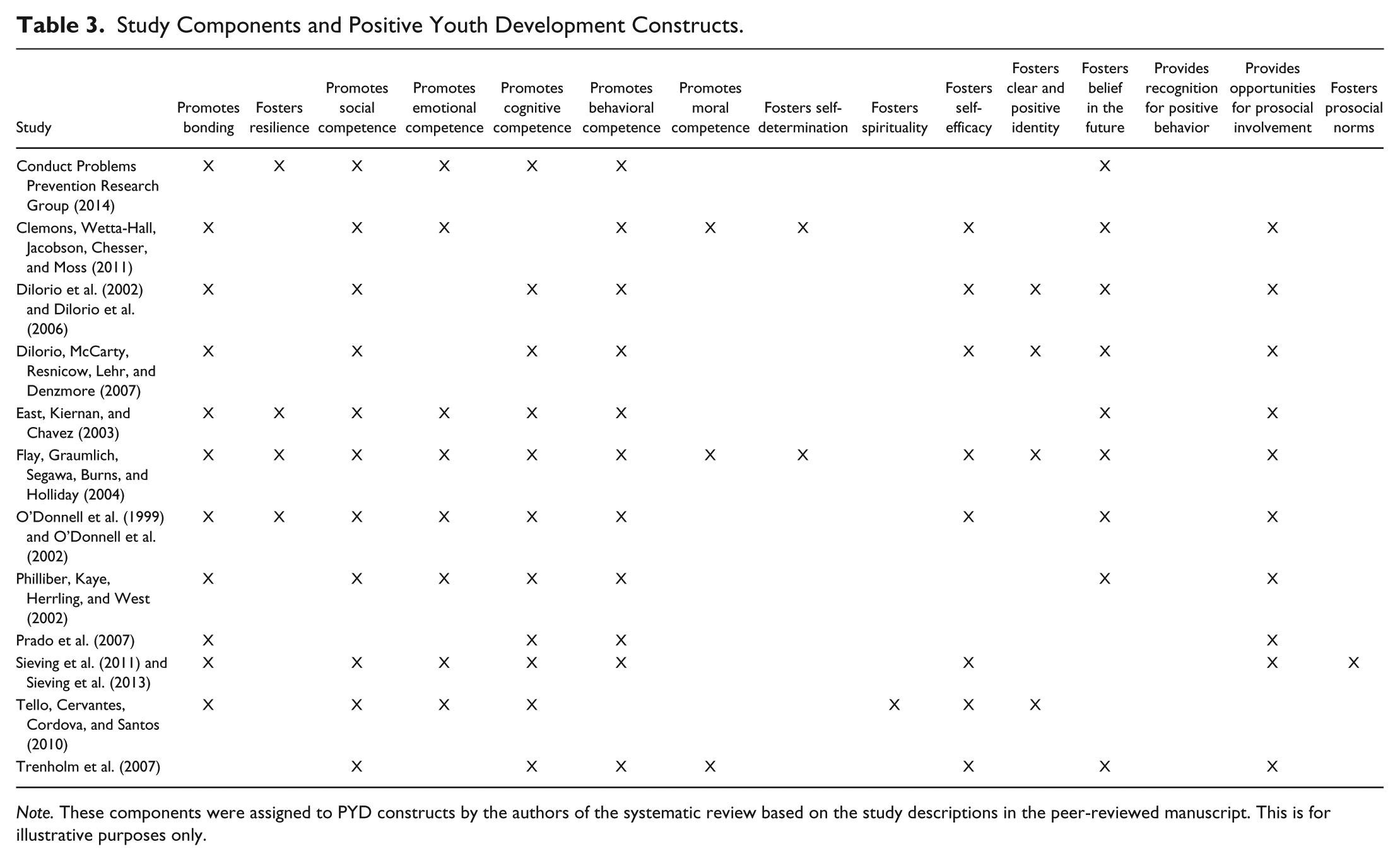
Note. These components were assigned to PYD constructs by the authors of the systematic review based on the study descriptions in the peer-reviewed manuscript. This is for illustrative purposes only.
Cultural tailoring
Tailored interventions are often recommended in health promotion as a way to improve program components to make them more culturally relevant to special populations, with the goal of increasing recruitment, retention, and health-promoting behavior change (Ewing, Wray, Mead, & Adams, 2012; Harrington & Noar, 2012; Kong, Singh, & Krishnan-Sarin, 2012). Four studies had tailored PYD curricula that emphasized the cultural norms and values of African American (Clemons et al., 2011; Flay et al., 2004) and Hispanic adolescent populations (Prado et al., 2007; Tello et al., 2010).
Implementation of Interventions
Interventions differed substantially in length, the “dose” of intervention components participants received, and when outcomes were measured. Interventions also differed in their sample size, recruitment, and retention strategies.
Recruitment
Recruitment efforts varied based on the intervention setting. School-based interventions recruited students through school orientations, referrals from instructors, other school personnel, and/or parents, and self-report screenings (Clemons et al., 2011; CPPRG, 2014; Flay et al., 2004; Trenholm et al., 2007). One school-based intervention did not recruit participants directly; instead, they randomized the intervention by school and allowed parents to consent (O’Donnell et al., 1999; O’Donnell et al., 2002). The clinic or community-based settings recruited participants primarily through screenings, clinic visits, and community organization membership lists (Dilorio et al., 2007; Dilorio et al., 2006; Dilorio et al., 2002; East et al., 2003; Philliber et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013; Tello et al., 2010).
Sample size
Baseline sample sizes varied from 253 to 1,538 participants. Nine of the 12 studies had sample sizes of more than 500 total participants (Clemons et al., 2011; CPPRG, 2014; Dilorio et al., 2007; Dilorio et al., 2006; Dilorio et al., 2002; East et al., 2003; Flay et al., 2004; O’Donnell et al., 1999; Tello et al., 2010; Trenholm et al., 2007). Two interventions were implemented with paired participants, with either a mother-child pair (Dilorio et al., 2002) or a father-son pair (Dilorio et al., 2007); the total number of pairs for each of the paired interventions was more than 250.
Retention
Retention rates differed greatly, with rates ranging from 29% to 93.3% One study with nonsignificant results had a retention rate of 29% (CPPRG, 2014) and the other study with nonsignificant results had a retention rate of 65% (Trenholm et al., 2007). Alternatively, most interventions with significant findings had attrition rates below 20% (East et al., 2003; Philliber et al., 2002; O’Donnell et al., 1999; O’Donnell et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013), one of which retained 93.3% of the participants at the final assessment (Sieving et al., 2013). One study with significant findings only retained about half of the original participants for the duration of the intervention (Flay et al., 2004). Two of the studies with significant findings that did not explicitly state their retention rates noted that either all participants completed posttest assessments or reported that the participant numbers increased at the posttest assessment (Clemons et al., 2011; Tello et al., 2010). The other two studies with significant findings that did not explicitly state retention rates noted the percent of participants that completed each follow-up assessment or provided approximate retention rates based on the maximum number of withdrawals per site (Dilorio et al., 2007; Dilorio et al., 2006).
Interventions with high retention rates had some common factors. First, two of the five studies with the highest retention rates offered clinical services (Philliber et al., 2002; Sieving et al., 2011; Sieving et al., 2013). Also, there was a focus on reducing attrition noted in three of the five studies, which included efforts such as contacting students several times throughout the year and offering additional services (East et al., 2003; Philliber et al., 2002; Sieving et al., 2011; Sieving et al., 2013). Furthermore, program components were implemented primarily by trained facilitators who developed trusting relationships with the participants and fostered a supportive environment (O’Donnell et al., 1999; O’Donnell et al., 2002; Philliber et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013). Lastly, four of the five studies with the highest retention rates offered monetary incentives to their program participants (East et al., 2003; Philliber et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013).
Dose of program components
The dosage of the intervention components varied widely and was not always related to intervention length or significant program effects. One intervention with significant findings was implemented for 3 years, 5 days a week, 3 hours a session (Philliber et al., 2002). Another was implemented monthly for 9 months, and averaged about 2 hours of programming a month (East et al., 2003). A third was implemented for 18 months (Sieving et al., 2011; Sieving et al., 2013). One study with nonsignificant findings was implemented for 35 sessions in 1st and 2nd grade, had monthly boosters in 3rd through 5th grade, and featured six child-only sessions and four family sessions from 6th through 10th grade (CPPRG, 2014); the other study with nonsignificant findings was implemented for 1 school year, every day of the school year (Trenholm et al., 2007).
Among the studies that documented a higher dose, most studies included an educational component, mostly curricula, that were implemented by trained facilitators over multiple time periods, with the shortest curriculum lasting six sessions (Clemons et al., 2011; CPPRG, 2014; Dilorio et al., 2007; Dilorio et al., 2006; Flay et al., 2004; O’Donnell et al., 1999; O’Donnell et al., 2002; Philliber et al., 2002; Prado et al., 2007; Tello et al., 2010; Trenholm et al., 2007).
Synthesis of Study Results
Sexual health outcomes
Sexual health outcomes assessed in minority adolescents included initiation of sexual intercourse, ever had sexual intercourse, perceived likelihood of contraceptive use, and actual contraceptive use (see Table 4). Table 4 depicts a breakdown of the sexual health outcomes measured. Seven of the 12 studies did limit their focus to younger adolescents (Dilorio et al., 2007; Dilorio et al., 2006; Flay et al., 2004; O’Donnell et al., 1999; O’Donnell et al., 2002; Philliber et al., 2002; Prado et al., 2007; Trenholm et al., 2007). These studies focusing on younger youth found significant increases in abstinence (Dilorio et al., 2007), refusing unwanted sex (Philliber et al., 2002), contraceptive use (Dilorio et al., 2007; Dilorio et al., 2006; Flay et al., 2004; Philliber et al., 2002; Prado et al., 2007), sexuality-related knowledge (Dilorio et al., 2006; Philliber et al., 2002), communication skills (Dilorio et al., 2007), and decreases in intimate behaviors (Dilorio et al., 2007), recent sex (Flay et al., 2004; O’Donnell et al., 1999; O’Donnell et al., 2002), pregnancy and birth (Philliber et al., 2002), and STDs (Prado et al., 2007). One of the studies that limited its focus to younger adolescents did not find any significant findings in any of the measured categories (Trenholm et al., 2007).
Summary of Outcomes Evaluated.
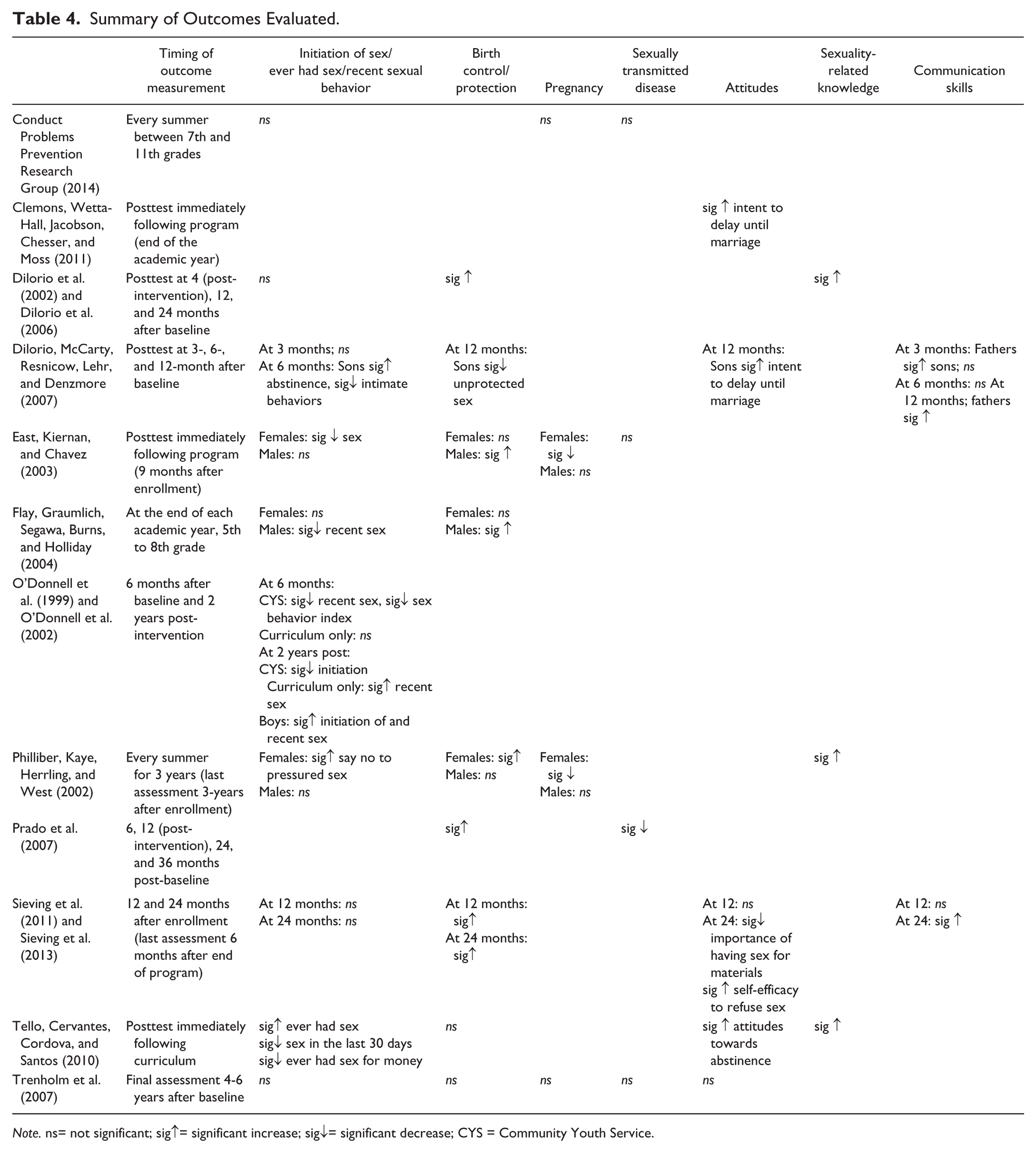
Note. ns= not significant; sig↑= significant increase; sig↓= significant decrease; CYS = Community Youth Service.
Outcomes by age
Studies that used a wide age range did not report outcomes by age. While all participants may have benefitted equally from exposure to the intervention, it was not possible to confirm this from reported results. Of the seven studies that focused on adolescents younger than 15, the most common significant outcomes were increased contraceptive use (Dilorio et al., 2007; Dilorio et al., 2006; Flay et al., 2004; Philliber et al., 2002; Prado et al., 2007), increased sexuality-related knowledge (Dilorio et al., 2006; Philliber et al., 2002), and decreased recent sexual intercourse (Flay et al., 2007; O’Donnell et al., 1999; O’Donnell et al., 2002).
Outcomes by gender
Nine studies included both girls and boys, while three studies were gender specific. Common significant outcomes after exposure to the PYD interventions for the girls were that they were significantly more likely to remain abstinent (East et al., 2003; Philliber et al., 2002), use a contraceptive method (Philliber et al., 2002; Sieving et al., 2011; Sieving et al., 2013), and less likely to have had sex (East et al., 2003), or become pregnant (East et al., 2003; Philliber et al., 2002). Females also had greater self-efficacy to refuse unwanted sex (Sieving et al., 2013) and reductions in perceived importance of having sex for material reasons (Sieving et al., 2013).
Common significant outcomes from the PYD interventions for the boys were that they were significantly less likely to ever have sex (Dilorio et al., 2007), to have recent sex (Flay et al., 2004; Tello et al., 2010), to have sex for money (Tello et al., 2010), and to use drugs before sex (Tello et al., 2010). Boys were significantly more likely to increase condom use (Dilorio et al., 2007; East et al., 2003; Flay et al., 2004), greater sexuality-related knowledge (Tello et al., 2010), intent to delay having sex (Dilorio et al., 2007), and attitudes toward abstinence (Tello et al., 2010). Three iatrogenic effects emerged for boys in two studies: Boys were more likely to have had sex after one study (Tello et al., 2010) and more likely to have initiated sex and had recent sex after another study (O’Donnell et al., 2002).
Outcomes by cultural tailoring
Four studies (Clemons et al., 2011; Flay et al., 2004; Prado et al., 2007; Tello et al., 2010) reported tailoring their interventions to make them more culturally relevant to minority adolescents. Clemons and colleagues (2011) tailored the Pursue Your Dreams intervention by utilizing a development model that incorporates key African American principles, such as the importance of faith, self-determination, unity, and working together. The Aban Aya project was developed with a focus on the African American community and based the project on two Ghanaian principles: “aban” which represents social protection and “aya” which represents self-determination (Flay et al., 2004). The Familias + PATH intervention was tailored to the Hispanic culture by focusing on strengthening the family unit and placing parents as leaders in the sexuality education of their children, which is consistent with the importance of the family unit in the Hispanic culture (Prado et al., 2007). Tello and colleagues (2010) tailored the Joven Noble curriculum by focusing on key factors that are important to the Hispanic culture (respect, family, interpersonal relationships, and working together) and dispelling misconceptions associated with certain cultural underpinnings, such as the “meaning of machismo.” Across studies that utilized a tailored approach, program outcomes were increased commitment to abstain from sex until marriage (Clemons et al., 2011), increased attitudes toward abstinence (Tello et al., 2010), contraceptive use (Flay et al., 2004; Prado et al., 2007), condom use (Flay et al., 2004; Prado et al., 2007), sexuality-related knowledge (Tello et al., 2010), decreased recent sex (Flay et al., 2004; Tello et al., 2010), use of alcohol before sex (Tello et al., 2010), and sex for money (Tello et al., 2010).
Outcomes by studies promoting abstinence and promoting safer sex practices
Most studies focused on safer sex practices, including abstinence and contraceptive use. Across the studies that promoted safer sex practices, common program outcomes were increased contraceptive use (Dilorio et al., 2007; Dilorio et al., 2006; East et al., 2003; Flay et al., 2004; Philliber et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013), increased refusal of unwanted sex or self-efficacy to refuse (Philliber et al., 2002; Sieving et al., 2013), increased rates of youth remaining abstinent (Dilorio et al., 2007; East et al., 2003), increased sexuality-related knowledge (Dilorio et al., 2006; Philliber et al., 2002), and decreased pregnancies and births (East et al., 2003; Philliber et al., 2002).
Two studies focused solely on promoting abstinence (Clemons et al., 2011; Trenholm et al., 2007). One study resulted in increased commitment to abstaining from sex until marriage (Clemons et al., 2011), and the other did not find any significant outcomes (Trenholm et al., 2007).
Two studies had abstinence or safer sex practices as secondary objectives (CPPRG, 2014; Tello et al., 2010). One study focused on aggressive behavior, which resulted in nonsignificant findings for initiation of sex, pregnancy, and STDs (CPPRG, 2014). Alternatively, the Joven Noble PYD Program focused primarily on character development through cultural values, positive identity, and trust with an emphasis on reducing pregnancies. The program resulted in decreases in number of youth who had sex in the last 30 days, and deceases in those who had sex for money. In addition, the program resulted in increases in sexuality-related knowledge (Tello et al., 2010).
Outcomes based on time of assessment
Studies assessed outcomes immediately following the intervention (Clemons et al., 2011; East et al., 2003; Tello et al., 2010), several years following the intervention (Trenholm et al., 2007), at multiple points during the intervention (CPPRG, 2014; Flay et al., 2004; Philliber et al., 2002), or at multiple points including follow-up assessments after the post-intervention assessment (Dilorio et al., 2007; Dilorio et al., 2006; O’Donnell et al., 1999; O’Donnell et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013). Of the studies that assessed outcomes immediately following the intervention, there was increased intention to remain abstinent (Clemons et al., 2011; East et al., 2003), increased contraceptive use (East et al., 2003), increased sexuality-related knowledge (Tello et al., 2010), decreased sex for money (Tello et al., 2010), and decreases in adolescents who have ever had sex (East et al., 2003; Tello et al., 2010).
The study that assessed outcomes solely several years following the intervention found no significant results (Trenholm et al., 2007). Of the studies that assessed outcomes at multiple points during the intervention, there was increased condom use (Flay et al., 2004; Philliber et al., 2002), increased sexuality-related knowledge (Philliber et al., 2002), increased ability to resist peer pressure to have sex (Philliber et al., 2002), decreases in pregnancies and births (Philliber et al., 2002), decreased ever had sex (Philliber et al., 2002), and one study resulted in no significant findings (CPPRG, 2014).
Of the studies that assessed outcomes at multiple points and followed up after the post-intervention assessments, there was increased contraceptive use (Dilorio et al., 2007; Dilorio et al., 2006; Prado et al., 2007; Sieving et al., 2013), increased self-efficacy to refuse unwanted sex (Sieving et al., 2013), increased abstinence (Dilorio et al., 2007), decrease in intimate behaviors/sexual behavior index (Dilorio et al., 2007; O’Donnell et al., 1999), decreased initiation of sex (O’Donnell et al., 2002), increased knowledge and decreased STDs (Prado et al., 2007), and increased communication skills, decreased importance of having sex, and decreased recent sex (Sieving et al., 2013).
Outcomes by study components
Several of the study researchers stated the importance of multicomponent PYD interventions to influence several behaviors, yet only one study looked at the outcomes by the type of component (East et al., 2003). There were several significant associations: (a) fostering belief in the future (school and job-related services) was associated with increased contraceptive use for females, (b) promoting more time devoted to sexuality education was associated with reduced likelihood of early parenting for all participants, (c) fostering resilience and promoting social and behavioral competence (psychosocial services—stress management, peer pressure, and decision-making skills) was associated with increased contraceptive use with most recent partner, and (d) providing opportunity for prosocial involvement (community and recreational services) was associated with increased male’s intentions to remain abstinent. There was an iatrogenic effect in that more time in sexuality education was related to a decrease in the male’s likelihood of remaining abstinent. Services offered in individual settings were associated with reduced likelihood of early parenting for all participants, while group setting services were associated with more certainty of contraceptive use for all participants, more intentions to remain abstinent, and delayed initiation of sex among males.
The most common characteristics of all of the studies that produced significant results across the varied sexual-health-related outcomes were that the program promoted bonding (e.g., focusing on parent-child relationships and relationships with community members), social competence (e.g., opportunities to develop interpersonal skills), cognitive competence (e.g., opportunities to develop reasonable ways to overcome stressors and solve problems), behavioral competence (e.g., practice expressing oneself through role-plays), and provided opportunities for prosocial involvement (e.g., community service involvement).
Although all studies did not assess the effectiveness of the program components as East and colleagues (2003), there were some common themes among the study components of the studies with significant findings. The six studies that found significant results in the sexual behavior category (decreases in initiation of sex, ever had sex, recent sex, intimate behaviors, saying no to unwanted sex or pressured sex, and sex for money), all studies included program components and activities that promoted bonding, social, cognitive, and behavioral competence; five of the six studies included components that promoted emotional competence and provided opportunities for prosocial involvement (Dilorio et al., 2007; East et al., 2003; Flay et al., 2004; O’Donnell et al., 1999; O’Donnell et al., 2002; Philliber et al., 2002; Tello et al., 2010). Among the seven studies that found significant results in the birth control/protection category (decreases in unprotected sex, and increases in protected sex, condom use, and other birth control use), all studies included components that promoted bonding, cognitive and behavioral competence, and provided opportunities for prosocial involvement (Dilorio et al., 2007; Dilorio et al., 2006; East et al., 2003; Flay et al., 2004; Philliber et al., 2002; Prado et al., 2007; Sieving et al., 2011; Sieving et al., 2013). Among the two studies that found significant results in reducing pregnancy, both included components that promoted bonding, social, emotional, cognitive, and behavioral competence, fostered belief in the future, and provided opportunities for prosocial involvement (East et al., 2003; Philliber et al., 2002). Among the four studies that found significant results in the attitudes category (increased self-efficacy to refuse unwanted sex and intent to delay sex until marriage, decreased importance of having sex for material items), all studies included components that promoted bonding and fostered self-efficacy; three included components that promoted social, emotional, behavioral, and cognitive competence and provided opportunities for prosocial involvement (Clemons et al., 2011; Dilorio et al., 2007; Sieving et al., 2013; Tello et al., 2010). Two studies improved communication skills; both studies included components that promoted bonding, social, cognitive, and behavioral competence; fostered self-efficacy; and provided opportunities for prosocial involvement (Dilorio et al., 2007; Sieving et al., 2013).
Discussion
Early adolescence is a prime opportunity to impact sexual health outcomes as most adolescents have not initiated sexual activity, nor have they already been affected by the consequences of sexual activity (Albert et al., 2003). In addition, the longer adolescents delay sexual initiation, the more likely they are to have fewer sexual partners and decreased chances of becoming a parenting teen or have a STD (Albert et al., 2003). PYD programs that target developmental outcomes are an important tool for impacting sexual health as the developmental outcomes provide young adolescents with the necessary support and assurance to make healthy sexual choices (Catalano et al., 2004).
PYD programs can have a positive impact on adolescent sexual health, especially when it is delivered in a supportive atmosphere, involves positive adult role models, and provides affirmative opportunities and experiences to the adolescent (Catalano et al., 2004; Gavin, Catalano, David-Ferdon, et al., 2010). The present review focused on the PYD components that impact young minority adolescents. Minority adolescents are an underserved population that needs increased opportunities to participate in positive PYD programs as they are the most at risk of unplanned pregnancies and STDs (CDC, 2013; Martin et al., 2013). Although overall teen birth rates have declined, African American and Hispanic teens still have disproportionately higher rates than other populations (CDC, 2013; Martin et al., 2013). Providing positive opportunities and resources is essential to their development.
Although the original intention of this review article was to focus solely on young adolescents 10 to 14 years old, the search identified few studies within this specific scope. Seven of the identified studies, however, did focus on adolescents 15 and younger. This highlights the continued need for more interventions focusing on the early adolescence time period.
In addition, there is still little information comparing the outcomes of young adolescents with older adolescents. Often, studies controlled for age rather than explored it. This is truly a missed opportunity to identify effective prevention strategies in this population, and specifically which PYD components are most effective in reducing sexual risk behaviors for this age group. Obtaining a large-enough sample size to extract age-specific data is important to this effort to identify components that more effective for the young adolescents. Future studies should examine the impact of PYD interventions by age and by sexual experience. Young adolescents who are not already sexually active should be encouraged to continue to delay sexual activity to decrease their likelihood of unplanned pregnancy and STDs (Albert et al., 2003). Adolescents who are already sexually active should not be targeted for PYD programs that focus primarily on promoting abstinence, but rather ones that emphasize safer sex practices. Promoting abstinence may not be as appropriate for older adolescents who may have already initiated sexual activity, especially because some of the studies saw an increase in sexual activity over the course of the study (Dilorio et al., 2006; Tello et al., 2010). The two PYD studies that did primarily promote abstinence until marriage as an outcome were the Pursue Your Dreams program that had more than 80% of participants younger than 14 and found significant increases in intention to remain abstinent until marriage (Clemons et al., 2011) and the ReCapturing the Vision program that had an average age of 15 and did not find any significant results (Trenholm et al., 2007). Age-appropriate interventions that take adolescents’ sexual experience into consideration may be more appropriate for addressing the needs of the population; however, additional age-specific data are needed to draw clearer conclusions.
Across all studies, PYD constructs were operationalized in various ways. Five constructs were utilized most frequently: promotes bonding, promotes cognitive competence, promotes behavioral competence, promotes social competence, and provides opportunities for prosocial involvement. Assessing the effectiveness of each of these constructs was difficult because most studies utilized a true PYD, multicomponent approach and did not assess effectiveness of each component. However, among the programs with significant findings, four constructs were consistently utilized: promotes bonding, cognitive and behavioral development, and provides opportunities for prosocial involvement. Effective levels of dose of the PYD components should also be explored so that adequate resources and time can be targeted to minority youth.
In addition, four of the reviewed studies tailored the interventions based on specific populations (Clemons et al., 2011; Flay et al., 2004; Prado et al., 2007; Tello et al., 2010). Although cultural tailoring is generally seen as more culturally relevant and potentially more effective than interventions that do not tailor to specific populations, it was not clear whether these interventions had any greater impact on the sexual health of participants due to the cultural tailoring. While the components chosen for the intervention were based on PYD constructs and values of the minority youth’s culture, it was not clear whether these activities were also based on best practices to reduce negative sexual risk behaviors within the targeted population. It also raised questions such as the following: Is cultural tailoring as important for middle school students as it might be for older adolescents? If so, then what are important cultural aspects for younger adolescents? Given the limited number of articles that used tailored interventions and the mixed results of those studies, additional research is needed to better understand the role of culturally tailored PYD interventions.
Limitations
Although the findings of this review are promising, there are some limitations. Few PYD interventions target sexual health outcomes. There is a persistent need for more intervention research to identify program components and methods that are particularly effective in impacting sexual health outcomes in young minorities. In addition, this review was limited to including only PYD interventions that incorporated activities focused on sexual health. This more restrictive criterion was used based on previous research that showed that the majority of PYD interventions targeting young, minority adolescents, with statistically significant results, included some sexual health components (Gavin, Catalano, David-Ferdon, et al., 2010). However, this point must be researched further to determine whether studies that include sexual health components and receive significant results are significantly different from studies that do not include sexual health components and also receive significant results.
In addition, there are a lack of studies that assess intervention results across adolescence and young adulthood. Evaluating intervention effects while participants are adolescents and evaluating the long-term intervention effects into young adulthood would be ideal to better understand the long-term PYD impact. Half of the interventions only measured effects at multiple points during the intervention or immediately following the intervention and most found significant results. However, it would be beneficial to know whether the intervention was able to foster long-term changes. Another limitation could be the way the program components were assigned to PYD constructs in Table 3. The researchers used this for demonstrative purposes only and based the assignment of the program components based on the program description provided. Some of the categorization of the program components may vary compared with other researchers who may have direct contact and relationships with program developers.
While the PYD approach is an innovative, comprehensive approach to reducing risk behaviors by building resources, promoting healthy supports and environment, there are some limitations to the approach as well. The PYD approach has not been operationalized as extensively as other traditional, theory-based approaches, which limits the evidence of its effectiveness (Catalano et al., 2004; Gavin, Catalano, David-Ferdon, et al., 2010). In addition, because of the varied definitions and interpretations of the PYD components, it is difficult to assess which components are most important to behavior change, compared with other theory-based interventions that have already undergone such analysis (Buhi & Goodson, 2007). It is also difficult to assess which components may have influenced the greatest change, because most studies did not provide this information. While Catalano et al. (2004) provided the organizing framework for this systematic review, other constructs have been proposed that organize and define constructs in a different manner, such as the five Cs (competence, confidence, connections, character, and caring), supportive atmosphere, and formal and informal opportunities (Roth & Brooks-Gunn, 2003). Although these constructs are organized differently, they are similar. The use of these varied definitions can cloud the understanding of program developers attempting to incorporate components that are the most beneficial for adolescents. Moreover, replicating a PYD intervention could be more intricate and challenging than replicating a sexuality education curriculum-centered intervention, as PYD interventions typically have multiple levels of implementation and often do not always use a structured curriculum. For example, East et al. (2003) used a case management approach and each site could use a different approach to prevent sexual risk behaviors as long as providers met with clients in person at least once a month and implemented a variety of services; sample programs were provided but providers did not implement a consistent structured approach. This would be difficult to replicate with fidelity. Conversely, Clemons et al. (2011) included the Pursue Your Dreams educational component that utilized a structured curriculum that would seemingly be more realistic to replicate with fidelity. Utilization of a structured approach across PYD programs would allow for more manageable replication of PYD interventions. The structured approach does not have to be a traditional curriculum approach, but a structured process that details the components of the intervention and how it should be used. Lastly, the instrument development and evaluation data collection tools were not made readily available by study researchers. Therefore, it was not possible to gain a full understanding of the full development phase. For example, providing the exact wording of the questions asked on evaluation tools could have potentially helped researchers to understand whether the way in which questions were asked influenced the adolescents’ responses.
Future Implications
Researchers should consider several implications for future PYD programs.
Focus on young adolescents
The adolescents that have had sex by age 13 are at a higher risk of pregnancy and STDs. Early initiation of sex has been linked to early initiation of tobacco and substance use relationships with peers who engage in risky behaviors, depression, and school disconnectedness and disruption (Albert et al., 2003). Therefore, a focus on developmental outcomes to reduce the likelihood of initiating sexual activity could have a positive, long-term impact on the adolescents’ lives.
Researchers should consider developing programs for age-specific populations. Obtaining a large-enough sample size to assess age-specific data is important. An intervention designed to be implemented across a large developmental age range could potentially be beneficial for one subset and not for the other subsets of the age range. Four of the 12 interventions implemented the interventions to students across the middle and high school age ranges, but did not assess intervention effects by age ranges. Researchers that implement programming across developmental age ranges should report effect sizes and conduct power analysis to determine whether age-specific outcomes are appropriate.
De-link ethnic minority status from socioeconomic status
It was difficult to determine whether intervention effects for participants were due to SES or other challenges specific to cultural and social experiences youth have as a result of their ethnic minority status. The exploration of these differences is necessary to determine the particular cultural influences each contributes to early sexual initiation and sexual risk behaviors.
Focus on retention
Most of the studies with significant findings retained the majority of the program participants. Retention is particularly important for long-term developmental interventions due to the longitudinal nature of the effects of PYD interventions. For instance, the Fast Track Program attempted to retain students for 12 years, implementing intervention components in elementary, middle, and high school, but was only able to retain 29% of the original program participants, and experienced no significant program effects at the posttest analysis (CPPRG, 2014). It was difficult to assess whether the attrition of program participants or the actual program itself resulted in the nonsignificant findings. Although some PYD interventions found significant findings in short-term follow-ups, it is important to retain program participants and assess program effectiveness at several points post-intervention to gain a true understanding of program effectiveness. Attrition is particularly a concern for mobile, high-risk populations; so retention efforts should be a part of the planning process. PYD objectives are not likely to change sexual health outcomes after implementation of a few lessons. Developmental changes cannot be addressed in one sitting; therefore, it is important to focus on retaining the majority of participants throughout the entire program by including retention methods in the planning of the program, such as maintaining contact with the students by phone or home visits, using activities they can enjoy, vary the activities to keep them entertained, and provide incentives. Free clinical services may be an attractive incentive, especially for students of lower SES who may not have access to quality medical care. In addition, it is important to consider conducting attrition analyses to assess the impact of those that remained in the program compared with those that dropped out. Additional analysis should also be employed if participants are able to join the intervention, similar to the analysis done by the Reach for Health intervention researchers (O’Donnell et al., 1999; O’Donnell et al., 2002). The students who do not participate in the entire program may have responses that vary from the other participants, which should be captured and assessed for the program evaluation.
Focus on evaluation
Evaluation is the key to furthering PYD programming. Evaluating results of PYD interventions several years after initiation to determine whether short-term positive results withstand time would provide much-needed information about the long-term effects of PYD programming. Understanding the relationship between timing and dose for specific intervention components is key to the effectiveness of PYD interventions. A higher dose of intervention components could improve the likelihood of producing significant results. It remains unclear whether implementing interventions at multiple periods in the adolescents’ life span is most effective in reducing risky behaviors (e.g., CPPRG, 2014), or if it may be more important to concentrate intervention implementation at early adolescence (especially middle school aged) and evaluate the outcomes at multiple time periods post-intervention. More research is needed to determine the most beneficial approach. However, it is clear that PYD interventions should be implemented during early adolescence and incorporate long-term evaluations in order to assess long-term intervention effects into adulthood. In addition, developing a compendium of PYD measures and instruments and having a venue in which to provide this information to fellow researchers would strengthen consistent evaluations of PYD interventions.
Conclusion
The prevention of adolescent risk behavior has undergone a shift; the focus has changed from a deficit-centered approach to a more positive, resource-enhancing approach. PYD interventions have significantly impacted a range of health behaviors, including sexual health behaviors. PYD interventions provide opportunities and resources to adolescents to help them make positive decisions. Research and prevention efforts to this point have not been effective in reducing the differences between minority and White youth in teen pregnancy and other risky sexual behaviors. Continued research to understand the impact of the PYD approach in young minority populations may provide public health with more effective tools to reduce health disparities in the future.
Footnotes
Acknowledgements
The authors would like to thank Mary Gowin for her assistance in the preparation of this review. The authors would also like to thank the guest editor and anonymous reviewers for their contribution to this review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.