
Abstract
The study aimed to explore the development trend of positive mental health and the interaction between adolescents’ perceived family support and positive mental health. A 3-year longitudinal survey of perceived family support and positive mental health (resilience and self-efficacy) for four waves was conducted with 564 junior high school students (297 girls, mean age = 11.12 ± 0.38 years at baseline). The Latent Growth Curve Modeling indicated that adolescents’ resilience and general self-efficacy showed a curve upward trend, which increased first and then decreased. The development rate decreased each year. The cross-lagged panel model and a random intercept cross-lagged panel model concluded that perceived family support was strongly associated with positive mental health of junior high school students. Family support was important for developing positive mental health in early adolescence. Therefore, attention and interventions targeting positive mental health changes in early adolescence are particularly effective. And, it is important to encourage parents of adolescents to continue to provide support and guidance.
Keywords
Introduction
Positive mental health (PMH) in adolescence has received increasing attention from scholars and practitioners in recent years (Hall et al., 2016; Marino et al., 2018; Michaelson et al., 2019). The junior high school students are in the early developmental period of adolescent (10 through 14 years of age). This stage is dynamic, characterized by dramatic changes in the adolescents themselves (Rasalingam et al., 2017; Stapley et al., 2020), such as changes in their mental health (Fink et al., 2015; Pachucki et al., 2015). At the same time, positive mental health in early adolescence is also vital for the development of mental health in late adolescence and adulthood (Hendriks et al., 2020; O’ Connor et al., 2017; Thomson et al., 2017). Based on positive psychology, positive mental health has been defined by various researchers as positive emotions, or personality traits including self-esteem, positive self-evaluation, control of psychological resources, such as self-efficacy, and resilience (World Health Organization, 2005). Therefore, this study focused on the positive aspects of mental health, using resilience and general self-efficacy as indicators of positive mental health.
Resilience is considered an important component of positive mental health (Hu et al., 2020; Srivastava, 2011). Connor and Davidson (2003) argued that resilience is a characteristic that enables people to thrive in adversity. The researchers suggest that resilience includes the tenacity, strength, and optimism that individuals show when facing stress (Yu & Zhang, 2007). Tenacity means that when an adaptable person becomes frustrated, he or she will consciously integrate goal-setting, control, and decision-making behaviors. Strength means that adaptable people usually view change not as a threat, but as a normal part of life. They not only can return to their previous state of life, but also actively achieve new integration then further growth after overcoming adversity. Optimism represents an individual’s overall positive attitude, with belief that they can overcome adversity or risky situations. People with higher optimism may be inclined to believe they can access coping resources, thus have the confidence to overcome difficulties. Resilience fluctuates in early adolescence. Some longitudinal studies have shown that the resilience of adolescents shows an upward trend with time (De Caroli & Sagone, 2014; Liu et al., 2013; Okuyama et al., 2018; Sagone et al., 2020). Some age-specific studies have shown different results. For example, studies have shown that the resilience development of middle school students (6th to 8th grade) often decreases first and then increases (Yang, 2014). However, some studies have shown that students’ resilience development tends to rise first and then decline (6th to 7th grade; Zheng et al., 2021), or shows a downward trend of fluctuations (7th to 8th grade; Liu et al., 2021).
Several researches investigated the relationship between resilience and self-efficacy (Konaszewski et al., 2019; Sagone & Indiana, 2017; Schwarzer & Warner, 2013). General self-efficacy is a vital part of positive mental health (Srivastava, 2011; World Health Organization, 2005). It typically indicates an individual’s sense of control over his or her environment (Bandura et al., 1999). Schwarzer et al. (1997) posited that general self-efficacy is a basic assessment and confidence judgment of an individual’s ability to effectively deal with problems in various situations. Longitudinal studies have shown an upward trend in self-efficacy over time in adolescence (Grevenstein & Bluemke, 2015; Sheikh et al., 2016), which is consistent with a latent growth model (Phan, 2012). However, some studies have reported that adolescents’ self-efficacy of shows a downward trend with time (Burger & Samuel, 2017). This is consistent with a 2-year longitudinal study of junior high school students (Jhang, 2019). Adolescents’ self-efficacy is closely related to their resilience (Sagone & Caroli, 2013; Sagone et al., 2020).
Based on previous empirical studies, the developmental trend of positive mental health in early adolescence is controversial. Erikson’s psychosocial development theory (Erikson, 1980) argues that adolescence is a period of confusion in roles or identities. In the face of this stage of conflict, the mental health status of adolescents will also change. If adolescents are able to overcome these conflicts well, they will gain self-confidence (self-efficacy). Some researchers have also proposed that early adolescence is dynamic, is characterized by great changes within himself or herself such as physical maturity, pursuit of independence, significant increase in social or peer interaction, and brain development (Blakemore, 2008; Casey et al., 2008, 2010). Junior high school students are at this stage, which is characterized by dramatic and rapid change. They will face many pressures and challenges (Baer, 1999; Jhang, 2019; Roeser et al., 1998). It is precisely because of many stresses and challenges that mental health trajectories can shift in early adolescence (DeLay et al., 2017; Stormshak et al., 2011). Because of the changeability of this stage, the development of junior high school students’ positive mental health is often analyzed through longitudinal research. Latent growth modeling (LGM) is regularly used to explore a variable’s developmental trajectory. Compared with repeated measures analysis of variance, LGM focuses not only on trends in group changes but also individual differences in development (Duncan & Duncan, 2004). Therefore, we surveyed junior high school students in four waves over 3 years, used LGM to explore the development trends and individual differences of junior high school students’ positive mental health (i.e., resilience and general self-efficacy).
The ecological development theory (Bronfenbrenner, 1979) regards the environment as a dynamic process, and the development of individuals comes from the interaction of people and the environment. During adolescence, the positive mental health often mutable and susceptible to environmental influences (Kearney & Bussey, 2015; Lavoie et al., 2014). Previous studies typically focus on the impact of peers or schools on adolescent mental health (Oberle et al., 2018; Roach, 2018), ignoring the role of family. Adolescents have experienced many changes in the way they interact with their families, peers, society and themselves (Choudhury et al., 2006). These changes reflect the transformation of individual emotional support from family to peer, then to self and intimate partner. However, this does not mean that there is or should be separation from the family, as healthy psychological development is highly dependent on continuous positive interaction with family (Larson & Brown, 2007). And based on cultural factors, family relationship is more important in Chinese culture than in Western culture (Lam, 1997; Shek & Chan, 1999). Therefore, the role of family support in the development of Chinese adolescents cannot be ignored (Tisak et al., 2017). Family support can be seen as social support from the family, which offers emotional and other forms of support that enables adolescents to cope with developmental stressors (Cauce et al., 1990; King et al., 1995). Studies have shown that it is vital for parents to provide timely support during adolescence, especially in junior high school (Waters et al., 2014), which can affect one’s mental health status in adulthood (Rothon et al., 2012; Sheikh et al., 2016). Family support can foster the mental health of junior high school students (Kelly et al., 2012). A longitudinal study of adolescents in the 5th to 7th grades showed that positive parental support was stable over time. Family supports that adolescent receive early in life can improve their ability to successfully adapt to the developmental changes of early adolescence. That is, the family support received by adolescents at this stage can more stably predict subsequent positive psychological outcomes (Bronstein et al., 1996). This is also consistent with a study of adolescents in Shanghai, China (Chen et al., 2019). Family support also has a significant impact on Chinese adolescents’ positive mental health development (Guo et al., 2018). Compared with friend support, the central role of family support in it is still evident. (Hu et al., 2022). Studies in some Asian countries have found similar results, such as South Korea, where family support plays an important role (Cho & Haslam, 2010; Kim & Kim, 2008) and is strongly associated with positive mental health among adolescents (You et al., 2018). This finding is consistent with previous research showing the importance of perceived family support among Hong Kong immigrant adolescents in Canada (Chow, 2007). Family support is closely related to individual resilience (Pinkerton & Dolan, 2007; Puckett et al., 2019) and can predict subsequent levels of resilience (Wu et al., 2014; Koelmel et al., 2017). Moreover, family support and self-efficacy are positively correlated, as individuals who feel more supported by their families tend to have more confidence in their own abilities (Anderson et al., 2006; Guerra et al., 2018). Further, the optimization function of positive mental health plays an important role throughout adolescence. Students with high levels of positive mental health showed higher levels of social support, as well as relationship satisfaction, including relationship satisfaction with family members (Suldo et al., 2016). Adolescents with higher levels of positive mental health perform better on a range of dimensions of perceived social support (Magalhães & Calheiros, 2017). Junior high school students with positive mental health have better relationships with family members and therefore receive more support (Antaramian et al., 2010; Suldo & Shaffer, 2008).
This study aimed to determine the changes in positive mental health of junior high school students and the bidirectional relationship between perceived family support and positive mental health. Based on previous findings and theoretical models, early adolescence is a critical stage of psychosocial development (AlBuhairan et al., 2012). In the face of this stage of conflict and their own contradictions, the mental health status of junior high school students will also change (Casey et al., 2010). So, we hypothesized that positive mental health of junior high school students fluctuates (Hypothesis 1). Furthermore, the positive mental health often mutable and susceptible to family influences (Kearney & Bussey, 2015; Orpana et al., 2016). It is vital to extend previous research by elucidating the pathways to improve positive mental health in this population. Therefore, we hypothesized that adolescents’ family support and positive mental health may influence each other (Hypothesis 2).
Method
Participants
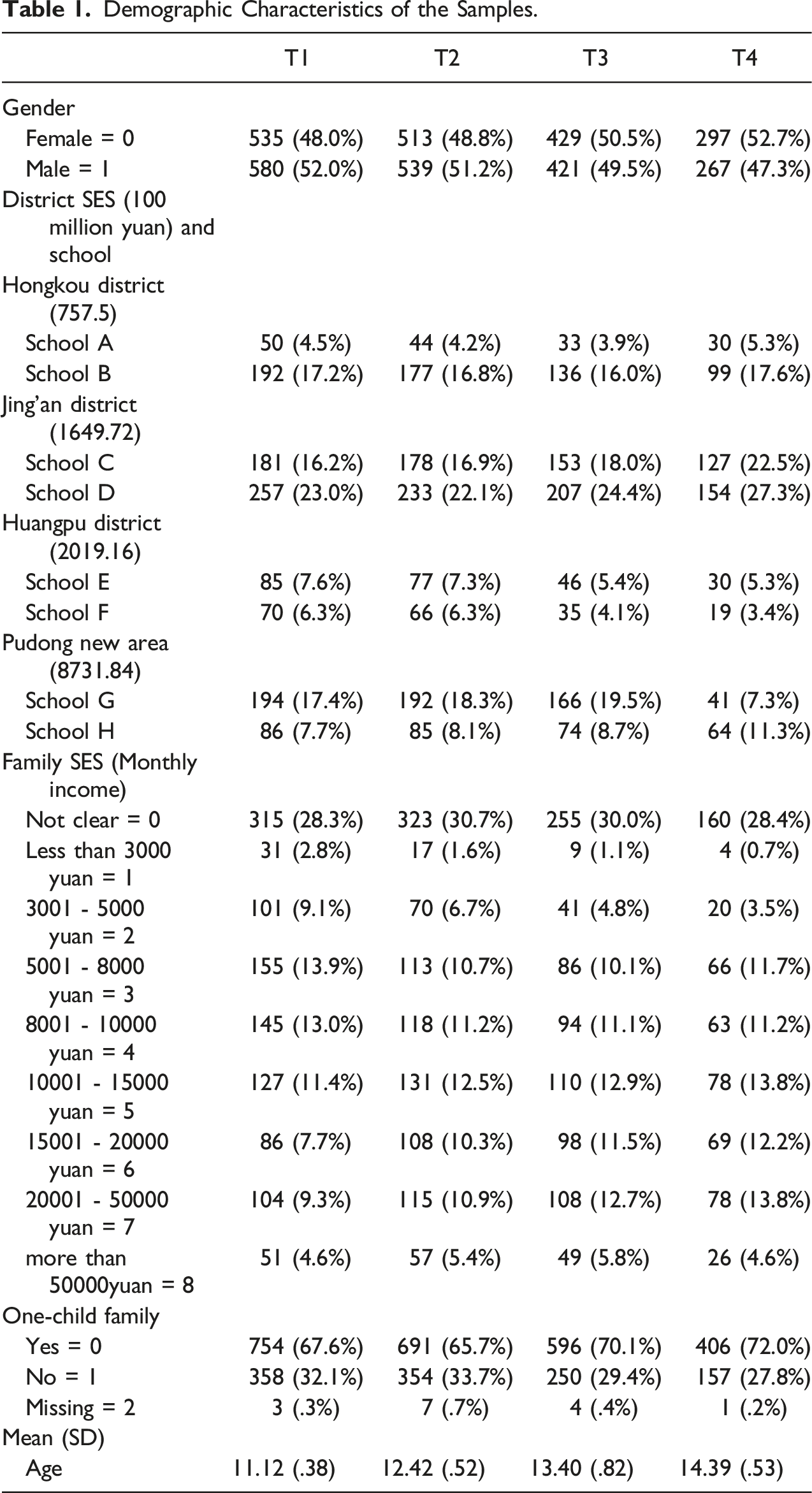
We selected sixth-grade students from eight schools in Shanghai as our population sample, including two private junior high schools and six public junior high schools. There were significant differences in family SES among the eight schools in Hongkou district, Jing’an District, Huangpu District and Pudong New District. According to documents published on the official website of each district government, the GDP (100 million yuan) these districts in 2016 were: Hongkou District (757.5; Shanghai Hongkou District People’s Government, 2018), Jing’an District (1649.72; Shanghai Jing’an District People’s Government, 2017), Huangpu District (2019.16; Shanghai Huangpu District People’s Government, 2017) and Pudong New Area (8731.84; Shanghai Pudong New Area People’s Government, 2018).
Demographic Characteristics of the Samples.
Measures
Personal Resilience
Chinese version of the Connor-Davidson Resilience Scale (CD-RISC; Connor & Davidson, 2003) revised by Yu and Zhang (2007) was used to measure resilience. There were 25 items in the scale, including the tenacity subscale (thirteen items, e.g., “I believe I can achieve my goals even if there are difficulties.”), the strength subscale (eight items, e.g., “No matter what the environment changes, I can adapt.”) and the optimism subscale (four items, e.g., “When faced with a problem, I try to look on the bright side.”). Participants respond on a 5-point Likert-type scale, ranging from 0 (never) to 4 (always). Cronbach’s α coefficients for resilience in the four surveys conducted in this study were .89, .91, .94, and .93, respectively.
General Self-Efficacy
Chinese version of the General Self-Efficacy Scale (GSES; Schwarzer et al., 1997) was used to measure general self-efficacy. There are 10 items (e.g., “If I try my best, I can always solve the problem.”) in this scale and the score ranges from 10 to 40 points. The higher the score, the higher the level of self-efficacy. The internal consistency coefficient of the Chinese version of GSES is .87, and the retest reliability is .83 (Wang et al., 2001). Cronbach’s α coefficients of general self-efficacy in the four surveys conducted in this study were .82, .88, .92, and .91, respectively.
Perceived Family Support
We used the family support dimension (four items, e.g., “My family was able to help me in a practical and concrete way.”) of the Perceived Social Support Scale (PSSS; Blumenthal et al., 1987), as revised by Jiang (1999). The revised internal consistency coefficient for this dimension is .87 (Jiang, 1999). Participants respond on a 7-point Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Higher scores of the scale indicate higher the perceived level of family support. Cronbach’s α coefficients for perceived family support in the four surveys conducted in this study were .84, .90, .90, and .92, respectively.
Data Collection
Participants filled out the questionnaire during the school’s activity class or class meeting time, and each class arranged for two trained psychology graduate students or psychology teachers as experimenters, who are members of the research team. Before each survey, an experimenter explained the principles of confidentiality to the students, and asked them to fill out the questionnaires according to the instructions. Each questionnaire took approximately 20−30 minutes to complete.
All procedures were performed in accordance with the ethical standards of the appropriate institution and/or national research committee for studies involving human participants. Informed consent was obtained from all individual participants and their parents/guardians included in the study.
Some students cannot take the senior high school entrance examination in Shanghai due to the restriction of household registration. And they will transfer to a city where they can continue their studies in the eighth grade. Therefore, the attrition rate in the eighth-grade survey was higher. Missing data analysis showed that Little’s missing completely at random (MCAR) was significant (p < .001), indicating that the model violated the MCAR assumption to some extent. Further attrition analysis revealed that 50.6% of the sample at T1 continued to provide data at T4. We included all variables in the analyses and utilized list-wise deletion techniques to account for missing data. With list-wise deletion, it is possible to get a complete dataset, which in turn allows for the use of standard analysis techniques (Baraldi & Enders, 2010).
Common Method Bias
We tested whether common method bias was a serious threat to accurate testing of our hypotheses. Harman’s one-factor test was used, with all the items were loaded on a single factor (Podsakoff et al., 2003). The results of the one-factor model were not acceptable, χ 2 /df = 4.20, RMSEA = .075, CFI = .718, AGFI = .717, TLI = .703, SRMR = .070. In this study, we collected the data multiple times (four surveys) to avoid common method bias. Therefore, taken together, we are confident that common method bias did not affect the results of the study.
Results
Relation between Positive mental health and Perceived Family Support
Descriptive Statistics and Correlations of Variables of Positive Mental Health and Perceived Family Support of Junior High School Students (N = 564).
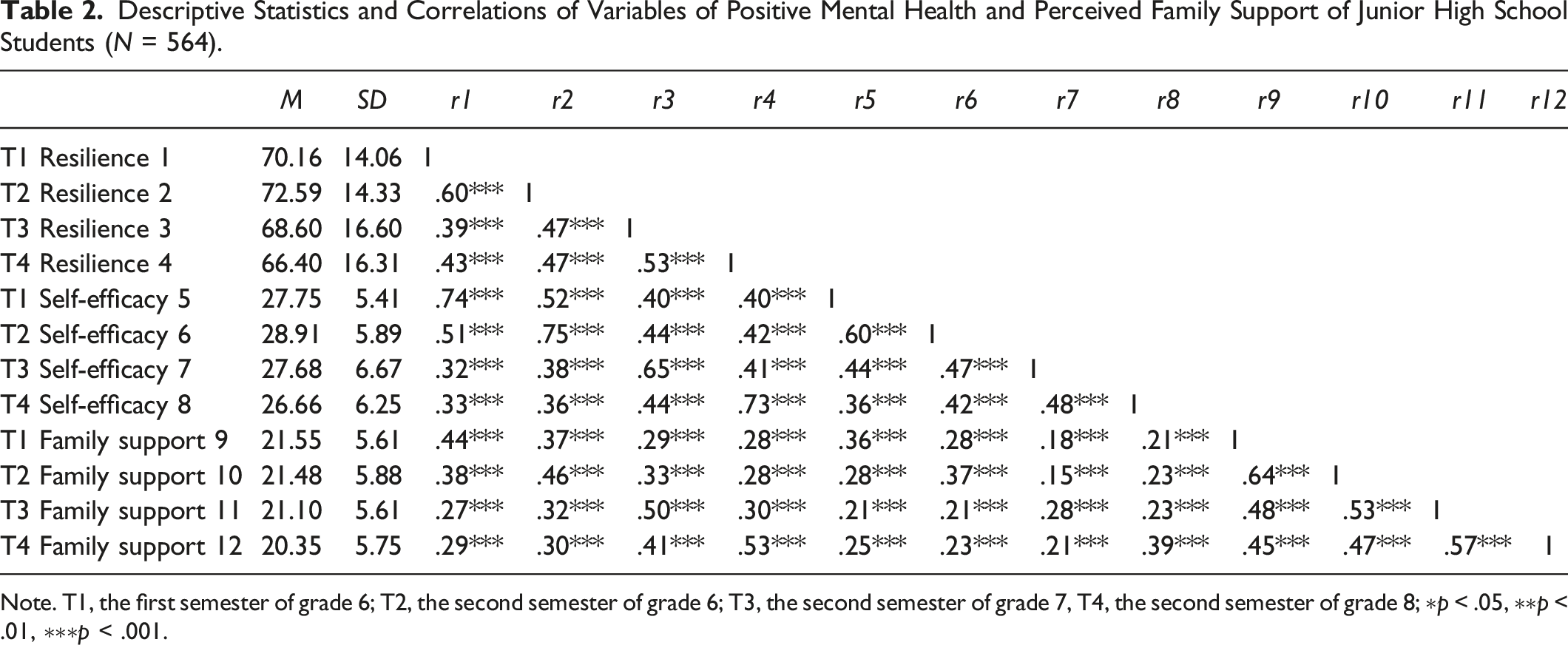
Note. T1, the first semester of grade 6; T2, the second semester of grade 6; T3, the second semester of grade 7, T4, the second semester of grade 8; ∗p < .05, ∗∗p < .01, ∗∗∗p < .001.
Changes in Positive mental health across Time
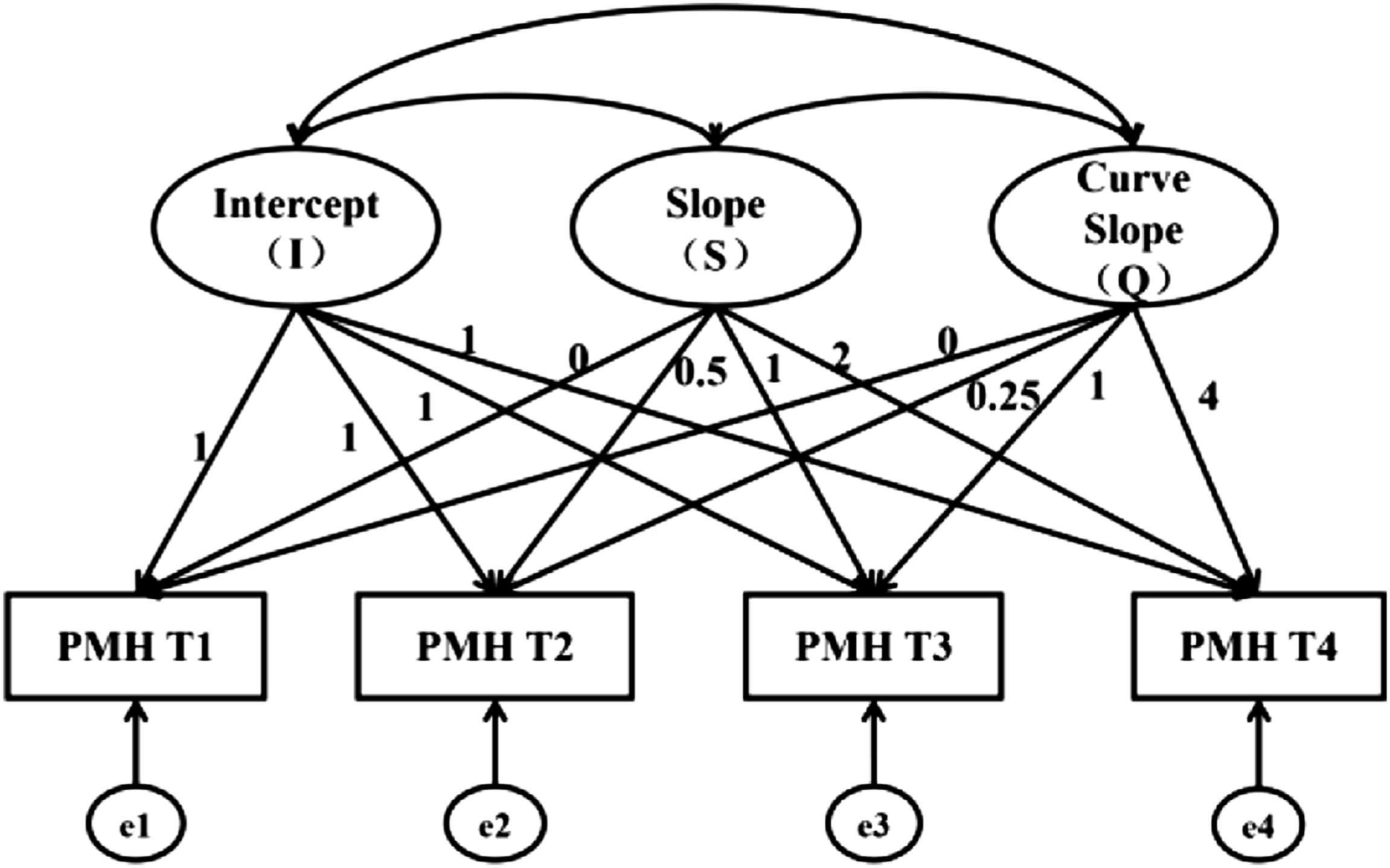
To test whether the developmental trend of the positive mental health indicators of junior high school students in the present study was linear or curvilinear, we constructed an unconditional latent growth linear model (Figure 1) and an unconditional latent growth curve model (Figure 2) for each dimension. The latent variables in the models were the intercept and slope. In the unconditional latent growth linear model, the factor loading from the measured value of resilience at each time point to the intercept were fixed at 1, and the factor loading to the slope were represented by 0, .5, 1, and 2, respectively. The unconditional latent growth curve model added a quadratic term to the unconditional latent growth linear model. The coefficients and fit indices of each model are shown in Table 3. Unconditional latent growth linear model. Unconditional latent growth curve model. Model Coefficients and Fitting Index. Note. M1, unconditional latent growth linear model; M2, unconditional latent growth curve model; * indicates significant at α = .05; ** indicates significant at α = .01; *** indicates significant at α = .001.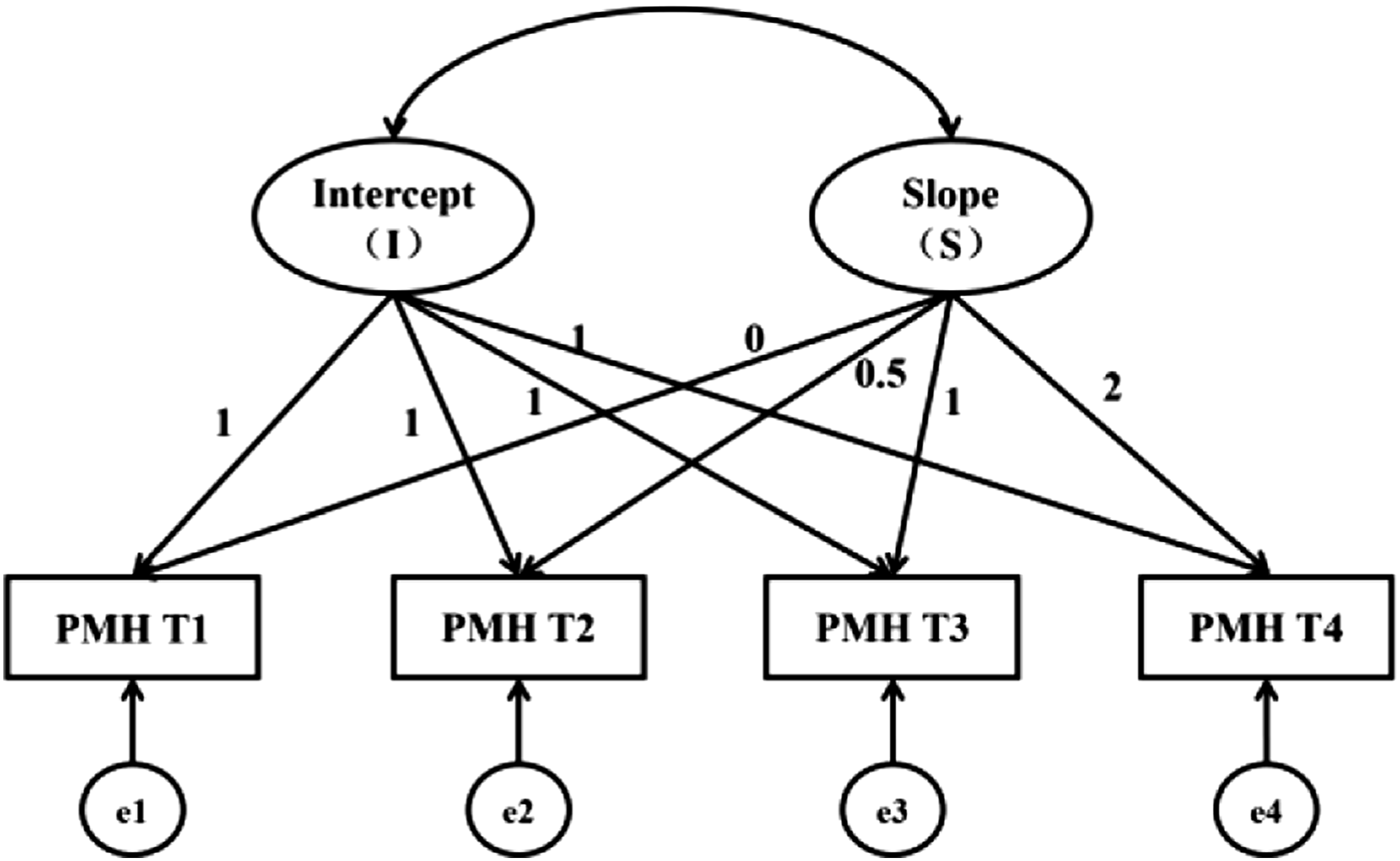
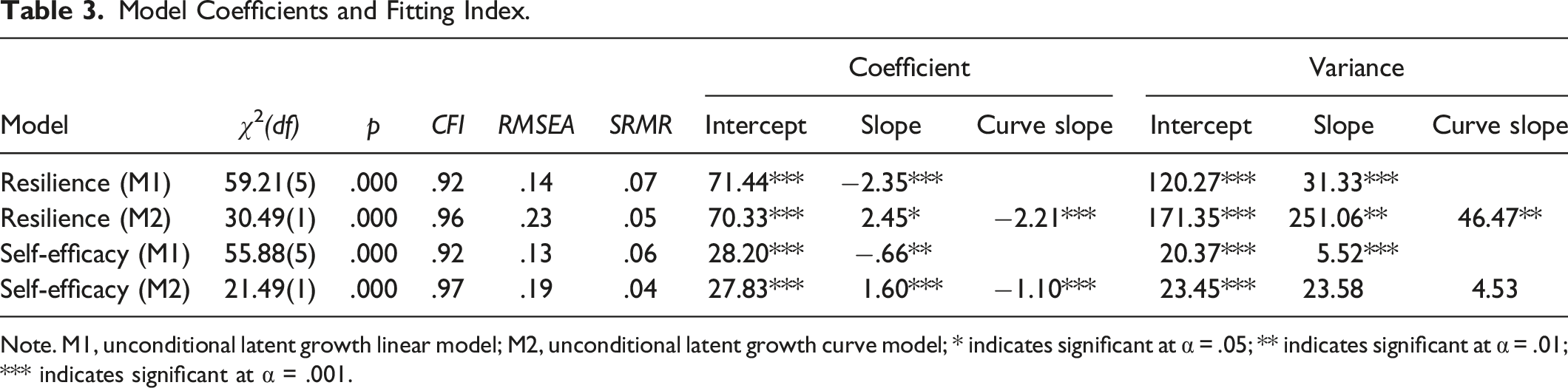
The resilience of junior high school students better fit the latent growth curve model, showing an upward trend of the curve (slope = 2.45, p = .029), and the growth rate decreased each year (curve slope = −2.21, p < .001). During the four waves, the variance of model intercept, slope and curve slope is significantly difference from 0, indicating that the initial level of resilience and the speed of change of junior high school students showed obvious individual differences. General self-efficacy fit better to the latent growth curve model, showing a rising trend of the curve (slope = 1.60, p < .001), and the growth rate decreased each year (curve slope = −1.10, p < .001). The variance of the model intercept is significantly difference from 0, indicating that the initial level of general self-efficacy of junior high school students showed obvious individual differences.
Cross-Lagged Panel Model and RI-CLPM of Perceived Family Support and Positive Mental Health
The cross-lagged panel model (CLPM) and the random intercept cross-lagged panel model (RI-CLPM) analysis were used to identify relationships between the perceived family support and positive mental health of the current study. CLPM has no constraints and focuses on how variables affect each other over a period of time. And RI-CLPM is a modified version of CLPM that disentangles the within-person process from stable between-person differences through the inclusion of a random intercept (Hamaker et al., 2015). This model controls for time-invariant trait-like individual differences, such that more insight is provided in how family support and positive mental health are linked at an intra-individual level. Referring to the existing research (Little et al., 2002), we parceled the items of positive mental health and used it as an indicator of latent variable. RI-CLPM fits well (χ2(9) = 4.448, p = .880, CFI = 1.000, TLI = 1.007, RMSEA = .000, SRMR = .012) and the CLPM does not fit very well according to some measures (χ2(12) = 133.838, p < .001, CFI = .933, TLI = .850, RMSEA = .134, SRMR = .080). The chi-square difference is 129.39, with 3 df, p < .001.
Comparing the standardized lagged parameter estimates from both models given in Figure 3, the RI-CLPM leads to the conclusion that the correlation between perceived family support and positive mental health in junior high school students is stable and does not change with time. The positive mental health at T3 (second semester of seventh grade) had a significant positive effect on subsequent perceived family support. But in other periods, there is no cross-time reciprocal influences between them. However, the CLPM results showed that perceived family support at T1 and T2 (sixth grade) can significantly predict subsequent positive mental health. In addition, positive mental health at T1 (first semester of sixth grade) and T3 (second semester of seventh grade) had a significant positive impact on subsequent perceived family support. Cross-lagged panel model and RI-CLPM of perceived family support and positive mental health. Note. FS, Family Support; PMH, Positive Mental Health. Standardized parameter estimates for data obtained with the RI-CLPM (above the arrows) and the CLPM (below the arrows). Standard errors are given between parentheses. * indicates significant at α = .05; ** indicates significant at α = .01; *** indicates significant at α = .001.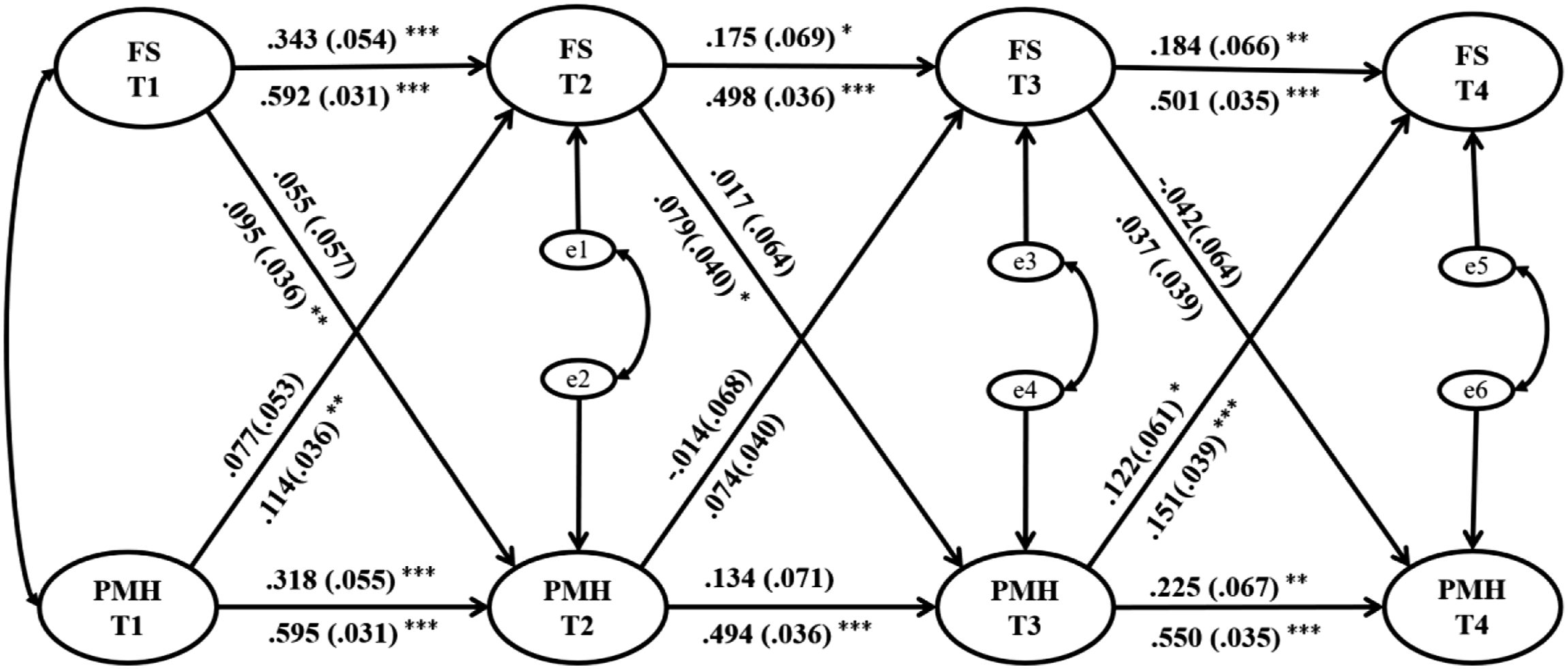
Discussion
The current study aimed to explore the development trend of positive mental health and the longitudinal relationship between adolescents’ perceived family support and positive mental health. First, we used LGM to examine the development trend of positive mental health indicators. As expected, we found that the positive mental health of junior high school students fluctuates. Resilience and general self-efficacy showed an upward trend; however, the development rate decreased each year, showing an inverted U-shaped curve trend. As the “imbalance” model shows, in adolescence, different times in brain development led to differences in the structural and functional maturity of brain systems critical for emotional processing. It also proposed that these changes in adolescence are non-linear unlike development during childhood and adulthood (Casey et al., 2010). Resilience and general self-efficacy showed low levels at the beginning of the school year, which may have been due to poor adaptation to a new environment at the beginning of school or simply entering a new life stage (Yao et al., 2013). However, there was a significant improvement in the second semester of sixth grade, which may have been due to students’ adaptation to the school environment (Leonard & Gudiño, 2021). This was consistent with Grevenstein and Bluemke (2015) and Okuyama et al. (2018), which reported that the mental state of freshmen showed an upward trend after enrollment. And this was consistent with previous studies, adolescent resilience and general self-efficacy also showed an upward trend (Sagone et al., 2020; Sheikh et al., 2016). Further, contrary to our hypothesis, resilience and general self-efficacy showed a continuous downward trend in the second semester of seventh grade and the second semester of eighth grade. This downward trend was in line with Bell’s (2013) research on resilience and Burger’s and Samuel (2017) research on general self-efficacy. The US findings have also found that mental health levels decline from early to late adolescence (Keyes, 2006). Erikson (1980) pointed out in his psychosocial development theory that the crisis of self-identity confusion is a necessary stage for adolescents. At this point, students have not yet reached a mature stage of psychological development. They must face not only physical and mental changes, but also various new pressures and challenges brought on by rapid development of the social economy and fierce competition. These pressures include school examinations, abnormal interpersonal relationships (e.g., loneliness, suspicion), and traumatic life events. Due to the limitations of their physical and mental development, adolescents at this stage may feel excessive stress and anxiety, which has a negative impact on students’ positive mental health (Petersen et al., 1991).
We constructed a cross-lagged panel model (CLPM) and a random intercept cross-lagged panel model (RI-CLPM) to verify the relationship between perceived family support and positive mental health. Under two different analytical approaches, we have obtained two different results.
The CLPM results showed that perceived family support of junior high school students in sixth grade could positively predict subsequent positive mental health, which supported the hypothesis (2). Family support is predictive of positive mental health. A supportive family environment in which adolescents feel close, connected and supported with their family is central to development of positive mental health (Bean et al., 2003). Therefore, parents provide more family support in the early stage to help students form a more positive mental state when they enter the next stage of junior high school (Kelly et al., 2012; Moore et al., 2018; Sheikh et al., 2016). However, perceived family support in the survey conducted during the second semester of the seventh grade could not significantly predict the positive mental health of the second semester of the eighth grade, which may be due to many possible reasons. For example, our study found that adolescents’ perceived family support declined over a 3-year period. When adolescents experience less and less family support in late junior high school, their positive mental health may be more influenced by other factors, such as from friends or schools support (Garthe, 2016; Bean et al., 2019). And students’ self-identity improves, their emotional support development begins to progress towards self-support (Larson & Brown, 2007), thus the influence of perceived family support on positive mental health decreases. We also found that perceived family support conducted in the second semester of seventh grade could predict the tenacity and self-efficacy in subsequent positive mental health, but not the strength and optimism. The factors that influence strength and optimism in the later stage of junior high school are in the process of transferring from the outside to the inside. And their development may be more dependent on the stable development of the individual self. Perceived family support may only serve as a protective resource (Kingon & O’Sullivan, 2001), and therefore could not predict the future development of positive mental health. Additionally, positive mental health of adolescents in the first semester of sixth grade (T1) and the second semester of seventh grade (T3) could significantly predict perceived family support in the next wave. Although positive mental health of adolescents in the second semester of sixth grade (T2) did not predict subsequent family support. However, we found that higher positive mental health in the first semester of sixth grade predicted higher levels of perceived family support subsequently, which also predicted higher positive mental health in seventh grade and higher perceived family support in eighth grade (T1 PMH → T2 FS → T3 PMH → T4 FS). This also supporting the hypothesis (2). The results of this study were consistent with previous research, in that individuals with high positive mental health are more likely to perceive support from others (Magalhães & Calheiros, 2017). Positive mental health of junior high school students is often associated with high emotional investment (Lyons et al., 2013). They can actively invest in their emotions and also feel the emotional support from others. At the same time, the research conducted by Antaramian et al. (2010) and Suldo et al. (2016) on mental health and family support also showed that adolescents with positive mental health are better able to use their family support system to cope with difficulties and problem-solve in negative situations, thus protecting their mental health. The ecological development theory (Bronfenbrenner, 1979) emphasizes the probabilistic influence of systemic factors on individual development, as well as the two-way interaction between developing individuals and the environment they live in overtime. During adolescent development, not only is positive mental health affected by the environment (family support), but the environment is also affected by an individual’s own positive mental health. When family support can help adolescents build more positive mental health, the family’s behaviors that provide support are strengthened; thus, subsequent perceived family support is enhanced. Therefore, the higher the level of an adolescent’s positive mental health, the more willing the parents are to invest more emotional and material support.
Consistent with CLPM, RI-CLPM showed that positive mental health in the second semester of seventh grade (T3) had a significant positive effect on subsequent perceived family support, and supporting the hypothesis (2). But in other periods, RI-CLPM showed different results, and there are no cross-time reciprocal influences between positive mental health and perceived family support. This may be due to changes in the nature of parent-adolescent relationships in early adolescence (Larson & Brown, 2007). By comparing RI-CLPM with CLPM, we focused on stable individual differences between subjects. RI-CLPM also showed that the correlation between perceived family support and positive mental health in junior high school students is stable and does not change with time. This is consistent with previous studies of Chinese (Guo et al., 2018) and South Korean adolescents (Cho & Haslam, 2010). The ecological development theory proposes that human development occurs in ecological systems, where the individuals interact with various environments. Some interacting proximal environments (family, school and community) may directly influence human development outcomes (Chen et al., 2019). Family support plays an important role in the positive mental health development of adolescents in every period (Kelly et al., 2012).
This study has some practical implications. First, the positive mental health in early adolescence is fluctuating. In particular, there is a curvilinear decline between ages 12 and 14. Therefore, attention and interventions targeting positive mental health changes in early adolescence are particularly effective. Furthermore, family support is closely related to positive mental health of junior high school students. Family support is essential for stable mental health at any stage, and positive and adequate family support in early adolescents contributes to the development of positive mental health (Cheung et al., 2017). It is important to encourage parents of adolescents to continue to provide support and guidance, to be responsive to their children’s changing needs and to be receptive to their children’s interests, concerns and feelings. In addition, the results of this study can serve as a suggestion for professionals who are developing prevention and intervention programs involving parenting support, education, or training.
Limitations and Future Studies
This was a longitudinal study on the development of junior high school students’ positive mental health, and clearly presented the development and changes of these students across 3 years. However, there were also some limitations that should be considered. First, we mainly used students’ self-reports for investigation. In future research, a variety of research methods, such as interviews and experiments, could be appropriately combined to obtain more accurate results. Second, our sample attrition rate is high, with 50.6% of the sample at T1 continued to provide data at T4, which is also a limitation of this study. In addition, we did not consider or measure some other covariates, such as the amount of time junior high students spent with their parents. This may lead to a lack of further discussion of the findings. In order to understand the impact of family support on adolescents’ positive mental health more accurately, future studies should include an investigation of covariates such as “How long/often these students really spend time with their parents?”. We could continue to track the same group of students used in this study, improve the understanding of the development of adolescent positive mental health, and explore the interaction between positive mental health and family variables (such as family economic status, family atmosphere, family activities, etc.), thus enrich the model of adolescent positive mental health.
Conclusion
In the present study, the positive mental health indicators of resilience and general self-efficacy of junior high school students showed a curve upward trend, which increased first and then decreased. The development rate decreased each year. Perceived family support is strongly associated with positive mental health of junior high school students. Family support is important for developing positive mental health in early adolescence. The purpose of understanding the development trend of positive mental health in early adolescence and the interaction between perceived family support and positive mental health is to help parents realize the importance of family support in the process of adolescent development. Early stable and sufficient family support can help adolescents to improve their positive mental health, to enhance the connection with their families and promote their development in many aspects.
Footnotes
Acknowledgments
The research was supported in part by grants from the Life Education and Career Development Action Research, Training & Practice Pilot Project funded by Tin Ka Ping Foundation and The Youth Foundation. We want to acknowledge Shanghai Guangming Junior Middle School, Shanghai Hongkou Experimental School, Junior Middle School Affiliated to No. 2 High School of East China Normal University, Shanghai Jinling Middle School, Shanghai Pengpu Junior Middle School, Shanghai Pengpu No. 3 Junior Middle School, Shanghai Changqing Middle School, and Pudong Foreign Language School Affiliated to Shanghai International Studies University for supporting us in collecting data. We also want to acknowledge Zhening Xu, Jialin Zhao, Caiyun Yang, Xixi Li, Qi Zhang, Dong Ma, Wen Li, Linni Zhang, Dandan Liang, Yue Fu, Ling Zha, Xiang Li, Jialv Zhao for hosting and participating the project, and Dr. Wei Wei for the assistance in data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the General Project of Education Science by Shanghai Philosophy and Social Sciences [grant numbers A2021002], and Shuguang Program supported by Shanghai Education Development Foundation and Shanghai Municipal Education Commission [grant numbers 20SG45].
Author Biographies
![]()