
Abstract
Antiretroviral therapy (ART) is one of the complexities of treatment and care for people living with HIV (PLHIV). It is essential to understand the challenges of admitting ART in PLHIV based on the Information Motivation Behavioral skills (IMB) model. This study was conducted using qualitative and directed content analysis on 15 participants. The participants included 10 patients and five health-care providers selected from the behavioral diseases counseling center affiliated with a medical university in southeast of Iran using purposive sampling method. Data were collected through semistructured interviews. Data analysis has led to three main categories—information, motivation, and behavioral skills—and eight subcategories. ART adherence in an Iranian context is like an iceberg that the IMB model can deeply identify underwater and unanticipated motivations and factors that lead to nonadherence. Therefore, it can be useful in designing and developing context-based nonadherence to ART interventions.
Introduction
The Joint United Nations Programme on HIV/AIDS (UNAIDS) has set the goal of ending the AIDS world epidemic by 2030. To end this epidemic, they have established a 90–90–90 goal to be achieved by 2020. 1 This goal includes 90% of people living with HIV (PLHIV) globally being diagnosed, on treatment, and virologically suppressed. To achieve this goal, antiretroviral therapy (ART) adherence should be higher than 95%. 2
The concept of ART adherence is one of the variables of health behavior. The goal of ART is to prevent the progress of the disease, improve the quality of life and prolong it, and the key to its success is the willingness PLHIV to ART adhere. 3 According to several studies, the ART adherence has been reported in Nigeria (25%), Canada (61%), 4 and Iran (35%). 5 Nonadherence to ART, in addition to reducing productivity in patients, can also increase the risk of multidrug resistant viruses. 2
Therefore, it is clear that knowledge and attitude of patients with regard to continuous use of drugs are at low levels. So, studies should be conducted on the barriers and adherence facilitators in this regard. Theory-based interventions were suggested to be more effective on health-related behaviors compared with nontheoretical approaches. 6 Qualitative methods can be used to study behaviors, attitudes, and experiences of people within their life context, where quantitative methods are not applicable. Some facilitators exist to ART adherence such as social support and self-efficacy. In the IMB model, facilitators that can encourage people to take medication includes information, motivation, and behavioral skills. The IMB is used in ART adherence, self-care behaviors in diabetics (nutrition and exercise), 7 predicted condom use, 8 and high-risk sexual behaviors among young people. 9 According to this model, information is a “prerequisite for performing health behavior and real knowledge about drugs.” 10 Motivation consists of two factors: personal motives, which include beliefs as well as beliefs and attitudes, and social motives, which include perceived social support for engagement in a particular behavior. 11 Perceived susceptibility or individual perception of risk is a prerequisite for the motivation to change risky behaviors. 12 Behavioral skills include the skills and self-efficacy needed to facilitate the change in particular behavioral health.
Few studies have applied theoretical frameworks to understand ART adherence. These studies have found that less medication information and social support from network members have been associated with worse ART adherence.13–15 For example, patients who received high social support from their providers had higher levels adherence. 13 Overall, the results of other studies have demonstrated support for the IMB model in designing interventions that improve and predict ART adherence among PLHIV.16,17 Therefore, the IMB model has proven to be effective in promoting ART adherence among other diseases and may be potentially successful among PLHIV. The IMB model posits that an individual who is well informed, motivated, and has the requisite behavioral skills will enact and maintain a health promotion behavior such as medication adherence. 18 Although ART adherence has been different based on cultural and social conditions, doing qualitative research in different societies can help clarify this issue. Therefore, this study seeks to further explain what determines the ART adherence based on the IMB model among PLHIV.
Methods
Study Design
A qualitative design was selected using semistructured interviews to collect data from the behavioral diseases’ counseling center. In such interviews, the investigator can interact freely with the participants. Therefore, it can be the best approach to generate new information on this topic. We aimed to capture feelings, ideas, perceptions, and attitudes of the participants.
Setting
This study was carried out in a behavioral disease counseling center affiliated with Kerman University of Medical Sciences in southeast Iran. People of different ethnicities live in Iran. They have different cultures, lifestyles, and socioeconomic status. 19 Kerman is the largest city in southeast of Iran, with a population of more than 800,000. People with different religious beliefs live in Kerman province including Shia Muslims, Zoroastrians, and Sheikhiyya sect and each have specific religious rituals. In general, Kerman culture has been based on two important factors including the specific climate and natural environment and history of hard battles. The number of people receiving free ART was 188 at the time of data collection. At this center, there were a nurse, pharmacist, psychologist, dentist, and blood sampling unit; two infectious disease specialists; two physicians; and admissions. The psychologist in particular has provided counseling to patients diagnosed as HIV-positive before and after ART initiation, while the physicians working in the clinic initiate ART based on patients’ clinical and laboratory findings. Nurses are also responsible for assessing patients’ progress, every month for the initial 6 months and every 3 months thereafter.
Sample and Sampling
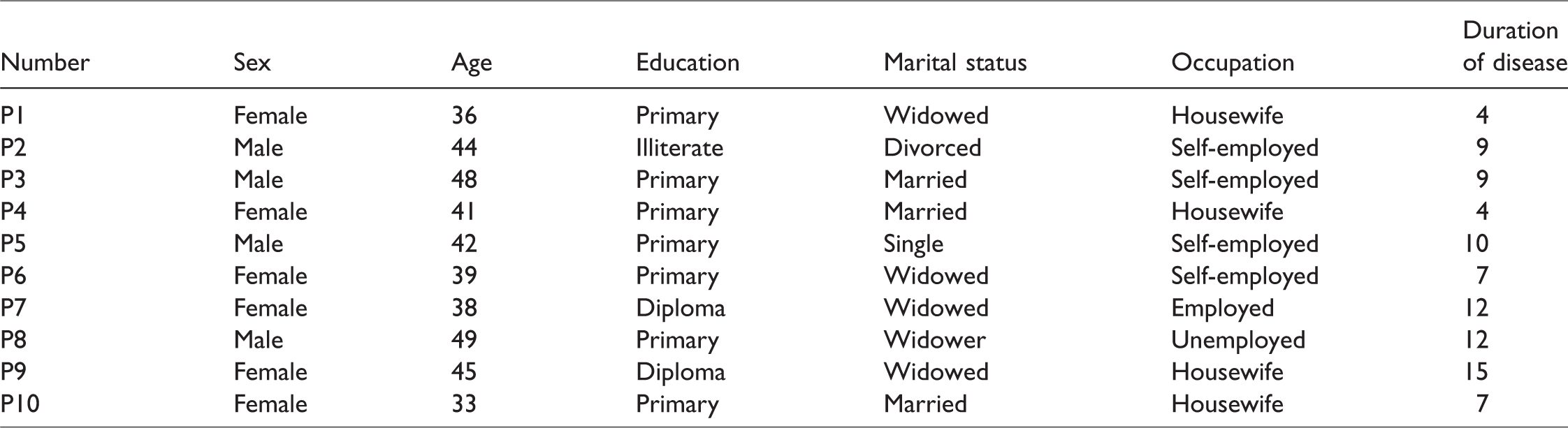
Purposive sampling was applied to select the participants. To collect the experiences about the research concept, patients and health-care providers were invited in the interviews. The saturation was achieved after 15 interviews with 10 PLHIV and five health-care providers including: one physician, two infectious disease specialists, one nurse, and one psychologist who had over 6-month experience (Tables 1 and 2). Inclusion criteria for participants were adult people 18 years or older with HIV-infection and CD4+ T cell count less than or equal to 350 cells/mm3 regardless of the clinical symptoms who received ART in the study clinic for at least 6 months.
Characteristics of PLHIV.
Characteristics of the Health-Care Providers.

Data Collection
In this study, data were collected from July to October 2017. Semistructured, in-depth, face-to-face individual interviews were recorded in Persian and translated into English by one of the researchers. Some of the guiding questions that elicit participants’ experiences about ART adherence are shown in Table 3. Interviews lasted 60 to 90 minutes.
Samples of Guide-Questions to Perform an Interview.
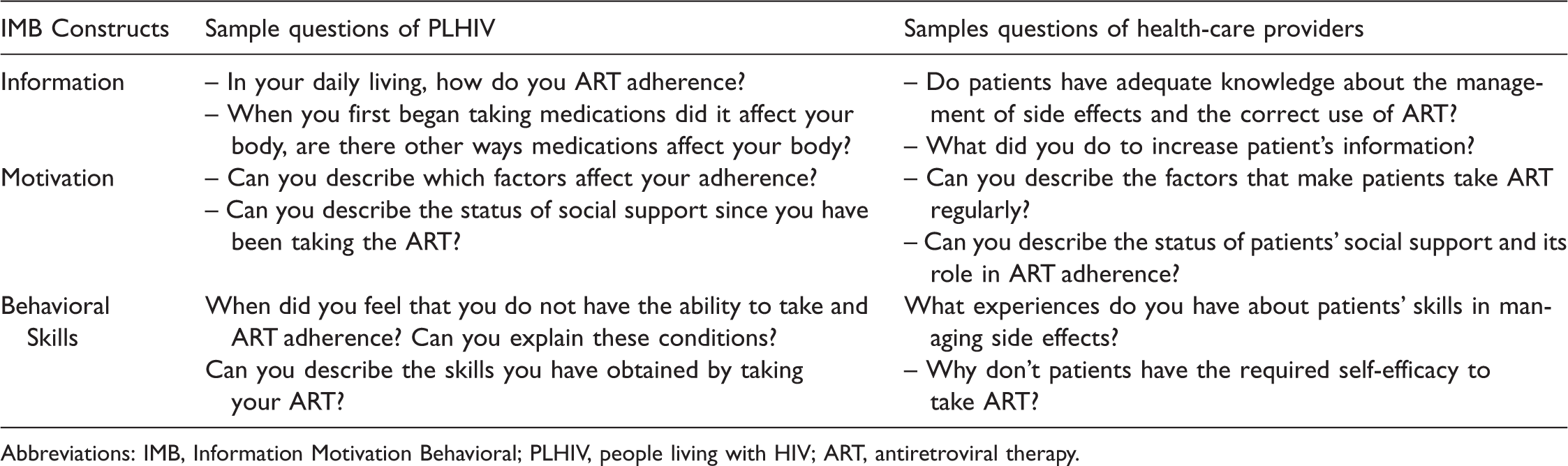
Abbreviations: IMB, Information Motivation Behavioral; PLHIV, people living with HIV; ART, antiretroviral therapy.
Data Analysis
A directed qualitative content analysis approach was used for data analysis. 20 Qualitative content analysis is used contextually to detect individual perceptions of everyday life phenomena and to interpret subjective data content. In this method, overt and covert concepts are revealed from the descriptions provided by participants. Then, these descriptions are coded, summarized, and classified, allowing codes using the meaning units derived from the descriptions. All interviews were recorded in Persian by a voice recorder. The transcribed texts were conformed to the recorded interviews in order to verify their validity. Qualitative studies require the researcher(s)’ full engagement in the data processing. Therefore, one of the researchers listened carefully to the recorded interviews and transcribed them. Later, the context of each hand-written text was reviewed several times by all researchers. The texts, which were typed in Microsoft Office Word, were transferred into a special qualitative data analyzing software called MAXQDA version 10. In the next stage, the meaning units were identified and codes were allocated to the meaning units. Then, codes were placed under the categories of the IMB model based on the similarities and differences. 21 The data collection process continued until data saturation was reached, and no new information was achieved after adding further data. All researchers discussed the contents of the categories. In the case of authors’ disagreement, discussions, and clarifications continued until achieving a consensus.
Trustworthiness
Trustworthiness is a criterion which constitutes rigor in qualitative researches. Four issues are normally used to describe various aspects of trustworthiness: credibility, confirmability, dependability, and transferability. 22 Several techniques were used to enhance trustworthiness of the following study. Peer checking has been done by the second researcher. Through frequent sessions between the second researcher and the supervisors, the study’s progress and process was reported and discussed. Member checking was completed with some of the participants for validation of interpreted findings. Some of the faculty members checked the encoding process and accessing categories. In addition, a clear and detailed description of culture, context, selection, and characteristics of participants; data collection; and process of analysis were provided.
Ethics Considerations
The Ethics Committee affiliated with Kerman University of Medical Sciences confirmed all processes and procedures used in the study (IR.KMU.REC.1396.2243). The purpose of the study was explained to all participants, and written informed consent was obtained before participation, participants were assured of the confidentiality of the data, and that they were free to withdraw from the study at any time. Interviews were conducted in private rooms.
Results
The results showed that the age of the PLHIV varied between 30 and 49 years. More than half of the participants were females. Among the PLHIV, four were living with HIV and six living with AIDS (Table 1).
In the next step, we show participants’ experiences in this study based on the IMB model under three main categories of information, motivation, and behavioral skills with eight subcategories (Table 4). These results are sequentially presented in the following sections using quotes of participants.
The Categories and Subcategories ART Adherence in PLHIV Based on IMB Model.

Abbreviation: ART, antiretroviral therapy.
Information
Information is one of the underlying principles of the ART adherence in PLHIV. The participants’ experiences with medicinal information have been discussed in three subcategories according to Table 4.
Taking Medication Regularly
Taking ART regularly, in addition to having a good effect on the disease, reduces the problem of recall of ART, but the PLHIV did not have enough information about the benefits of taking the drug at a specified time. A 41-year-old female HIV patient said: at right now, I take ART every day, I never forget, but I do not have a specific time to take the drug. Most days I take the drug 1 or 2 hours sooner or later than the specific time. I did not use to take drugs, but now I’m trying to take them whenever I remember. A 47-year-old physician indicated: We tell patients to take ART at the right time, but for this group of patients, because of the problems of forgetfulness, taking ART at any time during the night and day is better than not taking ART.
Drug Interactions
The lack of awareness about drug interactions and self-care did not allow patients to take care of themselves in emergency situations, so they unknowingly take a variety of ART and often do not achieve a proper response. A 44-year-old male HIV patient stated: When I was taking ART, I got worse, I did not know what to eat, so I used methadone, I even used medicinal plants. But, I didn’t get better, I got worse and was hospitalized.
Drug Side Effects and Management
Most PLHIV, due to poor knowledge of the side effects of drugs, had to consult with their friends and family to reduce the side effects and increase tolerance, they used to take ART arbitrarily, and, as a result, experienced the side effects. A female PLHIV with 45 years of age said: A patient called and told me she was not well, she could not tolerate the drug, she was spiritless. Drug side effects may be in the form of intolerance and allergies, or osteoporosis and nail deformity, especially in the addicted, the side effects are very difficult.
Motivation
Motivation is the stimulant of behavior, and it has the result and the goal, because no behavior is carried out without motivation. The motivational factors of the patients have been discussed in three subcategories of individual motivation, social motivation, and risk perception.
Individual Motivation
Individual motivation includes positive or negative attitudes toward behavior (ART adherence). The majority of participants believed in God as one of the sources of positive attitude. A 39-year-old male HIV patient said: Remembrance of God helped me keep my spirit, I have to take care of myself, because I believe that despair is a sin, so I am trying to get well, I thank God due to this achievement. The doctor assured me that my ART was free forever, now that I do not pay any money, I will take care of myself. I thought the doctors wanted to kill us soon with ART, so I was not taking my ART and if I had taken them, I would not have taken them regularly.
Social Motivation
Social motivation has been derived from perceived social support for engaging in a particular behavior. Social support resources include family members, friends, and neighbors. A daily recall from other important people and family members provides incentives for taking ART.
Some patients referred to their husbands as supporters and confidant individuals and considered them one of the most important encouragers. A 36-year-old female HIV patient stated: My husband made me take my ART because he wants to be sure that I am sexually safe and frequently encourages me to take ART. I remember when I went to the counselling center to get the ART, one of my relatives was working there. I did not go to the counseling center at all. The farther the behavioral diseases counseling center is from our home, the better it is.
Risk Perception
Risk perception is the likelihood of adverse consequences resulting from unhealthy behavior. One of the major outcomes acknowledged by almost all participants was that they considered themselves at risk of reduction of CD4+ T cell and progress of disease due to the poor adherence to ART. Many patients did not perceive the risk of poor adherence, which led to the nonadherence to ART. A female patient with 33 years of age indicated: At the beginning of my disease, I used to throw my ART into the trash bin because I hated taking ART. After a while, my mouth was full of thrush, I could not eat food, I was afraid so I started taking the medications, I have no problems right now. An infectious disease specialist with 55 years of age said: I tell my patients if they take ART one day and do not take them in another day, it's of no use because poor adherence leads to drug resistance, and viral suppression never occurs.
Behavioral Skills
Participants’ experiences in dealing with behavioral skills have been discussed in two subcategories of self-efficacy and ART-taking skill and side effects management.
Self-Efficacy
People with self-efficacy believe in their ability to organize and implement necessary measures in tempting situations. Some participants did not have the ability to resist against the tempting suggestions of friends. A 39-year-old psychologist stated that: Sick men are not able to take ART in any situation because of the use of drugs and alcohol, but women are more responsible. Women's responsibility has made the community accept them and they have higher self-efficacy.
ART-Taking Skill and Side Effects Management
Minimizing side effects of ART is one of the important strategies for taking ART correctly, and it is necessary to take ART at the right time. Many participants, especially men, did not have the skills to reduce the side effects of ART. A 49-year-old male HIV patient said: Whenever I go to work very early in the morning, I’ll take my ART at midnight so as not to forget it, I know I’ll forget about it if I do not take it. When I travel, I forget to take my ART, in case I took them with myself, I would forget to use them.
Discussion
Participants’ experiences showed that lack of information in various dimensions, lack of individual and social motivation, and lack of ART-taking skills were the main sources of nonadherence to ART in these patients.
According to participants’ experiences, patients’ knowledge of ART was low, and similar to the findings of another study, 16 information was emphasized as an essential element of interventions. It appears that drug information has clear and hidden layers similar to an iceberg; so, going deeply into the bottom of the iceberg is like the disclosure of hidden factors effecting the patients and their behaviors. Consequently, knowledge promotion leads to better adaptation in stressful situations. Another study 9 reported that lack of motivation and nonfavorable attitudes toward HIV-infected individuals was resulted from lack of knowledge; so, motivation is considered as a prerequisite for collecting information. However, the mere promotion of information does not change the healthy behavior and interventions are needed to provide information and promote motivation. 23 This difference seems to be due to the misconceptions made by some patients about ART. In other words, these misconceptions affect the individuals’ attitudes and adherence. In agreement with this study, a study showed that one of the factors affecting ART adherence was the patient’s motivation that was more effective than knowledge throughout the process of behavioral changes. 21 In other studies, the motivation was considered as an important mediator of the ART adherence.24,25
In this study, some PLHIV had a positive attitude towards the ART and indicated that long lifetime was the highest motivation for them. In confirming the abovementioned point, previous studies proved the positive effect of personal motivation on healthy behaviors.26,27 In addition, believing in God creates a positive force in patients for ART adherence. In this regard, participants of Park’s study 28 reported that having belief in God was a source of power that could control their health status. Contrary to our results, Rzeszutek et al. reported a negative relationship between religion and improved injuries in accidents.
According to our results, PLHIV had inadequate family, social, and financial support. Given the complexity of their emotional problems and stigma, HIV patients need family and community care along with complex treatment regimens. This need is more highlighted in a country like Iran, because nursing care at home has not been established in the health-care system of this country and the family is at the core of home care. Furthermore, the positive role of parents in supporting patients is very influential. The results of a study showed that spouse’s encouragement and support was very important in pursuit of HIV testing. 29 Moreover, Callaghan et al. showed that marital life and spouse support improved the quality of life in the elderly. 30 Matsumoto et al. also found that the expansion of using social networks by patients to communicate with their family members was recognized as an important potential for reducing depression. 31
In this study, patient’s friends were one of the valuable supporting sources. In agreement with these results, previous studies emphasized on communicating with friends more than the family, because in some cases, family members avoided discussing the health issues.32–34 In Iranian culture, according to the religious issues governing the society, it seems that no one is allowed to talk about HIV disease, which represents a culture of silence about HIV. In these cases, participants seek support from friends. Contrary to our study results, a study by Pitpitan et al. showed that presence of other people was the major barrier for accessing the treatment services, including HIV testing. 35 The patients were worried that friends and family members may prevent disease follow-up and ART adherence due to fear of stigma.
This study showed that PLHIV preferred a greater distance from the counseling treatment center to reduce stigma. Contrary to our results, researchers in a study reported that the proximity of the counseling treatment center to the home was considered as one of the additional health benefits, such as health monitoring with no additional cost. 29 According to the Iranian culture, stigma and anonymity seem to be important issues and patients preferred one counseling center in the city center for PLHIV rather than numerous counseling centers.
Based on the results of this study, risk perception was another important motivational factor in this model for appropriate behavior. For example, patients who were more sensitive to their longevity were more concerned about ART adherence and followed more risk-reducing behaviors. In one study, risk perception was recognized as an important motivational prerequisite for taking medication. 21
This study showed that women had more self-efficacy to take ART; so they were more active in pharmaceutical counseling classes. Considering that HIV was transmitted to women through their husbands, they were less ashamed and afraid. So, they had less self-blame and were more involved in the activities. However, a number of male participants did not believe in their ability to take ART regularly and were very weak in the counseling classes. In Kalichman et al.’s study, men were also more anxious and afraid of HIV, which prevented them from attending in social places and receiving ART. 36
In this study, despite the continuous follow-ups by the staffs of the counseling center regarding the ART and its punctual intake, participants did not consume ART on time; they took them 2 hours sooner or later. The findings of Rongkavilit et al. were similar to the results of the current research; they found that participants did not take ART punctually. 17 Due to the high amount of ART, the problem of forgetfulness, and the long-term use of ART, patients preferred not to take ART at a certain time.
The results of the this study showed that male participants did not have the required skills to manage and minimize the side effects of ART, which was due to their low awareness and self-efficacy. However, the female PLHIV had better status. In this regard, two studies showed that self-efficacy was the strongest predictor of drug acceptance and therefore overall risk reduction.37,38 Self-efficacy overshadows the individuals’ effort and performance. Solhi et al. showed that self-efficacy scores’ changes had the greatest effect on the performance score. They also found a direct relationship between self-efficacy and performance. 39 Two other studies indicated that participants with good behavioral skills had a high ART adherence.14,16 In the study by Guna et al., behavioral skills had the strongest direct impact on healthy behaviors. 40 The consistency among these studies indicates the importance of empowerment, as a strategy for health promotion. With regard to empowerment, the patient can be empowered by creating long-term programs and developing skills.
As with most studies, our study had some limitations. Therefore, quantitative and qualitative studies are recommended in different cultural contexts and among other health-care providers and PLHIV, such as children.
Conclusion
In an Iranian context, ART adherence is similar to an iceberg; the IMB model can deeply identify the underwater condition, unanticipated motivations, and factors that lead to nonadherence. The experience of participants confirmed that lack of information in various dimensions, lack of motivation and social motivation, as well as lack of skills were the main sources of nonadherence to ART in PLHIV. Therefore, the IMB model can be useful in designing and developing context-based nonadherence to ART interventions. Ultimately, the results of such comprehensive research can pave the way to institutionalize a complete and constructive medication adherence culture, which leads to a safe and high-quality care in a unique cultural context.
Footnotes
Authors’ note
Ehsan Movahed is now affiliated with School of Public Health, Jiroft University of Medical Sciences, Jiroft, Iran.
Acknowledgments
The authors would like to thank all the people who helped us to perform this study especially people living with HIV in Kerman.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.