
Abstract
We examined whether social resources from the family and the community moderate the risk associated with low socioeconomic status (SES) for reduced quality of life (QL) among youth across racial/ethnic groups. Data were from 4,824 fifth-grade youth (age
Keywords
Low socioeconomic status (SES) confers a heightened risk for a wide range of negative health and life outcomes (e.g., Chen, Matthews, & Boyce, 2002; Mistry, Vandewater, Huston, & McLoyd, 2002; Newacheck, Hung, Jane Park, Brindis, & Irwin, 2003). For example, Chen, Martin, and Matthews’s (2006) analysis of 33,911 children 0 to 18 years of age showed a linear positive association between family SES and overall health and a linear negative association with functional limitations. Larson, Russ, Crall, and Halfon (2008) reported that multiple SES-related risk factors had a cumulative negative effect on child health status across physical and psychosocial domains, with marked gradient effects. Low SES is thus a salient risk factor for poor health. It is alarming then that approximately 20% of children live in poverty and low SES has become increasingly prevalent in recent years (Macartney, 2011).
The majority of the research on the effects of low SES on health has examined specific health conditions (e.g., asthma, depression) or problem behaviors (e.g., violence, substance use). However, it is important to consider impact on health and well-being more broadly, in such as suggested by the World Health Organization’s (1948) definition of health as “a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity (p. 1).” One common holistic concept capturing broader outcomes in childhood is quality of life (QL), which can be defined as “the combination of objectively and subjectively indicated well-being in multiple domains of life considered salient in one’s culture and time, while adhering to universal standards of human rights” (Wallander, 2001, p. 34).
It is important to examine the effects of SES on QL in youth not just because it reflects health and well-being broadly but also because it captures essential daily functioning (Koot & Wallander, 2001). QL concerns how youth are able to engage physically in daily activities and feel about themselves and their lives, view their place among and relationships with others, and function in their major roles (Wallander, 2001). Measures of QL have the potential to describe the health and well-being of youth in the general population more comprehensively than conventional mortality and morbidity measures and provide better identification of specific groups with high rates of unrecognized conditions, social and emotional problems, and poor functioning (Barofsky, 2012; Koot & Wallander, 2001). In line with this definition, an evaluation of children’s QL requires extension beyond the traditional health-related dimensions. Self-esteem has been examined as one important aspect of children’s QL (Faria, Blanes, Hochman, Filho, & Ferreira, 2011; Fradkin et al., 2014; Ravens-Sieberer et al., 2008; Wallander et al., 2012). Moreover, confirmatory factor analysis has indicated that self-esteem is an important indicator of psychological health and encompassed by QL (Eser et al., 2008; Ravens-Sieberer et al., 2008).
Resilience
Despite the generally unfavorable circumstances associated with low SES, many youth are resilient and thus able to avoid associated risks, such as behavior problems or poor health. Masten (2001) defined resilience as “good outcomes in spite of serious threats to adaptation or development” (p. 28). Resilience is hypothesized to involve protective mechanisms, which are positive moderators of risk or adversity; that is, when present, protective mechanisms inhibit the effect of risk exposure, such that the negative outcome is not experienced. Furthermore, they are assets, or measurable characteristics predicting positive outcomes, which become salient once adversity is substantial (Masten, 2011; Masten & Tellegen, 2012).
Bronfenbrenner’s ecological systems theory provides a useful framework for conceptualizing contributions to risk and resilience (Bronfenbrenner, 1979; Bronfenbrenner & Morris, 2006). This theory accounts for differences in child development by highlighting levels of social influences such as at the family and broader social community levels. In relation to QL, specifically, previous research has informed about several levels of social resources that foster resilience among diverse youth (Cooper, Brown, Metzger, Clinton, & Guthrie, 2013). Protective mechanisms at the family level have included, for example, warm, secure family relations and at least one stable person competently attuned to the child’s needs, and at the social community level, for example, peers and other adults providing support and advice (e.g., McMahon, Felix, & Nagarajan, 2011; Moreira, Frontini, Bullinger, & Canavarro, 2013). These family and social mechanisms have been shown to be especially important for racial/ethnic minority and early adolescents.
Racial/Ethnic Minority Status
The United States consists of multi-racial/ethnic population. At least 43% of children younger than 18 years report a race/ethnicity other than (non-Hispanic) White, and these groups are expected to constitute more than half of all children in the United States by about 2040 (Wallander et al., 2012). Race/ethnicity matters in many aspects of children’s development, such as differences in morbidity and mortality (Flores, 2010) as well as cultural differences relevant for interventions (Hertzman & Boyce, 2010).
Hispanic youth, for example, on average put a strong emphasis on cooperation and interdependence among family members (e.g., Miranda, Bilot, Peluso, Berman, & Van Meek, 2006; Santiago-Rivera, Arredondo, & Gallardo-Cooper 2002; Skogrand, Hatch, Singh, & Rosenband, 2008). Taking advantage of Hispanic collectivism in a smoking prevention program promoted more desirable outcomes, including parental involvement, more accurate perceptions about smoking, and lower tobacco use (Gonzalez-Blanks, Lopez, & Garza, 2012). Among African American youth, family support and connectedness are considered to be consistent with the communal values promoted in the African American culture (Harris & Molock, 2000). Family support, family cohesion, and parental support have been shown to protect against depression (Marion & Range, 2003; Plant & Sachs-Ericsson, 2004). African American adolescents from cohesive families report less stress (Belgrave, Clark, & Nasim, 2008) and less substance use (Nasim, Belgrave, Jagers, Wilson, & Owens, 2007). Infusion of cultural values into prevention programs can reduce problem behaviors (Nasim et al., 2007). Therefore, family-level, and perhaps community-level, protective factors may be especially influential for Hispanic and African American youth.
Moreover, low SES is significantly more common among African American and Hispanic compared with White youth (Larson et al., 2008). Previous research has examined differences in QL across racial/ethnic groups while accounting for SES and other contextual factors (Fradkin et al., 2014; Schuster et al., 2012; Wallander et al., 2012), but little research has examined which protective mechanisms confer resilience in different racial/ethnic groups. Understanding how resilience processes can buffer the impact of low SES on QL among diverse youth can inform intervention efforts and possibly point to targeted interventions for specific racial/ethnic groups.
Early Adolescent Period
By early adolescence, around ages 10 to 11, substantial developmental changes are initiated physically, cognitively, emotionally, and interpersonally (Wallander, Fradkin, & Scott, 2013). Whereas the family remains primary in adolescence, other social relationships rise in prominence and become increasingly important for youth’s well-being (Oberle, Schonert-Reichl, & Thomson, 2010; Wentzel, 2009). Because a child will already have been exposed to the strain of low SES for a decade by age 10 (Chen et al., 2002), it is important to examine variation in the impact of SES on QL in early adolescence. Research on resilience can inform the development of early prevention programs that can be initiated before the effects of low SES are necessarily solidified (Durlak, Weissberg, Dymnicki, Taylor, & Schellinger, 2011). Guided by Bronfenbrenner’s framework (Bronfenbrenner & Morris, 2006), we selected four specific family and broader social mechanisms to examine in the present study based on prior research pointing to potential for fostering resilience.
These four mechanisms, parental nurturance, family cohesion, peer support, and other adult support, comprise family-level and community-level micro-systemic influences. In the ecological systems theory, the microsystem consists of the youth’s most immediate environment and reference point of the world (Swick & Williams, 2006). The effects of this most proximal process are presumed to be more powerful than the larger, more distal contexts (Bronfenbrenner, 1994). Most notably, the family provides an initial base for developing trust and shapes the youth’s personality (Swick, 2004). Growing in relevance over development, other examples of individuals within the microsystem include adults interacting with youth outside of the home, such as school personnel and peers (Bronfenbrenner, 1994). The experiences formed within and outside the family reinforce one another and can either facilitate or inhibit positive youth development (Bronfenbrenner, 1979).
Family Mechanisms
According to attachment theory and numerous empirical studies, the love and nurturance of at least one stable caregiver, usually a parent, is important for healthy development (Ainsworth & Bowlby, 1991; Prior & Glaser, 2006). For example, caregiver support predicts lower stress in African American, Hispanic, and White adolescents (Santiago, Etter, Wadsworth, & Raviv, 2012) and positive mother-adolescent relationships predict higher self-esteem among African American youth (Cooper & McLoyd, 2011; Laursen, Furman, & Mooney, 2006). Additionally, parent support buffers against depression in the context of environmental stressors among African American youth (McMahon, Coker, & Parnes, 2013).
Aside from relationships with any particular caregiver, more general family cohesion is marked by the emotional bonding that exists between family members, which decreases the likelihood that adolescents will engage in non-sanctioned behaviors (e.g., violence, substance use), and may help compensate for risk (Barnes, Hoffman, Welte, Farrell, & Dintcheff, 2007; Barr, Hanson, Begle, & Kilpatrick, 2012). Family cohesion has been positively associated with Latino children’s self-esteem (Leidy, Guerra, & Toro, 2010) and protective against substance use among Mexican-heritage and White youth (Kopak, Chen, Haas, & Gillmore, 2012). Family support protected against depression in the context of exposure to violence and poverty among African American early adolescents (Li, Nussbaum, & Richards, 2007).
Broader Social Mechanisms
The advice and encouragement from another adult outside the family, serving as a mentor, is also helpful in reducing psychological distress and problem behaviors and increasing positive attitudes toward school (Southwick, Morgan, Vythilingam, & Charney, 2006). For example, teacher support, in addition to family cohesion, was associated with more favorable outcomes in adolescents (Felner, Aber, Primavera, & Cauce, 1985) and perceived increases in teachers’ support predicted decreases in depressive symptoms and increases in self-esteem (Reddy, Rhodes, & Mulhall, 2003). In first-generation Latino youth, teacher support reduced internalizing symptoms (Potochnick & Perreira, 2010). Connection with teachers and peers has been associated with better health among African American and Latino youth (Solberg, Carlstrom, Howard, & Jones, 2007).
Supportive peer friendships may also promote resilience. Peer support is associated with fewer depressive symptoms and higher self-esteem (Weber, Puskar, & Ren, 2010) as well as higher global self-worth among African American youth (McMahon et al., 2011), reduced depression among African American and White youth (Vaughan, Foshee, & Ennett, 2010), and better general health among African American and Latino youth. (Solberg et al., 2007). Moreover, peer support buffers against depression in the context of stressful life events and environmental stressors (Brady, Dolcini, Harper, & Pollack, 2009; McMahon et al., 2013).
Aim and Hypotheses
This study is the first to examine separately and jointly family and social community factors as potential moderators of the effects of low SES among racially/ethnically diverse youth. Diversity is extended here to include Hispanic in addition to African American youth, of which there is a dearth of prior research. African American, Hispanic, and White youth constitute 90% of the childhood population (Child Trends Databank, 2014). Moreover, we extend previous work that has focused on specific health outcomes and problem behaviors by examining the broader outcome of QL. This study will examine family-based and broader social processes, as suggested by the ecological systems theory (Bronfenbrenner, 1979), that are hypothesized to protect against the effects of low SES reducing QL in youth from different racial/ethnic groups. More specifically, we hypothesize that family cohesion, nurturance from a parent caregiver, and social support from other adults and peers will moderate the negative QL associated with low SES among African American, Hispanic, and White youth, such that these social characteristics can be identified as protective mechanisms. We focus on youth in early adolescence, in fifth grade at ages 10 to 11, at an important juncture in development just prior to their transition to middle school.
Method
Participants
Data are from Healthy Passages,™ a multi-site community-focused study of health and health behaviors and their correlates among African American, Hispanic, and White youth (see Windle et al., 2004, and Schuster et al., 2012, for overviews) and were collected in 2004-2006. Participants were recruited from public schools located in three communities defined as (a) 10 contiguous public school districts in and around Birmingham, Alabama; (b) 25 contiguous public school districts in Los Angeles County, California; and (c) the largest public school district in Houston, Texas. The sampling frame consisted of public schools with an enrollment of at least 25 fifth graders, representing more than 99% of students enrolled in regular classrooms in the three areas. Schools and students were selected by using a two-stage probability sampling procedure with school-selection probabilities that were designed to achieve similar numbers of African American, Hispanic, and non-Hispanic White participants. Design and non-response weights were constructed so that weighted results represented the population of fifth graders in the public schools in each area. Information on the study was disseminated to the fifth-grade youth in the 118 selected schools to bring to their parents (or caregivers), which was a potential pool of 11,532 students. Youth were excluded from participation if they were not attending a regular academic classroom or if they or their parents could not complete interviews in English or Spanish.
A total of 6,663 (58%) parents returned permission to be contacted, of which 5,147 (77%) completed both a parent and a child interview. The Institutional Review Board’s (IRB) approved protocol did not allow for further contact with families that did not return the permission to contact form. To focus on the three major race/ethnic groups, the 6% who were not identified by their parents as being African American, Hispanic, or White (see details below) were eliminated from the current analysis. Of the 4,824 constituting the final sample, the unweighted (weighted) distribution was 36% (30%) African American, 38% (47%) Hispanic, and 26% (23%) White, and youth age
Distribution of SES and Site Variables.
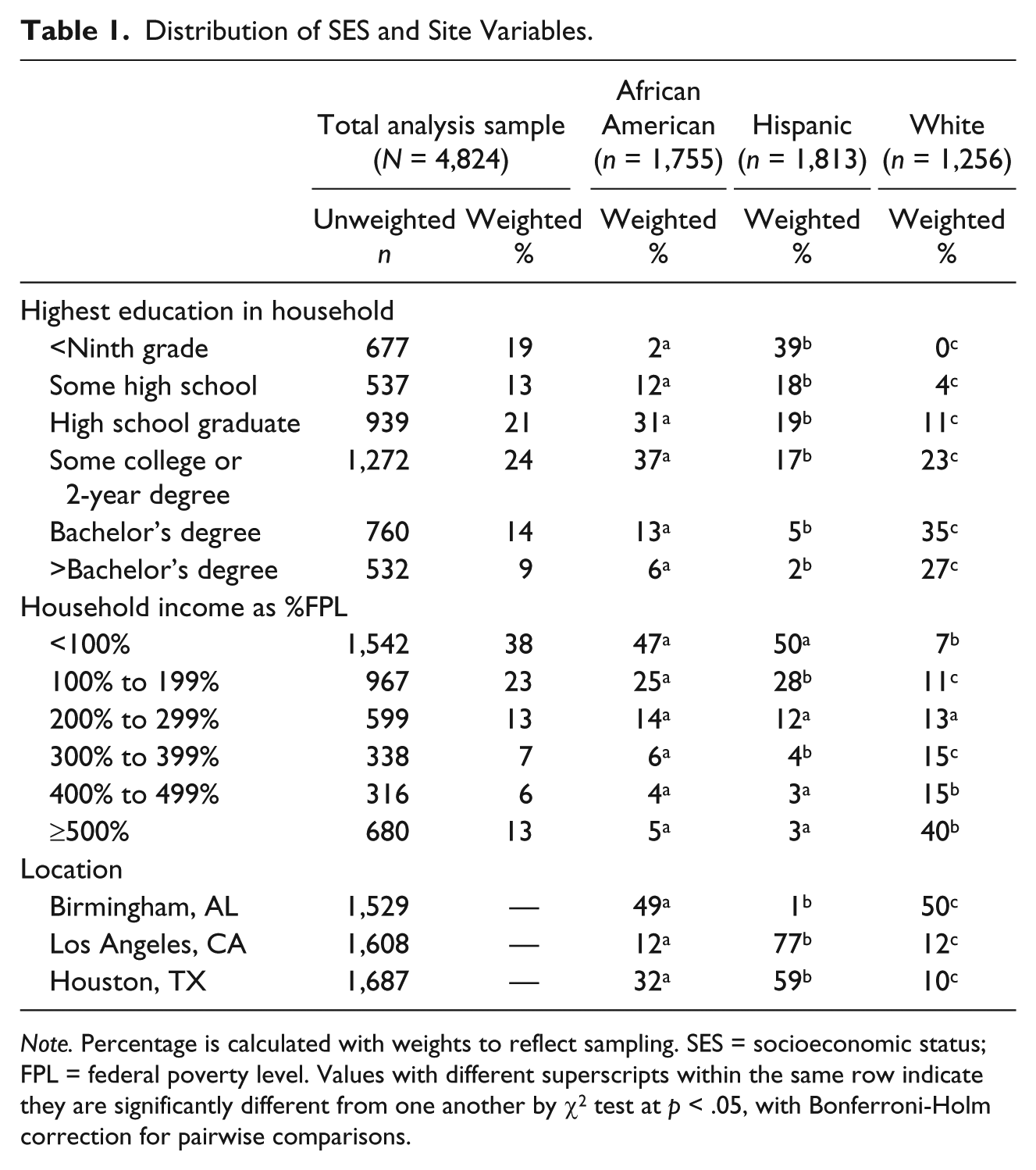
Note. Percentage is calculated with weights to reflect sampling. SES = socioeconomic status; FPL = federal poverty level. Values with different superscripts within the same row indicate they are significantly different from one another by χ2 test at p < .05, with Bonferroni-Holm correction for pairwise comparisons.
Procedures
Following standard procedures approved by the IRB at the three sites and the Centers for Disease Control and Prevention, two trained interviewers completed the full Healthy Passages™ assessment protocol with a child and one of his or her parents (mother, 88%; father, 6%; other, 6%) at their home or a research facility. The parent provided signed informed consent and the child signed assent. The interviews were conducted using both computer-assisted personal and self-interview procedures in English or Spanish with the child and parent separated in private spaces (Windle et al., 2004); 8% of the child interviews and 23% of parent interviews were conducted partly or fully in Spanish (prepared using standard back-translation).
Measures
QL is construed as a broad, multidimensional construct indicating a life of quality (Ravens-Sieberer et al., 2008; Wallander, 2001). Therefore, three dimensions of QL were measured with self-report forms, physical health-related QL, psychological health-related QL, and self-esteem, to reflect this broader conceptualization of QL.
The Pediatric Quality of Life Inventory Version 4.0 (PedsQL; Varni, Seid, & Kurtin, 2001) is a widely used, well-validated measure of the health-related dimensions of QL in childhood. For example, in a study involving 5,653 2- to 16-year-olds, the PedsQL demonstrated high construct validity when healthy youth reported significantly higher QL in all domains than chronically ill peers (Varni, Burwinkle, Seid, & Skarr, 2003). The PedsQL provides multiple subscales according to a structure that has been replicated across multiple racial/ethnic groups and ages (Limbers, Newman, & Varni, 2009). To reduce the number of correlated outcome measures, we restricted analysis to the Physical (8 items, α = .72; all reported αs are for the present sample) and Psychosocial (15 items, α = .84) Health-Related QL scales here, in which the latter scale is a composite of the Emotional, Social, and School subscales. Each item asked how much a certain behavior has been a problem in the past month (e.g., “I worry about what will happen to me,” “Other kids do not want to be my friend,” “I have trouble keeping up in school”). Answers were reported on 5-point scales (0 = never a problem, 4 = almost always a problem), but scale scores are calculated such that higher scores indicate better QL and transformed to a 0 to 100 scale.
The Self-Perception Profile for Children (Harter, 1983) Global Self-Worth subscale (6 items, α = .70) was used to measure the self-esteem dimension of QL (Ravens-Sieberer et al., 2008; Wallander, 2001). This subscale has demonstrated strong 3-year test-retest stability youth (Granleese & Joseph, 1994). Construct validity support is provided, for example, by substantial differences in scores between healthy youth and their peers with depression and anxiety problems (Muris, Meesters, & Fijen, 2003). Youth are asked for each item to identify which contrasting description best fits them (e.g., “Some kids like the kind of person they are, other kids often wish they were someone else,” “Some kids don’t like the way they are leading their life but other kids do like the way they are leading their life”) and how much (sort of true, really true). Higher scores indicate better self-esteem as a dimension of QL.
SES is multifaceted and no single variable adequately captures this construct (Chen et al., 2006), especially for racial/ethnic minorities (Wickrama, Simons, & Baltimore, 2012). SES was, therefore, measured as the mean of standardized (z score) parent-reported (a) highest level of education in the household and (b) net equivalent household income in the past 12 months, transformed as percentage of federal poverty level (see Table 1). The resulting composite is a continuous measure of SES, coded such that higher scores indicate higher SES, and was distributed as African American,
Youth race/ethnicity was based on the parent’s report when asked whether the child belongs to any of several Hispanic groups, followed by which of 15 races applied, consistent with the Office of Management and Budget standards. Hispanic ethnicity was determined using Census-Style classification, wherein the child was classified as Hispanic if the parent indicated this ethnicity regardless of responses regarding race. Children not categorized as Hispanic were classified based on parent report as African American, White, or Other (the 6% in the latter category were removed from the analysis sample).
Family cohesion was measured using the Family Cohesion subscale (10 items, α = .82) from the Family Adaptability and Cohesion Evaluation Scales–III (Olson, 1985), which was designed to assess the degree of emotional bonding among family members. Various studies have found support for the reliability and validity of the Family Cohesion subscale (e.g., Green, Harris, Forte, & Robinson, 1991). Examples of questions include “Family members feel very close to each other” and “We like to do things with just our immediate family.” Parents provided answers on 5-point scales (1 = almost never, 5 = almost always), which were summed to indicate higher familial cohesion.
Parental nurturance was measured using the Maternal (7 items, α = .74) and Paternal (6 items, α = .79) subscales derived from the Barnes Parental Nurturance Scale (Barnes & Windle, 1987). These scales assess the quality and quantity of parental guidance and support by child report. Both subscales have shown good reliability and validity (Mrug et al., 2008; Mrug, Gaines, Su, & Windle, 2010). If more than one parent was indicated as supportive, the highest scoring one was chosen to represent parental nurturance. Youth provided answers on 4-point scales (1 = almost never, 4 = almost always), which were summed to indicate more nurturing relationships.
Peer support was measured by adapting a subscale (4 items, α = .80) from the Loneliness Scale (Asher, Hymel, & Renshaw, 1984), which assesses dissatisfaction with relationships with peers in the school setting and has been used in past studies to assess friendship adjustment and acceptance (Parker & Asher, 1993). The Loneliness Scale has shown good internal consistency, a stable factor structure, and convergent validity with other measures of peer relationships (Asher & Wheeler, 1985; Bagner, Storch, & Roberti, 2004). Examples of questions include “You have lots of friends at school” and “You feel left out of things at school.” Youth provided answers on 5-point scales (1 = always true about you, 5 = not true at all about you), which were summed to indicate higher satisfaction with peer support.
Other adult support was assessed using items devised for the Healthy Passages™ project (6 items, α = .60). Adapted from the Social Support Rating Scale (SSRS; Cauce, Hannon, & Sargeant, 1992; MacLean, Paradise, & Cauce, 1999), this inventory assesses the perceived helpfulness of a number of different individuals, such as teachers, ministers, or coaches, who are potentially available to youth for support. The SSRS demonstrated good test-retest reliability and validity in prior research (Lu, Jia, Zhang, Wang, & Wang, 2011). Although the internal consistency reliability estimate is only moderate, this is consistent with this measure not having scale properties but rather being an inventory of people who are supportive in the lives of youth. Youth provided answers on 3-point scales (1 = very helpful, 3 = not at all helpful), which were summed to indicate more adults being supportive.
Statistical Analyses
All analyses incorporated weights and accounted for the two-stage sampling structure of students within schools using linearization (Windle et al., 2004) and robust “sandwich” estimators (Korn & Graubard, 1999), respectively, as implemented by the survey (svy) commands within Stata SE 10 (Statacorp, College Station, TX). Independent and dependent variables were assessed to meet the assumptions for multiple regression; the parental nurturance variable required log transformations. Although not an aim of this research, we first performed Wald F tests as a preliminary analysis to compare the racial/ethnic groups for each of the four positive characteristics and three QL variables, controlling for gender and location.
The hypotheses regarding protective mechanisms were addressed by examining for significant interaction between the risk factor (low SES) and a hypothesized protective factor (i.e., family cohesion, parental nurturance, peer support, other adult support, respectively). All risk and protective variables were first standardized as z scores. We performed a series of multiple linear regressions with each of the three QL dependent variables (physical health-related QL, psychosocial health-related QL, and self-esteem) in separate analyses. Separate regressions were computed using each of the four positive characteristics and for Hispanic, African American, and White racial/ethnic groups separately. Each regression included gender and location as covariates, SES, one of the positive characteristics, and the interaction between SES and the positive characteristic in question. Significant interactions were interpreted following recommendations by Aiken and West (1991) by graphing regression lines for each protective mechanism one standard deviation above and below the mean, as well as at the mean (shown in Figures 1 and 2). We also performed multivariable regressions, entering the covariates, SES, and all four positive characteristics and their interactions with SES. However, because these analyses yielded identical significant results, the results from theses analyses are not reported here.
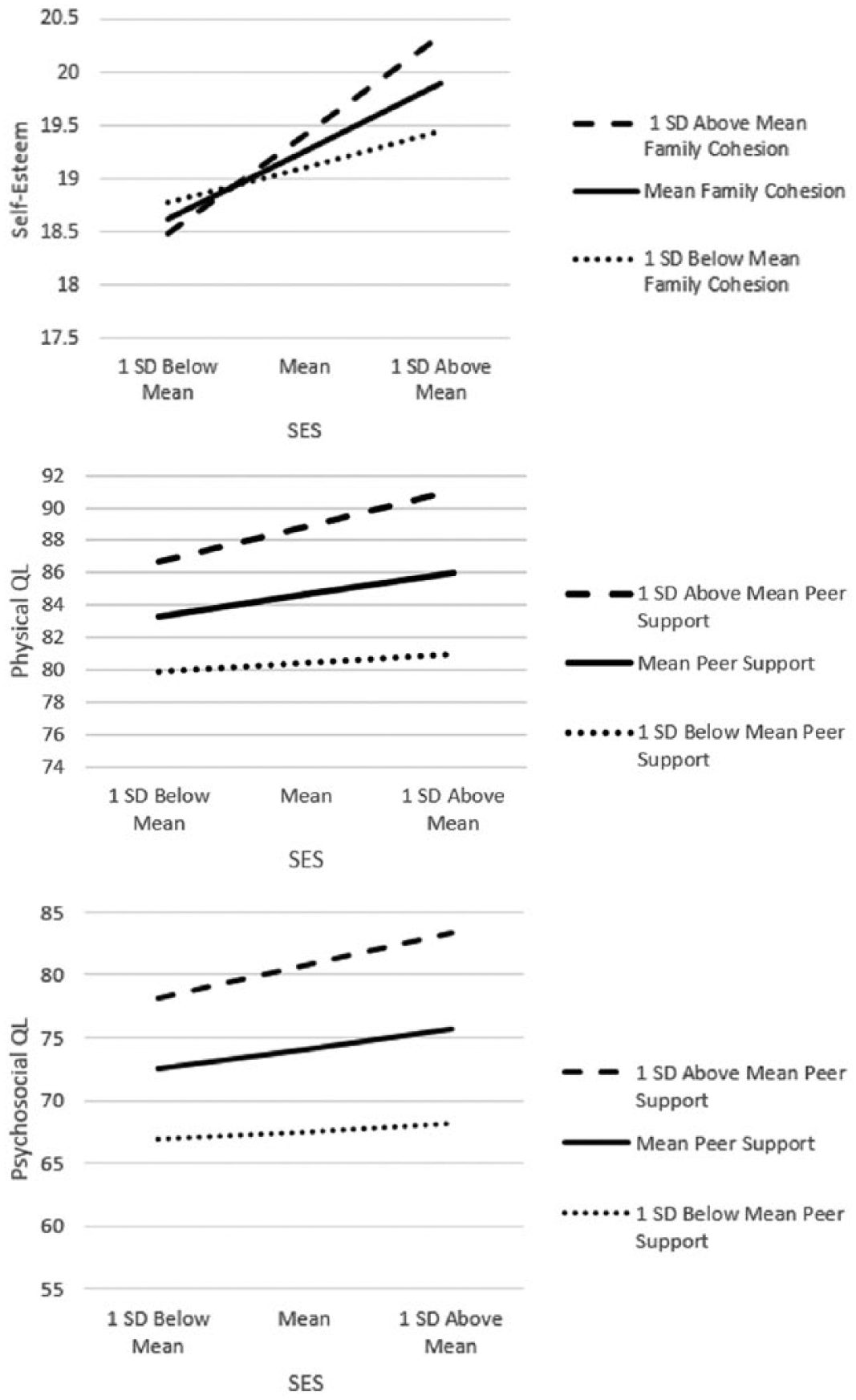
Illustrations of significant interactions among African American youth.
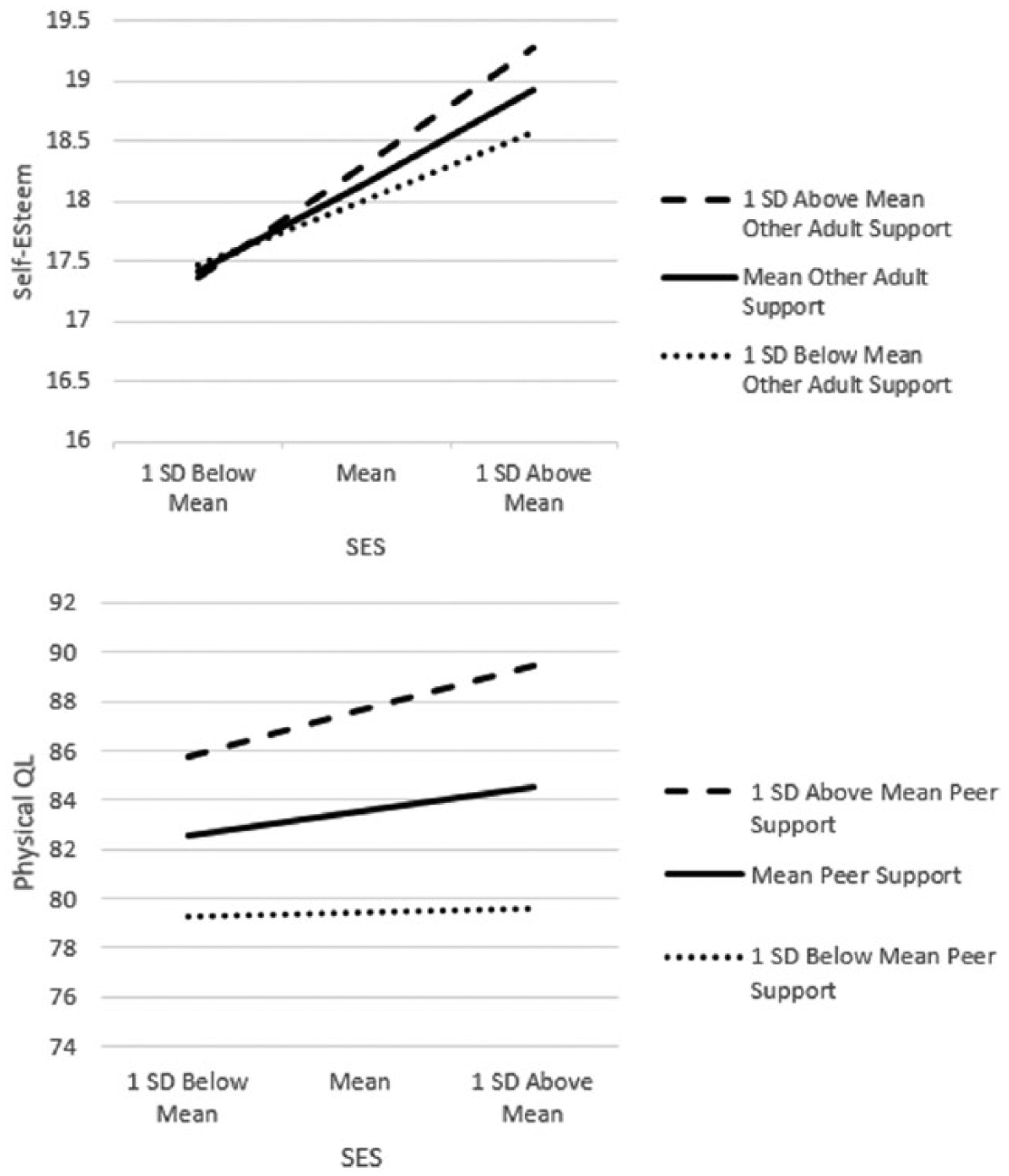
Illustrations of significant interactions among Hispanic youth.
Results
Although not an aim of this study, differences in positive characteristics and QL among the racial/ethnic groups are reported in Table 2 for descriptive purposes, and Table 3 shows the correlations among the study variables and their descriptive statistics. Results from regression of each QL variable on SES, single positive characteristics, and their interaction, controlling for gender and location, for each racial/ethnic group are shown in Table 4. Unless otherwise noted, the results were the same for the main effects regardless of whether they were assessed before or after the addition of the interaction terms to each model.
Disparities in Positive Characteristics and QL Associated With Race/Ethnicity.
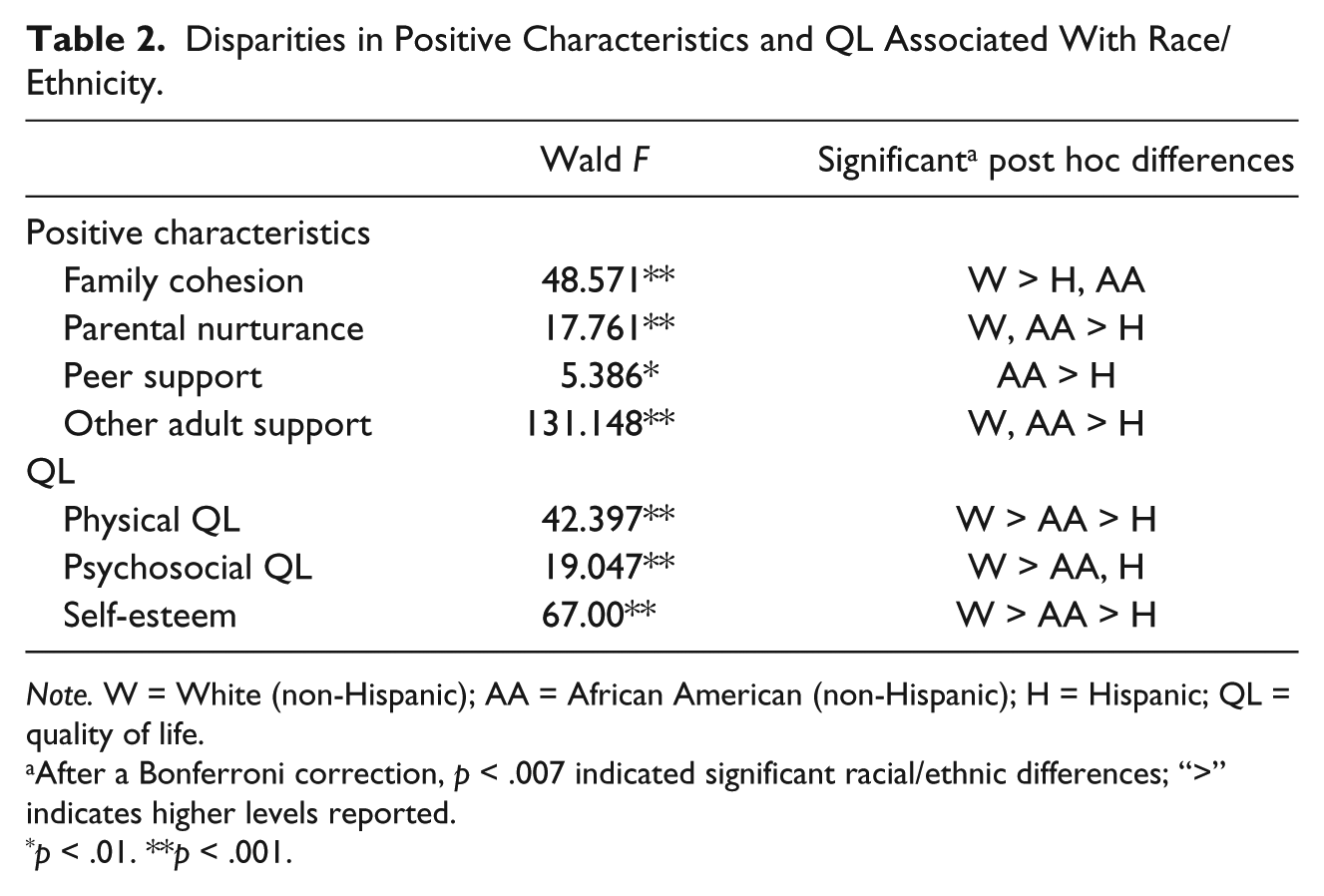
Note. W = White (non-Hispanic); AA = African American (non-Hispanic); H = Hispanic; QL = quality of life.
After a Bonferroni correction, p < .007 indicated significant racial/ethnic differences; “>” indicates higher levels reported.
p < .01. **p < .001.
Zero-Order Correlations and Descriptive Statistics for Study Variables.
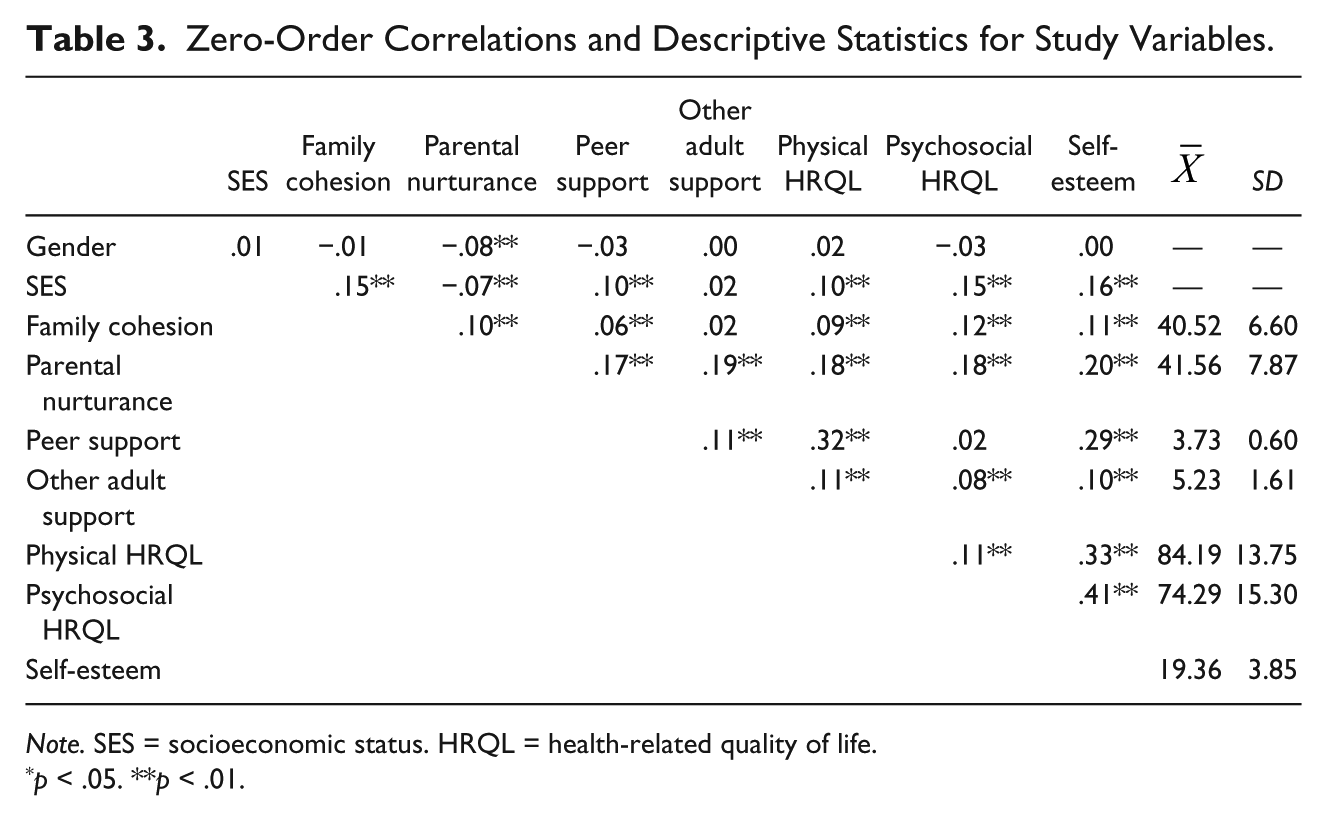
Note. SES = socioeconomic status. HRQL = health-related quality of life.
p < .05. **p < .01.
Regressions (Standardized Regression Coefficients in Final Model) of QL Variables on SES, Single Positive Characteristics, and Their Interactions Separately for Each Racial/Ethnic Group.
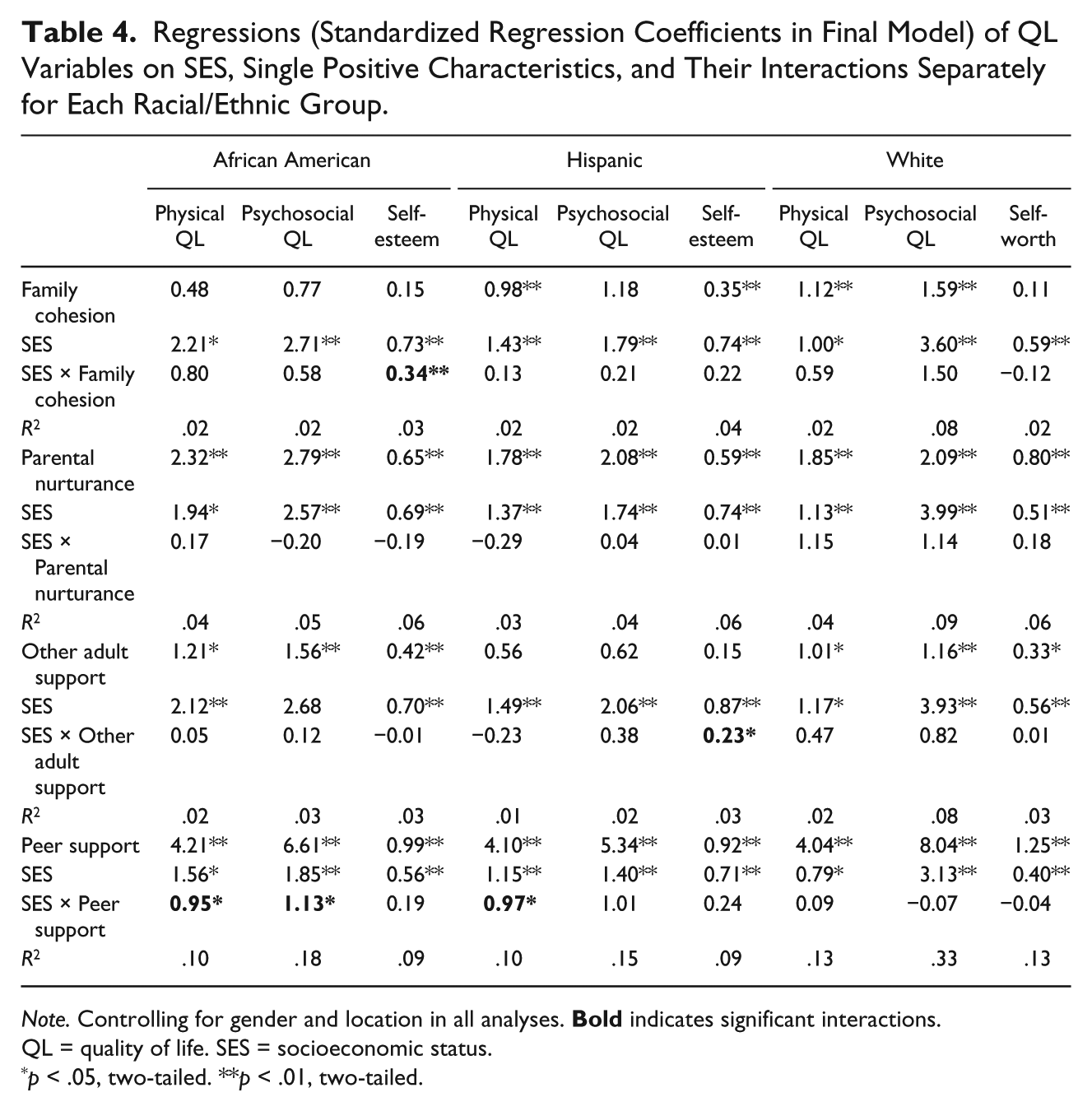
Note. Controlling for gender and location in all analyses.
QL = quality of life. SES = socioeconomic status.
p < .05, two-tailed. **p < .01, two-tailed.
Among African American youth, parental nurturance, other adult support, and peer support were positively associated with QL. There was a significant interaction between family cohesion and SES on self-esteem, F(5, 96) = 6.90, p < 0.001, as well as peer support and SES on physical health-related QL and psychosocial health-related QL, respectively, F(5, 96) = 41.58, p < 0.001 and F(5, 96) = 56.05, p < 0.001. Examining the illustrations of these interactions in Figure 1, it appears that family cohesion did not differentiate self-esteem at low SES, but did so primarily at higher SES. In the cases of peer support on physical as well as psychosocial health-related QL, there were differences in QL throughout the SES continuum, but this widened at higher SES.
Among Hispanic youth, family cohesion, parental nurturance, and peer support were positively associated with QL (see Table 4). There were significant interactions between other adult support and SES on self-esteem, F(5, 78) = 11.33, p < 0.001, and peer support and SES on physical health-related QL, F(5, 78) = 40.84, p < 0.001 When examining the illustrations of these interactions in Figure 2, it appears that other adult support did not differentiate self-esteem at low SES, but did so primarily at higher SES. In the case of peer support on physical health-related QL, there were differences in QL throughout the SES continuum, but this widened at higher SES.
Finally, among White youth, parental nurturance, other adult support, and peer support were positively associated with all QL dimensions, whereas family cohesion was so only with physical health-related QL (see Table 4). Once the interaction terms were added to the model, family cohesion was positively associated with psychosocial health-related QL as well. However, there were no significant interactions between any positive characteristic and SES on any QL variable for this group.
Discussion
Although all positive social characteristics were significantly positively correlated with QL dimensions, there were few indications that they moderated the relationships between SES and QL. Additionally, when significant interactions with SES were present, these positive characteristics appeared to be associated with higher QL primarily in youth at higher SES. More specifically, whereas family cohesion among African American youth and other adult support among Hispanic youth did not differentiate self-esteem at low SES, it did so at high SES. Moreover, whereas peer support among African American and Hispanic youth was associated with physical and psychosocial QL differences throughout the SES continuum, the benefits associated with high peer support widened toward higher SES.
These findings are contrary to expectations that positive social resources foster resilience in youth exposed to risk conditions, such as low SES (e.g., Herbers et al., 2011). However, as noted in previous studies, the ability for positive characteristics to buffer risk is likely dependent upon the outcome of interest (McMahon, Grant, Compas, & Thurm, 2003; Rosenfeld, Richman, Bowen, & Wynns, 2006). In the interactions presented here, higher SES youth appeared to benefit more than lower SES youth. Furthermore, in three of the significant interactions presented here (the interaction between peer support and SES on physical QL among African American and Hispanic youth and the interaction between peer support and SES on psychosocial QL among African American youth), higher SES youth exhibited higher QL across levels of positive characteristics. Each of these interactions involves peer support, leading to the suggestion that peers may provide more positive effects in higher than lower SES youth. However, this finding may vary across risk and outcome variables and should, therefore, be examined in a variety of contexts. There were no significant interactions for White youth, perhaps because this group has other advantages that overshadow the effects of the positive characteristics examined here. Given that White youth exhibited the highest levels of most of the positive characteristics and QL outcomes considered here, the deleterious effects of low SES on QL may be less noticeable in this group.
Nevertheless, Bronfenbrenner’s ecological systems theory provides a useful perspective on these interactions. For example, the finding that peers provide more benefits for higher than lower SES youth would be helpful to consider within other aspects of the micro-systemic as well as the larger macro-systemic context. Among African American youth in particular, peers have a higher likelihood of exhibiting problem behaviors (Beaver, Wright, & DeLisi, 2011), which have been shown to negatively impact youth development (Nichols & White, 2001). Beyond the peer environment, racial discrimination may disrupt the protectiveness of peer support among lower SES African American youth. In contrast, the absence of an interaction with SES among White youth may be because they lack comparable systemic oppression that works in concert with SES in producing group differences.
One of the distinct contributions of this study is identifying differences in positive characteristics in racial/ethnic groups. Whereas parental nurturance and peer support were associated with QL for each racial/ethnic group and accounted for the majority of main effects, family cohesion was not related to QL among African American youth and other adult support was not related to QL among Hispanic youth. It is important to note that even though the majority of these positive characteristics did not have differential effects depending on SES, they were still associated with QL. In fact, it is interesting to note that peer support emerged as the strongest correlate of QL across groups, surpassing parental nurturance (as well as SES) in each analysis. Although it is known that peers increase in importance during the adolescent period, finding this in early adolescence is more surprising (Wentzel, 2009).
We expected family cohesion to be associated with QL among African American youth, but it emerged as significant only in combination with SES and only for self-esteem, contrary to previous research (Li et al., 2007). It is unclear why this is the case, but perhaps this is because lower SES youth may be interpreting family cohesion differently from higher SES youth. Compared with the other two health-related QL dimensions, self-esteem may also be more malleable and more affected by social resources. For example, self-esteem is the target of many successful adolescent interventions in diverse at-risk populations (e.g., Craig, McInroy, Austin, Smith, & Engle, 2012; Tan & Martin, 2013). Health-related QL is also a more concrete manifestation of broader QL than is self-esteem, which is largely subjective. That is, health-related QL is mainly manifested in terms of abilities (Varni et al., 2003), such as being able to play and do school work and is not likely to change quickly. In line with Bronfenbrenner’s theory, self-esteem is a more proximal indicator of health that is more closely tied to the protective mechanisms examined here.
Finally, it was unexpected that other adult support was not associated with QL among Hispanic youth given previous research showing that teacher support and mentoring of at-risk Latino youth yields decreases in depressive symptoms, anxiety, and problem behaviors (Barron-McKeagney, Woody, & D’Souza, 2001; Potochnick & Perreira, 2010). This may be due to the greater emphasis on adults inside, as opposed to outside, the family among Hispanic youth (Miranda et al., 2006; Skogrand et al., 2008). Again, this corresponds with Bronfenbrenner’s theory that interactions with individuals that are physically and emotionally closer to the youth, even within the same microsystem, will have a greater influence on youth outcomes. As shown in Table 2, Hispanic youth also exhibited lower levels of social resources and QL than White and African American youth. Therefore, the absence of expected interactions may be due to the low levels of these positive characteristics in SES groups, which may make it difficult to observe significant effects.
As this is the first study to our knowledge that examined social resources in different racial/ethnic groups, further research is needed to build this knowledge base so that it can inform interventions. Limitations of this study include foremost that these results are correlational, with the consequence it is impossible to infer whether these positive characteristics resulted in higher QL or vice versa. Therefore, these findings are best seen as generating hypotheses that can be tested in experimental designs. Moreover, the effect sizes were modest due in part to the complexity of the associations examined. Additionally, this study was conducted in three metropolitan areas in the United States, and may not generalize to the national population. Whereas the three largest racial/ethnic groups in the United States were examined in this study, encompassing 90% of all children, other racial/ethnic groups could not be included. Furthermore, the Hispanic participants resided primarily in the Houston and Los Angeles areas and, therefore, predominately represent a heritage from Mexico and Central America. Non-response bias may be an issue because we did not have permission to contact all parents. However, the sampling weights account for differential non-response by gender, race/ethnicity, and school, ensuring the representativeness of the weighted sample and reducing potential non-response bias. Another limitation is the inherent biases of self-report data. For example, youth who are more likely to report positive characteristics are also more likely to report higher QL. Shared method bias is also a possibility because all but one independent and all dependent variables were based on youth report. Nevertheless, we expect that the differential findings across groups help address this concern. Finally, the study sample consisted of youth mainly on the low to middle end of the SES spectrum.
By focusing on developmental assets important for a life of quality, rather than problem outcomes, this study provides a perspective on youth well-being that is lacking in a literature that over-emphasizes pathology. This approach provides a more balanced perspective on positive growth opportunities in youth at risk for developmental problems. Although SES has strong implications for QL, certain protective mechanisms may mitigate its effect or even provide an advantage for low SES youth. Masten (2011) called for greater translational synergy of basic and applied resilience frameworks. Despite the increasing number of resilience-based interventions, these efforts must contribute to an iterative process to bridge the “translational gap” between field work and theory.
To this end, if confirmed in further research, our findings can have implications for practitioners, school personnel, and parents. Given that positive characteristics are generally associated with better QL and likely buffer against other risk contexts, if not low SES, efforts to foster these characteristics should still be encouraged. Moreover, intervention and prevention programs are beginning to draw upon positive characteristics particularly valued by racial/ethnic minority youth, such as collectivism, in order to increase their effectiveness (Lopez, Garza, & Gonzalez-Blanks, 2012). Our findings regarding the lower amounts of social resources found among Hispanic youth in particular indicate that although these groups highly value family and community support, their resources are lacking. Interventions to build these positive characteristics and improve QL outcomes relative to White and African American youth are sorely needed.
Especially among at-risk youth, opportunities to develop developmental assets through school and after-school programs early in life may be beneficial. Such program could yield gains beyond increasing QL (Deković, 1999; Walters & Bowen, 1997). A recent meta-analysis of universal, school-based social and emotional learning (SEL) programs concluded that compared with controls, SEL participants demonstrated improved social and emotional skills, attitudes, behavior, as well as academic performance (Durlak, et al., 2011). SEL programs bolster youth’s social and emotional competences by fostering self and other awareness, mood management, self-motivation, empathy, establishing positive friendships, and handling challenges and situations effectively (Zins & Elias, 2006). These competences overlap with the positive characteristics shown here to be associated with better QL, even if overcoming the risks associated with low SES is difficult.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Healthy Passages Study was funded by the Centers for Disease Control and Prevention, Prevention Research Centers (Cooperative Agreements CCU409679, CCU609653, CCU915773, U48DP000046, U48DP000057, U48DP000056, U19DP002663, U19DP002664, and U19DP002665).