
Abstract
Youth with conduct problems present frequently depressive symptoms. Academic skills are thought to be a mediating variable by which conduct problems could lead to depressive symptoms. No studies have longitudinally compared this model among school-aged boys and girls with different levels of conduct problems. Cascade models were tested to examine the relations between conduct problems, depressive symptoms, and academic skills over a 3-year period, and whether the severity of conduct problems and gender moderated these associations. Participants were 381 children presenting early clinically significant conduct problems (44.9% female) and 363 children with low levels of conduct problems (48.8% female). While results did not show any cascade or indirect associations, they revealed different direct links between conduct problems or depressive symptoms and academic skills in the four groups. These findings suggest that conduct problems severity and gender differences should be considered in treatment planning.
Children with conduct problems are at greater risk of developing a comorbid problem, especially depression, during adolescence (Barker, Oliver, & Maughan, 2010; Polier, Vloet, Herpertz-Dahlmann, Laurens, & Hodgins, 2012). Conduct problems and depressive symptoms frequently co-occur in community samples (Costello, Mustillo, Erkanli, Keeler, & Angold, 2003; Maughan, Rowe, Messer, Goodman, & Meltzer, 2004; Stringaris, Lewis, & Maughan, 2014), and even more frequently in clinical samples (Polier et al., 2012). Epidemiological studies have shown that between 45% and 75% of youth with conduct problems may present concurrent depressive symptoms (Angold, Costello, & Erkanli, 1999; Maughan et al., 2004; Polier et al., 2012). While the prevalence of conduct problems in childhood is higher in boys than in girls, the presence of depressive symptoms in youth with conduct problems is reported more frequently in girls than in boys (Lehto-Salo, Närhi, Ahonen, & Marttunen, 2009; Stringaris, Maughan, Copeland, Costello, & Angold, 2013).
Studies have demonstrated that comorbidity between conduct problems and depressive symptoms is associated with a high stability of problems (Capaldi & Stoolmiller, 1999; Van der Giessen et al., 2013), with girls being more likely than boys to follow a trajectory characterized by high levels of conduct problems and depressive symptoms (Diamantopoulou, Verhulst, & van der Ende, 2011). However, no clear conclusion can be drawn from the extant literature with respect to the directionality of the longitudinal association between conduct problems and depressive symptoms, as the results of previous studies on these associations have been mixed and sometimes contradictory. For example, some findings supported the idea that conduct problems predict depressive symptoms in children (Gooren, van Lier, Stegge, Terwogt, & Koot, 2011; Luby, Gaffrey, Tillman, April, & Belden, 2014; Van der Giessen et al., 2013), while other findings supported an acting-out perspective (Carlson & Cantwell, 1980) in which depressive symptoms constitute a risk factor for conduct problems (Loukas, Ripperger-Suhler, & Horton, 2009; Poirier et al., 2016). Other results suggested however that depressive symptoms could inhibit the continuation of conduct problems (Masten et al., 2005). Specifically in girls, the two problems could also mutually influence each other (Hipwell, 2011; Ritakallio et al., 2008), which suggest that the links between conduct problems and depressive symptoms could also be bidirectional. Finally, in other studies, conduct problems and depressive symptoms appear highly correlated at the same time point but are not associated longitudinally with each other (Brensilver, Negriff, Mennen, & Trickett, 2011; Vieno, Kiesner, Pastore, & Santinello, 2008). These inconsistent results suggest that the longitudinal association between conduct problems and depressive symptoms might be better explained by other factors than their mutual influence.
Whether conduct problems occur with depressive symptoms because they arise from the same risk factors, or whether conduct problems and depressive symptoms precede and predict changes in each other are important questions that have been addressed recently in empirical studies by testing “cascade” models of psychopathology. These cascade models were developed to test the links described in theoretical models explaining the associations between conduct problems, depressive symptoms, and potential mediators in samples of children and adolescents (e.g., Klosterman, Connell, & Stormshak 2016; Vaillancourt, Brittain, McDougall, & Duku, 2013; van Lier et al., 2012; Yong, Fleming, McCarty, & Catalano, 2014). Studies that support the idea that depressive symptoms precede conduct problems are based on the acting-out model, which suggests that difficulty in managing irritability, a symptom of depression observed in children and adolescents (American Psychiatric Association [APA], 2013), may lead to conflicts with parents and peers. In turn, these conflicts may lead to acting-out behaviors and association with deviant peers, and, eventually, to more severe delinquency (Klosterman et al., 2016; Wolff & Ollendick, 2006). Most of these studies are however based on the Dual Failure Model (Patterson & Capaldi, 1990; Patterson & Stoolmiller, 1991), which explains that children with conduct problems begin school with low school and social skills. This lack of abilities will lead these children to “failures” in the school context (e.g., peer rejection or underachievement). In turn, each of these “failures” will contribute independently to increase the likelihood of the development of depressive symptoms. The Dual Failure Model has found support in the empirical literature (e.g., van Lier et al., 2012). However, within this model, low academic skills have been largely understudied compared to low social skills, even though academic skills were hypothesized in the Dual Failure Model among the main mediators of the association between conduct problems and depressive symptoms.
Despite the contribution of previous studies to our understanding of conduct problems and depressive symptoms comorbidity, there are still a number of questions that remained unanswered in this research area. Specifically, most studies have been conducted analyzing internalizing problems (anxiety and depression) rather than depressive symptoms specifically. While the results of these studies support the hypothesis that conduct problems are indirectly linked to an increase in internalizing problems via school or social failures, it is unclear whether this association will also be present if only depressive symptoms are considered, particularly in childhood. Although depressive symptoms are low in general population during this developmental period (Hankin et al., 2015), they are already high among children with conduct problems (Barker et al., 2010; Polier et al., 2012). As conduct problems and depressive symptoms comorbidity is associated with a high stability of both problems (Capaldi & Stoolmiller, 1999; Van der Giessen et al., 2013), it is important to examine the dynamic interplay between conduct problems, depressive symptoms, and academic skills over time from childhood to adolescence. Moreover, studies have longitudinally tested the models explaining conduct problems and depressive symptoms comorbidity among school-aged boys and girls. They, however, did not take into account the possible differences between children with low level of symptoms and those with early, clinically significant conduct problems. Effectively, in previous studies, children or adolescents presented symptoms of conduct problems and depressive symptoms in the normal range (T score < 55; for example, Burt & Roisman, 2010; Englund & Siebenbruner, 2012; Masten et al., 2005). The Dual Failure Model was however specifically developed to explain the presence of depressive symptoms in children with early conduct problems. Examining the potential differences between these two groups will allow us to verify if the links between conduct problems, academic skills, and depressive symptoms are similar, regardless of conduct problems severity. Therefore, the aim of this study was to explore specifically the direction of the associations between conduct problems, depressive symptoms, and academic skills in a sample of elementary school children with and without early clinically significant conduct problems.
The Role of Academic Skills: Cascade Models
The negative associations between conduct problems and academic skills (Bierman et al., 2013; Nocentini, Calamai, & Menesini, 2012; Riglin, Frederickson, Shelton, & Rice, 2013), and between depressive symptoms and academic skills (Frojd et al., 2008; Herman, Lambert, Reinke, & Ialongo, 2008; Verboom, Sijtsema, Penninx, Verhulst, & Ormel, 2014) are well established, but few studies have addressed the mutual associations between conduct problems, depressive symptoms, and academic skills over time. While academic skills were evaluated in some studies, other studies examined academic skills using scales measuring academic competence, academic achievement, grade point average, or a composite score combining these measures. Most of them also controlled for intellectual or cognitive ability, as this factor is strongly associated with academic skills (Burt & Roisman, 2010; Masten et al., 2005; Molianen, Shaw, & Maxwell, 2010; van Lier et al., 2010).
To our knowledge, six studies tested the Dual Failure Model (Patterson & Capaldi, 1990; Patterson & Stoolmiller, 1991), taking into account both social and school problems (Boots, Wareham, & Weir, 2011; Burt & Roisman, 2010; Klosterman et al., 2016; Vaillancourt et al., 2013; van Lier et al., 2012; Yong et al., 2014). Examining a community-based sample of children between 54 months and 15 years, Burt and Roisman (2010) found a cascade effect between conduct problems at 54 months and depressive symptoms in Grade 3; conduct problems were associated with lower academic achievement, which was, in turn, linked to an increase in depressive symptoms. Similarly, Van Lier et al. (2012) reported a negative indirect effect between conduct problems and depressive symptoms (via low academic achievement) in a community sample of children from 6 to 8 years old. Conversely, using a randomly selected sample of children from third to eighth grade, Vaillancourt et al. (2013) found that while lower grade point average was associated with higher scores of conduct problems 1 year later, there was no indirect effect of grade point average in the association between conduct problems and depressive symptoms. Yong et al. (2014) did not report a cascade effect between conduct problems and higher depressive symptoms among a community sample of students between Grades 4/5 and Grade 8. However, their results showed that conduct problems in Grades 4/5 were linked with lower academic achievement in Grades 6/7. Finally, Boots et al. (2011) did not observe any association between school problems (attitudes about school and school performance) and conduct problems or depressive symptoms in a sample of children aged 8 to 13 years, followed by every 2 years over a 6-year period. However, they found that depressive symptoms at Time 1 were linked with higher conduct problems at Time 2, which were in turn associated with higher depressive symptoms at Time 3. This variability in results raises the question regarding the generalization of previous results to the longitudinal associations between conduct problems, depressive symptoms, and academic skills specifically.
Comparable results were observed in studies focusing exclusively on academic skills: Englund and Siebenbruner (2012), Masten et al. (2005), and Molianen et al. (2010) found a negative cross-lagged relationship from academic competence to conduct problems and depressive symptoms. However, only Molianen et al. (2010), studying a sample of vulnerable youth, observed a cascade effect from conduct problems to depressive symptoms via low academic competence. Providing support for the “academic incompetence hypothesis” (Molianen et al., 2010; Vaillancourt et al., 2013), these results suggest that low academic skills could exacerbate conduct problems. In addition, Masten et al. (2005) and Molianen et al. (2010) reported that conduct problems predicted lower academic competence, while Englund and Siebenbruner (2012) found that elevated scores of depressive symptoms predicted lower academic competence among children living below the poverty level. Englund and Siebenbruner (2012) and Masten et al. (2005) did not find evidence of a direct effect of conduct problems on depressive symptoms but have highlighted the inhibitive effect of depressive symptoms on conduct problems from childhood to adolescence.
Many factors could explain inconsistent findings in previous studies, such as the variability in sample composition (e.g., children’s ages, conduct problems severity), measures used (standardized instruments, combination of items), concepts evaluated (e.g., externalizing problems, conduct problems), informants considered (parent, teacher, child), interval between measurement time points (1-10 years) and number of measurement time points (3-5). The discrepancies in the extant literature impede us from drawing conclusions regarding if the Dual Failure Model might explain the associations between conduct problems, academic skills, and depressive symptoms from childhood to early adolescence in children presenting different levels of conduct problems. However, clarification of these links remains important in order to obtain a more accurate understanding of the evolution of conduct problems, academic skills, and depressive symptoms in a developmental period where child behavior may be malleable to behavioral modification (Halfon & Hochstein, 2002).
Gender Differences in the Associations Between Conduct Problems, Depressive Symptoms, and Academic Skills
Conduct problems are observed more frequently in boys than in girls (Maughan et al., 2004), while depressive symptoms tend to be higher in girls than in boys, at least from adolescence (Costello et al., 2003; Stringaris et al., 2014). These findings underscore the importance of taking into account possible gender differences in the association between conduct problems, depressive symptoms, and academic skills. In the literature, the associations observed between conduct problems, depressive symptoms, and academic skills appeared similar among both boys and girls, as generally the links observed were gender invariant (Burt & Roisman, 2010; Englund & Siebenbruner, 2012; Masten et al., 2005; Vaillancourt et al., 2013; van Lier et al., 2012). To our knowledge, only Boots et al. (2011), Klosterman et al. (2016), and Yong et al. (2014) observed differences in boys and girls examining the role of academic skills in explaining the comorbidity between conduct problems and depressive symptoms, as the links observed were only significant for boys in the three studies. More specifically, Boots et al. (2011) suggested that in boys, both depressive symptoms and conduct problems were associated with lower academic skills, while Yong et al. (2014) noted, also in boys, that academic achievement was associated with higher depressive symptoms only. Klosterman et al. (2016) reported that conduct problems in sixth grade were indirectly linked with higher depressive symptoms in ninth grade via lower academic achievement in seventh and eighth grades in boys but not in girls. These results also support the relevance of studying gender differences in the model.
The Current Study
The Dual Failure Model (Patterson & Capaldi, 1990; Patterson & Stoolmiller, 1991) has received some support in studies on the association between conduct problems, depressive symptoms, and academic skills in community samples of children and adolescents. As we already mentioned, further inquiry is needed, however, to verify if the mechanisms that contribute to the longitudinal associations between conduct problems, depressive symptoms, and academic skills are similar among boys and girls with and without early and significant conduct problems. Therefore, the aim of this study is to extend the findings of previous studies by evaluating a series of cascade models examining the longitudinal relations between conduct problems, depressive symptoms, and academic skills from childhood to early adolescence. This study compares a series of three nested models including four repeated measures, and tests possible differences in the links observed between boys and girls with and without early, clinically significant conduct problems. Reception of school-based mental health services for conduct problems, children’s age, cognitive abilities, and peer rejection at study inception were introduced in the final model to examine their potential effect on the links observed. According to the Dual Failure Model, conduct problems at an earlier time point would be associated with lower academic skills (an increase in school difficulties), which will, in turn, be linked to higher depressive symptoms at a later time point among children with different levels of conduct problems. Academic skills will be a mediator of the link between conduct problems and depressive symptoms.
Method
Participants
The sample includes all children participating in an ongoing longitudinal study on gender differences in the evolution of conduct problems throughout childhood (n = 744, 46.6% female, 98.6% French Canadian). In the present study, these children were divided into two groups: children with clinically significant conduct problems at study inception (n = 381, 44.9% girls) and children with low levels of conduct problems (n = 363, 48.8% girls). All children were recruited before age 10 (
Two strategies were used to recruit a relatively large number of children (particularly girls) with conduct problems before age 10. The majority of the sample (n = 370) was recruited from the list of children receiving school-based mental health services for conduct problems in public elementary schools. School-based mental health services varied for each child, as they were based on individual needs. They may include, for example, behavioral contracts, instructional accommodations, and/or psychological services. Most students (near 80%) received these services in regular classrooms, while about 20% received their services in special education classrooms. From the list of children receiving school-based mental health services, all girls less than 10 years and approximately one of four boys were randomly selected and invited to participate in the study. No differences emerged from the rates of participation of boys and girls, nor in grade level or deprivation index of school attended. The participation rate was 75.1%. Exclusion criteria were living in a foster family, or having comorbid intellectual or sensory disability or pervasive developmental disorder. In the present study, children were included in the clinically significant conduct problems group if they had a conduct disorder or an oppositional defiant disorder according to a diagnosis interview (Diagnostic Interview Schedule for Children [DISC 2.25]; Breton, Bergeron, Valla, Berthiaume, & St-Georges, 1998; Shaffer et al., 1993), or if they had a score above the clinical threshold (T score ≥ 70) on the Diagnostic and Statistical Manual of Mental Disorders (DSM)-Oriented Scales for Conduct Problems or Oppositional Defiant Problems, or on the Syndrome Scale of Externalizing Problems of the Achenbach System of Empirically Based Assessment (ASEBA; Achenbach & Rescorla, 2001), based on parent or teacher report (see the section “Measures”). With these criteria, 302 of the 370 children were included in the clinically significant conduct problems group, and 68 were included in the low levels of conduct problems group.
A complementary strategy for recruitment of children with conduct problems consisted of a multigated method of screening in classes to identify students who presented with early conduct problems but who were not receiving school-based mental health services. This method was applied to 881 students (first-third grade) from schools with an elevated deprivation index (participation rate = 71.5%). As above, no differences emerged from the rates of participation of boys and girls, nor in grade level. Using the same criteria as mentioned above, 79 of the 881 children were retained in the clinically significant conduct problems group. Among children who did not meet inclusion criteria, approximately one of three students was selected randomly to be included in the group of children with low levels of conduct problems (n = 295). Given that school-based mental health services reception varied among children with conduct problems at study inception and that some children with low levels of conduct problems also received these services, the reception of services were controlled in the analysis.
Procedure
Children were recruited between 2008 and 2010. A research assistant met the children’s primary caregiver at home to complete questionnaires. At study entry, parents received a description of the study and signed a consent form approved by the Institutional Ethics Board (Université de Sherbrooke). The consent form included the permission to obtain information from the teacher about the child’s academic functioning as well as his or her behaviors at school. Research assistants conducted a standardized phone interview with teachers to complete questionnaires. The initial assessment (Time 0) was followed by annual assessments over a 3-year period (Time 1-Time 3). Parents and teachers received a modest financial compensation for their participation at each measurement time point. Attrition rates were 8.4% at Time 1, 8.7% at Time 2, and 13.1% at Time 3. Participation rates were 97.8% for 2 measurement time points, 95.7% for 3 measurement time points, and 90.3% for the 4 measurement time points.
Measures
Selection of children
The presence or absence of clinically significant conduct problems among children was determined on the basis of two taxonomic approaches: a clinical diagnostic approach based on DSM criteria and an empirical-quantitative approach, using dimensional rating scales and standardized thresholds. We have discussed elsewhere that, despite some overlap, the joint use of these two approaches was more precise to identify the presence of conduct problems among children (see Toupin et al., 2016). Consistent with these approaches, in the present study, the children included in the clinically significant conduct problems group or in the low-level conduct problems group were selected on the basis of their results on two instruments. First, the DISC 2.25 (Shaffer et al., 1993) was used to assess the presence of conduct disorder and oppositional defiant disorder among children. This structured diagnosis interview was used with parent and teacher to determine the presence or the absence of the two disorders according to the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; APA, 1987) criteria. The French version of the DISC 2.25, translated by Breton et al. (1998), was slightly adapted to meet the criteria for conduct disorder and oppositional defiant disorder in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000). Kappa values calculated between DSM-III-R and DSM-IV-TR versions for the two disorders were satisfactory for both parent and teacher report (Déry, Toupin, Pauzé, & Verlaan, 2004). The criteria of conduct and oppositional disorders are essentially the same in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). The second instrument was the ASEBA (Achenbach & Rescorla, 2001). Three scales from the ASEBA were used with parent and teacher as informants: the DSM-oriented scale for conduct problems (17 and 13 items in parent version and teacher version, respectively; Cronbach’s α > .89), the DSM-oriented scale for oppositional problems (five items in both versions; α > .83), and the syndrome scale for externalizing problems (35 and 32 items in parent version and teacher version, respectively; α > .93). The items are scored on a 3-point scale ranging from 0 (not true) to 2 (very true or often true). Children who obtained a T score of 70 or more (the clinical threshold corresponding to the 98th percentile) on either scales according to parent report or teacher report were considered having clinically significant conduct problems. Despite the important overlap between the three scales, each has proved to have a unique contribution in identifying children with clinically significant problems.
Conduct problems across time
The level of conduct problems was assessed across time with the parent and the teacher versions of the DSM-oriented scale for conduct problems of the ASEBA (Achenbach & Rescorla, 2001) mentioned above. This scale that includes antisocial and delinquent behaviors (e.g., threatens people, attacks people, lies, skips school) is the most consistent with the diagnosis criteria of conduct disorder listed in DSM-IV-TR (APA, 2000) and DSM-5 (APA, 2013). The higher score for each item present in the parent (17 items) and teacher (13 items) versions was used to create a cross-informant composite scale of 18 items. These scores were added to the score of the five items that were only present in the parent version (cruel to animals, runs away, sets fire, steals at home) or in the teacher version (behaves irresponsibly). The composite scale showed a good internal consistency at each time of measurement (α = .89-.91).
Depressive symptoms
Parents and teachers assessed depressive symptoms with eight items of the ASEBA (Achenbach & Rescorla, 2001), scored on a 3-point scale ranging from 0 (not true) to 2 (very true or often true). Previously identified by Lengua, Sadowski, Friedrich, and Fisher (2001), these items (is lonely, cries a lot, feels unloved, feels worthless, is overtired, talks of suicide, lacks energy, is sad) are 8 of the 12 items most closely related to the construct of depression in the ASEBA. For each item, the higher score according to parent or teacher was used to create a cross-informant composite score. The composite scale had an adequate internal consistency over time (α = .76-.81).
Academic skills
Four items from the Academic Success subscale from the Academic Performance Rating Scale (DuPaul, Rapport, & Perriello, 1991) served to assess children’s academic skills. These items (learns material quickly, quality of reading skills, quality of speaking skills, recall difficulties [reversed]) were rated by teachers with different 5-point scales. The composite score was created by averaging the four items. This scale had an adequate internal consistency over time (α = .85-.87).
Child age
Child age was calculated from the child’s date of birth and interview date.
Peer rejection
Two items (“What percentage of this student’s peers like and accept him/her?” and “What percentage of this student’s peers dislike or reject him/her?”) from the Teacher Peer Social Skills (Dishion & Kavanagh, 2003) were used to assess peer rejection. Items were rated on a 5-point scale ranging from 1 (very few) to 5 (almost all) (r = .73, p < .001).
Cognitive abilities
Children’s cognitive abilities were estimated with the Peabody Picture Vocabulary Test–Revised (Dunn & Dunn, 1981) at study inception. In this study, the stability of the instrument at 12-month intervals is high (r = .72-.75).
Statistical analyses
Associations between conduct problems, depressive symptoms, and academic skills were examined using autoregressive cross-lagged models in Mplus version 7.2 (Muthén & Muthén, 2014). According to Little’s test, χ2(340) = 447.12, p < .001, data are not missing completely at random (MCAR), indicating that covariances among observed data in study variables differ significantly from covariances among estimated missing data. The missing values analysis suggests, however, that data are missing at random (MAR), indicating that missingness mechanism may be predicted by other observed variables and does not depend on the level of any unobserved variables. This mechanism allows using maximum-likelihood robust (MLR, full-information) estimator, which exploits all the available data information to produce robust estimates, and accounts for possible nonnormal distribution in the study variables. Due to the use of MLR, chi-square differences tests between models were conducted using the Satorra-Bentler scaled chi-square. Fit was assessed following the benchmarks proposed by Hu and Bentler (1999) and Kline (2011) for global fit measures.
Cascade analysis
The first model of measurement included only autoregressive (stability) paths and the within-time covariance terms across the three factors. Correlations between residuals over time were allowed. All paths estimated in the first models were included in subsequent models. Direct paths from conduct problems to depressive symptoms and from depressive symptoms to conduct problems were added in Model 2, and indirect paths involving academic skills were included in Model 3.
Group analysis
Model 3 was retained to test for possible differences between the four groups (boys and girls with low levels of conduct problems, and boys and girls with early clinically significant conduct problems). Group differences were examined in a series of nested cascade models beginning with the most constrained model (with all paths constrained equal across the four groups, Model 4), followed by a model in which continuity, covariance, and residual paths were allowed to vary according to the severity of conduct problems (Model 5). In Model 6, cross-lagged paths were also unconstrained according to the severity of conduct problems. Next, we allowed continuity, covariance, and residual paths to vary according to child gender (Model 7). Finally, in Model 8, all constraints were removed.
Control variables analysis
Follow-up analyses were conducted using Model 8 to investigate the potential effects of school-based mental health services reception, child age, cognitive abilities, and peer rejection on conduct problems, depressive symptoms, and academic skills at Time 0, and their indirect effect on the study variables at other time points via significant pathways (Model 9).
Post hoc analysis
Post hoc analyses were conducted to test the indirect effect observed between conduct problems and depressive symptoms via academic skills in Model 9 using the bias-corrected bootstrapping estimator method.
Results
Preliminary Analysis
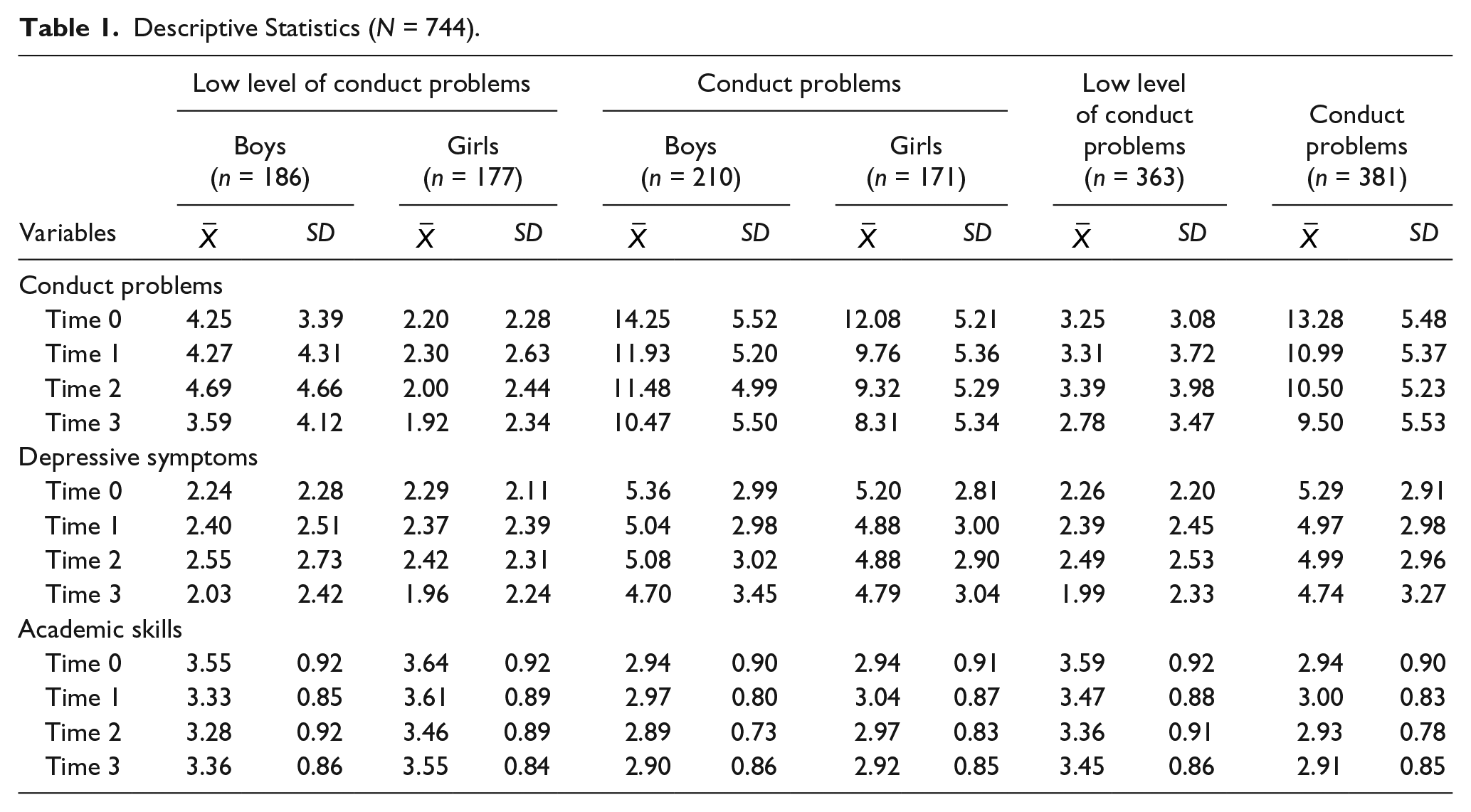
Descriptive statistics for conduct problems, depressive symptoms, and academic skills for boys and girls with low levels of conduct problems and for boys and girls with early clinically significant conduct problems at each time point are shown in Table 1. Overall, children with early clinically significant conduct problems had higher scores of conduct problems, F(1, 670) = 767.45, p < .001, depressive symptoms, F(1, 670) = 267.02, p < .001, and lower scores of academic skills, F(1, 498) = 67.88, p < .001, than children with low levels of conduct problems. Among children with early clinically significant conduct problems, boys and girls had similar means of depressive symptoms, F(1, 335) = .13, ns, and academic skills, F(1, 256) = .39, ns, but boys presented higher levels of conduct problems than girls, F(1, 335) = 19.03, p < .001. Among children with low levels of conduct problems, boys and girls also had similar means of depressive symptoms, F(1, 33) = .01, ns, but girls presented lower levels of conduct problems, F(1, 333) = 44.94, p < .001, and higher levels of academic skills than boys, F(1, 240) = 10.14, p < .05. Bivariate correlations among study variables for boys and girls in the low levels of conduct problems and in the clinically significant conduct problems groups are presented in Table 2.
Descriptive Statistics (N = 744).
Intercorrelations Among Conduct Problems, Depressive Symptoms, and Academic Skills for Boys and Girls According to Conduct Problems Severity.
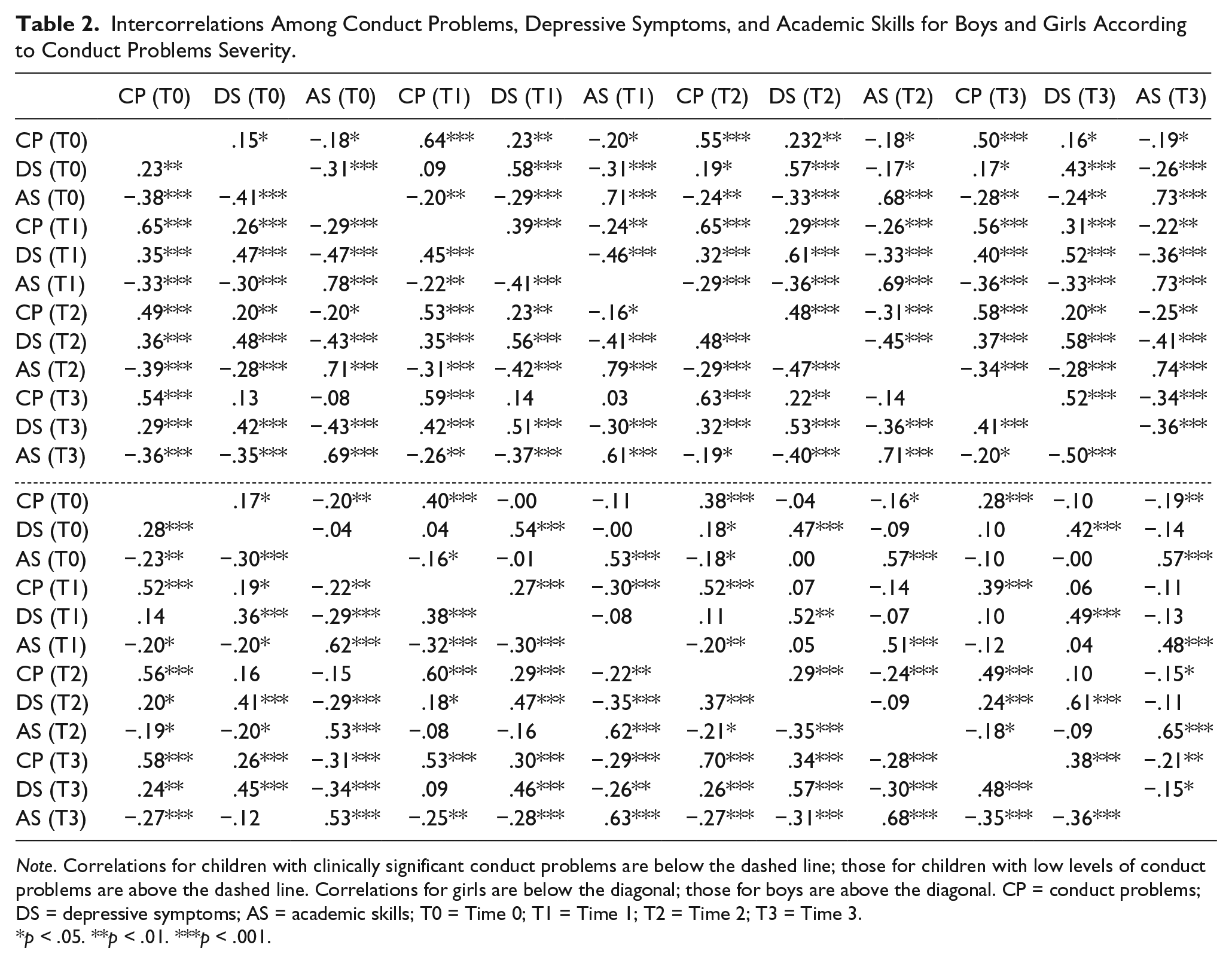
Note. Correlations for children with clinically significant conduct problems are below the dashed line; those for children with low levels of conduct problems are above the dashed line. Correlations for girls are below the diagonal; those for boys are above the diagonal. CP = conduct problems; DS = depressive symptoms; AS = academic skills; T0 = Time 0; T1 = Time 1; T2 = Time 2; T3 = Time 3.
p < .05. **p < .01. ***p < .001.
Cascade Analysis
Model fit statistics and model comparison are presented in Table 3. Model 3, including autoregressive paths, within-time covariance terms across the three factors, and all direct and indirect paths between conduct problems and depressive symptoms via academic skills, demonstrated an acceptable fit (comparative fit index [CFI] > .95, root mean square error of approximation [RMSEA] ideally < .06 but not higher than .10, and standardized root mean square residual [SRMR] < .08; Hu & Bentler, 1999; Kline, 2011). Model 3 also presented a better fit than Model 2, which had a better fit than Model 1, according to the chi-square differences tests.
Model Fit Statistics.
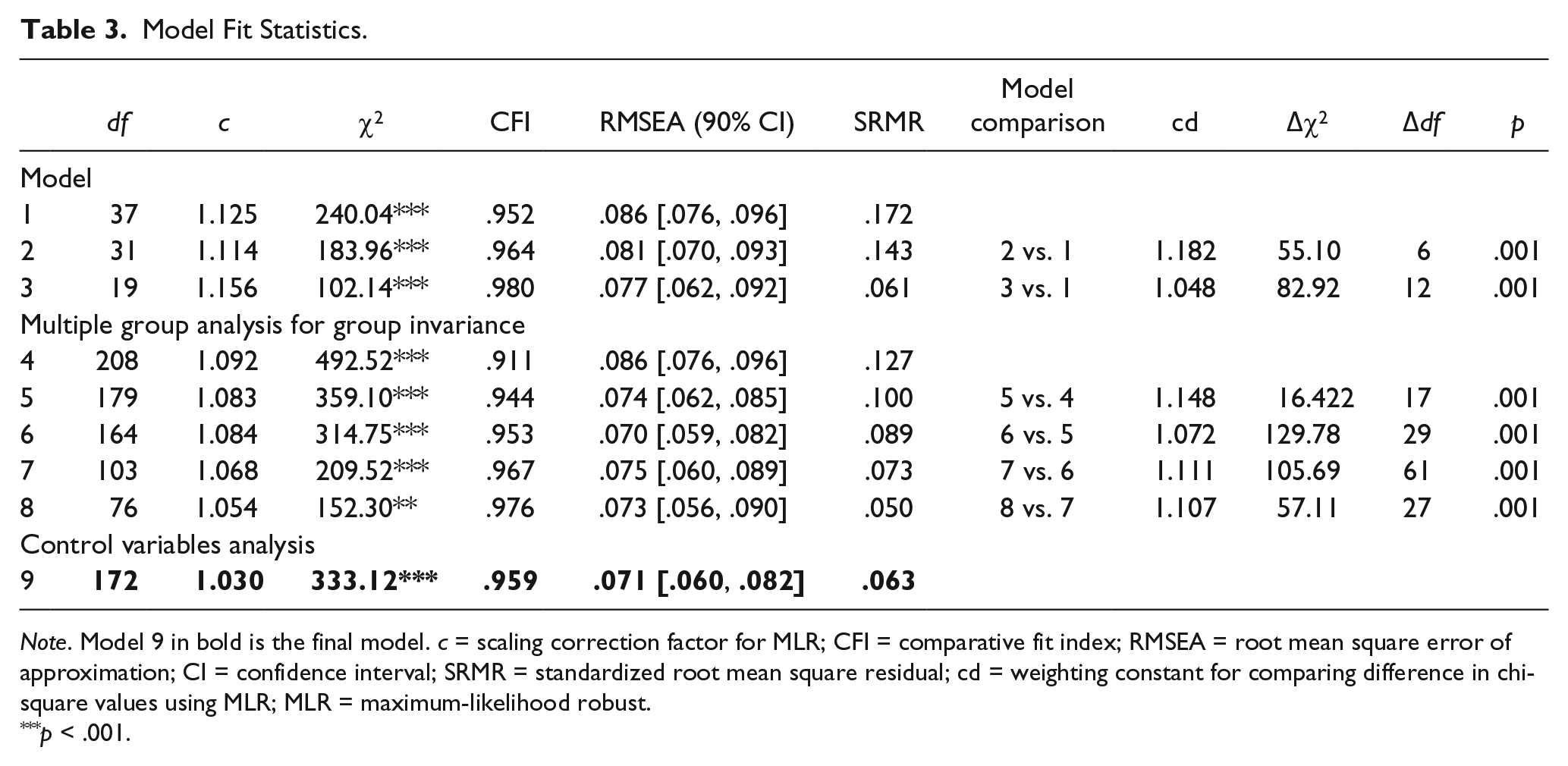
Note. Model 9 in bold is the final model. c = scaling correction factor for MLR; CFI = comparative fit index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean square residual; cd = weighting constant for comparing difference in chi-square values using MLR; MLR = maximum-likelihood robust.
p < .001.
Differences between boys and girls with different levels of conduct problems in cross-lagged longitudinal paths were tested using a multigroup analysis. A model constraining all paths to be equal for all children (Model 4) was compared to four models that allowed different paths to vary across groups. The inclusion of unconstrained covariance, residual and continuity paths (Model 5), and cross-lagged paths for children with different levels of conduct problems (Model 6) resulted in a significant improvement of the model fit according to the chi-square difference test. The inclusion of unconstrained covariance, residual and continuity paths (Model 7), and cross-lagged paths (Model 8) for boys and girls in the different levels of conduct problems groups also resulted in a significant improvement of the model fit according to the chi-square difference test. These results suggest that the links in Model 3 differ for boys and girls according to the presence of early clinically significant conduct problems. Model 8 presented an acceptable fit.
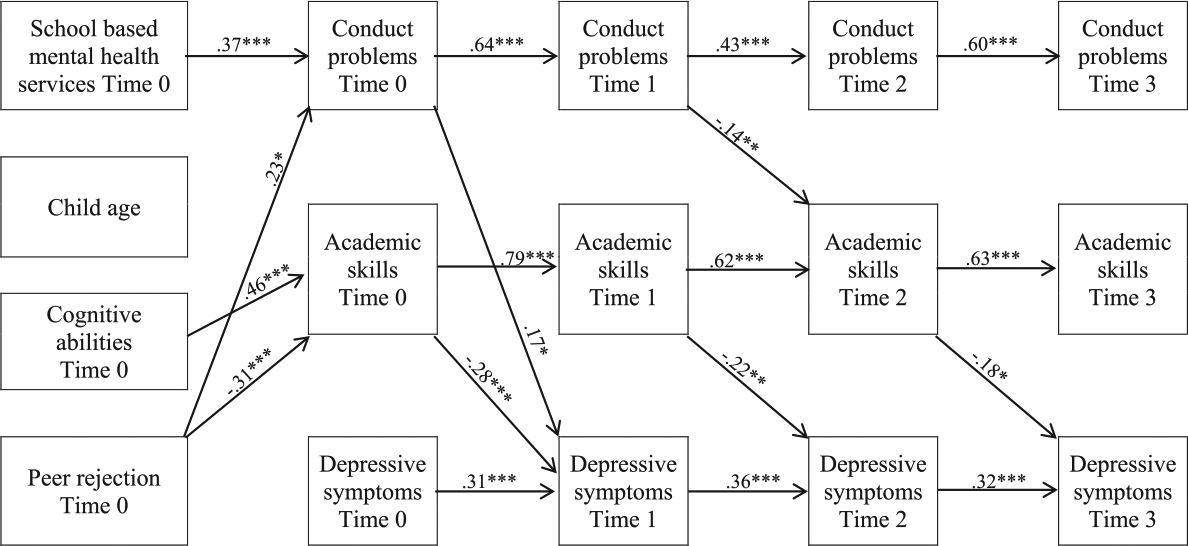
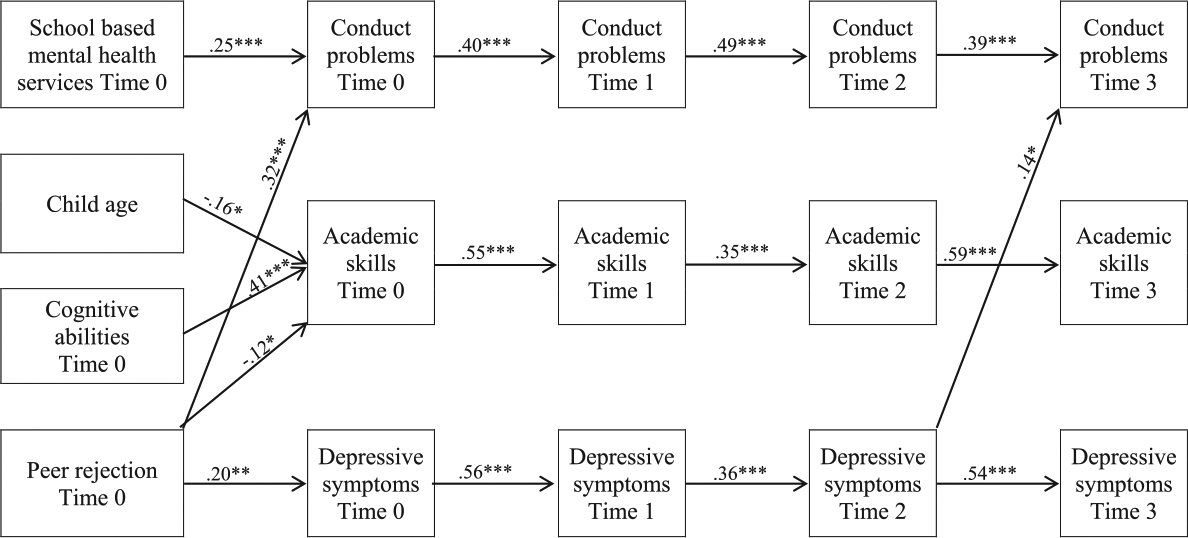
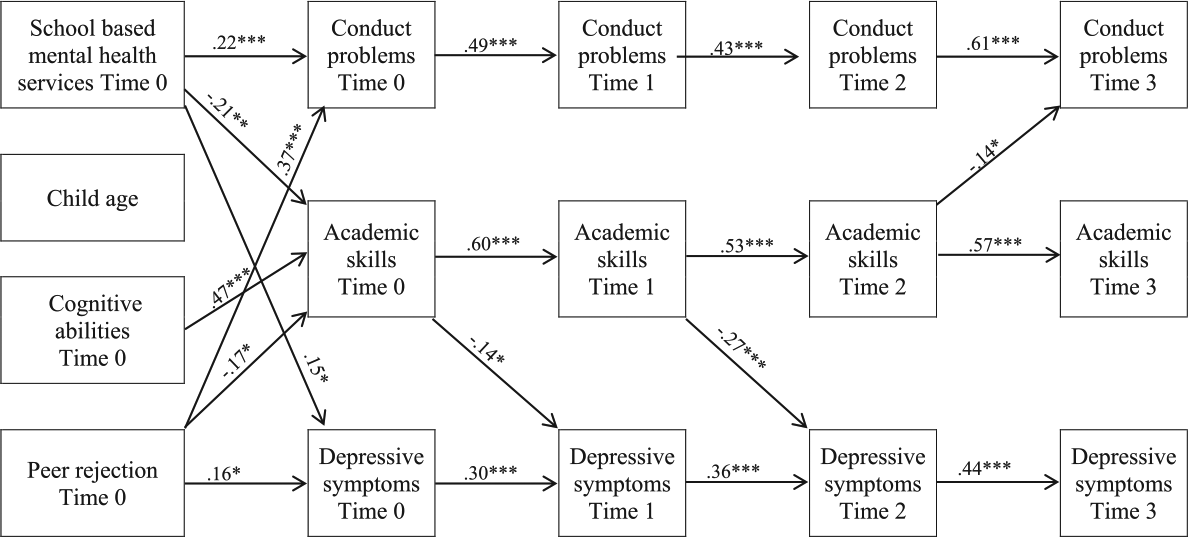
A further analysis was conducted to examine effects of control variables (school-based mental health services reception, child age, cognitive abilities, and peer rejection) at study inception in the final model. This addition resulted in a change in overall model fit, but the fit indices of Model 9 remained adequate. All significant cross-lagged paths in Model 8 were still significant after the inclusion of the control variables, apart from the link from depressive symptoms at Time 0 to conduct problems at Time 1 in girls with low levels of conduct problems, and from academic skills at Time 2 to depressive symptoms at Time 3 in girls with clinically significant conduct problems, that became nonsignificant. In the four groups (see Figures 1-4), reception of school-based mental health services and peer rejection were positively linked to conduct problems at Time 0. In girls with conduct problems, school-based mental health services were also linked to higher depressive symptoms and lower academic skills. Age was associated with lower academic skills only in boys with conduct problems, while cognitive abilities were associated with higher academic skills for all children. Peer rejection was associated with higher depressive symptoms in boys with low levels of conduct problems and in boys and girls with conduct problems. Peer rejection was also linked with lower academic skills in girls with low levels of conduct problems and in children with conduct problems.
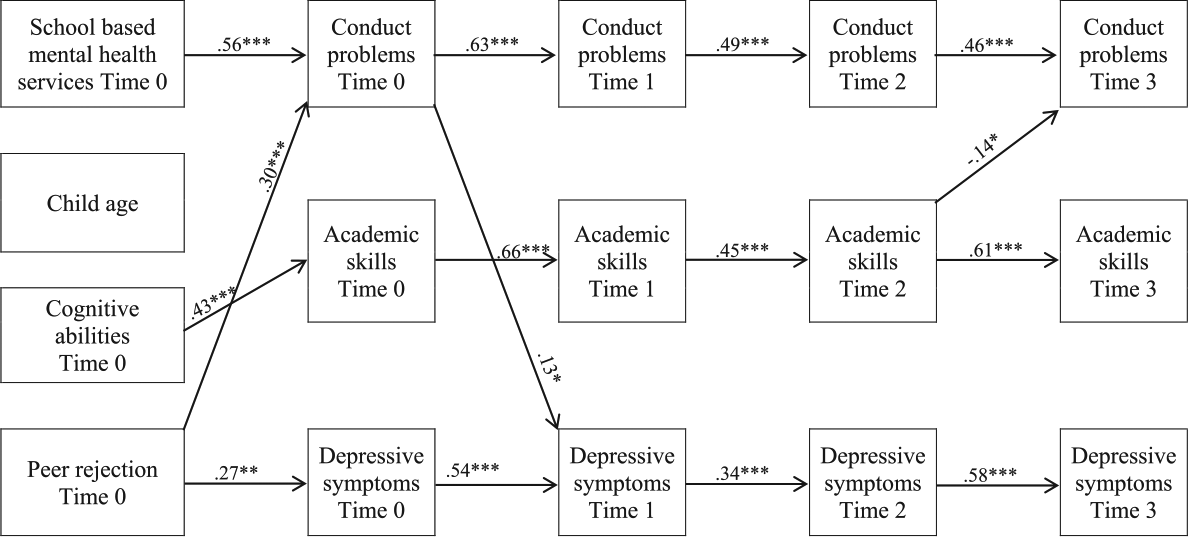
Standardized path coefficients for significant paths for boys with low levels of conduct problems.
Standardized path coefficients for significant paths for girls with low levels of conduct problems.
Standardized path coefficients for significant paths for boys with conduct problems.
Standardized path coefficients for significant paths for girls with conduct problems.
Specific Associations Between Conduct Problems, Academic Skills, and Depressive Symptoms for Boys and Girls With and Without Conduct Problems
Figure 1 shows standardized path coefficients from Model 9 for significant paths for boys with low levels of conduct problems. As expected, all stability paths are highly significant, suggesting a strong continuity in the three domains. These paths were also significant in the three other groups. There was no cascade effect from conduct problems to depressive symptoms via academic skills, and no association between depressive symptoms and academic skills over time in boys with low levels of conduct problems. However, lower academic skills at Time 2 predicted an increase in conduct problems 1 year later. Only one direct cross-lagged association was observed between conduct problems and depressive symptoms: Conduct problems at Time 0 predicted higher level of depressive symptoms at Time 1. In girls with low levels of conduct problems (see Figure 2), academic skills at Time 0 were negatively associated with depressive symptoms 1 year later. Moreover, conduct problems were directly and indirectly associated with depressive symptoms. At Time 0, conduct problems were positively associated with depressive symptoms at Time 1, while a possible cascade effect was observed from conduct problems at Time 1 to depressive symptoms at Time 3 via low academic skills at Time 2. Post hoc analysis conducted with the bias-corrected bootstrapping method revealed, however, that the indirect effect between conduct problems and depressive symptoms via academic skills was not significant, β = .03, p = .15. This result suggests that academic skills did not explain the association between conduct problems at Time 1 and depressive symptoms at Time 3: Conduct problems were rather directly associated with higher depressive symptoms 2 years later. In boys with conduct problems, only one significant cross-lagged path was observed (see Figure 3): Depressive symptoms at Time 2 were associated with higher conduct problems at Time 3. Finally, results presented in Figure 4 showed that the negative links between academic skills and depressive symptoms 1 year later observed in girls with low levels of conduct problems were also present in girls with conduct problems from Time 0 to Time 1, and from Time 1 to Time 2. Low academic skills at Time 2 were also linked to higher conduct problems at Time 3.
Discussion
The aim of this study was to examine the direction of the associations between conduct problems, depressive symptoms, and academic skills in a sample of elementary school boys and girls presenting with or without high level of conduct problems, and whether gender moderated these associations. The multi-informant procedure used to collect data and the longitudinal design of the study contributed to test the possibility of a cascade effect of conduct problems on depressive symptoms via low academic skills, in accordance with the Dual Failure Model (Patterson & Capaldi, 1990; Patterson & Stoolmiller, 1991). Our sample of children, recruited before age 10 and including roughly equal numbers of girls and boys, allowed us to evaluate the contribution of low academic skills in explaining the association between conduct problems and depressive symptoms in children with low levels of conduct problems and in those with early, clinically significant conduct problems. The Dual Failure Model was developed to explain the comorbidity between conduct problems and depressive symptoms in children with conduct problems, but the potential developmental cascading effect of academic skills has only been examined in community or “at-risk” samples with relatively low levels of conduct problems.
First, in line with our previous work (Poirier, Déry, Verlaan, Toupin, & Lemelin, 2015), our results suggest a relative stability of conduct problems, depressive symptoms, and academic skills across 4 measurement time points in the four groups. These findings indicate that the stability of functioning in various domains previously reported in community samples (e.g., Vaillancourt et al., 2013; van Lier et al., 2012) is also observed in children with early, clinically significant conduct problems. High levels of conduct problems and depressive symptoms and low levels of academic skills have been shown to increase the probability of negative consequences in high school children. For example, Englund and Siebenbruner (2012) demonstrated that these difficulties early in development are linked with adolescent alcohol and marijuana use. The stability of conduct problems, depressive symptoms, and academic skills is observed despite the fact that most children with high level of conduct problems received school-based mental health services. This result could suggest that a greater intensity of services is needed to prevent the negative consequences associated with these difficulties in elementary school children.
Second, our results, consistent with those previously reported by Englund and Siebenbruner (2012), did not support the hypotheses based on the Dual Failure Model (Patterson & Capaldi, 1990; Patterson & Stoolmiller, 1991). Among boys and girls with low levels of conduct problems, a positive association was found between conduct problems and depressive symptoms (Time 0-Time 1), such that higher levels of conduct problems were associated with higher levels of depressive symptoms. A positve link between conduct problems at Time 1 and depressive symptoms at Time 3 was also observed among girls. As previously discussed, findings in other studies supported the Dual Failure Model in community or at-risk samples with relatively low levels of conduct problems (Burt & Roisman, 2010; Klosterman et al., 2016; Masten et al., 2005; Molianen et al., 2010; van Lier et al., 2012). These findings and ours suggest that conduct problems could be linked directly or indirectly with higher depressive symptoms among children not already presenting high level of conduct problems in childhood. The absence direct or indirect effect from conduct problems to depressive symptoms in our study in the presence of high levels of conduct problems could be explained by the fact that children with early conduct problems already presented with higher levels of depressive symptoms and lower academic skills. In addition, these children could be less sensitive to school failures, which could explain the increase or the stability of conduct problems rather than the development of depressive symptoms. Indeed, the “academic incompetence hypothesis” (Molianen et al., 2010; Vaillancourt et al., 2013) was partially supported in this study: Low academic skills were linked to greater conduct problems 1 year later from Time 2 to Time 3 in boys with low levels of conduct problems and in girls with clinically significant conduct problems. However, low academic skills were also related to a higher level of depressive symptoms among girls with different levels of conduct problems from Time 0 to Time 2, and in girls with low levels of conduct problems between Time 2 and Time 3. Since these associations were not observed in boys, these results could indicate that academic skills are particularly a gender-sensitive variable for the development of depression in childhood.
It is also possible that the difference between our results with children with a high level of conduct problems and those of previous studies could be due to the variability in the measures used to assess school failures or academic skills. Effectively, academic skills and other concepts (e.g., academic achievement) could be differentially associated with depressive symptoms. The use of academic skills is however a strength of our study, as academic skills rather than other measures of school failures are included in the Dual Failure Model (Patterson & Capaldi, 1990; Patterson & Stoolmiller, 1991), and may contribute to a better understanding of the links hypothesized in this model.
Another possibility that could explain the absence of cascade associations in our study is that children with higher level of conduct problems were recruited before age 10. Though it was reasonable to examine these links in childhood, considering the fact that depressive symptoms are already high among children with high levels of conduct problems, it is possible that the indirect association between conduct problems and depressive symptoms via low academic skills could be better observed later in development, given that depressive symptoms tend to increase after puberty (Hankin et al., 2015). Longitudinal studies following participants from childhood to late adolescence remain necessary to explore the link between conduct problems, depressive symptoms, and academic skills later in development.
Concerning the direct and positive link between depressive symptoms and conduct problems, our results supported the acting-out perspective (Carlson & Cantwell, 1980) during the transition to early adolescence for boys with a high level of conduct problems, as depressive symptoms at Time 2 were associated with higher levels of conduct problems at Time 3. As explained previously, this relationship could reflect that some depressive symptoms (e.g., irritability) expressed with minor aggressive and delinquent acts could lead to conflict with parents, peers, and teachers, and eventually to association with deviant peers or involvement in more serious delinquency (conduct problems). These social failures, also included in the Dual Failure Model (Patterson & Capaldi, 1990; Patterson & Stoolmiller, 1991), could exert influence on the development of depressive symptoms in this population. Therefore, conflicts with significant others and deviant peer affiliation should be considered as potential mediators of the association between depressive symptoms, academic skills, and conduct problems. These links need however to be explored in future research.
The inclusion of control variables at Time 0 in the final model did not result in any significant changes in the cross-lagged paths observed at two exceptions: The link from depressive symptoms at Time 0 to conduct problems at Time 1 in girls with low levels of conduct problems and the link from academic skills at Time 2 to depressive symptoms at Time 3 in girls with conduct problems became nonsignificant. As expected, school-based mental health services reception was associated with higher conduct problems for all children and with higher depressive symptoms but lower academic skills for girls with clinically significant conduct problems. Age was only significantly associated with academic skills in boys with conduct problems. Cognitive abilities were associated with higher academic skills at Time 0 in the four groups. Finally, as suggested in the Dual Failure Model, peer rejection was associated with higher conduct problems in the four groups, and with higher depressive symptoms in children with high levels of conduct problems, and in boys with low levels of conduct problems. Peer rejection was also associated with lower academic skills in boys and girls with clinically significant conduct problems and in girls with low levels of conduct problems. These results suggest that peer rejection could be an important factor to include in future studies to better understand conduct problems and depressive symptoms comorbidity in children with early, clinically significant conduct problems.
Limitations
First, as discussed above, the links between conduct problems, academic skills, and depressive symptoms were observed during the elementary school period, and need to be examined until late adolescence. Effectively, other results could have been observed later in the development. Most children in the early clinically significant conduct problems group received school-based mental health services. Although service reception was statistically controlled in our analysis, this particularity of our sample could limit the generalizability of our results to children with high levels of conduct problems not receiving services. In addition, academic skills were assessed with only four items. Evaluating academic skills with a broader range of items, thereby taking into account a greater variety of academic skills, might lead to different results. This variable also reflects the teacher’s evaluation of the child’s abilities. It is possible that the child’s own perception of his or her school competence exerts a greater influence on his or her depressive symptoms than their abilities as rated by teachers. Moreover, a lack of statistical power limited our ability to examine the effect of peer rejection over time on the links between conduct problems and depressive symptoms. As peer rejection was positively associated with these two difficulties at study inception, at least in children with early clinically significant conduct problems, this social failure may influence the longitudinal links between conduct problems and depressive symptoms among children with high levels of conduct problems. Future studies should consider both types of failures to obtain a better understanding of the comorbidity between conduct problems and depressive symptoms.
Clinical Implications of the Findings
As discussed in the introduction to this article, children with early conduct problems are at high risk for continuity of conduct problems, as well as a host of negative sequelae throughout the life course. Identifying variables that could lead to a reduction in conduct problems among this vulnerable and difficult-to-treat population is therefore of utmost importance. The fact that these findings demonstrate that better academic skills were related to a decrease in conduct problems and in depressive symptoms 1 year later, at least among girls with a high level of conduct problems, has significant clinical implications. These results indicate a possible protective effect of school competency, and therefore suggest that one potentially interesting avenue for both treatment of conduct problems and prevention of other negative sequelae associated with conduct problems could be via interventions aimed at increasing academic success of these children.
In addition, while no links from conduct problems to later depressive symptoms were observed among children already presenting with a high level of conduct problems, our findings demonstrated that depressive symptoms at Time 2 were associated with an increase in conduct problems at Time 3 in boys from the high problem group. This suggests that the development or exacerbation of depressive symptoms is not negligible nor without consequence on conduct problems symptomatology in boys. Therefore, professionals working with this population of children should be sensitized to the importance of rapidly identifying and treating depressive symptoms should they develop in these children, not only because of the suffering that depressive symptoms can cause in children but also because of the implications that increases in depressive symptoms can have on levels of conduct problems over time.
Conclusion
This study showed that among girls with early clinically significant conduct problems, low academic skills at Time 0 and Time 1 were linked with higher depressive symptoms the following year, and low academic skills at Time 2 were associated with higher conduct problems 1 year later, which support the “academic incompetence hypothesis” (Molianen et al., 2010; Vaillancourt et al., 2013). Support for the acting-out model (Carlson & Cantwell, 1980) was also found in boys with early clinically significant conduct problems, as high depressive symptoms at Time 2 were associated with higher conduct problems at Time 3. These two models could be relevant to better understanding of the comorbidity between conduct problems and depressive symptoms in children with early conduct problems in the elementary school years. However, our results did not show an indirect link from conduct problems to depressive symptoms via low academic skills and, consequently, did not provide support for this variable of the Dual Failure Model (Capaldi, 1991, 1992; Patterson & Capaldi, 1990) in this subgroup. The mechanisms underlying the comorbidity between conduct problems and depressive symptoms among girls and boys with early clinically significant conduct problems should be clarified in future studies.
Footnotes
Acknowledgements
We thank the children, parents, and teachers who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (NRF 82694), and the Social Sciences and Humanities Research Council of Canada (SSHRC 37890). Support for this research was also provided by the Fonds de recherche du Québec—Société et Culture by means of a postdoctoral fellowship to the first author.