
Abstract
Introduction
In the East Mediterranean area, cardiovascular diseases are estimated to account for more than 50% of annual mortalities (2.2 million) and 60% of diseases. 1 the prevalence of cardiovascular diseases is ever growing in the East Mediterranean countries and they are considered the main cause of diseases and mortalities. 2 In fact, 55% of mortalities induced by non-contagious diseases relate to cardiovascular diseases. Hypertension is a main cause of cardiovascular diseases. As estimated by WHO, 62% of brain strokes and 49% of heart coronary diseases are caused by hypertension.3,4 Besides lifestyle and eating habits that might affect blood pressure, there is evidence that salt consumption is correlated with hypertension.2,5
Overconsumption of salt has been reported to account for about half of the disease loads attributed to hypertension. 6 Overconsumption of salt is associated with renal diseases, higher risk of obesity, osteoporosis, kidney stone and gastric cancer. Across different countries, salt overconsumption is prevalent and this prevalence has been reported to been higher in Asian countries including Iran.7,8 Many investigations have shown so far that reduced salt consumption in all age groups can lower blood pressure. Besides, a slight reduction in salt consumption can reduce the rate of brain stroke and can reduce the rate of mortalities induced by heart attack for more than 7%. 2 A reduction of sodium for 1.74 grams a day on average can lower systolic blood pressure for 3.4 mmHg and diastolic blood pressure for 1.5 mmHg. 9 The goal that WHO pursues is to reduce the rate of salt consumption for 25%, which can be one of the most effective ways of preventing cardiovascular diseases and the concomitant disabilities and can finally significantly improve public health. 6
In the light of the body of research on the positive effects of limited salt consumption at a global scale, it seems essential to design and implement effective interventions with the aim of reducing salt consumption among people. The first step to develop these interventions is consumer analysis and awareness of public perspectives and experiences especially women. This can be the key to the identification of facilitating factors resembling a trigger from inside such as perceived symptoms of a disease or from outside such as the affliction with a disease in the family. 10 To identify these factors, qualitative research is essential. The existing body of related literature lacks any work of research exploring these factors among women. Therefore, the present research aims to explain the facilitating factors involved in less salt intake among women.
Methods
Design of Study
The present qualitative research used conventional content analysis with 42 women and healthcare providers selected through purposeful sampling method. Semi-structured interviews were held to obtain in-depth information along with focal group discussions. Data analysis was done through Graneheim and Lundman’s approach. 11
Data Collection
The required data were collected through focal group discussions (three groups of 6) and semi-structured individual interviews with 13 women and 11 healthcare providers. All the interviews were audio-recorded and the data collection continued until data satiation. The initial questions of individual and focus group are shown in Table 1.
Participants
Demographic characteristics of the participants are shown in Table 2. The participants were 42 in number including 31 women whose age ranged between 20 and 65 years residing in Hamidia Town, Yazd, Iran, and 11 healthcare providers. Based on the inclusion criteria, women who participated in making foods, had the ability to communicate, had no heart disease, and had no low-salt diet were eligible for the study. With regard to the healthcare providers, having at least 2 years of work experience was required to enter the study. The exclusion criteria were pregnancy, lactation, and lack of willingness to participate in the study .The sampling method was varimax purposive to include different age groups, education levels and occupations.
Data Analysis
To analyze the data, Graneheim and Lundman’s approach was followed. 11 The qualitative content analysis was conventional in type. The recorded interviews were transcribed and initial codes were extracted. To set the main concepts, similar codes were assigned to the same category. Then, a number of sub-categories were defined and similar categories were arranged side by side and incorporated into larger main categories. Then, the themes were extracted.
Credibility and Reliability of Data
To set the validity and reliability of the study, the criterion suggested by Guba and Lincoln was used. To test the credibility of data, consistent examination of data was used along with voice-recording, transcription and data analysis immediately after the interviews. The extracted codes were also reviewed by participants (the process of member check) in order to confirm the relevance of content analysis. Data analysis was done with the help of two qualitative researchers and consistent involvement with data. Data dependency was tested through external check and providing several coded response texts to experienced professors to agree on the coding method. Participants’ exact description including varimax sampling, data collection factors and place were used for more data transfer. To maximize homogeneity and objectivity, the details of the research procedures were described and fully recorded for all the steps of data collection (text, coding, analysis). 12
Ethical Considerations
For ethical considerations, the purpose of research and interview procedure was explained to participants before the personal interviews or group discussions. Then, the interview was held with participants’ informed consent and confidentiality of the information they provided. This STUDY was approved by the ethics committee under ethical code of IR.SSU.SPH.REC.1397.141.
Results
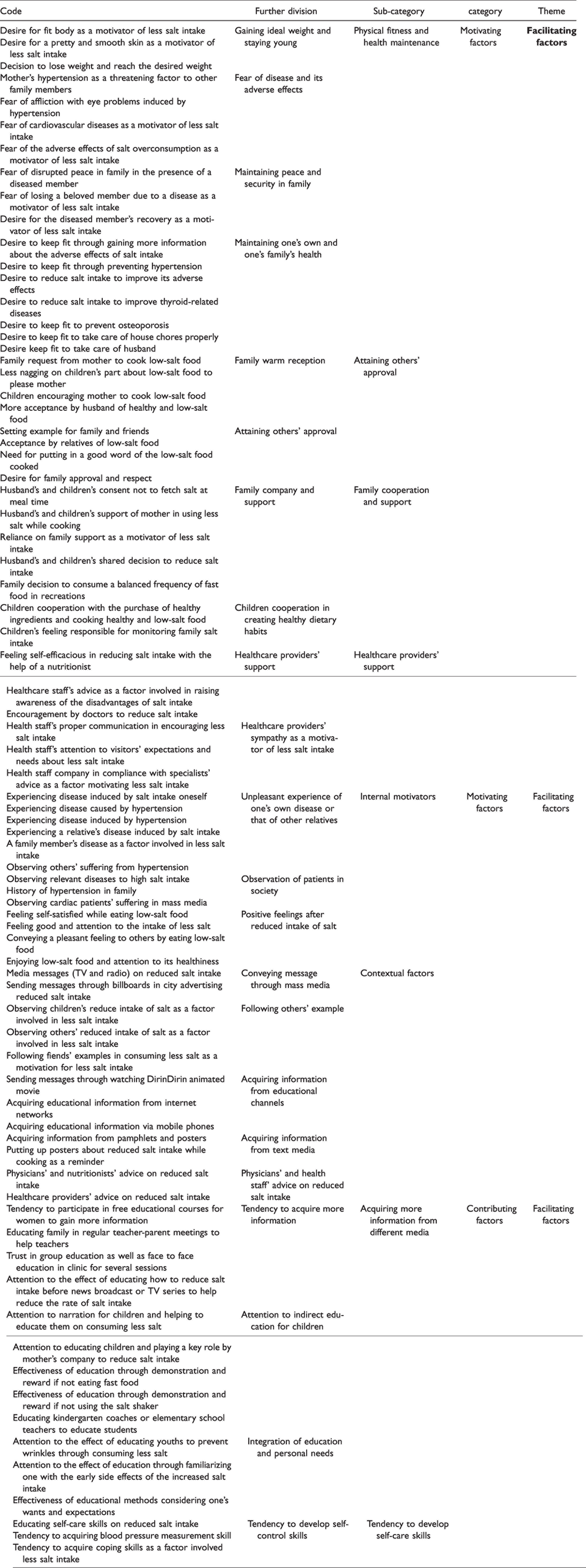
The data analysis led to the extraction of two main categories, motivating and facilitating factors involved in cutting down on salt consumption. As it can be observed in the following table 3, a sample of extracted codes in each sub-category can be observed.
Motivating Factors
This category consists of six sub-categories:
Physical Fitness and Health Maintenance
There are several additional sub-categories to physical fitness and health maintenance: desire to achieve ideal weight and stay young, fear of diseases and adverse effects, family peace and security, desire to maintain one’s own and family’s health. The majority of participants expressed health maintenance as the key motivation for reduced salt consumption in family. Here is a sample of participants’ accounts: “If I get down with a disease, such as hypertension, then I begin to reduce salt consumption”. (M10, housewife, 30 years old) “If I intend to go on a diet and lose weight, I should cut down on salt and sugar as much as I can or even do without them so that I can lose weight”. (M9, teacher, 50 years old)
Others’ Approval
This sub-category resembled some others such as warm family reception and desire for attracting others’ approval. The majority of mother participants expressed that if their family asked them to cook low-salt food and encourage them to do so; they will be motivated to reduce salt consumption. With this concern, here is a sample account: “It matters to me whether others put in a good word for my cooking. I really care”. (M6, employee, 29 years old) “My husband and children do not agree with doing without salt and salt shaker during main meals. They start nagging” (M1, housewife, 38 years old)
Family Support and Cooperation
This sub-category, similar to family company and support and children cooperation, was formed to create healthy dietary manners. In fact, family support was stated as the most significant factor affecting the reduction of salt consumption. “When my food has less salt in it, if my children do not nag and instead begin to put in a good word, I will feel good and be encouraged to add less salt to food”. (M2, FGD, housewife, 42 years old)
Internal Motivators
This sub-category, in its own turn, comprises several further subcategories such as unpleasant experience of getting sick or seeing others sick, observation of the sick in society, positive feelings resulting from less salt consumption. This internal feeling is a motivating factor for less salt consumption. It acts as an internal cue for action to guide one to a particular behavior.
With this concern, here is a sample of accounts: “Another motivator is to see those around us with the kind of problems they have due to salt consumption. This is instructive to me and pushes me to consume less salt”. (M9, teacher, 50 years old)
Contextual Motivators
This sub-category consists of further categorizations such as sending messages through mass media, following others’ example, acquiring more information from communication networks, acquiring information from text media, doctors’ or health specialists’ advice on less salt consumption, which all act as internal cues for action to guide on toward the target behavior.
Here is a sample account from the participants: “Billboards throughout cities near high-traffic intersections and places can be effective in raising public awareness”. (M1, employee, 37 years old) “Those around me especially my daughter really care about their health. When I see her, I tell myself why not me?!” (M9, teacher, 50 years old)
Healthcare Providers’ Support
This sub-category consists of several divisions such as healthcare providers’ support and healthcare providers’ sympathy to motivate reduced salt consumption.
As stated by the participants, “if they are encouraged by the visiting doctor to consume less salt and the doctor also shows enough follow-up, they might be able to add less salt to food while cooking”. (M9, teacher, 50 years)
Facilitating Factors
This category is made up of three sub-categories as it can be seen below.
Access to More Information Through Different Instructions
This subcategory consists of several divisions including desire to get more information considering indirect education for children and a mixture of educational methods and individuals’ primary wants or needs. With this respect, here is a sample account: “Knowledge of the disadvantages of salt can help consume less salt. Yet, we only think it increases blood pressure. There might be other outcomes of which we might be unaware. If we are aware of the disadvantages of salt, we take more care”. (M2, FGD, housewife, 42 years old) Another sample account is: “Holding free training courses in medical centers can positively affect our awareness”. (M5, housewife, 50 years old)
Acquisition of Self-Care Skills
This subcategory has several divisions such as one’s desire to develop self-care skills and coking skill. The majority of women participants perceived cooking different foods and acquiring self-control skills in adding salt to food as a facilitating factor involved in consuming less salt. With this concern, one of participants commented: “The variety of food and the way it is cooked really matter. If we use healthier alternatives, we can reduce the salt in food better and more”. (M10, housewife, 30 years) Another participant commented: “One skill is to provide us with a barometer to measure our blood pressure on a daily basis and take care of our health”. (M5, housewife, 50 years old)
Nutritional Advice as a Factor Involved in Reducing Salt Intake
As the majority of healthcare providers maintained, advising women and creating a sense of need encourage them to consume less salt. Consulting with a psychologist helps people pay more attention to their health and accept specialists’ recommendations on consuming less salt.
With this regard, the nutritionist at the healthcare center maintains: “A psychologist should talk them into the matter make them feel from inside so that when they visit the nutritionist, they can listen to him, accept what he sees and do as recommended”. (M32, nutritionist, 29 years old) “Psychologically speaking, it needs more efforts. They need to receive a package prepared prioritizing health. They should feel then need from inside”. (M36, family doctor, 30 years old)
Discussion
The present qualitative research aimed to explain the facilitating factors of reduced salt intake among women residents of Hamidia in Yazd province. The majority of participants in this research mentioned health maintenance as the main motivator of reducing salt consumption in family. This factor was also mentioned by other researchers such as de Brito‐Ashurst et al. 13 and Rahimdel et al. 14 as a personal facilitating factors. One other point raised by Layeghiasl et al. 15 concerning the benefits of less salt intake was maintaining health and preventing heart diseases and other diseases.
In the present research, attaining others’ approval and family support were categorized among motivating factors. In another study by Keshavarz, the role of spouse, mother and children showed to be significant in performing healthy nutritional behaviors. 16 With this respect, Zou also showed in his research that family member support was among the facilitating family-related factors involved in less salt intake. This is consistent with the present finding. 17 Educating family and making shared decision can turn the reduced salt consumption a pleasant experience for the family in his research, Zou pointed out the critical state of family healthcare as a main family-related factor that facilitated attempts to reduce salt intake. 17 Similarly, in the present research, one family member’s disease, unpleasant personal experience of a disease or that of a relative are mentioned among internal motivating factors which can act as a cue for action and move one toward consuming less salt. These factors if enhanced can bring about consistent attempts to consume less salt.
Moreover, observing patients’ suffering in mass media and in community was mentioned as a motivating factor. This was also raised by Zou 17 who drew attention to the effects of healthy diet in society and categorized it as a facilitating factor of less salt intake.
A contextual motivator in the present research was obtaining information from mass media, text media and following others’ example. These all acted as cues for action and moved one toward consuming less salt. In his research, Rahimdel 18 assigned these to the external cues for action sub-category and social factors category.
In this research, being supported by the healthcare provider was a motivator of consuming less salt. In explaining the facilitating factors of chronic diseases, the support of a professional healthcare providers showed to affect compliance with nutritional diet. 19 This is consistent with the finding of the present research.
Participants of the present research mentioned contextual and motivating support as the main factors involved in behavioral change. This is consistent with the findings reported by Ji and Cappuccio 20 and Kholdi et al. 21 Here, the participants mentioned one’s desire to get more information and acquire self-care skills among the facilitating factors of reduced salt intake. Having the required level of awareness and skills was also mentioned by de-Brito‐Ashurst et al. 13 as a facilitating factor. This was partially consistent with the present findings. With this respect, Zou 17 also pinpointed self-care as a facilitating personal factor. In a systematic review, Batcagan-Abueg et al. 22 maintained that an effective strategy to reduce salt intakein different countries was to make certain interventions to raise awareness of the disadvantages of salt over-consumption. In a qualitative study in India, 23 raising awareness of salt intake was mentioned as a facilitating factor involved in consuming less salt.
In some other qualitative research, Layeghiasl et al. 15 mentioned consultation on salt overconsumption and raising awareness of its disadvantages as among the strategies. In the present research too, consultation showed to be a facilitating factor for less salt intake by women due to their perceived need of doing so. It seems that holding personal consultation sessions with this concern can be an effective factor in reducing salt intake which needs to be considered in developing interventions.
In the present research, the majority of participants mentioned holding free training courses, family education and attention to child education along with narration and drama among the facilitating factors of reduced salt intake.
In the light of the body of different research, different educational programs based on the suggested strategies can help reduce salt intake.20,24 Thus, the facilitating factors of reduced salt intake and developing proper educational and advertising programs can help raise women’s awareness and change their behavior with this concern.
Strengths and Limitations
The strength of this study was considering health- care providers rather than women who have a definite role in designing and executing programs for this important target group. The study findings provided deeper understanding about the effective factors related to motivating women to practice salt reduction. These new findings are relevant for stakeholders to develop culturally proper educational interventions.
Among the main limitations of the study was people’s nothing feel free to tell the truth about the determinants of reduced salt intake. Thus, the researcher attempted to provide a secure environment to speak with the participants and enquire about their perspectives to make up for this limitation.The present finding, like any other qualitative research, depend on time and place. Moreover, as the research population here consisted of a group of women with a particular cultural and geographical background, generalization should only be done cautiously.
We conducted a qualitative study, for situation market analysis to elucidate the related factors that constrain behavior adoption. It is suggested to design an intervention program through multiple communication channels in our community. Based on our result we recommend using facilitators and motivators in future educational community programs.
Conclusions
Considering the qualitative findings about motivating and facilitating factors, it is essential to enhance internal motivators and information acquisition via different communication channels such as schools. Healthcare providers and public associations pave the way for attracting more family and healthcare staff support, developing proper educational and advertising plans in order to raise women’s awareness and change their attitude and behavior with this respect.
The Initial Questions in Individual and Focus Group Interviews.
Demographic Characteristics of the Interviewees.

Sample Codes, Categories, Sub-Categories and Further Divisions Extracted From Qualitative Results.

Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.