
Abstract
Background
The health information is an important factor for improving people's health behaviors. On the other hand, media literacy plays an important role in the search and selection of valid information and resources about health. Therefore, the present study aimed to investigate the correlation between health literacy and media literacy.
Method
This study was a cross-sectional study. Random cluster sampling was used to select 700 citizens in Kerman, Iran. Health literacy for Iranian adults’ questionnaire and media literacy questionnaire were used to collect the data.
Results
Health literacy of 53.2% of the citizens was insufficient. Media literacy of 38.6% of the citizens was moderate and it was high in 61.3%. A significant positive correlation was found between health literacy and media literacy.
Conclusion
The media literacy was an important determinant factor for health literacy. The development and increase of media literacy can also increase health literacy.
In the 21st century, everybody must have a wide range of abilities and competencies for a favorable function and in principle, they must have literacies, ranging from a simple reading to understanding information provided by health care providers.1,2 Health literacy is one of the most important social determinants of health.3,4 Health literacy is the ability to obtain, read, understand, and use healthcare information in order to make appropriate health decisions and follow instructions for treatment. . Health literacy includes a set of reading, hearing, analysis and decision skills and the ability to apply these skills in health situations that do not necessarily refer to academic years or general reading ability. 5 The U.S defines health literacy as the relationship between patients’ literacy and ability to adhere prescribed drug regimens. 6 A research was conducted in six Asian countries (Malaysia, Taiwan, Vietnam, Indonesia, Kazakhstan, and Myanmar). The mean score of health literacy in Malaysia, Taiwan, Vietnam, Indonesia, Kazakhstan, and Myanmar was 31.83 (ranging from 29.6 to 34.4)(the possible score was 0–50). 3 one study was conducted in five provinces of Iran; only 28.1% of the participants had adequate health literacy, 56.6% had inadequate literacy, and 15.3% had limited health literacy. 5 Ghanbari showed that limited health literacy is a common problem in pregnant women referred to a healthcare center, and since limited health literacy can prevent proper understanding of health messages and recommendations, healthcare providers must use effective ways to promote health literacy. 1 Therefore, according to various studies conducted in Iran, health literacy of the Iranian people is undesirable and inadequate.2,5–8
Research results have shown that health literacy helps individuals engage more in treatment decision-making and cooperate better with healthcare centers.2,8 Furthermore, people with poor health literacy may not understand the written and audio information provided by the healthcare providers. 5 On the other hand, the inappropriate use of medications and the lack of implementation of medical instructions are among the disadvantages of poor health literacy.1,9
Various factors can affect the level of health literacy one of which seems to be media literacy. Different organizations recommend media literacy as one of the effective strategies for promoting health. 10 Media can play a vital role in people's health because they spend a long time watching media. 10 People use the media information to change their health literacy and improve their health behaviors. 11 Therefore, one of the purposes of using media is health information.11,12 A person with media literacy has the skills of analysis, evaluation, grouping, induction, deduction, composition, and summarization. 13 Therefore, media literacy means research, analysis, education, and awareness of media influences, including radio, television, film and cinema, music, journals, internet on individuals and communities. 13 Health promotion, lifestyle, and health-promoting norms are among the positive effects of media literacy. In other words, media literacy (information literacy) increases health literacy.8,14 Individuals with media literacy are less vulnerable to fake information because they can detect messages, master the content, and have more control over their learning.13,15 Thus, the close relationship between the media and human health seems to be undeniable. 10 Mahmoudi showed a positive and significant correlation between health literacy and information literacy in postgraduate students, meaning that the higher the information literacy, the higher the level of health literacy, and vice versa. 8
According to the literature review, a few studies have evaluated the correlation between health and media literacies. Since we are at the beginning of the 21st century, the individuals are encountering new communication tools and a large number of messages; all viewers have different interpretations depending on the level of literacy, education, and job. Many people search the word “health” on the internet every day, and much information is being retrieved, but is all info correct? Can we trust all of them? The health information provided in the media can have a significant impact on people's health behaviors. Therefore, this study aimed to investigate the health literacy and media literacy levels in citizens of Kerman, Iran. The study also aimed to investigate the correlation between health literacy and media literacy and if the media literacy was a determinant factor for health literacy.
Methods and Materials
Study Design and Setting
This descriptive-correlational cross-sectional study was conducted in 2018, in Kerman, in southeast of Iran with a population of more than 722,000.
Sampling and Sample Size
Random cluster sampling was used. Four districts of Kerman (based on local division) were considered as clusters. Research settings in each district were shopping centers, commercial centers, parks, recreational areas were considered, and according to the sample size, each cluster was equally sampled. According to the previous studies (r = 0.437) 8 and with the confidence coefficient of 95% and the type II error of 10%, the sample size was 323 individuals. Regarding the cluster sampling method, the sample size required for the present study became twice (646), so 700 people were considered due to dropout probability.
Instrument
The instruments used in this study include three parts: demographic characteristics form, the questionnaires of health literacy of Iranian adults and media literacy. The first part of the survey was related to the demographic data including: age, gender, marital status, education, occupation, income, living place, source of information and news, the amount of watching the health channel, the acquisition of health-related materials, the amount of internet usage, being employed and have a family member working in the healthcare system.
The questionnaire of health literacy of Iranian adults was designed and validated by Montazeri et al. The qualitative content validity, construct validity, and the reliability have been evaluated. The results of the exploratory factor analysis showed that the 33-item questionnaire consists of five subscales, including reading (4 items), access (6 items), comprehension (7 items), evaluation (4 items), and decision-making and behavior (12 items). The Cronbach's alpha level of items in the related constructs was acceptable (0.72–0.89). The items were answered based on a five-point scale from strongly agree to strongly disagree. The total score varies from 33 to 165. The total score and the score of each dimension were then standardized from 0 to 100. The score between 0–50 means low health literacy, 50.1–66 is inadequate, the score of 66.1–84 shows sufficient health literacy, and the score of 84.1–100 shows excellent health literacy. This questionnaire has been used by other authors, including Mahmudi 7 and Montazeri et al. 16
The media literacy questionnaire developed by Falsafi et al. consists of 20 items with five subscales of ‘Understanding the contents of media message', ‘Knowing the hidden objectives of a media message', ‘Deliberate choices of media messages', ‘critical view on media messages', and ‘analysis of media messages'. Its validity and reliability have been confirmed (Cronbach's alpha coefficient is between 0.75 and 0.8). 17 The items were answered based on a five-point-Likert scale from strongly agree to strongly disagree. The total score varies from 20 to 100. The score between 20–33 means poor health literacy, the score of 33.1–66 shows moderate health literacy, and the score of 66.1–100 indicates high health literacy. 17
Data Collection and Analysis
The researchers referred to research settings in the morning, afternoon, and night after obtaining the code of ethics and presented a written letter to each of them. The participants completed the self-administering questionnaires. The inclusion criteria were participants aged ≥18 years old with writing and reading skills, and access to at least one kind of media. Data collection lasted three months (from January to March 2018).
Data were analyzed using SPSS version 25. Frequency, percentage, mean and standard deviation were used to describe the studied variables. Since the health and media literacy scores had normal distributions, the Pearson correlation coefficient was used to determine the correlation between media literacy and health literacy. Uni- and multivariate linear regression tests were used to determine the predictors of health literacy score. P-value of < 0.05 was considered significant.
Ethical Consideration
The Kerman University of Medical Sciences approved this project (IR.KMU.REC. 1396,1793). After approval, the researchers provided some oral information, including the goals and objectives of the study, the confidentialityand anonymity of the data, and the participants’ withdrawal from the study at any time. Then written consent was taken individually.
Results
Socio-Demographic Characteristics
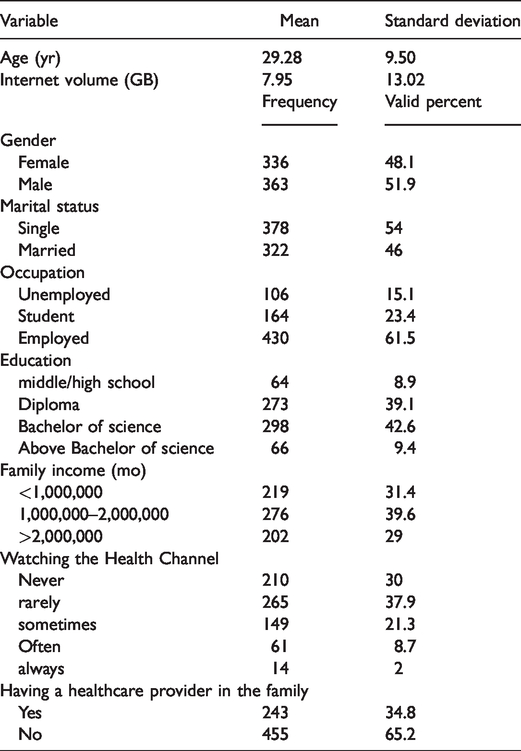
In total, 700 participants were assessed. The mean age of participants was 29.28 ± 9.5. The mean internet volume per month was 7.95 ± 13.02 gigabytes (GB). 51.9% of them were male, and 54% were single. 61.5% were employed (Table 1). The source of health information in most cases was the internet (66.3%) and the healthcare providers (41.2%) (It should be noted that citizens could choose more than one item). Moreover, the source of information and news in most cases was internet (79.7%) and television (61.1%) (It should be noted that citizens could choose more than one item).
Socio-Demographic Characteristics of Participants (n = 700).
Health Literacy and Media Literacy
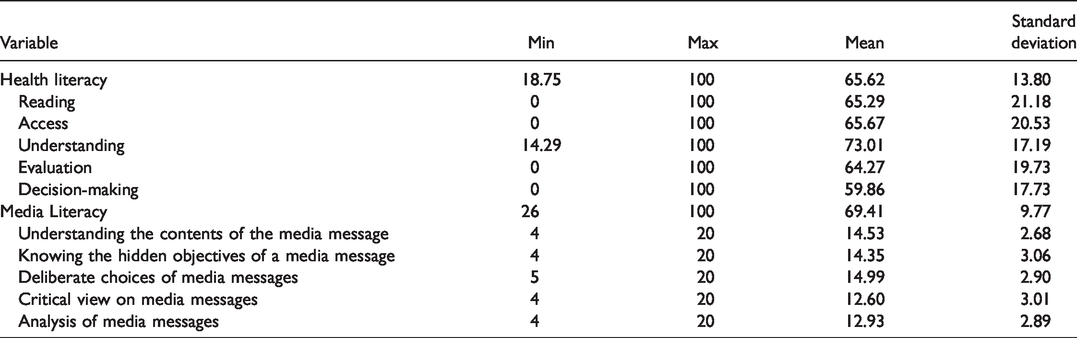
The mean total score of health literacy was 65.62 ± 13.80. 11.9% (n = 83) of the citizens had low health literacy, 41.3% (n = 289) had inadequate health literacy, 36.9% (n = 258) had sufficient health literacy, and 10% (n = 70) had excellent health literacy. Mean score of media literacy was 9.77 ± 69.41. 38.6% (n = 270) had moderate media literacy and 61.3% (n = 429) had high media literacy (Table 2). The results of Pearson correlation coefficient showed a significant statistical correlation between the mean scores of health literacy and media literacy and their dimensions. In addition, a significant statistical correlation was found between the media literacy dimensions and most components of the health literacy (Table 3).
Health Literacy and Media Literacy and Their Dimensions’ Scores.
The Correlation Between Health Literacy, Media Literacy, and Their Dimensions.
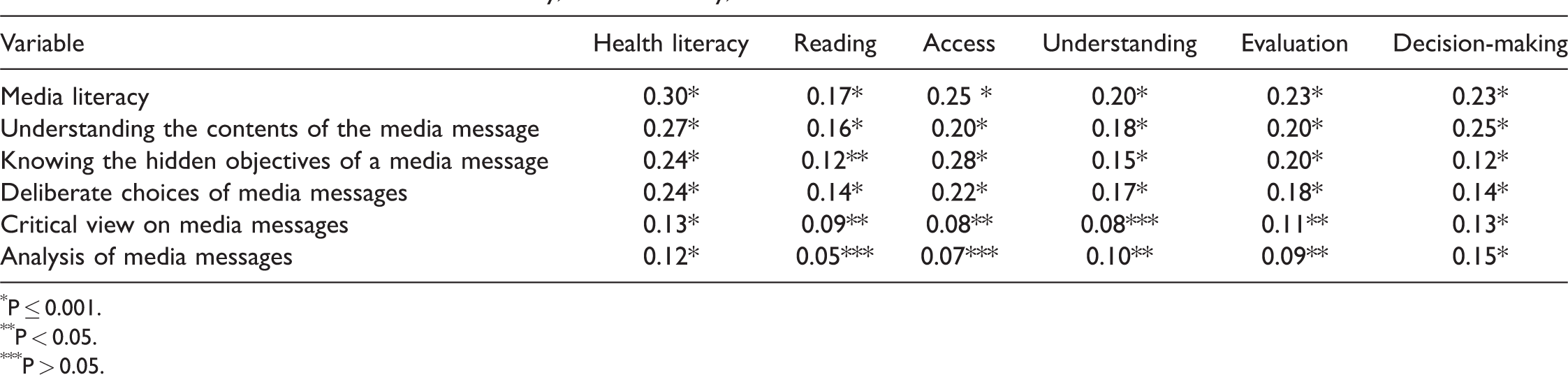
∗P ≤ 0.001.
∗∗P < 0.05.
∗∗∗P > 0.05.
Determinant Factors for Health Literacy
The results of univariate linear regression indicated a significant association between the score of media literacy, sex, education, occupation, income, watching the Health channel, and having a healthcare provider in the family, and the score of health literacy (Table 4). The results of multivariate linear regression indicated that among variables, the media literacy, sex, education, occupation, income, watching the Health channel, and having a healthcare provider in the family predicted the score of health literacy. Therefore, a high level of media literacy, female sex, academic education, unemployed/students, watching the Health channel, having a healthcare provider in the family associated with a high level of health literacy (Table 4).
Determinant Factors for Health Literacy.
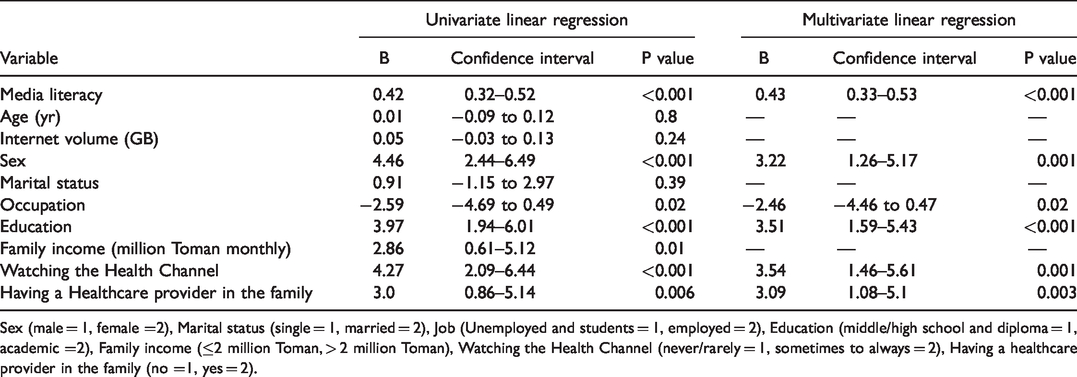
Sex (male = 1, female =2), Marital status (single = 1, married = 2), Job (Unemployed and students = 1, employed = 2), Education (middle/high school and diploma = 1, academic =2), Family income (≤2 million Toman, > 2 million Toman), Watching the Health Channel (never/rarely = 1, sometimes to always = 2), Having a healthcare provider in the family (no =1, yes = 2).
Discussion
The results showed a positive correlation between media literacy and health literacy; the higher the health literacy, the higher the media literacy.
The results of Akbarinejad et al., Mahmoudi et al. and Yvonnes Chen conducted in Iran, and the US showed a direct positive correlation between health literacy and media literacy.8,14,18 It is noteworthy that the research populations and the instruments used to measure the two concepts of health literacy and media literacy were different between the three studies and the present study.
The results also indicate that the mean score of citizens' health literacy was higher than the average. However, 53.2% of the participants had inadequate health literacy. The mean health literacy in the Nekoei study conducted in Iran was lower than the average of the present study, which can be due to the measurement tool, and the time and date of the research, which was carried out six years ago. It is evident that citizens' health literacy has increased over time. 19 The mean health literacy in current research is approximately the same as some other studies in Iran. The mean scores of health literacy in the studies conducted by Ghanbari, Hosieni, Zareban, and Akbarinejad et al. in Iran during 2012 to 2017 were higher than the average.1,14,20,21 In some surveys by Duong (in Malaysia, Kazakhstan, Myanmar, Vietnam, Taiwan, and Indonesia), and Kendir and lindahl's from 2016 to 2020 (although the statistical population of the study was students and patients with cardiovascular disease), the mean score of health literacy was slightly higher than the average.3,22,23 However, it should be noted that the studied communities are culturally different from one another, and the questionnaire used in these countries is different from the instrument used in the present study.
The results of studies conducted by Tehrani Banihashemi, Shoou-Yih and Heinrich in Iran, Taiwan and the US during 2007–2012 showed people with poor health literacy.5,24,25 The reason for this difference is that communities have paid more attention to health literacy over time. Although the mentioned studies were conducted in different cities with somehow different cultural context, their results confirmed our results. The policies, media educational contents, and strategies for increasing citizen health literacy are similar in different Iranian cities and are assessed with the central governmental organization. In addition, there is a T.V channel specific to health issues which is accessible for all urban and rural citizens in Iran.
In the present study, the mean score of media literacy was moderate and 61.3% of the participants had high media literacy. The results of the studies conducted by Mahmoudi and Sohrabi in Iran were consistent with that of the present study.8,13 Moreover, in a survey by McLean in Australia, the results showed that the media literacy of the studied community was more than average. 26 In studies conducted by Falsfi and Akbarinejad in Iran, despite the same measuring instrument, the results indicated that the mean media literacy score was less than that in current study due to different populations (teens aged 15–18 years old and women).14,17 On the other hand, studies by Piscina et al. and Culver Sherri et al. showed an unfavorable level of media literacy which is not consistent with the present study.27,28 It should be noted that the timing of the study is different, and the use of media has increased among individuals over time, and as a result, their media literacy has increased.
The results of this study showed that health literacy of women is more than that of men because women observe more health issues, and they are more interested in periodic checkups and refer to healthcare centers more. The results of Afshari et al. and Mahmoudi in Iran and the results of Duong in Malaysia, Kazakhstan, Myanmar, Vietnam, Taiwan, and Indonesia respectively, showed that the health literacy of women was more than that of men.3,8,29 In the current study, those with university education had higher levels of health literacy than other people. The results of Duong in Malaysia, Kazakhstan, Myanmar, Vietnam, Taiwan, and Indonesia, and the results of Akbarinejad et al. in Iran showed higher health literacy in people with higher education.3,29 Furthermore, people who occasionally or often watch the Health channel have higher health literacy than other people. The media is like a double-edged blade that can either increase awareness and knowledge by providing accurate information or mislead people with incorrect information and news. The media play a significant role in shaping the culture and personality of every individual. 30 People whose one of their family members was in the healthcare system had more health literacy than other people. It is clear that people working in the healthcare system have more health information than other people and living with such people can gradually increase the health literacy of other family members.
In the present study, most people received health information through the Internet and then by asking questions from the healthcare providers, and they less used resources such as radio, television, newspapers and magazines, satellite networks, family, and friends. In this regard, the results of Mahmoudi et al. showed that students got most of their information through internet and interaction with friends. 8 According to the Official Portal of Measuring Information Society of Iran, 53.23 percent of Iranians used the internet in 2015. Given the prevalence of virtual networks and the internet in the community, people are expected to receive most of their information through these ways.
One of the limitations of this study was not assessing other individuals' skills and cultural backgrounds of the participants. These factors may interact with health literacy and media literacy. However, we tried to select a homogenous population with similar cultural backgrounds.
In conclusion, our results revealed that more than half of our participants had insufficient health literacy but nearly three fifths of them had high media literacy. In addition, the media literacy was an important determinant factor for health literacy. Therefore, the development and increase of media literacy can increase health literacy. Health literacy is already seen as a crucial tool for the prevention of non-communicable diseases. Therefore, community health policies can be used to increase health literacy and media literacy of citizens because people with adequate health literacy may behave better in health crises and epidemics. In addition, people with health literacy are more likely to be at the frontline of disease prevention and reduce treatment costs. Nurses and doctors, the main foundations of the health care, have a special role in promoting the health literacy of citizens. They can increase citizens' health literacy through virtual educational programs. In order for the citizens to be aware of the most up-to-date health and medical principles and improve their health literacy, further study is suggested to assess the correlation between other important factors such as individual skills, media programs, and health literacy.
Footnotes
Acknowledgments
The authors of this article appreciate the cooperation of the citizens living in the city of Kerman who helped the researchers in collecting data.
Author Contributions
P. P. A., F. K., M. S., R. F. M., E. K., and F. N. wrote the proposal, gathered the data, and wrote the main manuscript text. M. D. supervised the study protocol designation, data collection, data analysis, and writing the manuscript. All authors reviewed the manuscript.
Compliance With Ethical Standard
The Kerman University of Medical Sciences approved this project (IR.KMU.REC. 1396,1793). After approval, the researchers provided some oral information, including the goals and objectives of the study, the confidentiality, and anonymity of the data, and the participants’ withdrawal from the study at any time. Then written consent was taken individually.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.