
Abstract
Background
Gestational diabetes mellitus (GDM) is one of the most common metabolic dysfunction in pregnancy and as overweight and obesity are of the major risk factors. The aim of this study was to determine the effect of Information-Motivation and Behavioral skills (IMB) model-based counseling on preventing GDM in overweight and obese pregnant women.
Methods
This randomized controlled trial study was conducted on 137 pregnant women in two groups; education and counseling IMB model-based for four sessions (n = 70), and antenatal usual care (AUC) (n = 67). This study was conducted on overweight and obese pregnant women, at the 12 to 16 weeks' gestation and recruited from the Prenatal Clinic of Rohani Hospital in north of Iran. Blood glucose was measured before and 8 weeks after the intervention. Descriptive and inferential statistics including mean, frequency, t-test, chi-square and ANCOVA were used.
Results
The prevalence of GDM was lower in the intervention group than the control group (10% and 29.9%, respectively, RR = 0.33, CI 95% (0.15– 0.74) p = .004) as well as mean fasting blood glucose (Cohen's d = 0.28, p = .07), and glucose tolerance test at the first and second hour (d = 0.41 and Cohen's d = 0.73, respectively, p < .01).
Conclusions
A lifestyle intervention in early pregnancy by IMB counseling in overweight and obese pregnant women can be effective in decrease GDM.
Keywords
Background
Gestational diabetes is the most common metabolic disorder in pregnant women, which is associated with serious complications for both mother and baby. This phenomenon is first diagnosed in late pregnancy. 1 The number of diabetics will be doubled by 2030, which will also affect pregnant women. 2 The prevalence of gestational diabetes worldwide is estimated at 1–14%. 3 In a meta-analysis study in Iran, the highest and the lowest prevalence rates of GDM was 18.6% and 1.3%, respectively. 4 Some of the most important complications of gestational diabetes include increased risk of preeclampsia and eclampsia, macrosomia, polyhydramnios, preterm delivery, abortion and cesarean section. As a matter of fact, women with gestational diabetes also have an increased risk of permanent diabetes in the future.5–8
The risk of GDM is higher among obese women, and the dramatic increase in prevalence of obesity around the world over the recent years reflects a worrying increase in the prevalence of GDM. Individual medical and treatment costs can be significant in the future because obesity and GDM not only increase the risk of adverse pregnancy and the consequences for the baby, but also increase the risk of developing type 2 diabetes late in life in both mother and baby.9–12 In general, weight control can significantly help regulate maternal blood glucose levels, which in turn, helps prevent the complications of gestational diabetes. 13 To achieve this goal, self-care has an important role in regulating blood glucose level, which can improve fetal and maternal health. Self-care practices that can potentially prevent gestational diabetes include diet, physical activity, and weight control. 2
As a result, various methods have been studied to prevent gestational diabetes with the participation of the mother herself.14–16 Obviously, one of the most important preventive strategies is to control overweight and obesity, which are closely connected to diabetes. 17 Diet change, physical activity and exercise, 18 mental and social health, 19 lifestyle change, 20 and weight loss in a year before pregnancy 21 are among factors that are effective in preventing diabetes. Weight loss is one of the most important factors in preventing gestational diabetes. 22 On the other hand, strengthening motivation, which encourages people to stick to their weight loss plans, is highly effective on weight loss. 23
Information-Motivation-Behavioral skill (IMB) model is a comprehensive model for promoting health behaviors, especially in chronic diseases. 24 This model has proved successful in explaining health behaviors over the past ten years. 16 Numerous studies have demonstrated the positive effect of IMB model-based interventions on improving self-care practices and related health outcomes in patients with diabetes through weight loss and HbA1c reduction.24,25
Considering the background of effective studies on IMB model, the importance of gestational diabetes and its impact on maternal and fetal health, and the increased prevalence of overweight and obesity, some approaches are needed to reduce the likelihood of obesity in order to reduce the prevalence of gestational diabetes. Since the IMB model is an easy, inexpensive, accessible and sustainable method, the aim of the present study was to evaluate the effectiveness of early intensive lifestyle intervention applied through the IMB model in preventing the incidence of gestational diabetes in overweight and obese pregnant women. The hypothesis was that the number of overweight and obese women diagnosed with GDM were fewer in the intervention group compared to the antenatal usual care group.
Materials and Methods
Study Design
This parallel-group randomized controlled trial was registered in the Iranian Clinical Trial registry under number IRCT 20120125008822N3 and the ethical approval was obtained from the Iranian Research Ethics Committee (IR.MUBABOL.HRI.REC.1397.068) on 09/06/2018. Moreover, a written informed consent was received from all participants. The study population was consisted of all pregnant women who visited the prenatal clinics of Rouhani Educational Hospital in Babol, affiliated with Babol University of Medical Sciences, in their first trimester between July and December 2018. The study was conducted and reported using the CONSORT recommendations. 26
Sample Size Estimation
The Results of the study by Quinlivan et al. were used to determine the sample size based on the prevalence of gestational diabetes in the intervention and the usual care groups. 27 In this study, the overweight women (BMI > 25) received educational intervention about diet, increased physical activity, and stress management. The incidence of gestational diabetes mellitus in the 24–28 weeks of gestation was 29% in the control group and 6% in the intervention group. Using the formula for comparison between two ratios in G-power, the sample size was at first calculated to be 110 (55 participants for each group) for a two-tailed test with a confidence level of 95%, test power of 80%. Considering a dropout rate of 20%, the sample size for each group increased to 74. The final sample size therefore totaled 148.
Randomization Procedure
Permuted block randomization was used to randomly allocate participants to each study group. For this purpose, a random allocation sequence with a 1:1 ratio was generated by a computer program. Then a midwife, who was not a member of the research team and therefore was not biased, drew numbers from opaque envelopes consecutively and assigned participants to intervention and control groups.
Participants
The eligible participants were randomly assigned to intervention group (n = 74) or the control group (n = 74). Four participants in the intervention group and seven participants in control group did not complete the questionnaires at the post-trial. Figure 1 shows the flow diagram of the participants during the trial.
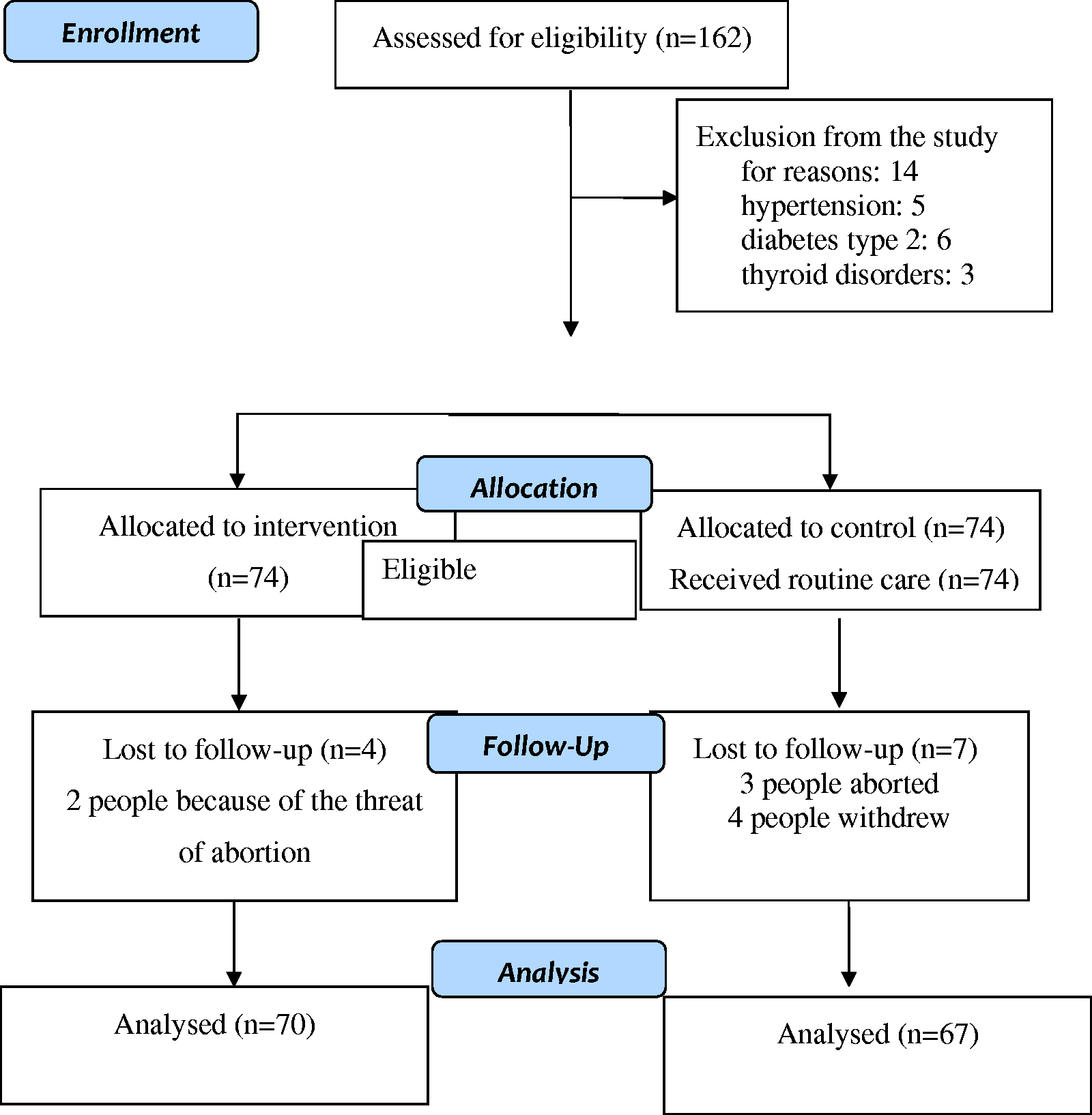
Process of enrollment of participants in the study.
Inclusion criteria were pregnant women over 16 years old, a BMI of ≥25 kg/m2, basic literacy, singleton pregnancy, normal results from the first-trimester test for fasting glucose based on the national and international protocols (maximally, 92 mg/dl28,29 and gestational age from 12 weeks and 1 day to 16 weeks and 6 days. Exclusion criteria included women: with pre-existing diabetes (types 1 and 2), a past history of gestational diabetes, unable to give informed consent in Persian, currently experiencing vaginal bleeding or having severe medical conditions preventing them from doing regular low impact exercises. Moreover, withdrawal from the study at any stage and incomplete questionnaire were the other exclusion criteria.
Eligible participants were selected from pregnant women who visited the Prenatal Care Clinic. First their medical records were studied and then they were contacted and invited to the clinic. Participants were prone to diabetes due to their high BMI. After explaining the objectives of the study thoroughly and obtaining written informed consent, the participants were randomly assigned to the counseling and the usual care groups. Before the study began, all participants had completed the demographic questionnaire and the results of the initial blood glucose test were extracted from their health records.
Intervention
Antenatal usual care (AUC) for all pregnant women was performed according to the national protocol. AUC was provided based on antenatal guidelines of “The Iranian national program on safe motherhood, integrated care on mother’s health”. The antenatal usual care provided by a midwife included eight stages of care; weeks 6–10, 16–20, 26–30, 31–34, 35–37, 38, 39, and 40.The women in the intervention group received four training and counseling sessions based on the IMB model In addition to the AUC . The first consultation session was 90 minutes and was held on the first day of the visit. Subsequent sessions consisted of three 60–90 minute sessions that were held in person each week. Counseling sessions were conducted by the researcher using the IMB model over a four-week period at the gynecology clinic.
In addition, the participants were provided with a booklet on how to perform appropriate physical activities during pregnancy. During each session, PowerPoint presentations, image presentation and question and answer techniques were used. The content of the sessions was as follows: First session: counseling for obesity, nutrition during pregnancy and the impact of obesity on gestational diabetes; second session: counseling on how to do physical activities during pregnancy and its benefits; third session: counseling for diabetes self-care, how to manage stress in pregnancy and its effect on gestational diabetes; fourth session: counseling on the impact of motivation on mental health and continuity of chronic disease control. Standard maternal care was also provided to both groups. Women in the control group received usual care, which in this setting includes initial weighing to calculate BMI. 30 At the end of the counseling sessions, mean plasma glucose levels were measured for both groups at 24 to 28 weeks of gestation. A two-hour, 75-gram oral glucose tolerance test (OGTT) was used to measure blood glucose. In case a blood glucose test result was higher than or equal to normal index (fasting glucose and one hour and two hours later, 92, 180 and 153 mg/dl, respectively)28,29 it was diagnosed as gestational diabetes and the pregnant woman was referred to a gynecologist. Due to the type of intervention in the present study, double-blindness (researchers and pregnant women) was not possible. The outcome was assessed by a prenatal clinic staff who was unaware of the allocation of intervention groups. Moreover, the person who performed the statistical analysis did not know the coding of intervention or control groups.
Data Collection Instruments
The data collection instrument included para-clinical test reports and a two-part questionnaire including demographic characteristics, which was completed by inquiring the participants and also using the information extracted from their medical records by the researcher. The first part of the questionnaire included demographic, social, reproductive, and laboratory information with 17 questions about weight, height, age, number of pregnancies, date of the last menstruation, expected date of delivery, gestational age by week, etc. The second part of the questionnaire consisted of baseline FBS and the result of re-measuring FBS and OGTT at weeks 24–28 with 75 g glucose according to ADA criteria, the national protocol and the World Health Organization's protocol.28–31 It should be noted that fasting glucose test and glucose tolerance test were both performed at the same center.
Data Analysis
The collected data was inputted into SPSS 21 with an appropriate code. Demographic variables were reported using descriptive statistics (mean and standard deviation for quantitative variables and frequency for qualitative variables) and the between-group comparison was performed using t-test and chi-square. Moreover, ANCOVA was used to compare blood glucose between groups and Leven test was used to test homogeneity of variance and homogeneity of regression coefficients. Furthermore, the results of the glucose tolerance test were compared between the two groups using independent t-test. To compare the incidence of diabetes between the two groups, chi-square and relative risk calculations were used.
Results
Of 162 pregnant women evaluated, 148 met the inclusion criteria and agreed to participate in this study. Others were excluded because of type 2 diabetes, high blood pressure, and thyroid disorders. Finally, 137 participants were divided into two groups (70 participants in the counseling and 67 participants in the routine care group) (Figure 1).
Comparison of socio-demographic data showed that there was no significant difference between the two groups (Table 1).
Comparison of Demographic and Social Characteristics of the Samples in Two Groups of Counseling Based on Motivational Model and Behavioral and Control Skills.
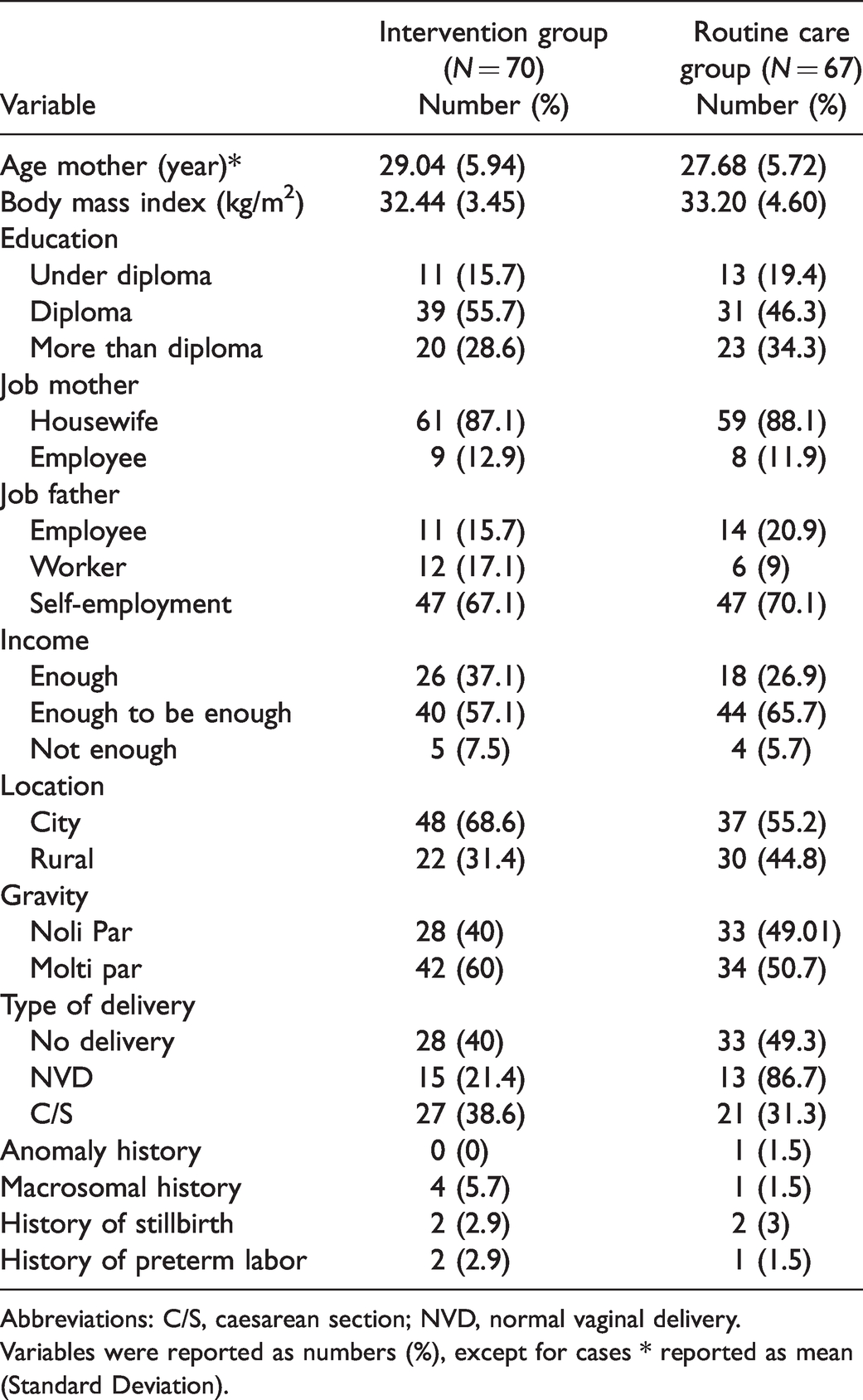
Abbreviations: C/S, caesarean section; NVD, normal vaginal delivery.
Variables were reported as numbers (%), except for cases * reported as mean (Standard Deviation).
Fasting Blood Glucose
Second-trimester fasting blood glucose in both groups was lower than that of the first trimester, but the mean difference in the two groups increased in weeks 24–28, with fasting blood glucose level being significantly lower in the counseling group than in the routine care group (Table 2).
Comparison of Fasting Blood Sugar Levels in Usual Routine Care and Intervention Groups.

Comparison between groups using ANCOVA demonstrated that the difference in fasting blood glucose between the two groups was close to significance level, though it was not statistically significant. The mean difference between the two groups was d = 0.28, indicating a slight difference (Table 2).
OGGT Test
According to the independent t-test, the mean blood glucose in the first-hour and second-hour glucose tolerance tests were significantly lower in the counseling group. In addition, the mean difference of blood glucose level in the first-hour screening of the glucose tolerance test was d = 0.41 and in the second hour of the glucose tolerance test was d = 0.73, which were significantly lower in the counseling group than in the control group (Table 3).
Comparison of First- and Second-Hour Glucose Tolerance Test in Routine Care and Intervention Groups.

Incidence of Gestational Diabetes
In the follow-up, 80.3% of participants did not have gestational diabetes while 19.7% of them had. Chi-square test showed that there was a significant difference between the two groups in terms of the incidence of diabetes (p = .004). The relative risk of gestational diabetes in overweight and obese women who received IMB counseling reduced by 67%, while in the intervention group it was 0.33, 95% CI 95% =0.15– 0.74 (Table 4).
Comparison of Diabetes Frequency (According to National Protocol) Between Counseling and Routine Care Groups.

Discussion
Results of the comparison of mean fasting glucose in overweight and obese pregnant women in both counseling and routine care groups showed that the variance of blood glucose was similar between the two groups. Intergroup comparison suggested that there was a difference in fasting blood glucose between the two groups, which was not statistically significant. In addition, the prevalence of gestational diabetes was significantly lower in the counseling group.
Quinlivan et al. used a four-step motivational counseling approach to antenatal care in overweight and obese women. The results showed that the rate of GDM was significantly reduced, 27 which is consistent with the results of the present study. In the study of Luoto et al., which investigated the effect of the IMB model on self-care in people with type 2 diabetes, it was observed that employing this model controlled glycaemia significantly, 32 which is consistent with the findings of the present study, where using this model also reduced glycaemia but it was not significant. In a study which aimed to evaluate the effect of IMB model on adherence to recommended treatment regimens in patients with diabetes in Babol, using this model was effective on improving self-care and quality of life of patients with diabetes. 33 In addition, Khosravi et al. Conducted a study to investigate the effect of the IMB model on improving weight and body size control in women undergoing weight loss surgery in Shiraz. The results showed that this model has a significant effect on weight control and body size in these women, 34 which is relatively consistent with the present study. In all of the abovementioned studies, the effect of the model on improving diabetes and controlling weight was significant.
In the present study, although there was a difference between the fasting blood glucose in the two groups, it was not statistically significant which may be due to the difference in the study population. Since the participants in the present study were pregnant women and considering pregnancy conditions, diet restrictions and weight control regiments were more stringent for them compared to other populations.
In another study, the authors suggested that the IMB model might be one of the most important factors that enhance physical activities and encourage consumption of fruits and vegetables in adolescents. Moreover, they found that IMB decreased weight, HbA1c levels and blood pressure over the past year, 35 which complies with the results of the present study.
The IMB model is a comprehensive model that promotes health behaviors through encouraging an improved lifestyle, reducing and maintaining weight in an ideal or near-ideal state, strengthening the will to improve health behaviors and avoiding risk factors for chronic diseases including high blood glucose level. The most important strength of this study was evaluation of the effects of behavioral interventions on biological variables (fasting glucose and glucose tolerance test). Other strengths of this study included observing the full principles of counseling, random allocation of participants, and the use of standard questionnaires.
However, the present study has some potential limitations. First, this research was restricted to the pregnant women at a single hospital. Therefore, the results cannot be generalized to all overweight and obese pregnant women. It is suggested that subsequent studies be carried out with a larger number of samples in many different centers. Second, this study was not able to perform blinding due to the nature of the intervention in the study. Third, clinical information including pre-pregnancy height and weight were self-reported, which tend to be slightly different from when directly measured; however, these approaches had been previously used and had been widely mentioned in the literature. 36
Conclusion
Although a lifestyle intervention in early pregnancy using IMB counseling did not significantly decrease fasting blood glucose in overweight and obese pregnant women, there was a significant difference between the mean glucose levels in the two groups. In addition, it can be concluded that the lifestyle intervention was clinically efficacious because it decreased the incidence of gestational diabetes in the intervention group. Therefore, the results of the study showed the positive effect of this model on the prevention of gestational diabetes. It is recommended to investigate the effect of IMB counseling on other maternal and fetal outcomes in overweight and obese pregnant women.
Supplemental Material
sj-pdf-1-qch-10.1177_0272684X211020300 - Supplemental material for The Effectiveness of Information-Motivation-Behavioral Skills Model on Self-Care Practices in Early Pregnancy to Prevent Gestational Diabetes Mellitus in Iranian Overweight and Obese Women: A Randomized Controlled Trial
Supplemental material, sj-pdf-1-qch-10.1177_0272684X211020300 for The Effectiveness of Information-Motivation-Behavioral Skills Model on Self-Care Practices in Early Pregnancy to Prevent Gestational Diabetes Mellitus in Iranian Overweight and Obese Women: A Randomized Controlled Trial by Narges Sadat Motahari-Tabari, F. Nasiri-Amiri, Mahbobeh Faramarzi, Marjan Ahmad Shirvani, Afsaneh Bakhtiari and Shabnam Omidvar in International Quarterly of Community Health Education
Footnotes
Ethics Approval and Consent to Participate
All procedures were carried out on the basis of ethics standards of the responsible committee on human experimentation (institutional and national) and to the Declaration of Helsinki. In addition, the ethics Committee of BUMS approved the study (NO. IR.MUBABOL.HRI.REC.1397.068). All participants provided an informed written and signed consent form. All patients provided written informed consent.
Acknowledgments
This paper was a thesis for receiving M.Sc. degree in counseling in Midwifery which approved by Babol University of Medical Sciences. The authors would like to thank this university for its financial support. The authors also would like to extend their sincere thanks to all the participants who helped them in this research despite their difficult pregnancy conditions.
Author Contributions
N. Motahari-Tabari conceived and designed the study, she also did data collection. M. Faramarzi, M. Shirvani, A. Bakhtiari, S. Omidvar, F. Bakouei reviewed the literature, analyzed and interpreted data, drafted and prepared the manuscript. F. Nasiri-Amiri developed the first draft of this manuscript and had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved and funded by the Deputy for Research of Babol University of Medical Sciences (grant no. 9705313).
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.